
Validation of a Wearable Medical Device for Automatic Diagnosis of OSA against Standard PSG


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Protocol
2.2. Eligibility Criteria
2.3. Reference Standard
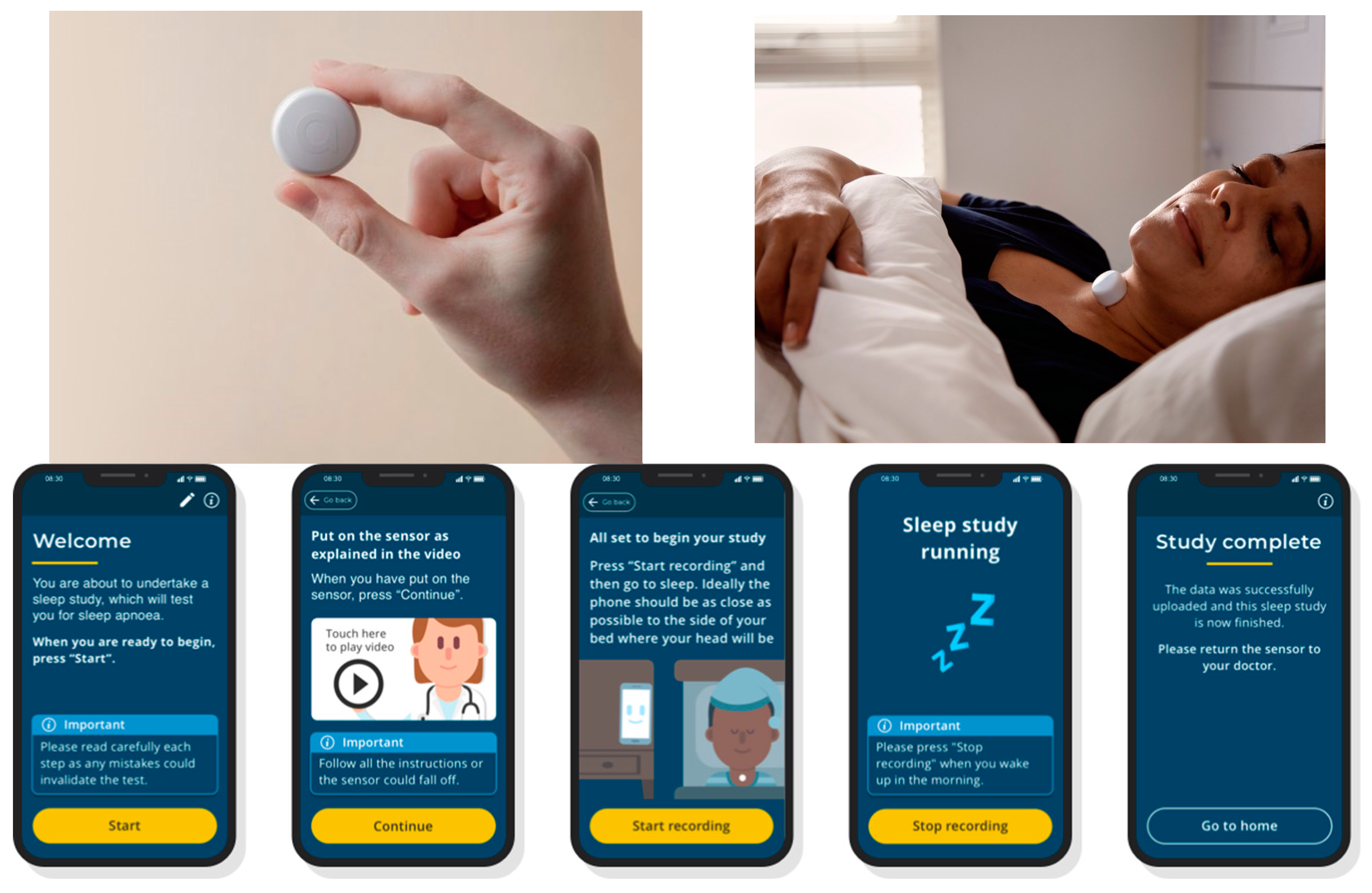
2.4. AcuPebble SA100
2.5. Data Analysis
- AHI criteria: Diagnosis based on AHI, marking apnea and hypopnea as defined by the current recommended AASM rules, i.e., for apnea, there is a drop in the peak signal excursion by ≥90% of pre-event baseline. For hypopnea, there is a drop in the peak signal excursion by ≥30% of the pre-event baseline, and there is a ≥3% oxygen desaturation from the pre-event baseline or the event is associated with an arousal. The duration of the drop in signal excursion is ≥10 s for both apnea and hypopnea.
- ODI criteria: Diagnosis based on ODI, marking desaturation events as a drop of ≥3% in the oxygen saturation value.
- A diagnostic output was classified as a True Positive (TP) when both AcuPebble SA100 and the gold standard concurred on diagnosing a patient with either moderate or severe sleep apnea, that is, when the threshold for the index in comparison is 15 events/h. This classification was chosen because moderate and severe OSAs are the diagnostic categories for which gold-standard treatment (continuous positive airway pressure (CPAP)) is recommended [20].
- A diagnostic output was labeled as a True Negative (TN) when both AcuPebble SA100 and the gold standard agreed that the patient did not have moderate or severe OSA.
- A diagnostic output from AcuPebble SA100 was deemed a False Negative (FN) if the gold standard diagnosed the patient with moderate or severe OSA, while the AcuPebble SA100 diagnosis indicated mild or normal.
- A diagnostic output from AcuPebble SA100 was identified as a False Positive (FP) if the gold standard diagnosed the patient with normal or mild sleep apnea, and the AcuPebble SA100 diagnosis suggested moderate or severe sleep apnea.
2.6. Sample Calculation
3. Results
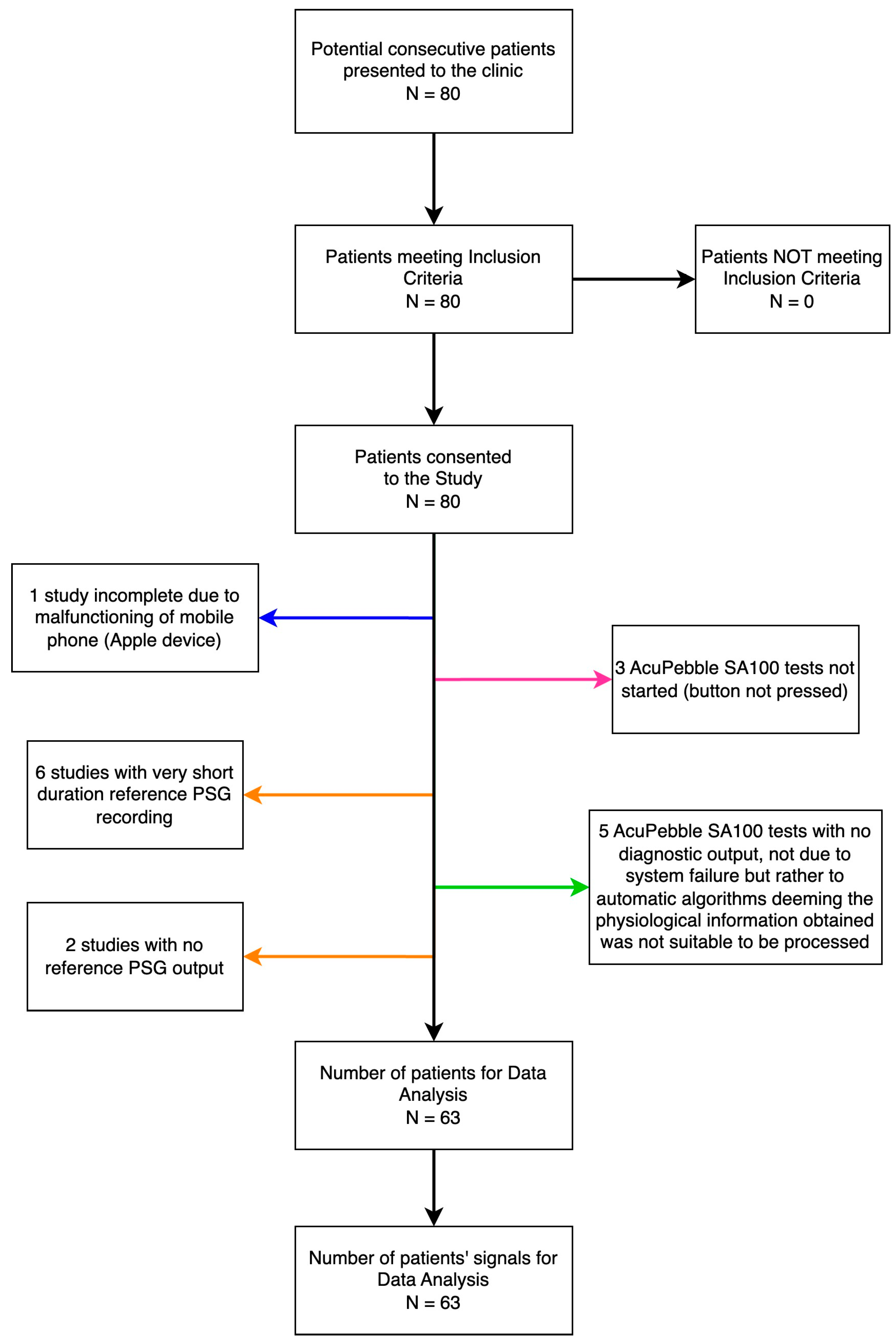
3.1. Participants
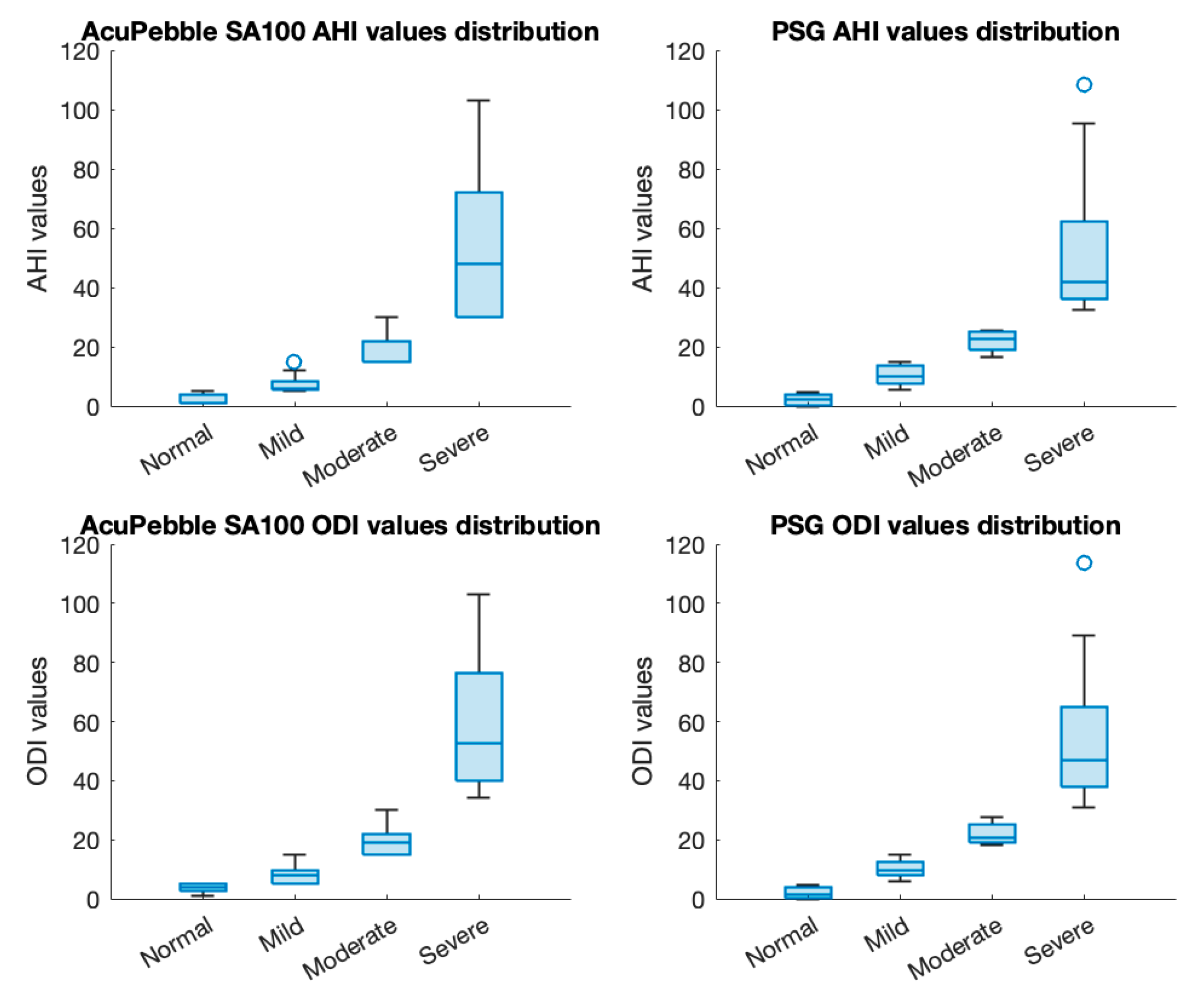
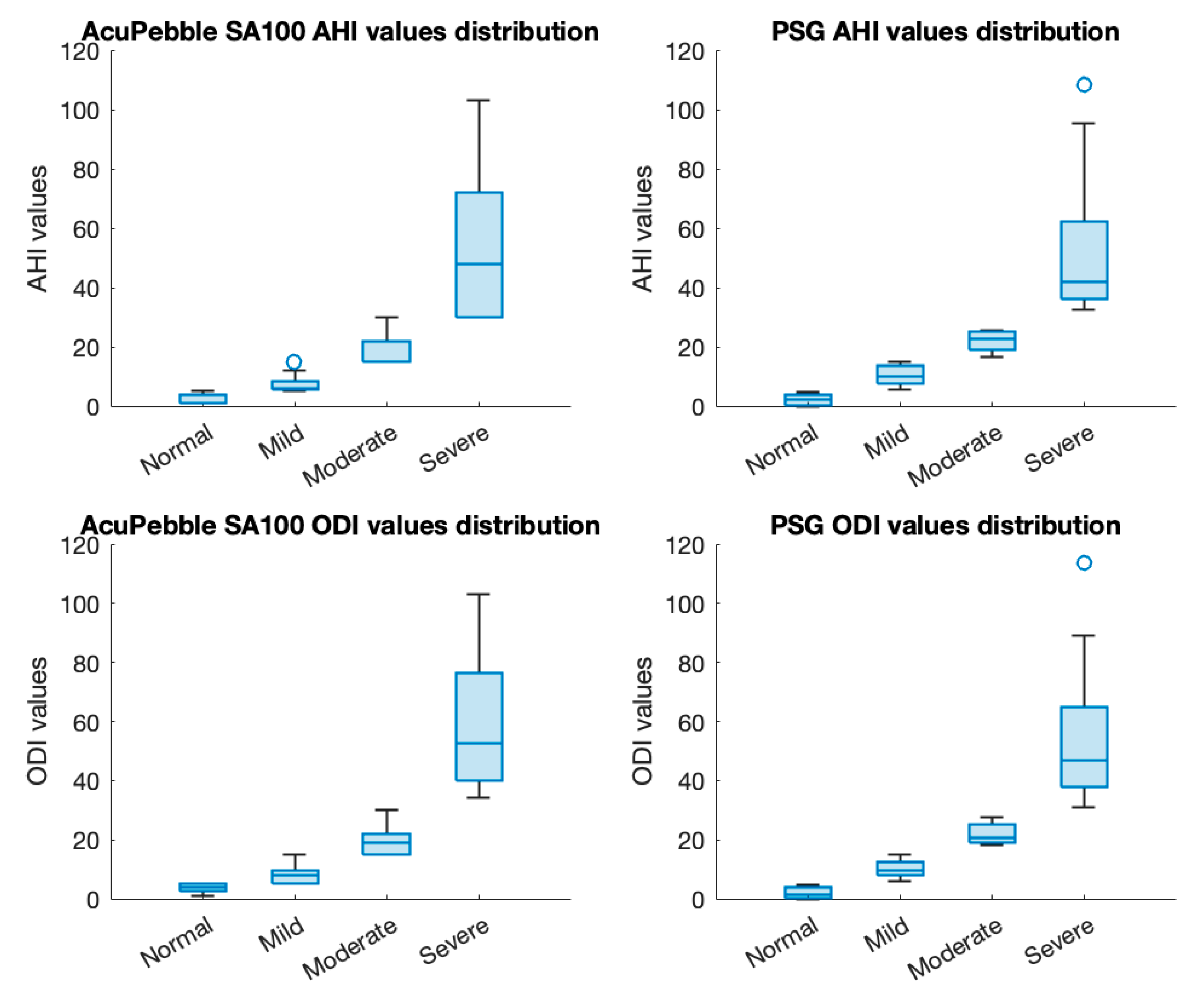
3.2. Diagnostic Accuracy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R.; Heinzer, R.; Ip, M.S.M.; Morrell, M.J.; Nunez, C.M.; Patel, S.R.; Penzel, T.; Pépin, J.L.; et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Maniaci, A.; Riela, P.M.; Iannella, G.; Lechien, J.R.; La Mantia, I.; De Vincentiis, M.; Cammaroto, G.; Calvo-Henriquez, C.; Di Luca, M.; Chiesa Estomba, C.; et al. Machine Learning Identification of Obstructive Sleep Apnea Severity through the Patient Clinical Features: A Retrospective Study. Life 2023, 13, 702. [Google Scholar] [CrossRef] [PubMed]
- Mulgrew, A.T.; Nasvadi, G.; Butt, A.; Cheema, R.; Fox, N.; Fleetham, J.A.; Ryan, C.F.; Cooper, P.; Ayas, N.T. Risk and severity of motor vehicle crashes in patients with obstructive sleep apnoea/hypopnoea. Thorax 2008, 63, 536–541. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, W.T.; Bonsigore, M.R.; Management Committee of EU COST ACTION B26. Sleep apnoea as an independent risk factor for cardiovascular disease: Current evidence, basic mechanisms and research priorities. Eur. Respir. J. 2007, 29, 156–178. [Google Scholar] [CrossRef] [PubMed]
- Daulatzai, M.A. Evidence of neurodegeneration in obstructive sleep apnea: Relationship between obstructive sleep apnea and cognitive dysfunction in the elderly. J. Neurosci. Res. 2015, 93, 1778–1794. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Culebras, A. Sleep apnoea and stroke. Stroke Vasc. Neurol. 2016, 1, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Van Ryswyk, E.; Mukherjee, S.; Chai-Coetzer, C.L.; Vakulin, A.; McEvoy, R.D. Sleep Disorders, Including Sleep Apnea and Hypertension. Am. J. Hypertens. 2018, 31, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Budhiraja, R.; Quan, S.F. Long-term All-Cause Mortality Risk in Obstructive Sleep Apnea Using Hypopneas Defined by a ≥ 3 Percent Oxygen Desaturation or Arousal. Southwest J. Pulm. Crit. Care 2021, 23, 23. [Google Scholar] [CrossRef] [PubMed]
- AASM. Hidden Health Crisis Costing America Billions—Underdiagnosing and Undertreating Obstructive Sleep Apnea Draining Healthcare System. Available online: https://aasm.org/resources/pdf/sleep-apnea-economic-crisis.pdf (accessed on 12 November 2023).
- Wickwire, E.M.; Albrecht, J.S.; Towe, M.M.; Abariga, S.A.; Diaz-Abad, M.; Shipper, A.G.; Cooper, L.M.; Assefa, S.Z.; Tom, S.E.; Scharf, S.M. The impact of treatments for OSA on monetized health economic outcomes: A systematic review. Chest 2019, 155, 947–961. [Google Scholar] [CrossRef] [PubMed]
- Fu, Y.; Xia, Y.; Yi, H.; Xu, H.; Guan, J.; Yin, S. Meta-analysis of all-cause and cardiovascular mortality in obstructive sleep apnea with or without continuous positive airway pressure treatment. Sleep Breath. 2017, 21, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Choo, B.P.; Mok, Y.; Oh, H.C.; Patanaik, A.; Kishan, K.; Awasthi, A.; Biju, S.; Bhattacharjee, S.; Poh, Y.; Wong, H.S. Benchmarking performance of an automatic polysomnography scoring system in a population with suspected sleep disorders. Front. Neurol. 2023, 14, 1123935. [Google Scholar] [CrossRef] [PubMed]
- Wickwire, E.M.; Zhang, X.; Munson, S.H.; Benjafield, A.V.; Sullivan, S.S.; Payombar, M.; Patil, S.P. The OSA patient journey: Pathways for diagnosis and treatment among commercially insured individuals in the United States. J. Clin. Sleep Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- Devani, N.; Pramono, R.X.A.; Imtiaz, S.A.; Bowyer, S.; Rodriguez-Villegas, E.; Mandal, S. Accuracy and usability of AcuPebble SA100 for automated diagnosis of obstructive sleep apnoea in the home environment setting: An evaluation study. BMJ Open 2021, 11, e046803. [Google Scholar] [CrossRef]
- ISO Standard No. 14155:2011; Clinical Investigation of Medical Devices for Human Subjects. International Organization for Standardization: Geneva, Switzerland, 2011. Available online: https://www.iso.org/standard/45557.html (accessed on 12 November 2023).
- BMJ Best Practice. Diagnostic Test Studies: Assessment and Critical Appraisal. Available online: https://bestpractice.bmj.com/info/toolkit/learn-ebm/diagnostic-test-studies-assessment-and-critical-appraisal/ (accessed on 12 November 2023).
- Balk, E.M.; Moorthy, D.; Obadan, N.O.; Patel, K.; Ip, S.; Chung, M.; Bannuru, R.R.; Kitsios, G.D.; Sen, S.; Iovin, R.C.; et al. Diagnosis and Treatment of Obstructive Sleep Apnea in Adults; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2011.
- Berry, R.B.; Brooks, R.; Gamaldo, C.; Harding, S.M.; Lloyd, R.M.; Quan, S.F.; Troester, M.T.; Vaughn, B.V. AASM Scoring Manual Updates for 2017 (Version 2.4). J. Clin. Sleep Med. 2017, 13, 665–666. [Google Scholar] [CrossRef]
- The Price of Fatigue: The Surprising Economic Costs of Unmanaged Sleep Apnea; Harvard Medical School Division of Sleep Medicine: Boston, MA, USA, 2010.
- Flemons, W.W.; Littner, M.R.; Rowley, J.A.; Gay, P.; Anderson, W.M.; Hudgel, D.W.; McEvoy, R.D.; Loube, D.I. Home diagnosis of sleep apnea: A systematic review of the literature. An evidence review cosponsored by the American Academy of Sleep Medicine, the American College of Chest Physicians, and the American Thoracic Society. Chest 2003, 124, 1543–1579. [Google Scholar] [CrossRef] [PubMed]
- University of Illinois Chicago. Diagnostic Test Calculator. Available online: http://araw.mede.uic.edu/cgi-bin/testcalc.pl (accessed on 12 November 2023).
- Van Pee, B.; Massie, F.; Vits, S.; Dreesen, P.; Klerkx, S.; Bijwadia, J.; Verbraecken, J.; Bergmann, J. A multicentric validation study of a novel home sleep apnea test based on peripheral arterial tonometry. Sleep 2022, 45, zsac028. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.L.; Ben Messaoud, R.; Joyeux-Faure, M.; Terrail, R.; Tamisier, R.; Martinot, J.B.; Le-Dong, N.N.; Morrell, M.J.; Pépin, J.L. Diagnosis of sleep apnoea using a mandibular monitor and machine learning analysis: One-night agreement compared to in-home polysomnography. Front. Neurosci. 2022, 16, 726880. [Google Scholar] [CrossRef]
- Pillar, G.; Berall, M.; Berry, R.; Etzioni, T.; Shrater, N.; Hwang, D.; Ibrahim, M.; Litman, E.; Manthena, P.; Koren-Morag, N.; et al. Detecting central sleep apnea in adult patients using WatchPAT—A multicenter validation study. Sleep Breath. 2020, 24, 387–398. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Age (years) | Median | 48 |
| Mean | 50 | |
| SD | 12 | |
| Range | (25, 78) | |
| BMI | Median | 28.7 |
| Mean | 30.7 | |
| SD | 7.0 | |
| Range | (16.7, 54.0) | |
| Number of patients per BMI classification | Underweight (<18.5) | 1 (1.59%) |
| Healthy weight (18.5–24.9) | 11 (17.46%) | |
| Overweight (25–29.9) | 25 (39.68%) | |
| Obese (30–39.9) Severely obese (>40) | 20 (31.75%) 6 (9.52%) | |
| Sex | Male | 40 |
| Female | 23 | |
| Epworth Scale | Median | 10 |
| Mean | 10.4 | |
| SD | 6.8 | |
| Range | (0, 24) | |
| Stop Bang Score | Median | 4 |
| Mean | 4.1 | |
| SD | 1.6 | |
| Range | (1, 8) | |
| Total Sleep Time (minutes) | Median | 456.7 |
| Mean | 453.6 | |
| SD | 42.0 | |
| Range | (307.2, 563.4) | |
| Sleep Efficiency | Median | 84.8% |
| Mean | 82.6% | |
| SD | 9.9% | |
| Range | (58.3%, 97.3%) | |
| Percentage of Sleep in REM | Median | 15.9% |
| Mean | 15.5% | |
| SD | 6.8% | |
| Range | (0%, 30%) |
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 92.86% | 76.50% to 99.12% |
| Specificity | 97.14% | 85.08% to 99.93% |
| Positive predictive value | 96.30% | 78.98% to 99.45% |
| Negative predictive value | 94.44% | 81.71% to 98.48% |
| Positive likelihood ratio | 32.50 | 4.70 to 224.92 |
| Negative likelihood ratio | 0.07 | 0.02 to 0.28 |
| Disease prevalence | 44.44% | - |
| Accuracy | 95.24% | 86.71% to 99.01% |
| Statistic | Value | 95% CI |
|---|---|---|
| Sensitivity | 92.00% | 73.97% to 99.02% |
| Specificity | 92.11% | 78.62% to 98.34% |
| Positive predictive value | 88.46% | 72.01% to 95.81% |
| Negative predictive value | 94.59% | 82.19% to 98.51% |
| Positive likelihood ratio | 11.65 | 3.91 to 34.73 |
| Negative likelihood ratio | 0.09 | 0.02 to 0.33 |
| Disease prevalence | 39.68% | - |
| Accuracy | 92.06% | 82.44% to 97.37% |
| AcuP. vs. PSG in Clinic | AcuP. vs. CR-PG at Home | Combined Diagnostic Performance | |||||
|---|---|---|---|---|---|---|---|
| CI | CI | CI | |||||
| AHI based validation | Sensitivity (%) | 92.86 | 76.50 to 99.12 | 92.59 | 82.11 to 97.94 | 93.83 | 86.18 to 97.97 |
| Specificity (%) | 97.14 | 85.08 to 99.93 | 96.88 | 91.14 to 99.35 | 96.21 | 91.38 to 98.76 | |
| Positive Likelihood Ratio | 32.50 | 4.70 to 224.92 | 29.63 | 9.70 to 90.48 | 24.77 | 10.47 to 58.63 | |
| Negative Likelihood Ratio | 0.07 | 0.02 to 0.28 | 0.08 | 0.03 to 0.20 | 0.06 | 0.03 to 0.15 | |
| Disease prevalence (%) | 44.44 | 31.92 to 57.51 | 36.00 | 28.33 to 44.23 | 38.03 | 31.48 to 44.91 | |
| PPV (%) | 96.30 | 78.98 to 99.45 | 94.34 | 84.52 to 98.07 | 93.83 | 86.53 to 97.30 | |
| NPV (%) | 94.44 | 81.71 to 98.48 | 95.88 | 90.05 to 98.35 | 96.21 | 91.57 to 98.34 | |
| Accuracy (%) | 95.24 | 86.71 to 99.01 | 95.33 | 90.62 to 98.10 | 95.31 | 91.54 to 97.73 | |
| ODI based validation | Sensitivity (%) | 92.00 | 73.97 to 99.02 | 91.03 | 82.38 to 96.32 | 90.38 | 83.03 to 95.29 |
| Specificity (%) | 92.11 | 78.62 to 98.34 | 93.06 | 84.53 to 97.71 | 93.58 | 87.22 to 97.38 | |
| Positive Likelihood Ratio | 11.65 | 3.91 to 34.73 | 13.11 | 5.61 to 30.62 | 14.07 | 6.85 to 28.90 | |
| Negative Likelihood Ratio | 0.09 | 0.02 to 0.33 | 0.10 | 0.05 to 0.20 | 0.10 | 0.06 to 0.19 | |
| Disease prevalence (%) | 39.68 | 27.57 to 52.80 | 52.00 | 43.70 to 60.22 | 48.83 | 41.94 to 55.75 | |
| PPV (%) | 88.46 | 72.01 to 95.81 | 93.42 | 85.87 to 97.07 | 93.07 | 86.74 to 96.50 | |
| NPV (%) | 94.59 | 82.19 to 98.51 | 90.54 | 82.48 to 95.11 | 91.07 | 84.96 to 94.85 | |
| Accuracy (%) | 92.06 | 82.44 to 97.37 | 92.00 | 86.44 to 95.80 | 92.02 | 87.53 to 95.28 | |
| Device | Subjects Count | Index Test | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | Accuracy % (95% CI) | Tested at Intended Environment | |
|---|---|---|---|---|---|---|---|---|---|
| This study | AcuPebble SA100 | 213 | AHI ≥ 15 vs. AHI ≥ 15 | 93.83 (86.18–97.97) | 96.21 (91.38–98.76) | 93.83 (86.53–97.30) | 96.21 (91.57–98.34) | 95.31 (91.54–97.73) | Yes |
| 213 | ODI ≥ 15 vs. ODI ≥ 15 | 90.38 (83.03–95.29) | 93.58 (87.22–97.38) | 93.07 (86.74–96.50) | 91.07 (84.96–94.85) | 92.02 (87.53–95.28) | |||
| Van Pee (2022) [23] | NightOwl | 228 | PAT-AHI ≥ 15 vs. PSG-AHI ≥ 15 | 91 (85–96) | 76 (65–87) | 82 (72–92) | 88 (81–94) | 86 (80–91) | No |
| Kelly (2022) [24] | Sunrise | 31 | MM-ORDI > 12.65 vs. PSG ORDI > 15 | 100 (79–100) | 75 (45–92) | 80 | 100 | 88 | No |
| Pillar (2020) [25] | WatchPAT 200U | 84 | WP-AHI ≥ 15 vs. PSG AHI ≥ 15 | 85.1 | 70.3 | 79.4 | 78.8 | 86 | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez Gomez, J.; Pramono, R.X.A.; Imtiaz, S.A.; Rodriguez-Villegas, E.; Valido Morales, A. Validation of a Wearable Medical Device for Automatic Diagnosis of OSA against Standard PSG. J. Clin. Med. 2024, 13, 571. https://doi.org/10.3390/jcm13020571
Sanchez Gomez J, Pramono RXA, Imtiaz SA, Rodriguez-Villegas E, Valido Morales A. Validation of a Wearable Medical Device for Automatic Diagnosis of OSA against Standard PSG. Journal of Clinical Medicine. 2024; 13(2):571. https://doi.org/10.3390/jcm13020571
Chicago/Turabian StyleSanchez Gomez, Jesus, Renard Xaviero Adhi Pramono, Syed Anas Imtiaz, Esther Rodriguez-Villegas, and Agustin Valido Morales. 2024. "Validation of a Wearable Medical Device for Automatic Diagnosis of OSA against Standard PSG" Journal of Clinical Medicine 13, no. 2: 571. https://doi.org/10.3390/jcm13020571
APA StyleSanchez Gomez, J., Pramono, R. X. A., Imtiaz, S. A., Rodriguez-Villegas, E., & Valido Morales, A. (2024). Validation of a Wearable Medical Device for Automatic Diagnosis of OSA against Standard PSG. Journal of Clinical Medicine, 13(2), 571. https://doi.org/10.3390/jcm13020571