Abstract
Objective: to review evidence on the efficacy of auditory training in adult cochlear implant recipients. Data Sources: PRISMA guidelines for a systematic review of the literature were followed. PubMed, Scopus, and CINAHL databases were queried on 29 June 2023 for terms involving cochlear implantation and auditory training. Studies were limited to the English language and adult patient populations. Study Selection: Three authors independently reviewed publications for inclusion in the review based on a priori inclusion and exclusion criteria. Inclusion criteria encompassed adult cochlear implant populations, an analysis of clinician- or patient-directed auditory training, and an analysis of one or more measures of speech recognition and/or patient-reported outcome. Exclusion criteria included studies with only pediatric implant populations, music or localization training in isolation, and single-sample case studies. Data Extraction: The data were collected regarding study design, patient population, auditory training modality, auditory training timing, speech outcomes, and data on the durability of outcomes. A quality assessment of the literature was performed using a quality metric adapted from the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group guidelines. Data Synthesis and Meta-Analysis: Data were qualitatively summarized for 23 studies. All but four studies demonstrated significant improvement in at least one measured or patient-reported outcome measure with training. For 11 studies with sufficient data reporting, pre-intervention and post-intervention pooled means of different outcome measures were compared for 132 patients using meta-analysis. Patient-direct training was associated with significant improvement in vowel-phoneme recognition and speech recognition in noise (p < 0.05 and p < 0.001, respectively), and clinician-directed training showed significant improvement in sentence recognition in noise (p < 0.001). Conclusions: The literature on auditory training for adult cochlear implant recipients is limited and heterogeneous, including a small number of studies with limited levels of evidence and external validity. However, the current evidence suggests that auditory training can improve speech recognition in adult cochlear implant recipients.
1. Introduction
Cochlear implantation has become the standard of care for rehabilitation of moderate to profound sensorineural hearing loss, with studies showing consistent improvement in speech recognition and quality of life following implantation [1,2]. Such successes have spurred the gradual broadening of cochlear implant (CI) candidacy criteria, with the global economic impact of cochlear implantation expected to exceed USD 2.5 billion in the next several years [3,4,5]. Despite advances in device design, surgical technique, and programming strategies, post-CI speech recognition still falls well short of normal hearing, with significant variability in speech recognition outcomes [6,7,8]. Unfortunately, other than changes in CI programming by audiologists, few interventions are available to help improve CI outcomes following surgery. One potential avenue to optimize CI outcomes is aural rehabilitation. Broadly, comprehensive aural rehabilitation consists of the components of sensory management, instruction, counseling, and perceptual training, with the latter most often being auditory (or audiovisual) training [9]. However, while likely beneficial to the CI population, current evidence to guide these interventions remains scarce. To address this knowledge gap, this systematic review and meta-analysis summarizes the available evidence regarding the efficacy of auditory training in adult CI users [10,11,12,13,14,15].
Hearing with a CI is a unique experience compared to normal acoustic hearing. While patients typically show significant improvements in speech recognition and quality of life, there remains a deficit in speech recognition, with mean word recognition ability in the quiet of approximately 50–70% and substantial unexplained variability among individuals [6,8,16]. A large portion of hearing deficits and variability among patients may be related to patients having to learn how to process the electrically coded speech signal. For some patients, this process comes passively during daily life, but for others, it may require more intentional practice or rehabilitation. For some adults, the learning process for adaptation to hearing with a CI can be protracted, with reports of peak CI speech recognition ability reaching 1–2 years after implantation [17,18]. Post-CI auditory training may improve or accelerate this learning process and is inexpensive or free, in contrast to the high costs of cochlear implantation itself.
A variety of auditory training exercises have been developed, but there is no standardization for use in the adult CI population [10]. In general, auditory training can be broken down into two categories: patient-directed, at-home exercises and clinician-directed training sessions, which are typically led by a speech-language pathologist. The patient-directed, at-home exercises include passive listening exercises, such as listening to recorded speech or audiobooks, listening to the radio, or watching television, and active listening exercises. Active exercises can include listening exercises with communication partners with feedback, speech-tracking exercises, or computer-based auditory training (CBAT), which employs interactive software that has often been developed by CI companies.
Research on the effectiveness of auditory training in adult CI users is scarce, but the limited data show evidence of speech and quality-of-life benefits in those patients who pursue auditory training; a recent survey of CI audiologists demonstrated that 85% recommended the use of such resources in the immediate post-activation period [10,14,15,19,20]. A report by Dornhoffer et al. also showed benefits in CI-specific quality-of-life outcomes with the use of at-home CBAT software programs [21]. However, many extant studies are limited in their scope and external validity, fail to include commonly available forms of auditory training, or have an insufficient sample size to draw meaningful conclusions [10,11,12,13,14,15]. As a result, most audiologists and physicians are limited to empirically recommending various patient-driven rehabilitation strategies due to scant evidence on the benefits of specific resources [10,11,12,13]. Therefore, a formal evaluation of the efficacy of commonly used clinician- or patient-directed auditory training techniques is of great importance to fill this research gap.
This study aims to provide an updated literature review and meta-analysis to determine the effectiveness of commonly available auditory training/listening activities in improving outcomes related to speech recognition and CI-specific quality of life. The goal is to provide preliminary, specific recommendations on appropriate post-CI auditory training, which can offer an affordable measure by which to optimize implant outcomes.
2. Material and Methods
2.1. Systematic Search Strategy
The literature search was performed following the Preferred Reporting Items for Systemic Reviews and Meta-analyses (PRISMA) guidelines [22]. Inclusion criteria were generated using the Participants, Intervention, Control, Outcomes, and Study Designs (PICOS) strategy. PICOS inclusion and exclusion criteria are detailed in Table 1 and broadly include studies examining post-CI auditory training in adult patients [23]. This study was not registered.

Table 1.
PICOS inclusion criteria.
2.2. Study Identification
A flow diagram of the study identification and review is detailed in Figure 1. Three reviewers independently searched the PubMed, Scopus, and CINAHL databases on 29 June 2023 for appropriate studies of auditory training for adult CI recipients. The following search terms were used: cochlear implant OR cochlear implantation OR cochlear implants AND listening activities OR aural rehabilitation OR aural training OR training OR activities OR exercises OR auditory training OR auditory rehabilitation OR speech therapy OR speech pathology OR speech pathologist. The following filters were employed: English language, full text, and adult patient. Our search yielded 2154 articles. Ten additional articles were identified from a previous literature review by Cambridge et al. and an analysis of review article reference lists encountered in our search [24]. After removing duplicate articles, 2130 unique articles were identified.
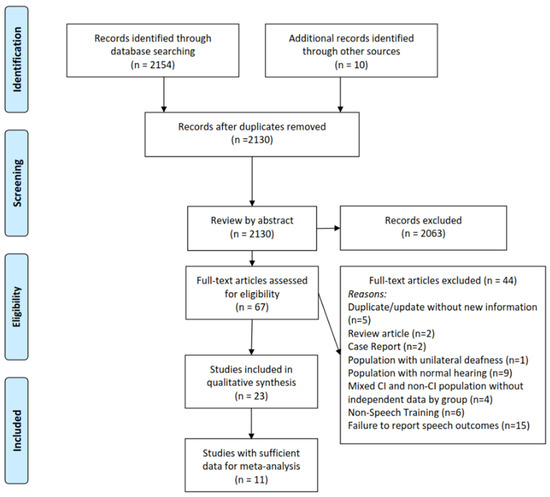
Figure 1.
Flow diagram of study selection, eligibility, and inclusion.
2.3. Study Screening and Selection
Articles identified in our search were reviewed by title and abstract for our PICOS inclusion and exclusion criteria by three independent reviewers (J.R.D., T.P., and K.R.K.). Discrepancies were resolved by a senior author. There was no time range or limitation on the publication date. After review by title and abstract, 67 articles underwent full-text review for inclusion. After a full-text review, 23 articles were included in the review. Reasons for dismissal of full-text articles from review included: duplicate article or update of article without new information (n = 5), review article (n = 2), case report (n = 2), population with unilateral deafness (n = 1), population with normal hearing (n = 9), mixed CI and non-CI population without independent data by group (n = 4), non-speech training (n = 6), and no report of speech recognition outcomes (n = 15). Additionally, articles were reviewed to ensure no overlapping study populations were included.
2.4. Data Extraction
Data collected from studies included the first author, year of publication, study design, patient population, patient demographics, implant laterality, implant duration of use, target pre-intervention implant performance if noted, training modality, training frequency, training duration, training time period, training environment, speech recognition scores, patient-reported outcome scores, reports of auditory training compliance where available, and any commentary offering insight on follow-up outcome measures or the durability of outcome measures (e.g., data collection any period of time after the initial post-training timepoint). If a study had two study arms or protocols without crossover and with different populations, each population and its data were selected and detailed separately.
Given the heterogeneity of the interventions noted in the literature, different interventions were grouped based on the level of clinician interaction: patient-directed, which were interventions solely reliant on patient usage of the resource; clinician-directed, which were interventions that relied heavily on clinician interaction or guidance during a patient’s use of the training program; and mixed, for those interventions with distinct portions performed independently by the patient and also with clinician interaction.
2.5. Analysis of Quality
Assessment of quality was performed utilizing a metric adapted from that utilized by Henshaw et al. for the analysis of auditory training [25]. The metric was developed in accordance with the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group guidelines [26]. Three authors (J.R.D., T.P., and K.R.K.) independently reviewed each article and assigned their quality assessment. If unanimity was not achieved, scores were assigned to the majority score or averaged if all authors disagreed.
The metric involved assessing ten factors for quality in each study. Five factors dealt with general scientific quality: randomization, presence of a control, power calculation/large sample size, blinding, and scientific reporting of outcome measures. Low scores on such factors would indicate poor internal validity or the potential for bias. Five factors dealt with the general external validity of each study with respect to real-world auditory training: external validity of outcome measure, external validity of training or training environment, reporting on training compliance, reporting of long-term or durable results (outcome reporting any time after the initial post-intervention period), and the presence of constructive/corrective feedback during training. Scores for each factor ranged from 0 to 2. As per Henshaw et al., a score of 0 indicated flawed or no information from which to make a judgment, a score of 1 indicated weak information or lack of detail, and a score of 2 indicated appropriate use and reporting [25]. Scores were totaled for each factor to form an overall quality assessment score. As adapted from the GRADE guidelines, studies with scores from 0 to 5 represented a very low level of evidence, 6 to 10 a low level of evidence, 11 to 15 a moderate level of evidence, and 16 to 20 a high level of evidence.
2.6. Statistical Analysis
Studies with sufficient reporting on outcomes and population data were included in a meta-analysis of outcomes. Each study’s sample data were combined, with the weighted mean and standard deviation determined. Differences were noted using the variable delta (Δ). Pre-intervention and post-intervention pooled means of each subdomain were compared using a comparison of weighted means using a meta-analysis of continuous measures performed with Cochrane Review Manager (RevMan Version 5.4 Cochrane Collaboration 2020). The fixed-effects model was used after consideration of both fixed- and random-effects models. This assumption is tested using the heterogeneity test or I2 statistic. I2 values of 25%, 50%, and 75% represented low, medium, and high heterogeneity, respectively. If this test yields a low probability value (p < 0.05), then there is a high likelihood that the fixed-effects model is invalid and the random-effects model is more appropriate [27]. The random-effects model incorporates both the random variation within the studies and the variation between the different studies.
3. Results
3.1. Study Characteristics
The study characteristics are summarized in Table 2. In total, 23 publications were identified that met a priori inclusion and exclusion criteria. Publication dates ranged from 1991 to 2023. One study by Tyler et al. featured two different treatments for different populations. As such, these were considered as separate studies [28]. The majority of studies (n = 13) were repeated measure studies, examining a single uncontrolled cohort [13,20,28,29,30,31,32,33,34,35,36,37,38]. A total of seven studies were randomized controlled trials or crossover trials [39,40,41,42,43,44,45], and four studies were nonrandomized controlled trials or cohort studies [21,28,46,47].
Table 2.
Details of study design and patient populations.
3.2. Patient Populations
The characteristics of the study samples are detailed in Table 2. With the exception of Dornhoffer et al., an observational study of 72 patients [21], patient samples were generally small (n = 3–24), with the next largest experimental group being 24 CI recipients [41]. Most studies (n = 13) examined a majority of patients with unilateral implantation, with only Tyler et al. reporting bilaterally implanted patients [28].
Most studies examined patient populations of experienced CI users. Only four studies examined auditory training in new CI users [21,31,43,47]. Of those studies examining experienced CI recipients, nine targeted specific levels of pre-training CI performance. Fu et al. [20], Ingvalson et al. [33], and Borel et al. [30] reported on patients with poor word recognition scores, subjective poor performance, or poor performance with a phone, respectively. In contrast, Schuman et al. [39], Barlow et al. [29], and Greene et al. [29] included CI users with high pre-training word or speech recognition. All other studies did not report on the population targeted for the intervention or examined typically performing CI users.
3.3. Interventions
All studies utilized unique resources or algorithms for auditory training. Most studies utilized or reported on some form of CBAT. Six studies utilized the Computer Assisted Speech Training (CAST) program developed at the House Ear Institute [20] or programs developed from it, such as Angel Sound™ [20,21,34,35,38,47]. All other studies employed custom CBAT programs created for the individual study or featured interventions still in development.
A small number of studies (n = 4) did not utilize any form of computer program-based intervention. Gagne et al. [31] utilized an individualized, clinician-based auditory training strategy; Bernstein et al. [45] also reported on a clinician-based strategy combined with equipment and listening-strategy counseling. Ihler et al. [44] utilized a CD recording of spectrally filtered or normal speech in various conditions and difficulties, the degree of which was chosen by patient preference, and Borel et al. [30] utilized listening tasks directed by a speech-language therapist over a phone. Dornhoffer et al. [21] reported on patients utilizing clinician-directed therapies and passive-home-based exercises; however, patients were free to use any resource, such as a CBAT program. Moberly et al. [47] and Völter et al. [37] reported on a strategy using both clinician-directed and computer-based training. Specific details of the training exercises used in each study are described in Table 3.
Table 3.
Details of study interventions.
Most studies exclusively used some form of phoneme-, word-, or digit-recognition exercise in various signal-to-noise ratios (SNR) as training material. A smaller proportion utilized additional or alternative training methodologies. Tyler et al. used localization training in addition to word recognition training [28]. Ihler et al. used spectrally filtered speech to train CI use with a phone [44]. Borel et al. [30] used clinician-directed listening exercises over the phone [30]. Lastly, Shafiro et al. used environmental noise identification exercises, which included human vocalization in addition to common environmental sounds [36]. Given the current study’s focus on speech recognition skills, studies with music and localization training in isolation were excluded from our analysis based on our a priori criteria.
The length, timing, and duration of interventions varied widely among studies. The length of individual training sessions, when prescribed, ranged from fifteen minutes to three hours. Most studies utilized daily, or close to daily, training, although three studies employed a twice-weekly intervention and one used weekly training [31,39,42,46]. Two studies used a combination of weekly clinician-directed training with additional training either based on patient preference [47] or completed daily [37]. The overall duration of the studies ranged from 4 days to 16 weeks, with the majority of studies offering training over the course of 3–6 weeks.
Most studies offered auditory training at home, with nine requiring at least one portion of intervention in a laboratory or clinic setting. However, home-based interventions did not always represent a normal home environment. Six studies with patient-directed training in the home actively monitored compliance, with notifications from the research team for patients to resume or complete their auditory training [13,29,32,35,38,44]. Additionally, Tyler et al. [28] required patients to use specific speakers and a unique speaker setup that was provided by the lab for their home-based intervention.
3.4. Qualitative Analysis of Outcomes
A summary of CI outcome measures for each study is detailed in Table 4. As per our a priori inclusion criteria, included studies were required to report at least one measure of speech recognition or patient-reported outcome measure. Beyond that, there was no one measure that was common to all studies examined, with studies employing variable outcome measures in a variety of noise conditions. Less than half of studies used patient-reported outcome measures [13,21,30,34,37,41,43,44,45,47]. As with speech measures, patient-reported outcomes varied, with no single instrument common to all studies. Examples of patient-reported outcome measures utilized included the Cochlear Implant Quality-of-Life 35 Profile [48], the Abbreviated Profile of Hearing Aid Benefit (APHAB) [49], the Glascow Benefit Inventory [50], the Hearing Handicap Inventory [51], and the Nijmegen Cochlear Implant Questionnaire [52].
Table 4.
Speech outcomes, statistical significance, and long-term follow-up for included studies.
A summary of outcomes demonstrating statistical significance for each study is also detailed in Table 4. Despite the large variety of training stimuli and outcome measures, all but four studies demonstrated significant improvement in at least one measure of phoneme, word, or sentence recognition with training [31,36,42,47]. Where reported, improvements were often generalizable, with a majority of the studies demonstrating improvement in off-task outcome tests, meaning word/sentence stimuli used in the outcome measure were not included in the trained stimuli. For example, Ihler et al. [44] trained CI users with spectrally filtered speech in order to use phones more proficiently, but the cohort that trained with the spectrally filtered speech also had improvement in tests of unfiltered speech in quiet as compared to the control group. Additionally, Miller et al. (2008) [42] showed that patients trained in their Speech Perception and Training System (SPATS) improved in recognition of both study materials and untrained CNC (Consonant-Nucleus-Consonant) lists and HINT (Hearing in Noise Test) sentences in quiet and in noise. However, this was not universal, as Reis et al. [41] reported little to no off-task training in a randomized cross-over study of a CBAT protocol with and without visual components. For studies detailing at least one patient-reported outcome measure, significant improvement was reported for most [21,30,37,41,43,45], but not all studies [13,34,44,47]. No study showed a decline in any patient-reported outcome measure with training. Similarly, no study showed a significant decline in any measure of speech recognition.
Regarding the durability of these improvements, 13 studies reported on follow-up or data taken after the cessation of training. The time period in these studies ranged anywhere from 4 days to 8 months. Most studies that reported follow-up showed the durability of the training effect. Green et al. [32], for example, showed that the SRTs of Bamford–Kowal–Bench (BKB) [53] and IEEE sentences in both male and female voices remained stable or even continued to improve over the 1-month post-training period. Schumann et al. [39] also showed stability of training at 6 months for speech recognition in noise at 0 dB SNR and +5 dB SNR. However, Reis et al. [41] demonstrated that significant improvements were seen in CNC word scores in quiet and the Quality-of-Life Scale [54]. Scores immediately after training were no longer significant relative to baseline one to three months after the cessation of training.
3.5. Meta-Analysis of Outcomes
Of the 23 studies included in this review, 11 had sufficient data reporting for meta-analysis of outcomes, as detailed in Table 4. A summary of the pooled patient sample for meta-analysis is detailed in Table 5. For the purposes of outcome synthesis, each meta-analysis was performed based on the type of auditory training provided. The pooled analysis outcomes are detailed for each type of training in Table 6 and in Figure 2, Figure 3 and Figure 4. The heterogeneity of outcomes ranged from low to medium in this body of the literature.
Table 5.
Demographic summary of study samples included in meta-analysis.
Table 6.
Pooled mean difference of intervention by subtype.
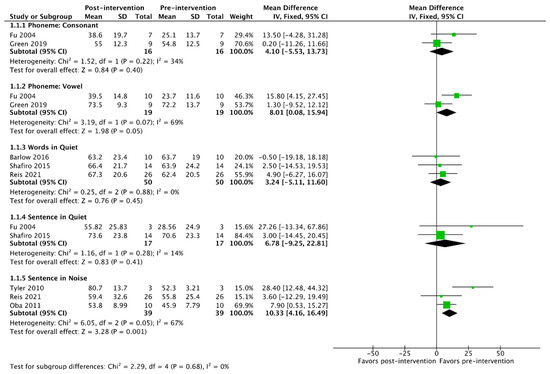
Figure 2.
Meta-analysis of outcomes for patient-directed interventions [20,28,29,32,35,36,41].
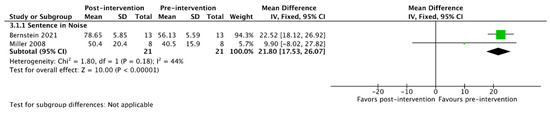
Figure 3.
Meta-analysis of outcomes for clinician-directed interventions [42,45].
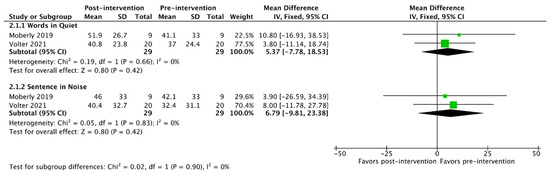
Figure 4.
Meta-analysis of outcomes for mixed: patient-directed and clinician-directed interventions [37,47].
Of the studies included in the meta-analysis, seven detailed the use of some form of primarily patient-directed training intervention. Table 6 and Figure 2 display that there was a significant improvement in vowel phoneme recognition in quiet and sentence recognition in noise. No other improvements were observed.
Considering interventions that were primarily clinician-directed, two studies were identified. The only common metric of speech recognition available for meta-analysis was sentence recognition in noise, which demonstrated a significant improvement from pre- to post-intervention (Table 6 and Figure 3).
Finally, two studies were identified that utilized a mixed intervention with distinct clinician-directed and patient-directed components. Word recognition in quiet and sentence recognition were available for pooled analysis in these studies (Table 6 and Figure 4). While both metrics trended toward improved outcomes from pre- to post-intervention, the change was not significant (95% confidence interval of improvement crosses 0).
3.6. Quality Assessment
The total quality assessment scores and scores for each quality assessment factor are detailed in Table 7. Overall, the quality of the literature on this topic is low. Only eight studies qualified as a moderate level of evidence, which is the highest seen in this body of the literature. The remaining 15 studies had either a very low level of evidence (2) or a low level of evidence (13).
Table 7.
Study quality scores and levels of evidence for included articles.
4. Discussion
4.1. Overview
Learning to listen with a new CI is often equated to learning a new language. To help with this process, auditory training is often recommended for new CI recipients. These training approaches may range from simple at-home exercises, such as listening to an audiobook or radio, or they may involve focused, in-office therapy with a clinician or therapist. Computer-based CI training programs have also been developed, with each major CI company having developed its own proprietary software in addition to several other programs that are free or available for purchase. Angel SoundTM is one program developed in part from the CAST and SoundExpress computer programs used by Fu et al. [20], Oba et al. [35], and Zhang et al. [38]. Unfortunately, while auditory training is almost universally recommended, there is a paucity of the literature on the subject among adult CI users, and there is a lack of consensus on recommendations to guide auditory training or broader aural rehabilitation programs. In this study, we have reviewed the extant literature and found evidence of improvements in CI outcomes with auditory training, but studies generally suffer from low-quality evidence.
4.2. Efficacy of Auditory Training
Twenty-three studies were ultimately reviewed to analyze the effect of auditory training on CI outcomes. Most examined the effects of some form of patient-directed CBAT (Table 3), with a handful analyzing clinician-directed training or a combination of clinician-directed and/or other patient-directed interventions such as listening to spectrally filtered recorded stimuli on a CD [21,30,31,37,44,45,47]. Outcome measures varied widely from study to study and ranged from validated metrics, such as CNC words or AzBio sentences, to study-specific measures of speech recognition and sound localization. Of the 23 studies, 9 included at least one patient-reported outcome measure [13,21,30,34,37,41,43,44,47]. However, outcome measures were heterogeneous, and outcome reporting was variable, limiting the inclusion of some studies in the meta-analysis.
Meta-analysis of the available studies demonstrates an overall benefit from different types of auditory training, with significant improvements in various measures of speech recognition for both clinician-directed and patient-directed interventions (Figure 2, Figure 3 and Figure 4). However, while general benefit is demonstrated, the effectiveness of any specific training resource cannot be ascertained from this review due to near-universal small sample sizes and oftentimes mixed results within individual studies, with patients improving significantly on some measures while failing to improve on a similar measure in the same sample (Table 3). Additionally, the effectiveness of training—the ability to have a meaningful impact on patients under typical clinical conditions—is unclear based on the more controlled assessment and training settings applied for most of the studies reviewed.
Similarly, few conclusions can be drawn regarding the durability of outcomes. Only half of the studies collected data at any time beyond the immediate testing period. However, where available, all follow-up data appear largely to show durable outcomes, excepting one study that showed that improvement in quality of life was no longer significant 3 months after training [41].
Given the sparse literature on the efficacy of auditory training, other systematic reviews to date have been limited. Sweetow et al. [55] performed a similar systematic review on the efficacy of auditory training for non-CI hearing-impaired patients, and Henshaw et al. [25] reviewed the literature on auditory training in the general population, including CI and non-CI patients. Both reviews were limited by the number and quality of publications at their respective times of authorship; however, both reported similar results to this review. Namely, the evidence is heterogeneous and limited in statistical power, but the literature generally supports auditory training as a possible therapy for hearing-impaired patients. These conclusions are given with particular note to the affordability and lack of risk entailed in most auditory training exercises. Cambridge et al. [24] reviewed the results of auditory training in adult CI users after 2010. Their findings are similar to our own, albeit with a limited number of studies and a lack of meta-analyses, likely secondary to a limited search window. That said, as with the current study, they showed that all studies demonstrated some benefit in at least one measure of speech recognition skill, but the quality of the data was limited, concluding that only two studies controlled for covariables in such a manner that benefits could be attributable to training effects alone [39,46]. Rayes et al. [56] published a review of auditory training for pediatric CI users. Despite different target age groups, their findings are similar to our own in adults, namely, auditory training appears to afford benefits in both trained and off-task measures of speech recognition. However, as in the current review, the quality of the data and reporting of off-task testing were limited. Additionally, no studies on pediatric CI auditory training, as described by Rayes et al. [56], reported on patient-reported outcome measures.
While we do see that the literature on auditory training generally demonstrates benefits, we can primarily comment on CBAT, as this is the training modality utilized in the vast majority of studies. Only one study [31] examined clinician-directed therapy in isolation and did so with only four patients and no statistical analysis beyond qualitative assessment. Clinician-directed therapy was examined in three additional studies but in combination with other training modalities [21,47]. Similarly, only one study [44] examined a patient-directed training modality that was not a computer program using a CD of various speech scenarios. As such, the conservative findings that we derive from this review are primarily applicable to CBAT. The efficacy of many common exercises recommended to CI recipients, such as listening to an audiobook or the radio, is less certain. That said, longitudinal data from the use of such exercises in newly implanted adults demonstrated no significant benefits of these activities at 3 months post-activation [21].
4.3. Quality of Literature
While the outcomes of auditory training can be generalized as beneficial, the ability to make firm conclusions is restricted. The studies we examined were generally limited to one or two domains: the internal validity of the study and the external validity of the auditory training. Regarding internal validity, studies were often inadequate with respect to sample size, utilization of control groups, blinding, and randomization. As such, the power of these studies is limited. Moreover, the common lack of a control group makes it difficult to parse out the effect of intervention from passive CI learning, particularly in less experienced CI users.
Regarding external validity, we found that most studies failed to directly address the modalities of auditory training that are available for the standard CI recipient. As detailed above, almost all studies examined study-specific computer programs or programs still under development, and only six studies use a resource that is widely available or was ultimately developed into a currently available CBAT program (e.g., Angel SoundTM) [20,21,34,35,38,47]. Therefore, the results of many of these studies are not necessarily generalizable to the CBAT that is typically recommended by clinicians for adult CI users. Additionally, all but four studies included experienced CI users. The greatest gain in speech understanding for an average CI recipient is in the first 3 months, with some additional gain occurring up to 2 years [8,57]. Therefore, the application of these training interventions in the early post-CI period is likely important, as this is a key period of learning and plasticity for CI recipients. Unfortunately, the timing of many studies in the current literature precluded any evaluation of the value of auditory training during this time period.
4.4. Limitations and Future Goals
The limitations of this study were primarily related to the availability and quality of published data, as detailed above. Available data were generally heterogeneous and often not in compliance with recent guidelines for outcome reporting; as such, meta-analysis was only possible using data from less than half of the identified studies [58]. Additionally, due to a scarcity of data, meta-analysis was not possible on patient-reported outcome measures. Therefore, we can offer mostly qualitative generalizations regarding the impact of auditory training on the functional abilities of adult CI users. In general, auditory training appears to result in improved speech recognition in experienced CI users, but the strength of these effects and their generalizability to the overall adult CI population are low.
Future research will require additional prospective analysis of larger CI samples to determine the effect of commonly available exercises and interventions for auditory training on CI recipients. Studies should be designed to determine the efficacy of specific interventions that are widely available for use in the clinical setting. Future studies should also assess the impact of the timing of auditory training on CI outcomes, particularly during periods of rapid speech recognition growth, such as the early post-CI period. The current literature deals primarily with experienced CI users and often fails to assess the impact of auditory training during the key 6–12 months of CI speech recognition gain immediately after device activation [8].
5. Conclusions
Auditory training for CI users appears to be beneficial in improving various measures of speech recognition and quality-of-life. However, the extant literature is markedly variable in training modality, outcome measure, and quality of reporting. These limitations impede making definitive conclusions regarding the efficacy of any specific form of auditory training. Interventions in the literature are also often nonrepresentative of clinically available forms of auditory training. As such, future prospective studies are necessary to optimize post-CI auditory training. However, given their low cost and risk, practitioners can offer general recommendations for auditory training in that both clinician- and patient-directed approaches appear to provide benefits for adult CI users.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gaylor, J.M.; Raman, G.; Chung, M.; Lee, J.; Rao, M.; Lau, J.; Poe, D.S. Cochlear implantation in adults: A systematic review and meta-analysis. JAMA Otolaryngol.-Head Neck Surg. 2013, 139, 265–272. [Google Scholar] [CrossRef] [PubMed]
- McRackan, T.R.; Bauschard, M.; Hatch, J.L.; Franko-Tobin, E.; Droghini, H.R.; Nguyen, S.A.; Dubno, J.R. Meta-analysis of quality-of-life improvement after cochlear implantation and associations with speech recognition abilities. Laryngoscope 2018, 128, 982–990. [Google Scholar] [CrossRef]
- Gomaa, N.A.; Rubinstein, J.T.; Lowder, M.W.; Tyler, R.S.; Gantz, B.J. Residual speech perception and cochlear implant performance in postlingually deafened adults. Ear Hear. 2003, 24, 539–544. [Google Scholar] [CrossRef]
- Rubinstein, J.T.; Parkinson, W.S.; Tyler, R.S.; Gantz, B.J. Residual speech recognition and cochlear implant performance: Effects of implantation criteria. Am. J. Otol. 1999, 20, 445–452. [Google Scholar] [PubMed]
- Dietz, A.; Buschermohle, M.; Sivonen, V.; Willberg, T.; Aarnisalo, A.A.; Lenarz, T.; Kollmeier, B. Characteristics and international comparability of the Finnish matrix sentence test in cochlear implant recipients. Int. J. Audiol. 2015, 54 (Suppl. 2), 80–87. [Google Scholar] [CrossRef] [PubMed]
- Firszt, J.B.; Holden, L.K.; Skinner, M.W.; Tobey, E.A.; Peterson, A.; Gaggl, W.; Runge-Samuelson, C.L.; Wackym, P.A. Recognition of speech presented at soft to loud levels by adult cochlear implant recipients of three cochlear implant systems. Ear Hear. 2004, 25, 375–387. [Google Scholar] [CrossRef] [PubMed]
- Gifford, R.H.; Shallop, J.K.; Peterson, A.M. Speech recognition materials and ceiling effects: Considerations for cochlear implant programs. Audiol. Neuro-Otol. 2008, 13, 193–205. [Google Scholar] [CrossRef]
- Holden, L.K.; Finley, C.C.; Firszt, J.B.; Holden, T.A.; Brenner, C.; Potts, L.G.; Gotter, B.D.; Vanderhoof, S.S.; Mispagel, K.; Heydebrand, G.; et al. Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 2013, 34, 342–360. [Google Scholar] [CrossRef]
- Boothroyd, A. Adult aural rehabilitation: What is it and does it work? Trends Amplif. 2007, 11, 63–71. [Google Scholar] [CrossRef]
- Harris, M.S.; Capretta, N.R.; Henning, S.C.; Feeney, L.; Pitt, M.A.; Moberly, A.C. Postoperative Rehabilitation Strategies Used by Adults With Cochlear Implants: A Pilot Study. Laryngoscope Investig. Otolaryngol. 2016, 1, 42–48. [Google Scholar] [CrossRef]
- Humes, L.E.; Burk, M.H.; Strauser, L.E.; Kinney, D.L. Development and efficacy of a frequent-word auditory training protocol for older adults with impaired hearing. Ear Hear. 2009, 30, 613–627. [Google Scholar] [CrossRef] [PubMed]
- Raman, G.; Lee, J.; Chung, M.; Gaylor, J.M.; Rao, M.; Lau, J.; Poe, D.S.; Neault, M.W. Effectiveness of Cochlear Implants in Adults with Sensorineural Hearing Loss [Internet]. Available online: https://www.cms.gov/medicare/coverage/determinationprocess/downloads/id80ta.pdf (accessed on 15 July 2023).
- Stacey, P.C.; Raine, C.H.; O’Donoghue, G.M.; Tapper, L.; Twomey, T.; Summerfield, A.Q. Effectiveness of computer-based auditory training for adult users of cochlear implants. Int J Audiol. 2010, 49, 347–356. [Google Scholar] [CrossRef]
- Fu, Q.-J.; Galvin, J.J., 3rd. Maximizing cochlear implant patients’ performance with advanced speech training procedures. Hear. Res. 2008, 242, 198–208. [Google Scholar] [CrossRef]
- Fu, Q.-J.; Galvin, J.J., 3rd. Perceptual learning and auditory training in cochlear implant recipients. Trends Amplif. 2007, 11, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Gifford, R.H.; Noble, J.H.; Camarata, S.M.; Sunderhaus, L.W.; Dwyer, R.T.; Dawant, B.M.; Dietrich, M.S.; Labadie, R.F. The Relationship Between Spectral Modulation Detection and Speech Recognition: Adult Versus Pediatric Cochlear Implant Recipients. Trends Hear. 2018, 22, 2331216518771176. [Google Scholar] [CrossRef] [PubMed]
- Manrique, M.J.; Espinosa, J.M.; Huarte, A.; Molina, M.; Garcia-Tapia, R.; Artieda, J. Cochlear implants in post-lingual persons: Results during the first five years of the clinical course. Acta Otorrinolaringol. Esp. 1998, 49, 19–24. [Google Scholar]
- Dillon, M.T.; Buss, E.; Adunka, M.C.; King, E.R.; Pillsbury, H.C., 3rd; Adunka, O.F.; Buchman, C.A. Long-term speech perception in elderly cochlear implant users. JAMA Otolaryngol.-Head Neck Surg. 2013, 139, 279–283. [Google Scholar] [CrossRef]
- Reis, M.; Boisvert, I.; Beedell, E.; Mumford, V. Auditory Training for Adult Cochlear Implant Users: A Survey and Cost Analysis Study. Ear Hear. 2019, 40, 1445–1456. [Google Scholar] [CrossRef]
- Fu, Q.J.; Galvin, J.; Wang, X.; Nogaki, G. Effects of auditory training on adult cochlear implant patients: A preliminary report. Cochlear Implant. Int. 2004, 5 (Suppl. 1), 84–90. [Google Scholar] [CrossRef]
- Dornhoffer, J.R.; Reddy, P.; Ma, C.; Schvartz-Leyzac, K.C.; Dubno, J.R.; McRackan, T.R. Use of Auditory Training and Its Influence on Early Cochlear Implant Outcomes in Adults. Otol. Neurotol. 2022, 43, e165–e173. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Miller, S.A.; Forrest, J.L. Enhancing your practice through evidence-based decision making: PICO, learning how to ask good questions. J. Evid. Based Dent. Pract. 2001, 1, 136–141. [Google Scholar] [CrossRef]
- Cambridge, G.; Taylor, T.; Arnott, W.; Wilson, W.J. Auditory training for adults with cochlear implants: A systematic review. Int. J. Audiol. 2022, 61, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Henshaw, H.; Ferguson, M.A. Efficacy of individual computer-based auditory training for people with hearing loss: A systematic review of the evidence. PLoS ONE 2013, 8, e62836. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T.; Haugh, M.C.; Henry, D.; et al. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef]
- Adriani, N.; Dimitris, M.; Georgia, S. How to interpret meta-analysis models: Fixed effect and random effects meta-analyses. Evid. Based Ment. Health 2014, 17, 64. [Google Scholar] [CrossRef]
- Tyler, R.S.; Witt, S.A.; Dunn, C.C.; Wang, W. Initial development of a spatially separated speech-in-noise and localization training program. J. Am. Acad. Audiol. 2010, 21, 390–403. [Google Scholar] [CrossRef]
- Barlow, N.; Purdy, S.C.; Sharma, M.; Giles, E.; Narne, V. The Effect of Short-Term Auditory Training on Speech in Noise Perception and Cortical Auditory Evoked Potentials in Adults with Cochlear Implants. Semin Hear. 2016, 37, 84–98. [Google Scholar] [CrossRef]
- Borel, S.; Dupré, S.; de Bergh, M.; Sterkers, O.; Mosnier, I.; Ferrary, E. Rehabilitation of telephone communication in cochlear-implanted adults. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 381–386. [Google Scholar] [CrossRef]
- Gagne, J.P.; Parnes, L.S.; LaRocque, M.; Hassan, R.; Vidas, S. Effectiveness of an intensive speech perception training program for adult cochlear implant recipients. Ann. Otol. Rhinol. Laryngol. 1991, 100, 700–707. [Google Scholar] [CrossRef]
- Green, T.; Faulkner, A.; Rosen, S. Computer-Based Connected-Text Training of Speech-in-Noise Perception for Cochlear Implant Users. Trends Hear. 2019, 23, 2331216519843878. [Google Scholar] [CrossRef]
- Ingvalson, E.M.; Lee, B.; Fiebig, P.; Wong, P.C. The effects of short-term computerized speech-in-noise training on postlingually deafened adult cochlear implant recipients. J. Speech Lang. Hear. Res. JSLHR 2013, 56, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Kerneis, S.; Galvin, J.J., 3rd; Borel, S.; Baqué, J.; Fu, Q.J.; Bakhos, D. Preliminary evaluation of computer-assisted home training for French cochlear implant recipients. PLoS ONE 2023, 18, e0285154. [Google Scholar] [CrossRef]
- Oba, S.I.; Fu, Q.J.; Galvin, J.J., 3rd. Digit training in noise can improve cochlear implant users’ speech understanding in noise. Ear Hear. 2011, 32, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Shafiro, V.; Sheft, S.; Kuvadia, S.; Gygi, B. Environmental Sound Training in Cochlear Implant Users. J. Speech Lang. Hear. Res. 2015, 58, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Völter, C.; Stöckmann, C.; Schirmer, C.; Dazert, S. Tablet-Based Telerehabilitation Versus Conventional Face-to-Face Rehabilitation After Cochlear Implantation: Prospective Intervention Pilot Study. JMIR Rehabil. Assist. Technol. 2021, 8, e20405. [Google Scholar] [CrossRef]
- Zhang, T.; Dorman, M.F.; Fu, Q.J.; Spahr, A.J. Auditory training in patients with unilateral cochlear implant and contralateral acoustic stimulation. Ear Hear. 2012, 33, e70–e79. [Google Scholar] [CrossRef]
- Schumann, A.; Serman, M.; Gefeller, O.; Hoppe, U. Computer-based auditory phoneme discrimination training improves speech recognition in noise in experienced adult cochlear implant listeners. Int. J. Audiol. 2015, 54, 190–198. [Google Scholar] [CrossRef]
- Reynard, P.; Attina, V.; Idriss, S.; Hermann, R.; Barilly, C.; Veuillet, E.; Joly, C.A.; Thai-Van, H. Effect of Serious Gaming on Speech-in-Noise Intelligibility in Adult Cochlear Implantees: A Randomized Controlled Study. J. Clin. Med. 2022, 11, 2880. [Google Scholar] [CrossRef]
- Reis, M.; McMahon, C.M.; Távora-Vieira, D.; Humburg, P.; Boisvert, I. Effectiveness of Computer-Based Auditory Training for Adult Cochlear Implant Users: A Randomized Crossover Study. Trends Hear. 2021, 25, 23312165211025938. [Google Scholar] [CrossRef]
- Miller, J.D.; Watson, C.S.; Kistler, D.J.; Wightman, F.L.; Preminger, J.E. Preliminary evaluation of the speech perception assessment and training system (SPATS) with hearing-aid and cochlear-implant users. Proc. Meet Acoust. 2008, 2, 1–9. [Google Scholar] [CrossRef]
- Magits, S.; Boon, E.; De Meyere, L.; Dierckx, A.; Vermaete, E.; Francart, T.; Verhaert, N.; Wouters, J.; van Wieringen, A. Comparing the Outcomes of a Personalized Versus Nonpersonalized Home-Based Auditory Training Program for Cochlear Implant Users. Ear Hear. 2023, 44, 477–493. [Google Scholar] [CrossRef]
- Ihler, F.; Blum, J.; Steinmetz, G.; Weiss, B.G.; Zirn, S.; Canis, M. Development of a home-based auditory training to improve speech recognition on the telephone for patients with cochlear implants: A randomised trial. Clin. Otolaryngol. 2017, 42, 1303–1310. [Google Scholar] [CrossRef]
- Bernstein, C.M.; Brewer, D.M.; Bakke, M.H.; Olson, A.D.; Machmer, E.J.; Spitzer, J.B.; Schauer, P.C.; Sydlowski, S.A.; Levitt, H. Maximizing Cochlear Implant Outcomes with Short-Term Aural Rehabilitation. J. Am. Acad. Audiol. 2021, 32, 144–156. [Google Scholar] [CrossRef]
- Miller, S.E.; Zhang, Y.; Nelson, P.B. Efficacy of Multiple-Talker Phonetic Identification Training in Postlingually Deafened Cochlear Implant Listeners. J. Speech Lang. Hear. Res. JSLHR 2016, 59, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Moberly, A.C.; Vasil, K.; Baxter, J.; Klamer, B.; Kline, D.; Ray, C. Comprehensive auditory rehabilitation in adults receiving cochlear implants: A pilot study. Laryngoscope Investig. Otolaryngol. 2020, 5, 911–918. [Google Scholar] [CrossRef] [PubMed]
- McRackan, T.R.; Hand, B.N.; Velozo, C.A.; Dubno, J.R. Cochlear Implant Quality of Life (CIQOL): Development of a Profile Instrument (CIQOL-35 Profile) and a Global Measure (CIQOL-10 Global). J. Speech Lang. Hear. Res. JSLHR 2019, 62, 3554–3563. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.M.; Alexander, G.C. The abbreviated profile of hearing aid benefit. Ear Hear. 1995, 16, 176–186. [Google Scholar] [CrossRef]
- Hendry, J.; Chin, A.; Swan, I.R.; Akeroyd, M.A.; Browning, G.G. The Glasgow Benefit Inventory: A systematic review of the use and value of an otorhinolaryngological generic patient-recorded outcome measure. Clin. Otolaryngol. 2016, 41, 259–275. [Google Scholar] [CrossRef]
- Cassarly, C.; Matthews, L.J.; Simpson, A.N.; Dubno, J.R. The Revised Hearing Handicap Inventory and Screening Tool Based on Psychometric Reevaluation of the Hearing Handicap Inventories for the Elderly and Adults. Ear Hear. 2020, 41, 95–105. [Google Scholar] [CrossRef]
- Hinderink, J.B.; Krabbe, P.F.; Van Den Broek, P. Development and application of a health-related quality-of-life instrument for adults with cochlear implants: The Nijmegen cochlear implant questionnaire. Otolaryngol.-Head Neck Surg. Off. J. Am. Acad. Otolaryngol.—Head Neck Surg. 2000, 123, 756–765. [Google Scholar] [CrossRef] [PubMed]
- Bench, J.; Kowal, A.; Bamford, J. The BKB (Bamford-Kowal-Bench) sentence lists for partially-hearing children. Br. J. Audiol. 1979, 13, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, C.S.; Anderson, K.L. The Quality of Life Scale (QOLS): Reliability, validity, and utilization. Health Qual Life Outcomes 2003, 1, 60. [Google Scholar] [CrossRef]
- Sweetow, R.; Palmer, C.V. Efficacy of individual auditory training in adults: A systematic review of the evidence. J. Am. Acad. Audiol 2005, 16, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Rayes, H.; Al-Malky, G.; Vickers, D. Systematic Review of Auditory Training in Pediatric Cochlear Implant Recipients. J. Speech Lang. Hear. Res. JSLHR 2019, 62, 1574–1593. [Google Scholar] [CrossRef]
- Ma, C.; Fried, J.; Nguyen, S.A.; Schvartz-Leyzac, K.C.; Camposeo, E.L.; Meyer, T.A.; Dubno, J.R.; McRackan, T.R. Longitudinal Speech Recognition Changes After Cochlear Implant: Systematic Review and Meta-analysis. Laryngoscope 2023, 133, 1014–1024. [Google Scholar] [CrossRef]
- Adunka, O.F.; Gantz, B.J.; Dunn, C.; Gurgel, R.K.; Buchman, C.A. Minimum Reporting Standards for Adult Cochlear Implantation. Otolaryngol.-Head Neck Surg. Off. J. Am. Acad. Otolaryngol.-Head Neck Surg. 2018, 159, 215–219. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).