
A Comparative Study of 1-Year Postprocedural Outcomes in Transcatheter Mitral Valve Repair in Advanced Primary Mitral Regurgitation: PASCAL vs. MitraClip

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Echocardiographic Assessment
2.3. Statistical Analysis
3. Results
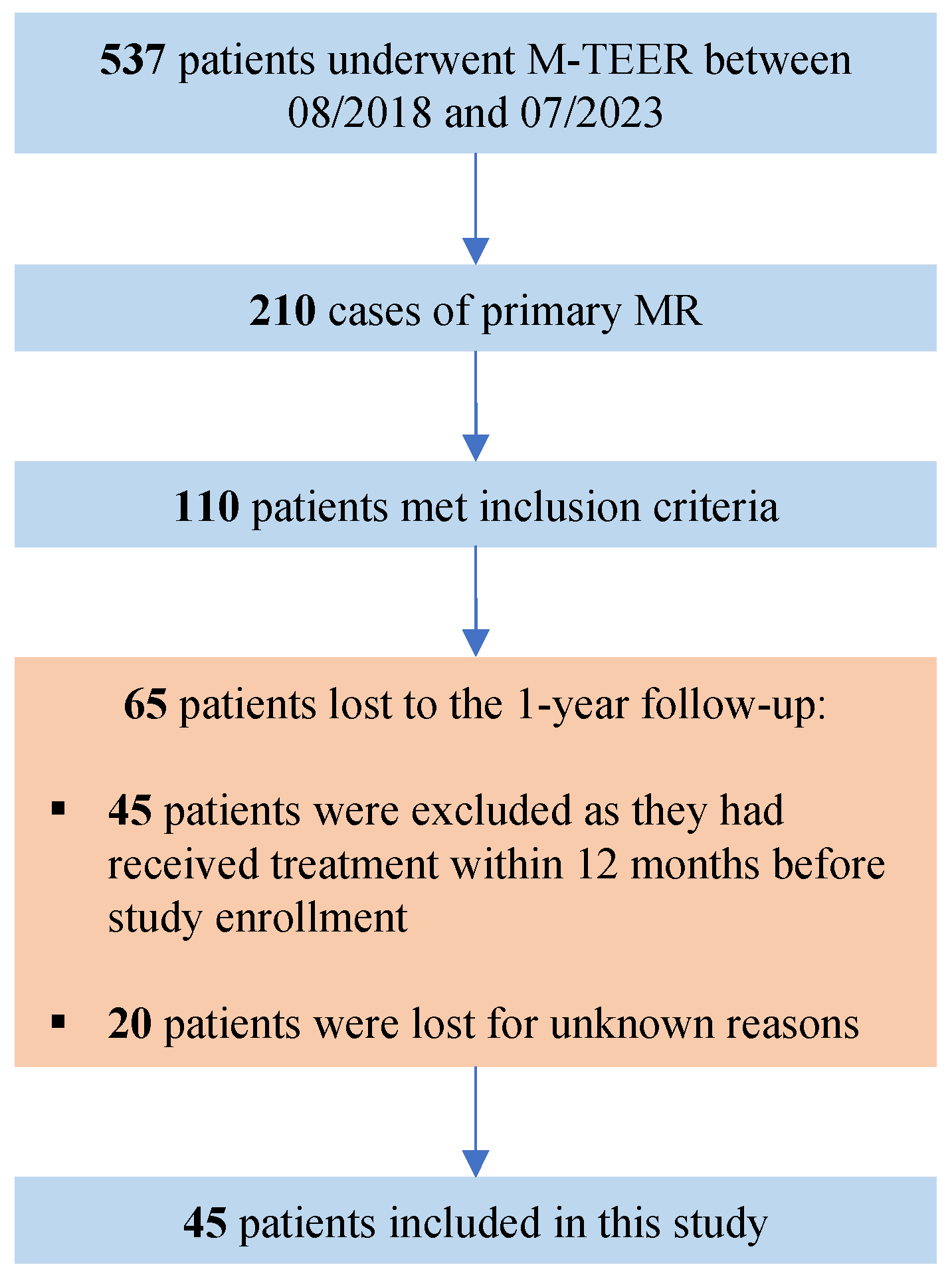
3.1. Study Population
3.2. Periprocedural Data
3.3. Baseline Echocardiography
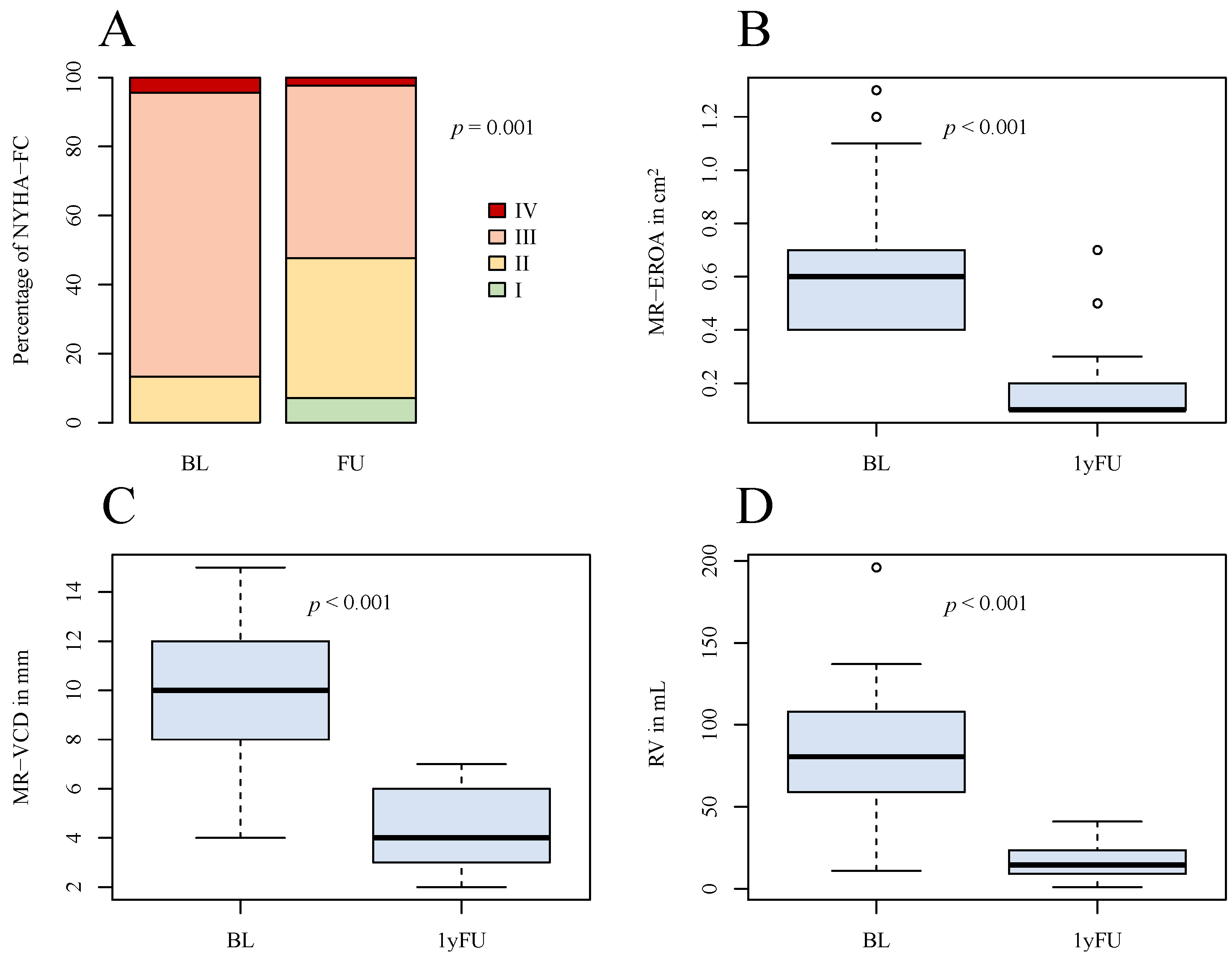
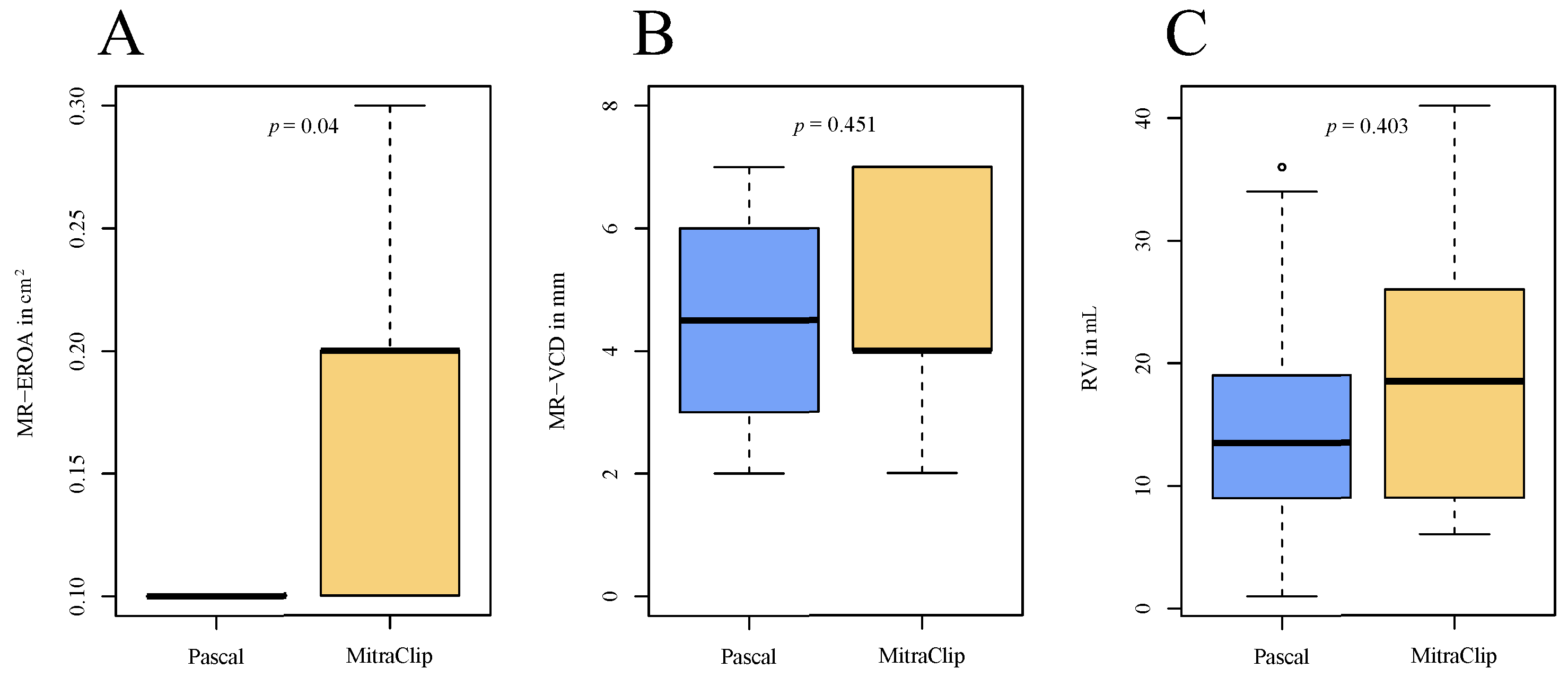
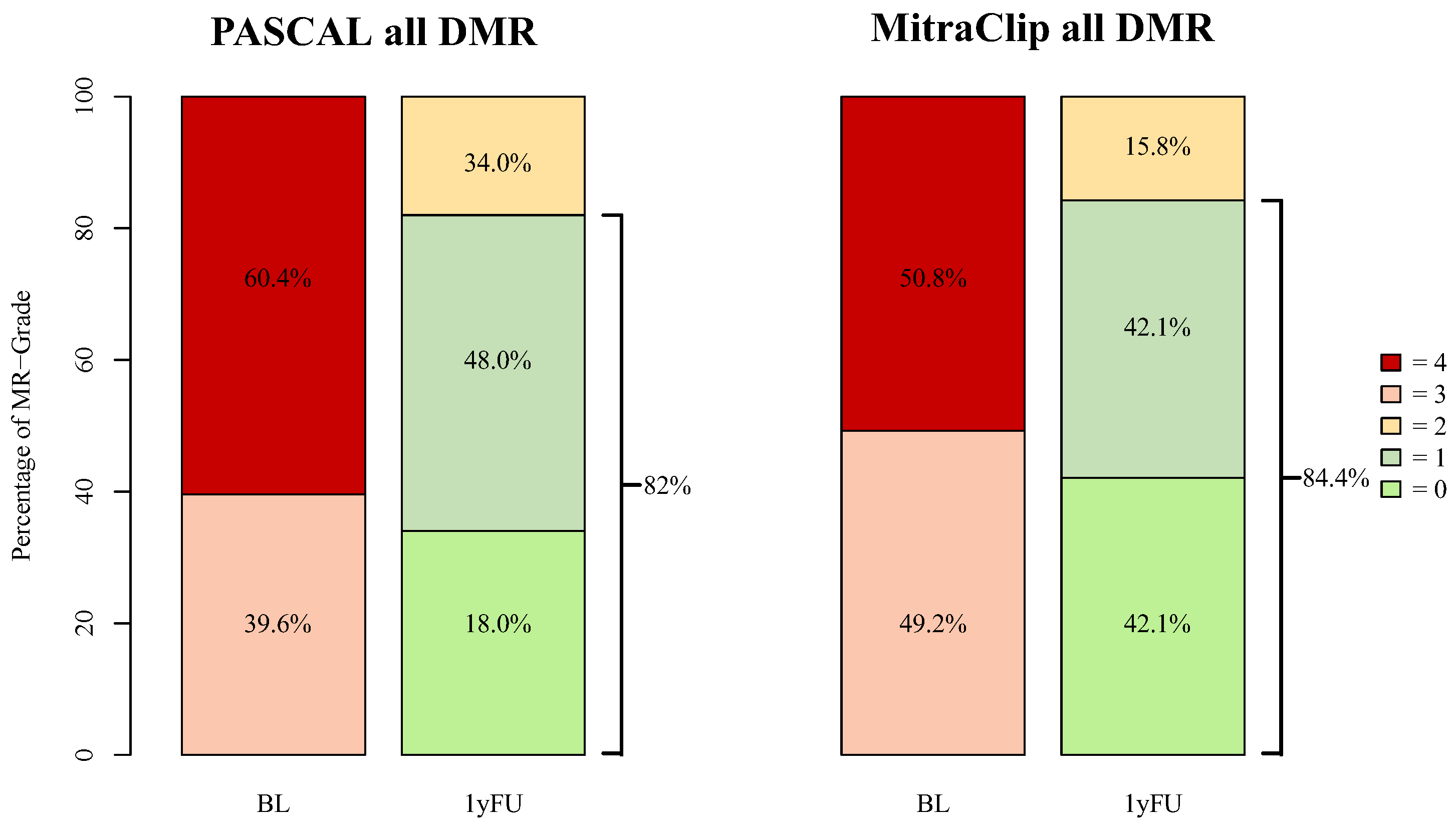
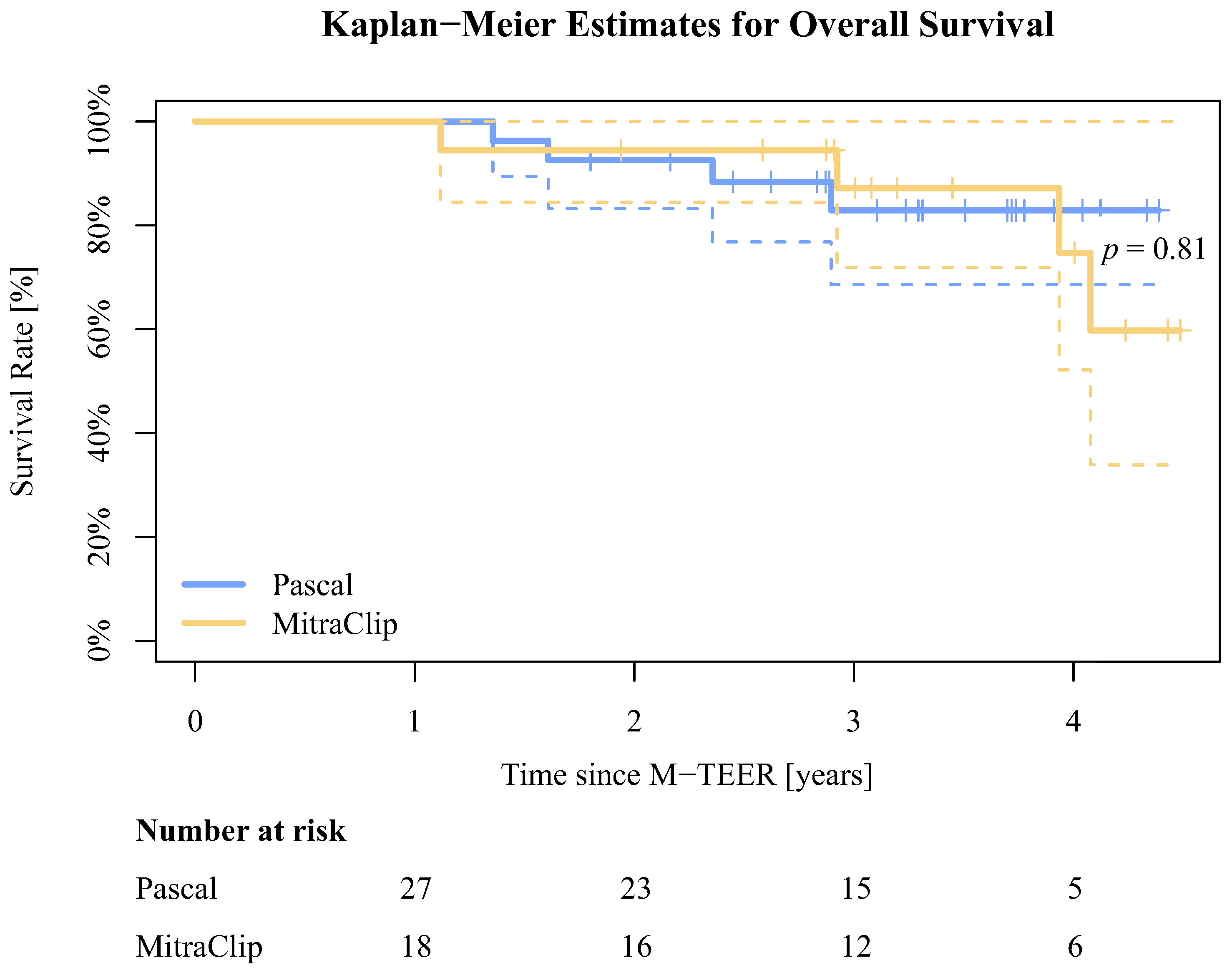
3.4. Outcome
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lim, D.S.; Smith, R.L.; Gillam, L.D.; Zahr, F.; Chadderdon, S.; Makkar, R.; von Bardeleben, R.S.; Kipperman, R.M.; Rassi, A.N.; Szerlip, M.; et al. Randomized Comparison of Transcatheter Edge-to-Edge Repair for Degenerative Mitral Regurgitation in Prohibitive Surgical Risk Patients. JACC Cardiovasc. Interv. 2022, 15, 2523–2536. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Rev. Esp. Cardiol. (Engl. Ed.) 2022, 75, 524. [Google Scholar] [CrossRef]
- Geis, N.A.; Schlegel, P.; Heckmann, M.B.; Katus, H.A.; Frey, N.; López, P.C.; Raake, P.W. One-year results following PASCAL-based or MitraClip-based mitral valve transcatheter edge-to-edge repair. ESC Heart Fail. 2022, 9, 853–865. [Google Scholar] [CrossRef] [PubMed]
- Hausleiter, J.; Lim, D.S.; Gillam, L.D.; Zahr, F.; Chadderdon, S.; Rassi, A.N.; Makkar, R.; Goldman, S.; Rudolph, V.; Hermiller, J.; et al. Transcatheter Edge-to-Edge Repair in Patients with Anatomically Complex Degenerative Mitral Regurgitation. J. Am. Coll. Cardiol. 2023, 81, 431–442. [Google Scholar] [CrossRef]
- Mauri, V.; Sugiura, A.; Spieker, M.; Iliadis, C.; Horn, P.; Öztürk, C.; Besler, C.; Riebisch, M.; Al-Hammadi, O.; Ruf, T.; et al. Early Outcomes of 2 Mitral Valve Transcatheter Leaflet Approximation Devices: A Propensity Score–Matched Multicenter Comparison. Cardiovasc. Interv. 2022, 15, 2541–2551. [Google Scholar] [CrossRef]
- Gerçek, M.; Roder, F.; Rudolph, T.K.; Fortmeier, V.; Zittermann, A.; Rudolph, V.; Friedrichs, K.P. PASCAL mitral valve repair system versus MitraClip: Comparison of transcatheter edge-to-edge strategies in complex primary mitral regurgitation. Clin. Res. Cardiol. 2021, 110, 1890–1899. [Google Scholar] [CrossRef] [PubMed]
- Lubos, E.; Schlüter, M.; Vettorazzi, E.; Goldmann, B.; Lubs, D.; Schirmer, J.; Treede, H.; Reichenspurner, H.; Blankenberg, S.; Baldus, S.; et al. MitraClip Therapy in Surgical High-Risk Patients: Identification of Echocardiographic Variables Affecting Acute Procedural Outcome. JACC Cardiovasc. Interv. 2014, 7, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.H.; Asch, F.; Sorajja, P.; Mahoney, P.; Price, M.J.; Maisano, F.; Denti, P.; Morse, M.A.; Rinaldi, M.; Bedogni, F.; et al. Expanding the Spectrum of TEER Suitability: Evidence from the EXPAND G4 Post Approval Study. JACC Cardiovasc. Interv. 2023, 16, 1474–1485. [Google Scholar] [CrossRef] [PubMed]
- Buzzatti, N.; De Bonis, M.; Denti, P.; Barili, F.; Schiavi, D.; Di Giannuario, G.; La Canna, G.; Alfieri, O. What is a ‘good’ result after transcatheter mitral repair? Impact of 2+ residual mitral regurgitation. J. Thorac. Cardiovasc. Surg. 2016, 151, 88–96. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PASCAL | MitraClip | |||
|---|---|---|---|---|
| Availability | n = 141 | n = 69 | p | |
| Age Median (IQR), years | 210/210 | 83 (80–85) | 83 (78–86) | 0.96 |
| Female Gender n (%) | 210/210 | 78 (100) | 40 (100) | 0.77 |
| BMI Median (IQR), kg/m2 | 210/210 | 24.7 (22.1–28.7) | 24.6 (22.2–29.1) | 0.89 |
| Atrial Fibrillation n (%) | 208/210 | 128 (91.4) | 61 (89.7) | 0.63 |
| Arterial Hypertension n (%) | 210/210 | 106 (75.2) | 53 (76.8) | 0.87 |
| Diabetes n (%) | 209/210 | 20 (14.3) | 13 (18.8) | 0.42 |
| COPD n (%) | 210/210 | 9 (6.4) | 11 (15.9) | 0.043 |
| Coronary Artery Disease n (%) | 210/210 | 63 (44.7) | 36 (52.2) | 0.38 |
| LVEF Median (IQR), % | 192/210 | 44 (38–51) | 43 (36.5–48) | 0.36 |
| STS-Score Median (IQR), % | 129/210 | 2.34 (1.6–3.4) | 3.07 (1.5–5.9) | 0.19 |
| EuroSCORE II Median (IQR), % | 171/210 | 3.63 (2.5–5.7) | 4.65 (2.6–7.3) | 0.15 |
| GFR Median (IQR), mL/min | 144/210 | 56 (41–71) | 52 (33–72) | 0.21 |
| Creatinine Median (IQR), mg/dL | 207/210 | 1.1 (0.8–1.4) | 1.2 (1–1.7) | 0.021 |
| NT-proBNP Median (IQR), pg/mL | 154/210 | 2010 (876.3–3985) | 2910 (859.8–5807.5) | 0.43 |
| 6-MWD mean ± SD, m | 79/210 | 280 (160–360) | 200 (180–250) | 0.24 |
| NYHA Grade | 209/210 | I:0; II:20; III:109; IV:12 | I:0; II:6; III:52; IV:10 | 0.10 |
| n of Clips Implanted n | 209/210 | 1:59; 2:64; 3:15 | 1:35; 2:25; 3:8 | 0.10 |
| Procedure Time Median (IQR), min | 209/210 | 91 (66–115) | 84 (66–114) | 0.49 |
| Fluoroscopy Time Median (IQR), min | 143/210 | 7.1 (5.1–12.38) | 10.2 (7–15.7) | 0.020 |
| Prolapse n (%) | 141/210 | 69 (66.99) | 28 (73.68) | 0.30 |
| Flail n (%) | 141/210 | 53 (51.46) | 13 (34.21) | 0.007 |
| Flail Gap Median (IQR), mm | 72/210 | 4 (3–5) | 3 (2–3) | 0.16 |
| Flail Width mean ± SD, mm | 72/210 | 7 (5–9) | 7 (5–8) | 0.81 |
| MR-EROA Median (IQR), cm2 | 190/210 | 0.4 (0.3–0.7) | 0.4 (0.2–0.6) | 0.21 |
| Mean MV-Gradient Median (IQR), mmHg | 186/210 | 2.4 (1.8–3.6) | 2 (1.6–3) | 0.14 |
| MR-Grade n, Grade | 204/210 | I:1; II:0; III:54; IV:84 | I:1; II:0; III:31; IV:33 | 0.19 |
| TR-Grade n, Grade | 196/210 | 0:13; I:55; II:33; III:25; IV:4; V:4 | 0:4; I:27; II:22; III:9; IV:0; V:0 | 0.66 |
| PASCAL | MitraClip | |||
|---|---|---|---|---|
| Availability | n = 27 | n = 18 | p | |
| Age Median (IQR), years | 45/45 | 81 (78–85) | 83 (77–86.75) | >0.99 |
| Female Gender n (%) | 45/45 | 7 (25.93) | 7 (38.89) | 0.51 |
| BMI Median (IQR), kg/m2 | 45/45 | 25 (23.91–26.79) | 24.46 (22.88–26.49) | 0.43 |
| Atrial Fibrillation n (%) | 45/45 | 18 (66.67) | 10 (55.56) | 0.54 |
| Arterial Hypertension n (%) | 45/45 | 26 (96.3) | 14 (77.78) | 0.14 |
| Diabetes n (%) | 45/45 | 4 (14.81) | 2 (11.11) | >0.99 |
| COPD n (%) | 45/45 | 4 (14.81) | 3 (16.67) | >0.99 |
| Coronary Artery Disease n (%) | 45/45 | 10 (37.04) | 7 (38.89) | >0.99 |
| LVEF Median (IQR), % | 45/45 | 55 (54.5–55) | 55 (51.25–55) | 0.60 |
| STS-Score Median (IQR), % | 45/45 | 2.07 (1.14–3.3) | 2.28 (1.2–3.9) | 0.69 |
| EuroSCORE II Median (IQR), % | 45/45 | 3.25 (2.07–4.98) | 3.62 (2.79–4.6) | 0.35 |
| GFR Median (IQR), mL/min | 45/45 | 58 (39–70.5) | 51 (35–71.75) | 0.67 |
| Creatinine Median (IQR), mg/dL | 45/45 | 1.1 (0.95–1.4) | 1.05 (0.94–1.67) | 0.74 |
| NT-proBNP Median (IQR), pg/mL | 39/45 | 2410 (892–3580) | 3355 (1048–5690) | 0.27 |
| 6-MWD mean ± SD, m | 27/45 | 270 ± 112.8 | 249.23 ± 118.78 | 0.65 |
| NYHA Grade | 45/45 | I:0; II:3; III:23; IV:1 | I:0; II:3; III:14; IV:1 | 0.77 |
| PASCAL | MitraClip | |||
|---|---|---|---|---|
| Availability | n = 27 | n = 18 | p | |
| n of Clips Implanted n | 45/45 | 1:9; 2:16; 3:2 | 1:7; 2:8; 3:3 | 0.77 |
| Type of Clips n | 45/45 | P10: 22; ACE: 6 | XTR: 16; NTR: 4; NT: 1; NTW: 1 | - |
| Procedure Time Median (IQR), min | 45/45 | 103 (82–123.5) | 88 (72.75–115.5) | 0.52 |
| Fluoroscopy Time Median (IQR), min | 45/45 | 6.8 (5.15–9.25) | 8.75 (7.05–14.23) | 0.026 |
| Dose Area Product Median (IQR), min | 45/45 | 374 (212.05–680.95) | 324 (224.25–685.15) | 0.72 |
| PASCAL | MitraClip | |||
|---|---|---|---|---|
| Availability | n = 27 | n = 18 | p | |
| M. Barlow n (%) | 45/45 | 0 (0) | 1 (5.56) | 0.40 |
| Prolapse n (%) | 45/45 | 11 (40.74) | 4 (22.22) | 0.33 |
| Flail n (%) | 45/45 | 19 (70.37) | 10 (55.56) | 0.35 |
| Flail Gap Median (IQR), mm | 29/45 | 4 (2–5) | 5.5 (2.25–6.75) | 0.29 |
| Flail Width mean ± SD, mm | 29/45 | 9.68 ± 4.46 | 10 ± 3.13 | 0.83 |
| MR-EROA Median (IQR), cm2 | 43/45 | 0.6 (0.45–0.7) | 0.45 (0.4–0.8) | 0.47 |
| Regurgitant Volume Median (IQR), mL | 42/45 | 87.54 ± 36.27 | 75 ± 37.36 | 0.29 |
| MR-VCD Median (IQR), mm | 45/45 | 9.67 ± 2.81 | 9.89 ± 2.47 | 0.78 |
| PISA radius Median (IQR), mm | 45/45 | 9.33 ± 2.06 | 10.39 ± 2.83 | 0.18 |
| Mean MV-Gradient Median (IQR), mmHg | 38/45 | 2 (1–3) | 2.5 (2–3) | 0.20 |
| MR-Grade n, Grade | 45/45 | I:0; II:0; III:9; IV:18 | I:0; II:0; III:3; IV:15 | 0.23 |
| PASCAL | MitraClip | |||
|---|---|---|---|---|
| Availability | n = 27 | n = 18 | p | |
| MR-EROA Median (IQR), cm2 | 44/45 | 0.1 (0.1–0.1) | 0.2 (0.1–0.2) | 0.04 |
| ΔMR-EROA Median (IQR), cm2 | 42/45 | 0.5 (0.4–0.6) | 0.3 (0.3–0.6) | 0.18 |
| Regurgitant Volume mean ± SD, mL | 44/45 | 13.5 (9.3–18.5) | 18.5 (9.3–26) | 0.4 |
| ΔRegurgitant Volume mean ± SD, mL | 41/45 | 70.7 ± 34.9 | 56.8 ± 38 | 0.19 |
| MR-VCD median (IQR), mm | 44/45 | 4.5 (3–6) | 4 (4–6.75) | 0.45 |
| ΔMR-VCD median (IQR), mm | 44/45 | 5.2 ± 3.2 | 5 ± 2.9 | 0.81 |
| PISA Radius median (IQR), mm | 44/45 | 5 (4–5) | 5 (4–6) | 0.29 |
| ΔPISA Radius mean ± SD, mm | 44/45 | 4.5 ± 2.8 | 5.2 ± 3.1 | 0.47 |
| Mean MV-Gradient Median (IQR), mmHg | 39/45 | 3 (2.9–4.5) | 3 (1.8–4) | 0.22 |
| ΔMean MV-Gradient Median (IQR), mmHg | 36/45 | 1.9 ± 1.7 | 0.6 ± 1.6 | 0.028 |
| MR-Grade n, Grade | 45/45 | I:16; II:8; III:1; IV:0 | I:9; II:8; III:0; IV:0 | 0.54 |
| ΔMR-Grade median (IQR), Grade | 45/45 | 2 (2–3) | 2 (2–3) | 0.87 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rudolph, F.; Kirchner, J.; Ivannikova, M.; Fortmeier, V.; Rudolph, T.K.; Friedrichs, K.P.; Rudolph, V.; Gerçek, M. A Comparative Study of 1-Year Postprocedural Outcomes in Transcatheter Mitral Valve Repair in Advanced Primary Mitral Regurgitation: PASCAL vs. MitraClip. J. Clin. Med. 2024, 13, 484. https://doi.org/10.3390/jcm13020484
Rudolph F, Kirchner J, Ivannikova M, Fortmeier V, Rudolph TK, Friedrichs KP, Rudolph V, Gerçek M. A Comparative Study of 1-Year Postprocedural Outcomes in Transcatheter Mitral Valve Repair in Advanced Primary Mitral Regurgitation: PASCAL vs. MitraClip. Journal of Clinical Medicine. 2024; 13(2):484. https://doi.org/10.3390/jcm13020484
Chicago/Turabian StyleRudolph, Felix, Johannes Kirchner, Maria Ivannikova, Vera Fortmeier, Tanja Katharina Rudolph, Kai Peter Friedrichs, Volker Rudolph, and Muhammed Gerçek. 2024. "A Comparative Study of 1-Year Postprocedural Outcomes in Transcatheter Mitral Valve Repair in Advanced Primary Mitral Regurgitation: PASCAL vs. MitraClip" Journal of Clinical Medicine 13, no. 2: 484. https://doi.org/10.3390/jcm13020484
APA StyleRudolph, F., Kirchner, J., Ivannikova, M., Fortmeier, V., Rudolph, T. K., Friedrichs, K. P., Rudolph, V., & Gerçek, M. (2024). A Comparative Study of 1-Year Postprocedural Outcomes in Transcatheter Mitral Valve Repair in Advanced Primary Mitral Regurgitation: PASCAL vs. MitraClip. Journal of Clinical Medicine, 13(2), 484. https://doi.org/10.3390/jcm13020484