
Is the Ventilatory Efficiency in Endurance Athletes Different?—Findings from the NOODLE Study

 , , ,
, , ,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. CPET Protocol
2.3. Study Endpoints
2.4. Sample Characteristics
2.5. Selection of Prediction Models for Validation
2.6. Statistical Analysis
3. Results
3.1. Interdependency of VE/VCO2 Measurements
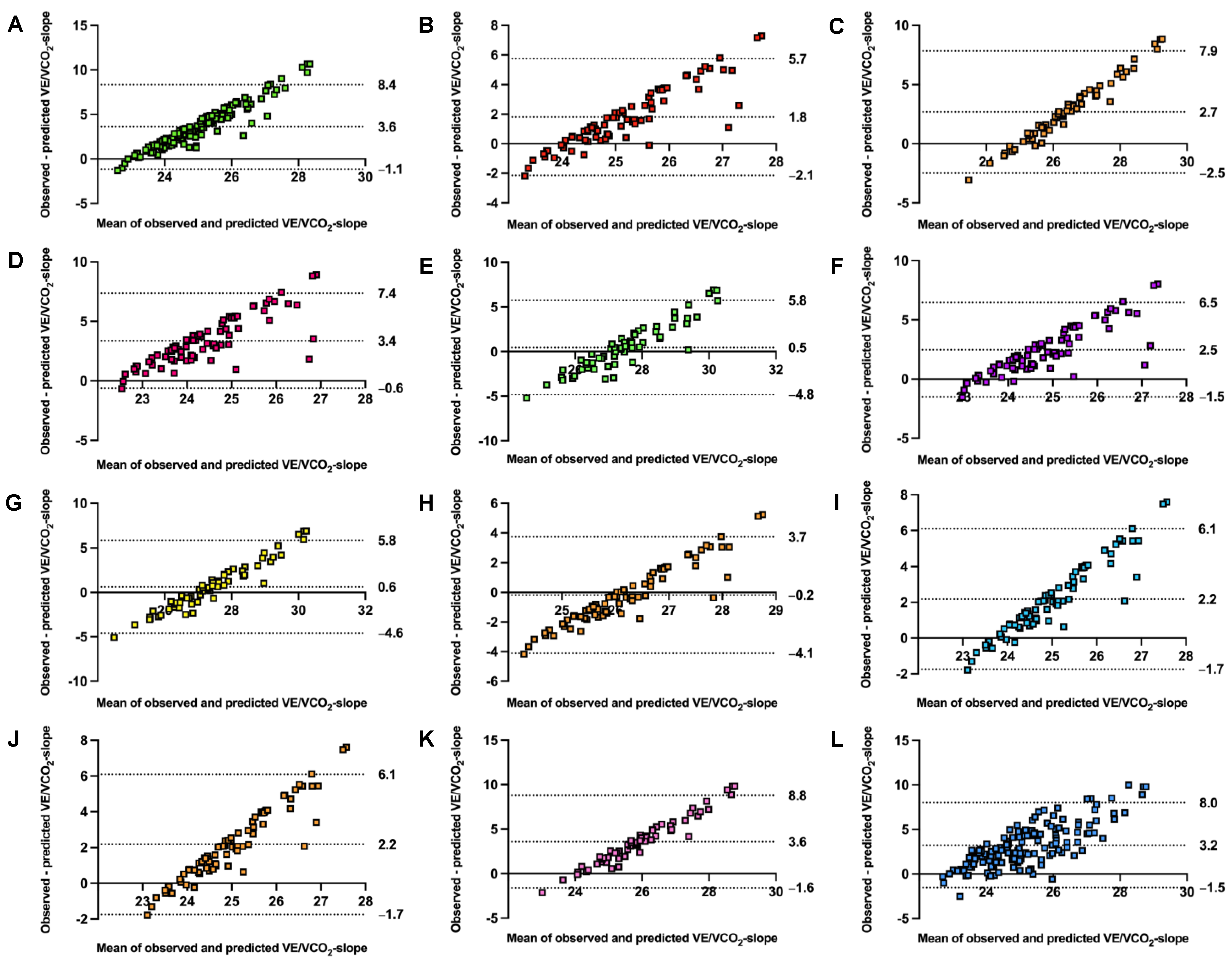
3.2. Validity of VE/VCO2-Slope Predictions
4. Discussion
4.1. Practical and Clinical Implications
4.2. Limitations and Interpretation
4.3. Further Research Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arena, R.; Myers, J.; Hsu, L.; Peberdy, M.A.; Pinkstaff, S.; Bensimhon, D.; Chase, P.; Vicenzi, M.; Guazzi, M. The minute ventilation/carbon dioxide production slope is prognostically superior to the oxygen uptake efficiency slope. J. Card. Fail. 2007, 13, 462–469. [Google Scholar] [CrossRef]
- Phillips, D.B.; Collins, S.E.; Stickland, M.K. Measurement and Interpretation of Exercise Ventilatory Efficiency. Front. Physiol. 2020, 11, 659. [Google Scholar] [CrossRef]
- Petek, B.J.; Churchill, T.W.; Gustus, S.K.; Schoenike, M.W.; Nayor, M.; Moulson, N.; Guseh, J.S.; VanAtta, C.; Blodgett, J.B.; Contursi, M.; et al. Characterization of ventilatory efficiency during cardiopulmonary exercise testing in healthy athletes. Eur. J. Prev. Cardiol. 2023, 30, e21–e24. [Google Scholar] [CrossRef]
- Myers, J.; Arena, R.; Oliveira, R.B.; Bensimhon, D.; Hsu, L.; Chase, P.; Guazzi, M.; Brubaker, P.; Moore, B.; Kitzman, D.; et al. The lowest VE/VCO2 ratio during exercise as a predictor of outcomes in patients with heart failure. J. Card. Fail. 2009, 15, 756–762. [Google Scholar] [CrossRef]
- Kim, J.H.; Baggish, A.L. Strenuous Exercise and Cardiovascular Disease Outcomes. Curr. Atheroscler. Rep. 2017, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Noonan, V.; Dean, E. Submaximal Exercise Testing: Clinical Application and Interpretation. Phys. Ther. 2000, 80, 782–807. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.; Bakken, K.; D’Elia, E.; Lewis, G.D. Cardiopulmonary Exercise Testing in Heart Failure. JACC Heart Fail. 2016, 4, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Salvioni, E.; Corra, U.; Piepoli, M.; Rovai, S.; Correale, M.; Paolillo, S.; Pasquali, M.; Magri, D.; Vitale, G.; Fusini, L.; et al. Gender and age normalization and ventilation efficiency during exercise in heart failure with reduced ejection fraction. ESC Heart Fail. 2020, 7, 371–380. [Google Scholar] [CrossRef]
- Ponikowski, P.; Francis, D.P.; Piepoli, M.F.; Davies, L.C.; Chua, T.P.; Davos, C.H.; Florea, V.; Banasiak, W.; Poole-Wilson, P.A.; Coats, A.J.; et al. Enhanced ventilatory response to exercise in patients with chronic heart failure and preserved exercise tolerance: Marker of abnormal cardiorespiratory reflex control and predictor of poor prognosis. Circulation 2001, 103, 967–972. [Google Scholar] [CrossRef]
- Sun, X.G.; Hansen, J.E.; Garatachea, N.; Storer, T.W.; Wasserman, K. Ventilatory efficiency during exercise in healthy subjects. Am. J. Respir. Crit. Care Med. 2002, 166, 1443–1448. [Google Scholar] [CrossRef]
- Guazzi, M.; Arena, R.; Halle, M.; Piepoli, M.F.; Myers, J.; Lavie, C.J. 2016 Focused Update: Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2016, 133, e694–e711. [Google Scholar] [CrossRef] [PubMed]
- Guazzi, M.; Adams, V.; Conraads, V.; Halle, M.; Mezzani, A.; Vanhees, L.; Arena, R.; Fletcher, G.F.; Forman, D.E.; Kitzman, D.W.; et al. Clinical Recommendations for Cardiopulmonary Exercise Testing Data Assessment in Specific Patient Populations. Circulation 2012, 126, 2261–2274. [Google Scholar] [CrossRef] [PubMed]
- Petek, B.J.; Tso, J.V.; Churchill, T.W.; Guseh, J.S.; Loomer, G.; DiCarli, M.; Lewis, G.D.; Weiner, R.B.; Kim, J.H.; Wasfy, M.M.; et al. Normative cardiopulmonary exercise data for endurance athletes: The Cardiopulmonary Health and Endurance Exercise Registry (CHEER). Eur. J. Prev. Cardiol. 2021, 29, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Kasiak, P.S.; Wiecha, S.; Cieslinski, I.; Takken, T.; Lach, J.; Lewandowski, M.; Barylski, M.; Mamcarz, A.; Sliz, D. Validity of the Maximal Heart Rate Prediction Models among Runners and Cyclists. J. Clin. Med. 2023, 12, 2884. [Google Scholar] [CrossRef]
- Sun, X.G.; Hansen, J.E.; Stringer, W.W. Oxygen uptake efficiency plateau: Physiology and reference values. Eur. J. Appl. Physiol. 2012, 112, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Myers, J.; Aslam, S.S.; Varughese, E.B.; Peberdy, M.A. Technical considerations related to the minute ventilation/carbon dioxide output slope in patients with heart failure. Chest 2003, 124, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Kleber, F.X.; Vietzke, G.; Wernecke, K.D.; Bauer, U.; Opitz, C.; Wensel, R.; Sperfeld, A.; Glaser, S. Impairment of ventilatory efficiency in heart failure: Prognostic impact. Circulation 2000, 101, 2803–2809. [Google Scholar] [CrossRef]
- Neder, J.A.; Nery, L.E.; Peres, C.; Whipp, B.J. Reference values for dynamic responses to incremental cycle ergometry in males and females aged 20 to 80. Am. J. Respir. Crit. Care Med. 2001, 164, 1481–1486. [Google Scholar] [CrossRef]
- Ashikaga, K.; Itoh, H.; Maeda, T.; Itoh, H.; Ichikawa, Y.; Tanaka, S.; Ajisaka, R.; Koike, A.; Makita, S.; Omiya, K.; et al. Ventilatory efficiency during ramp exercise in relation to age and sex in a healthy Japanese population. J. Cardiol. 2021, 77, 57–64. [Google Scholar] [CrossRef]
- Loe, H.; Steinshamn, S.; Wisloff, U. Cardio-respiratory reference data in 4631 healthy men and women 20-90 years: The HUNT 3 fitness study. PLoS ONE 2014, 9, e113884. [Google Scholar] [CrossRef]
- Wiecha, S.; Kasiak, P.S.; Cieslinski, I.; Takken, T.; Palka, T.; Knechtle, B.; Nikolaidis, P.; Malek, L.A.; Postula, M.; Mamcarz, A.; et al. External validation of VO2max prediction models based on recreational and elite endurance athletes. PLoS ONE 2023, 18, e0280897. [Google Scholar] [CrossRef]
- Brown, S.J.; Raman, A.; Schlader, Z.; Stannard, S.R. Ventilatory efficiency in juvenile elite cyclists. J. Sci. Med. Sport. 2013, 16, 266–270. [Google Scholar] [CrossRef]
- Salazar-Martinez, E.; de Matos, T.R.; Arrans, P.; Santalla, A.; Orellana, J.N. Ventilatory efficiency response is unaffected by fitness level, ergometer type, age or body mass index in male athletes. Biol. Sport. 2018, 35, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Salazar-Martinez, E.; Terrados, N.; Burtscher, M.; Santalla, A.; Naranjo Orellana, J. Ventilatory efficiency and breathing pattern in world-class cyclists: A three-year observational study. Respir. Physiol. Neurobiol. 2016, 229, 17–23. [Google Scholar] [CrossRef]
- Arena, R.; Myers, J.; Harber, M.; Phillips, S.A.; Severin, R.; Ozemek, C.; Peterman, J.E.; Kaminsky, L.A. The V E/V CO2 Slope during Maximal Treadmill Cardiopulmonary Exercise Testing: Reference standards from friend (fitness registry and the importance of exercise: A national database). J. Cardiopulm. Rehabil. Prev. 2021, 41, 194–198. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Moulson, N.; Gustus, S.K.; Scirica, C.; Petek, B.J.; Vanatta, C.; Churchill, T.W.; Guseh, J.S.; Baggish, A.; Wasfy, M.M. Diagnostic evaluation and cardiopulmonary exercise test findings in young athletes with persistent symptoms following COVID-19. Br. J. Sports Med. 2022, 56, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Paap, D.; Takken, T. Reference values for cardiopulmonary exercise testing in healthy adults: A systematic review. Expert. Rev. Cardiovasc. Ther. 2014, 12, 1439–1453. [Google Scholar] [CrossRef]
- Takken, T.; Mylius, C.F.; Paap, D.; Broeders, W.; Hulzebos, H.J.; Van Brussel, M.; Bongers, B.C. Reference values for cardiopulmonary exercise testing in healthy subjects—An updated systematic review. Expert. Rev. Cardiovasc. Ther. 2019, 17, 413–426. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Shrout, P.E.; Fleiss, J.L. Intraclass correlations: Uses in assessing rater reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Petek, B.J.; Gustus, S.K.; Wasfy, M.M. Cardiopulmonary Exercise Testing in Athletes: Expect the Unexpected. Curr. Treat. Options Cardiovasc. Med. 2021, 23, 49. [Google Scholar] [CrossRef]
- Klaassen, S.H.C.; Liu, L.C.Y.; Hummel, Y.M.; Damman, K.; van der Meer, P.; Voors, A.A.; Hoendermis, E.S.; van Veldhuisen, D.J. Clinical and Hemodynamic Correlates and Prognostic Value of VE/VCO(2) Slope in Patients with Heart Failure with Preserved Ejection Fraction and Pulmonary Hypertension. J. Card. Fail. 2017, 23, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.P.; Gardner, R.M.; Adams, T.D.; Yanowitz, F.G.; Crapo, R.O. “Anaerobic threshold”: Problems of determination and validation. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 55, 1178–1186. [Google Scholar] [CrossRef]
- Ceaser, T.G.; Fitzhugh, E.C.; Thompson, D.L.; Bassett, D.R. Association of Physical Activity, Fitness, and Race: NHANES 1999–2004. Med. Sci. Sports Exerc. 2013, 45, 286–293. [Google Scholar] [CrossRef]
- Lucia, A.; Hoyos, J.; Perez, M.; Chicharro, J.L. Heart rate and performance parameters in elite cyclists: A longitudinal study. Med. Sci. Sports Exerc. 2000, 32, 1777–1782. [Google Scholar] [CrossRef]
- Price, S.; Wiecha, S.; Cieśliński, I.; Śliż, D.; Kasiak, P.S.; Lach, J.; Gruba, G.; Kowalski, T.; Mamcarz, A. Differences between Treadmill and Cycle Ergometer Cardiopulmonary Exercise Testing Results in Triathletes and Their Association with Body Composition and Body Mass Index. Int. J. Environ. Res. Public Health 2022, 19, 3557. [Google Scholar] [CrossRef]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular Effects and Benefits of Exercise. Front. Cardiovasc. Med. 2018, 5, 135. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 140) | Sex | ||
|---|---|---|---|---|
| Females (n = 63) | Males (n = 77) | |||
| Age (years) | 22.7 ± 4.6 | 23.8 ± 4.2 | 21.8 ± 4.8 | |
| Height (cm) | 174.8 ± 9.9 | 166.3 ± 6.2 | 181.6 ± 6.3 | |
| Weight (kg) | 69.3 ± 10.1 | 61.0 ± 5.5 | 76.1 ± 7.6 | |
| BMI (kg·m−2) | 22.6 ± 1.7 | 22.1 ± 1.6 | 23.1 ± 1.7 | |
| Primary sport | Speedskating | 59 (42.1) | 26 (41.3) | 33 (42.9) |
| Triathlon or cycling | 56 (40.0) | 30 (47.6) | 26 (33.8) | |
| Other | 25 (17.9) | 7 (11.1) | 18 (23.3) | |
| HR (beats·min−1) | 190.9 ± 8.9 | 191.0 ± 9.1 | 190.8 ± 8.7 | |
| VE (L·min−1) | 154.5 ± 34.1 | 127.8 ± 21.1 | 176.3 ± 26.3 | |
| VO2peak (L·min−1) | 3.86 ± 0.82 | 3.21 ± 0.48 | 4.40 ± 0.64 | |
| VCO2 (L·min−1) | 4.36 ± 0.96 | 3.57 ± 0.52 | 5.00 ± 0.73 | |
| VO2peak (mL·kg−1·min−1) | 55.2 ± 8.6 | 52.1 ± 7.0 | 57.8 ± 9.0 | |
| RR (breaths·min−1) | 60.0 ± 7.6 | 60.2 ± 6.7 | 59.9 ± 8.3 | |
| VT (L) | 2.81 ± 0.64 | 2.30 ± 0.32 | 3.22 ± 0.53 | |
| RER (VO2/VCO2) | 1.14 ± 0.05 | 1.13 ± 0.05 | 1.15 ± 0.05 | |
| VE/VCO2-slope | 26.8 ± 2.4 | 27.7 ± 2.6 | 26.1 ± 2.0 | |
| VE/VCO2-Nadir | 25.2 ± 2.3 | 26.2 ± 2.4 | 24.5 ± 2.0 | |
| VE/VCO2-Total | 28.0 ± 2.5 | 28.7 ± 2.7 | 27.3 ± 2.2 | |
| O2P (VO2/HR) | 20.7 ± 4.4 | 17.3 ± 3.0 | 23.5 ± 3.3 | |
| Testing duration (minutes) | 21.3 ± 2.6 | 21.1 ± 2.7 | 21.4 ± 2.6 | |
| Workload (watts) | 320.4 ± 76.2 | 266.7 ± 40.8 | 364.4 ± 70.0 | |
| Reference | Model | Testing Protocol | Sample Size (Total/Males/Females) | Age (Years) | |
|---|---|---|---|---|---|
| Males | Females | ||||
| Salvioni et al. [8] | 20.227 + 0.095 · age | 23.808 + 0.052 · age |
| 1136/773/363 | 13–83 |
| 21.413 + 0.08 · age | |||||
| Kleber et al. [17] | 19.9 + 0.13 · age | 24.4 + 0.12 · age | Running CPET; modified Naughton protocol with increases in gradient and speed of 1 MET every 2 min. | 101/45/56 | 16–75 |
| Neder et al. [18] | 21 + 0.12 · age | 25.2 + 0.08 · age | Cycling CPET; ramp protocol with increases in power of 10–25 W·min−1 in females and 15–30 W·min−1 in males. | 120/60/60 | 20–80 |
| Loe et al. [20] | 23.897 + 0.072 · age + 0.826 | 25.549 + 0.072 · age | Running CPET; ramp protocol with increase in speed of 1 km·h−1 or gradient of 2% every 2–3 min. | 4631/2261/2370 | 20–90 |
| Ashikaga et al. [19] | 22.4 + 0.07 · age | 22.467 + 0.07 · age | Cycling CPET; ramp protocol with increases in power of 10 W·min−1 or 20 W·min−1. | 529/274/255 | 20–78 |
| Sun et al. [10] | 34.38 + 0.082 · age − 0.0723 · height | Running or cycling CPET; incremental maximal protocols with varying duration. | 474/310/164 | 37–74 | |
| Prediction Equation | Predicted VE/VCO2-Slope | Difference | RMSE (%RMSE) | MAPE | p-Value | ICC3,1 (95% CI) | R2 |
|---|---|---|---|---|---|---|---|
| Salvioni et al. (general model) [8] | 23.2 ± 0.4 | −3.6 ± 2.4 | 4.3 (16.2) | 13.0 | <0.001 | 0.028 (0.002, 0.053) | 0.009 |
| Salvioni et al. (males) [8] | 24.3 ± 0.4 | −1.8 ± 2.0 | 2.7 (10.3) | 7.5 | <0.001 | 0.043 (0.017, 0.069) | 0.010 |
| Salvioni et al. (females) [8] | 25.1 ± 0.2 | −2.7 ± 2.6 | 3.8 (13.5) | 10.1 | <0.001 | <0.001 (−0.026, 0.026) | 0.004 |
| Kleber et al. (males) [17] | 22.7 ± 0.6 | −3.4 ± 2.0 | 3.9 (15.1) | 12.5 | <0.001 | 0.056 (0.031, 0.082) | 0.010 |
| Kleber et al. (females) [17] | 27.3 ± 0.5 | −0.5 ± 2.7 | 2.7 (9.8) | 7.5 | 0.44 | <0.001 (−0.026, 0.026) | 0.004 |
| Neder et al. (males) [18] | 23.6 ± 0.6 | −2.5 ± 2.0 | 3.2 (12.3) | 9.4 | <0.001 | 0.052 (0.027, 0.078) | 0.010 |
| Neder et al. (females) [18] | 27.1 ± 0.3 | −0.6 ± 2.6 | 2.7 (9.8) | 7.5 | 0.20 | <0.001 (−0.026, 0.026) | 0.004 |
| Loe et al. (males) [20] | 26.3 ± 0.3 | +0.2 ± 2.0 | 2.0 (7.6) | 6.3 | 0.03 | 0.036 (0.010, 0.062) | 0.010 |
| Loe et al. (females) [20] | 27.3 ± 0.3 | −0.5 ± 2.6 | 2.7 (9.6) | 7.4 | 0.33 | <0.001 (−0.026, 0.026) | 0.004 |
| Ashikaga et al. (males) [19] | 23.9 ± 0.3 | −2.2 ± 2.0 | 2.9 (11.3) | 8.5 | <0.001 | 0.033 (0.007, 0.059) | 0.010 |
| Ashikaga et al. (females) [19] | 24.1 ± 0.3 | −3.6 ± 2.6 | 4.5 (16.1) | 12.6 | <0.001 | <0.001 (−0.026, 0.026) | 0.003 |
| Sun et al. (general model) [10] | 23.6 ± 0.9 | −3.2 ± 2.4 | 4.0 (15.1) | 11.7 | <0.001 | 0.112 (0.087, 0.138) | 0.031 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasiak, P.; Kowalski, T.; Rębiś, K.; Klusiewicz, A.; Ładyga, M.; Sadowska, D.; Wilk, A.; Wiecha, S.; Barylski, M.; Poliwczak, A.R.; et al. Is the Ventilatory Efficiency in Endurance Athletes Different?—Findings from the NOODLE Study. J. Clin. Med. 2024, 13, 490. https://doi.org/10.3390/jcm13020490
Kasiak P, Kowalski T, Rębiś K, Klusiewicz A, Ładyga M, Sadowska D, Wilk A, Wiecha S, Barylski M, Poliwczak AR, et al. Is the Ventilatory Efficiency in Endurance Athletes Different?—Findings from the NOODLE Study. Journal of Clinical Medicine. 2024; 13(2):490. https://doi.org/10.3390/jcm13020490
Chicago/Turabian StyleKasiak, Przemysław, Tomasz Kowalski, Kinga Rębiś, Andrzej Klusiewicz, Maria Ładyga, Dorota Sadowska, Adrian Wilk, Szczepan Wiecha, Marcin Barylski, Adam Rafał Poliwczak, and et al. 2024. "Is the Ventilatory Efficiency in Endurance Athletes Different?—Findings from the NOODLE Study" Journal of Clinical Medicine 13, no. 2: 490. https://doi.org/10.3390/jcm13020490
APA StyleKasiak, P., Kowalski, T., Rębiś, K., Klusiewicz, A., Ładyga, M., Sadowska, D., Wilk, A., Wiecha, S., Barylski, M., Poliwczak, A. R., Wierzbiński, P., Mamcarz, A., & Śliż, D. (2024). Is the Ventilatory Efficiency in Endurance Athletes Different?—Findings from the NOODLE Study. Journal of Clinical Medicine, 13(2), 490. https://doi.org/10.3390/jcm13020490