

Relationship between Handgrip Strength and Incident Diabetes in Korean Adults According to Gender: A Population-Based Prospective Cohort Study

Abstract
1. Introduction
2. Materials and Methods
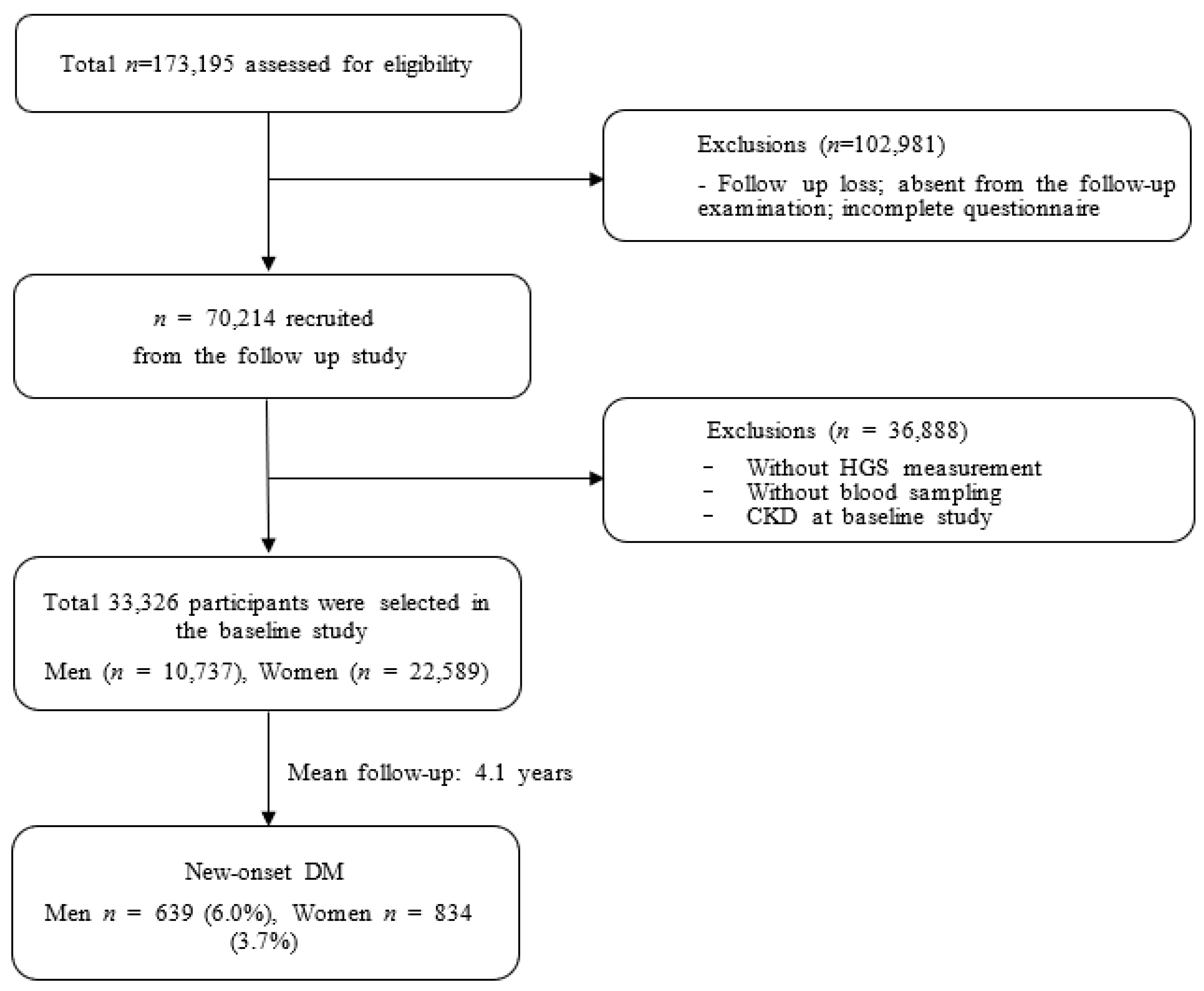
2.1. Study Population
2.2. Measurement of Handgrip Strength
2.3. Anthropometric and Laboratory Measurements and General Data
2.4. Definition of DM
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nolan, C.J.; Damm, P.; Prentki, M. Type 2 diabetes across generations: From pathophysiology to prevention and management. Lancet 2011, 378, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of Diabetes and Diabetes-Related Complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.J.; Doherty, T.J. Sarcopenia: Prevalence, mechanisms, and functional consequences. Interdiscip. Top Gerontol. 2010, 37, 94–114. [Google Scholar] [PubMed]
- Mayhew, A.J.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.D.; de Souza, R.J.; Thabane, L.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2018, 48, 48–56. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-J.; Peng, L.-N.; Chiou, S.-T.; Chen, L.-K. Relative Handgrip Strength Is a Simple Indicator of Cardiometabolic Risk among Middle-Aged and Older People: A Nationwide Population-Based Study in Taiwan. PLoS ONE 2016, 11, e0160876. [Google Scholar] [CrossRef] [PubMed]
- Choquette, S.; Bouchard, D.R.; Doyon, C.Y.; Sénéchal, M.; Brochu, M.; Dionne, I.J. Relative strength as a determinant of mobility in elders 67–84 years of age. A nuage study: Nutrition as a determinant of successful aging. J. Nutr. Health Aging 2010, 14, 190–195. [Google Scholar] [CrossRef]
- Lombardo, M.; Padua, E.; Campoli, F.; Panzarino, M.; Mîndrescu, V.; Annino, G.; Iellamo, F.; Bellia, A. Relative handgrip strength is inversely associated with the presence of type 2 diabetes in overweight elderly women with varying nutritional status. Acta Diabetol. 2020, 58, 25–32. [Google Scholar] [CrossRef]
- Lee, S.-B.; Moon, J.-E.; Kim, J.-K. Association of Handgrip Strength with Diabetes Mellitus in Korean Adults According to Sex. Diagnostics 2022, 12, 1874. [Google Scholar] [CrossRef]
- Wander, P.; Boyko, E.; Leonetti, D.; McNeely, M.; Kahn, S.; Fujimoto, W. Greater Hand-grip strength predicts a lower risk of developing type 2 diabetes over 10 years in leaner Japanese Americans. Diabetes Res. Clin. Pract. 2011, 92, 261–264. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.-G.; Group, K. Cohort profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.-J.; Lee, S.K.; Shin, C. Normalized Hand Grip and Back Muscle Strength as Risk Factors for Incident Type 2 Diabetes Mellitus: 16 Years of Follow-Up in a Population-Based Cohort Study. Diabetes, Metab. Syndr. Obes. Targets Ther. 2021, 14, 741–750. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-B.; Kwon, Y.-J.; Jung, D.-H.; Kim, J.-K. Association of Muscle Strength with Non-Alcoholic Fatty Liver Disease in Korean Adults. Int. J. Environ. Res. Public Health 2022, 19, 1675. [Google Scholar] [CrossRef]
- Li, D.; Guo, G.; Xia, L.; Yang, X.; Zhang, B.; Liu, F.; Ma, J.; Hu, Z.; Li, Y.; Li, W.; et al. Relative Handgrip Strength Is Inversely Associated with Metabolic Profile and Metabolic Disease in the General Population in China. Front. Physiol. 2018, 9, 59. [Google Scholar] [CrossRef]
- Lee, J.S.; Song, Y.H. Relationship between Waist Circumference and Cardiovascular Risk Factors in Adolescents: Analysis of the Korea National Health and Nutrition Examination Survey Data. Korean Circ. J. 2020, 50, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.G.; Kim, K.H.; Koh, J.S.; Park, J.R.; Hwang, S.J.; Hwang, J.Y.; Ahn, J.H.; Jang, J.Y.; Jeong, Y.H.; Kwak, C.H. Association between pulse pressure and body mass index in hypertensive and normotensive populations in the korea national health and nutrition examination survey v, 2010–2012. J. Clin. Hypertens. 2016, 19, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V. National heart, lung, and blood institute joint national committee on prevention, detection, evaluation, and treatment of high blood pressure; national high blood pressure education program coordinating committee: The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar]
- Yoshimoto, H.; Takayashiki, A.; Goto, R.; Saito, G.; Kawaida, K.; Hieda, R.; Kataoka, Y.; Aramaki, M.; Sakamoto, N.; Maeno, T.; et al. Association between Excessive Alcohol Use and Alcohol-Related Injuries in College Students: A Multi-Center Cross-Sectional Study in Japan. Tohoku J. Exp. Med. 2017, 242, 157–163. [Google Scholar] [CrossRef]
- Kang, K.; Sung, J.; Kim, C.-Y. High Risk Groups in Health Behavior Defined by Clustering of Smoking, Alcohol, and Exercise Habits: National Heath and Nutrition Examination Survey. J. Prev. Med. Public Health 2010, 43, 73–83. [Google Scholar] [CrossRef]
- Kim, S.; Choi, S.; Kim, J.; Park, S.; Kim, Y.-T.; Park, O.; Oh, K. Trends in health behaviors over 20 years: Findings from the 1998–2018 Korea National Health and Nutrition Examination Survey. Epidemiol. Health 2021, 43, e2021026. [Google Scholar] [CrossRef]
- Association, A.D. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [PubMed]
- Labott, B.K.; Bucht, H.; Morat, M.; Morat, T.; Donath, L. Effects of Exercise Training on Handgrip Strength in Older Adults: A Meta-Analytical Review. Gerontology 2019, 65, 686–698. [Google Scholar] [CrossRef]
- Ahn, H.; Choi, H.Y.; Ki, M. Association between levels of physical activity and low handgrip strength: Korea national health and nutrition examination survey 2014–2019. Epidemiol. Health 2022, 44, e2022027. [Google Scholar] [CrossRef] [PubMed]
- Seong, J.Y.; Ahn, H.Y.; Park, Y.; Shin, S.; Ha, I.-H. Association Between Aerobic Exercise and Handgrip Strength in Adults: A Cross-Sectional Study Based on Data from the Korean National Health and Nutrition Examination Survey (2014–2017). J. Nutr. Health Aging 2020, 24, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Lawman, H.G.; Troiano, R.P.; Perna, F.M.; Wang, C.Y.; Fryar, C.D.; Ogden, C.L. Associations of relative handgrip strength and cardiovascular disease biomarkers in u.S. Adults, 2011–2012. Am. J. Prev. Med. 2015, 50, 677–683. [Google Scholar] [PubMed]
- Hu, S.; Gu, Y.; Lu, Z.; Zhang, Q.; Liu, L.; Meng, G.; Yao, Z.; Wu, H.; Bao, X.; Chi, V.T.Q.; et al. Relationship Between Grip Strength and Prediabetes in a Large-Scale Adult Population. Am. J. Prev. Med. 2019, 56, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Momma, H.; Sawada, S.S.; Kato, K.; Gando, Y.; Kawakami, R.; Miyachi, M.; Huang, C.; Nagatomi, R.; Tashiro, M.; Ishizawa, M.; et al. Physical Fitness Tests and Type 2 Diabetes Among Japanese: A Longitudinal Study From the Niigata Wellness Study. J. Epidemiol. 2019, 29, 139–146. [Google Scholar] [CrossRef]
- Richter, E.A.; Hargreaves, M. Exercise, GLUT4, and Skeletal Muscle Glucose Uptake. Physiol. Rev. 2013, 93, 993–1017. [Google Scholar] [CrossRef]
- Agostinis-Sobrinho, C.A.; Moreira, C.; Abreu, S.; Lopes, L.; Sardinha, L.B.; Oliveira-Santos, J.; Oliveira, A.; Mota, J.; Santos, R. Muscular fitness and metabolic and inflammatory biomarkers in adolescents: Results from LabMed Physical Activity Study. Scand. J. Med. Sci. Sports 2016, 27, 1873–1880. [Google Scholar] [CrossRef]
- Visser, M.; Pahor, M.; Taaffe, D.R.; Goodpaster, B.H.; Simonsick, E.M.; Newman, A.B.; Nevitt, M.; Harris, T.B. Relationship of interleukin-6 and tumor necrosis factor-α with muscle mass and muscle strength in elderly men and women: The Health ABC Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M326–M332. [Google Scholar] [CrossRef]
- Taaffe, D.R.; Harris, T.B.; Ferrucci, L.; Rowe, J.; Seeman, T.E. Cross-sectional and Prospective Relationships of Interleukin-6 and C-Reactive Protein With Physical Performance in Elderly Persons: MacArthur Studies of Successful Aging. J. Gerontol. Ser. A 2000, 55, M709–M715. [Google Scholar] [CrossRef] [PubMed]
- Derbré, F.; Gratas-Delamarche, A.; Gómez-Cabrera, M.C.; Viña, J. Inactivity-induced oxidative stress: A central role in age-related sarcopenia? Eur. J. Sport Sci. 2014, 14, S98–S108. [Google Scholar] [CrossRef] [PubMed]
- Kamijo, Y.; Kanda, E.; Ishibashi, Y.; Yoshida, M. Sarcopenia and Frailty in PD: Impact on Mortality, Malnutrition, and Inflammation. Perit. Dial. Int. J. Int. Soc. Perit. Dial. 2018, 38, 447–454. [Google Scholar] [CrossRef]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, A.D.; Cross, J.; Kharbanda, R.K.; Mullen, M.J.; Bhagat, K.; Taylor, M.; Donald, A.E.; Palacios, M.; Griffin, G.E.; Deanfield, J.E.; et al. Acute Systemic Inflammation Impairs Endothelium-Dependent Dilatation in Humans. Circulation 2000, 102, 994–999. [Google Scholar] [CrossRef] [PubMed]
- Pinkney, J.H.; DA Stehouwer, C.; Coppack, S.W.; Yudkin, J.S. Endothelial Dysfunction: Cause of the Insulin Resistance Syndrome. Diabetes 1997, 46, S9–S13. [Google Scholar] [CrossRef] [PubMed]
- Caturano, A.; D’angelo, M.; Mormone, A.; Russo, V.; Mollica, M.P.; Salvatore, T.; Galiero, R.; Rinaldi, L.; Vetrano, E.; Marfella, R.; et al. Oxidative Stress in Type 2 Diabetes: Impacts from Pathogenesis to Lifestyle Modifications. Curr. Issues Mol. Biol. 2023, 45, 6651–6666. [Google Scholar] [CrossRef] [PubMed]
- Sreedhar, A.; Zhao, Y. Uncoupling protein 2 and metabolic diseases. Mitochondrion 2017, 34, 135–140. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine–Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Powers, S.K.; Radak, Z.; Ji, L.L. Exercise-induced oxidative stress: Past, present and future. J. Physiol. 2016, 594, 5081–5092. [Google Scholar] [CrossRef]
- Ji, L.L.; Kang, C.; Zhang, Y. Exercise-induced hormesis and skeletal muscle health. Free Radic. Biol. Med. 2016, 98, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Manda, C.M.; Hokimoto, T.; Okura, T.; Isoda, H.; Shimano, H.; Wagatsuma, Y. Handgrip strength predicts new prediabetes cases among adults: A prospective cohort study. Prev. Med. Rep. 2020, 17, 101056. [Google Scholar] [CrossRef] [PubMed]
- Nevill, A.M.; Tomkinson, G.R.; Lang, J.J.; Wutz, W.; Myers, T.D. How Should Adult Handgrip Strength Be Normalized? Allometry Reveals New Insights and Associated Reference Curves. Med. Sci. Sports Exerc. 2021, 54, 162–168. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Men | Q1 | Q2 | Q3 | Q4 | p-Value | |
|---|---|---|---|---|---|---|
| ≤1.40 | 1.40–1.61 | 1.61–1.84 | >1.84 | |||
| n | 10,737 | 2693 | 2675 | 2715 | 2654 | |
| HGS (kg) | 39.1 ± 8.5 | 30.1 ± 6.2 | 37.3 ± 37.3 | 41.4 ± 4.3 | 47.5 ± 7.6 | <0.001 |
| RGS (kg/BMI) | 1.62 ± 0.37 | 1.18 ± 0.2 | 1.51 ± 0.06 | 1.72 ± 0.07 | 2.08 ± 0.26 | <0.001 |
| Age (years) | 54.8 ± 8.5 | 57.9 ± 8.1 | 55.9 ± 8.1 | 54.2 ± 8.2 | 50.9 ± 7.9 | <0.001 |
| Waist circumference (cm) | 85.1 ± 7.4 | 88.0 ± 7.4 | 86.0 ± 6.7 | 84.6 ± 6.9 | 81.4 ± 7.0 | <0.001 |
| BMI (kg/m2) | 24.3 ± 2.7 | 25.6 ± 2.8 | 24.8 ± 2.4 | 24.1 ± 2.4 | 22.8 ± 2.4 | <0.001 |
| Total cholesterol (mg/dL) | 193.6 ± 33.9 | 193.9 ± 34.5 | 195.0 ± 34.4 | 193.9 ± 33.8 | 191.7 ± 33.0 | 0.004 |
| HDL-cholesterol (mg/dL) | 50.0 ± 12.0 | 48.4 ± 11.3 | 49.4 ± 11.9 | 50.3 ± 11.9 | 52.0 ± 12.6 | <0.001 |
| Triglyceride (mg/dL) | 145.5 ± 96.1 | 150.5 ± 92.5 | 151.0 ± 98.2 | 145.4 ± 93.6 | 135.0 ± 99.4 | <0.001 |
| AST (IU/L) | 24.8 ± 12.9 | 25.2 ± 11.5 | 25.5 ± 15.8 | 24.8 ± 13.1 | 23.8 ± 10.5 | <0.001 |
| ALT (IU/L) | 25.4 ± 18.2 | 26.7 ± 16.5 | 26.7 ± 24.6 | 25.2 ± 15.6 | 22.9 ± 13.8 | <0.001 |
| SBP (mmHg) | 125.3 ± 13.8 | 126.9 ± 14.1 | 125.6 ± 13.7 | 125.3 ± 13.7 | 123.5 ± 13.6 | <0.001 |
| DBP (mmHg) | 78.1 ± 9.4 | 79.0 ± 9.3 | 78.2 ± 9.30 | 78.0 ± 9.4 | 77.2 ± 9.5 | <0.001 |
| Alcohol intake, n (%) | 3662 (34.1) | 803 (29.8) | 896 (33.5) | 982 (36.2) | 981 (37.0) | <0.001 |
| Smoking status, n (%) | <0.001 | |||||
| Never smoker | 2903 (27.1) | 782 (29.1) | 719 (27.0) | 740 (27.3) | 662 (25.0) | |
| Ex-smoker | 4828 (45.1) | 1266 (47.2) | 1229 (46.1) | 1236 (45.7) | 1097 (41.5) | |
| Current smoker | 2968 (27.7) | 635 (23.7) | 716 (26.9) | 730 (27.0) | 887 (33.5) | |
| Regular exercise, n (%) | 4467 (41.6) | 1141 (42.4) | 1160 (43.4) | 1570 (42.2) | 1633 (38.5) | 0.002 |
| Hypertension, n (%) | 2402 (22.4) | 872 (32.4) | 651 (24.4) | 552 (20.4) | 327 (12.3) | <0.001 |
| CVD, n (%) | 395 (3.7) | 136 (5.1) | 114 (4.3) | 89 (3.3) | 56 (2.1) | <0.001 |
| Women | Q1 | Q2 | Q3 | Q4 | p-Value | |
|---|---|---|---|---|---|---|
| ≤0.85 | 0.85–1.01 | 1.01–1.17 | >1.17 | |||
| n | 22,589 | 5492 | 5752 | 5717 | 5628 | |
| HGS (kg) | 23.5 ± 2.2 | 17.9 ± 3.7 | 22.4 ± 2.5 | 25.0 ± 2.6 | 28.7 ± 4.6 | <0.001 |
| RGS (kg/BMI) | 1.02 ± 0.25 | 0.71 ± 0.13 | 0.93 ± 0.05 | 1.09 ± 0.05 | 1.33 ± 0.18 | <0.001 |
| Age (years) | 52.9 ± 7.7 | 56.5 ± 7.5 | 54.0 ± 7.4 | 51.9 ± 7.2 | 49.3 ± 6.8 | <0.001 |
| Waist circumference (cm) | 77.5 ± 8.0 | 81.7 ± 8.2 | 78.8 ± 7.5 | 76.5 ± 7.1 | 73.2 ± 6.7 | <0.001 |
| BMI (kg/m2) | 23.5 ± 2.9 | 25.3 ± 3.1 | 24.0 ± 2.6 | 23.0 ± 2.3 | 21.6 ± 2.2 | <0.001 |
| Total cholesterol (mg/dL) | 200.2 ± 35.0 | 204.2 ± 36.3 | 202.3 ± 35.1 | 199.6 ± 34.8 | 194.9 ± 33.3 | <0.001 |
| HDL-cholesterol (mg/dL) | 56.7 ± 13.0 | 54.3 ± 12.3 | 55.8 ± 12.6 | 57.0 ± 12.9 | 59.8 ± 13.5 | <0.001 |
| Triglyceride (mg/dL) | 111.0 ± 70.0 | 124.2 ± 73.9 | 116.3 ± 76.4 | 108.3 ± 66.0 | 95.2 ± 58.9 | <0.001 |
| AST (IU/L) | 22.0 ± 9.9 | 23.1 ± 10.5 | 22.4 ± 12.4 | 21.7 ± 8.8 | 20.8 ± 7.0 | <0.001 |
| ALT (IU/L) | 19.0 ± 14.6 | 21.2 ± 17.8 | 19.7 ± 17.0 | 18.4 ± 11.1 | 16.8 ± 10.6 | <0.001 |
| SBP (mmHg) | 120.6 ± 14.6 | 122.7 ± 14.6 | 121.4 ± 14.7 | 120.3 ± 14.7 | 117.8 ± 14.1 | <0.001 |
| DBP (mmHg) | 74.1 ± 9.4 | 75.3 ± 9.3 | 74.5 ± 9.4 | 73.9 ± 9.5 | 72.6 ± 9.3 | <0.001 |
| Alcohol intake, n (%) | 1117 (4.9) | 206 (3.8) | 267 (4.6) | 306 (5.4) | 338 (6.0) | <0.001 |
| Smoking status, n (%) | 0.019 | |||||
| Never smoker | 21,774 (96.9) | 5314 (97.2) | 5536 (96.9) | 5527 (97.3) | 5397 (96.3) | |
| Ex-smoker | 289 (1.3) | 73 (1.3) | 71 (1.2) | 66 (0.2) | 79 (1.4) | |
| Current smoker | 405 (1.8) | 81 (1.5) | 105 (1.8) | 89 (1.6) | 130 (2.3) | |
| Regular exercise, n (%) | 9386 (41.6) | 3359 (38.8) | 2368 (41.2) | 2477 (43.3) | 2408 (42.8) | <0.001 |
| Hypertension, n (%) | 3592 (15.9) | 1290 (23.5) | 1019 (17.8) | 796 (13.9) | 487 (8.7) | <0.001 |
| CVD, n (%) | 439 (1.9) | 199 (3.6) | 120 (2.1) | 84 (1.5) | 36 (0.6) | <0.001 |
| Men | Women | ||||
|---|---|---|---|---|---|
| HR | p-Value | HR | p-Value | ||
| Unadjusted | 0.52 (0.42–0.65) | <0.001 | Unadjusted | 0.27 (0.20–0.36) | <0.001 |
| Model 1 | 0.57 (0.45–0.72) | <0.001 | Model 1 | 0.43 (0.31–0.58) | <0.001 |
| Model 2 | 0.55 (0.40–0.74) | <0.001 | Model 2 | 0.43 (0.28–0.67) | <0.001 |
| Model 3 | 0.62 (0.45–0.85) | 0.003 | Model 3 | 0.61 (0.39–0.95) | 0.029 |
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | |
| ≤1.40 | 1.40–1.61 | 1.61–1.84 | >1.84 | ≤0.85 | 0.85–1.01 | 1.07–1.17 | >1.17 | |
| n | 2693 | 2675 | 2715 | 2654 | 5492 | 5752 | 5717 | 5628 |
| Unadjusted | 1.00 | 0.84 (0.69–1.02) | 0.64 (0.51–0.79) | 0.49 (0.39–0.63) | 1.00 | 0.82 (0.69–0.97) | 0.57 (0.48–0.69) | 0.41 (0.33–0.51) |
| Model 1 | 1.00 | 0.86 (0.71–1.05) | 0.67 (0.54–0.83) | 0.54 (0.42–0.69) | 1.00 | 0.91 (0.76–1.08) | 0.70 (0.58–0.84) | 0.56 (0.45–0.71) |
| Model 2 | 1.00 | 0.78 (0.61–1.01) | 0.68 (0.51–0.89) | 0.52 (0.38–0.72) | 1.00 | 0.95 (0.75–1.22) | 0.74 (0.57–0.97) | 0.56 (0.41–0.77) |
| Model 3 | 1.00 | 0.82 (0.63–1.06) | 0.72 (0.54–0.95) | 0.60 (0.43–0.84) | 1.00 | 1.03 (0.80–1.32) | 0.82 (0.63–1.08) | 0.72 (0.52–0.99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-B.; Jo, M.-K.; Moon, J.-E.; Lee, H.-J.; Kim, J.-K. Relationship between Handgrip Strength and Incident Diabetes in Korean Adults According to Gender: A Population-Based Prospective Cohort Study. J. Clin. Med. 2024, 13, 627. https://doi.org/10.3390/jcm13020627
Lee S-B, Jo M-K, Moon J-E, Lee H-J, Kim J-K. Relationship between Handgrip Strength and Incident Diabetes in Korean Adults According to Gender: A Population-Based Prospective Cohort Study. Journal of Clinical Medicine. 2024; 13(2):627. https://doi.org/10.3390/jcm13020627
Chicago/Turabian StyleLee, Sung-Bum, Min-Kyeung Jo, Ji-Eun Moon, Hui-Jeong Lee, and Jong-Koo Kim. 2024. "Relationship between Handgrip Strength and Incident Diabetes in Korean Adults According to Gender: A Population-Based Prospective Cohort Study" Journal of Clinical Medicine 13, no. 2: 627. https://doi.org/10.3390/jcm13020627
APA StyleLee, S.-B., Jo, M.-K., Moon, J.-E., Lee, H.-J., & Kim, J.-K. (2024). Relationship between Handgrip Strength and Incident Diabetes in Korean Adults According to Gender: A Population-Based Prospective Cohort Study. Journal of Clinical Medicine, 13(2), 627. https://doi.org/10.3390/jcm13020627