Abstract
Background: Chronic kidney disease (CKD) is a significant public health issue globally. The importance of its timely identification and early intervention is paramount. However, a systematic approach for early CKD management in the primary care setting is currently lacking, receiving less attention compared to upstream risk factors such as diabetes and hypertension. This oversight may lead to a failure in meeting quality-of-care indicators. Digital health interventions (DHIs), which leverage digital tools to enhance healthcare delivery, have shown effectiveness in managing chronic diseases and improving the quality, safety, and efficiency of primary care. Our research aimed to evaluate the effectiveness of DHIs in the care process, focusing on their reach, uptake, and feasibility. Methods: In this systematic review and meta-analysis, we searched PubMed, Embase, Cochrane Central Register of Controlled Trials, Web of Science, and ClinicalTrials.gov for randomized controlled trials (RCTs) assessing DHIs’ effectiveness in CKD patient care among adults in primary care settings. The search, conducted on 30 June 2023, included studies published in English from 1 January 2009. Screening was conducted using Covidence, adhering to Cochrane’s guidelines for data extraction. We primarily evaluated changes in care processes (testing, documentation, medication use, etc.) and the use of renin–angiotensin–aldosterone system inhibitors (RAASi), referrals, among others. Multilevel meta-analysis was employed to address within-study clustering, and meta-regression analyzed the impact of study characteristics on heterogeneity in effect sizes. Clinical endpoints were recorded where available. Bias risk was assessed using the Cochrane Risk of Bias 2 tool. Data on reach, uptake, and feasibility were narratively summarized. The study is registered with PROSPERO (CRD42023449098). Results: From 679 records, 12 RCTs were included in the narrative synthesis, and 6 studies (encompassing 7 trials) in the meta-analysis. The trials indicated a −0.85% change (95%CI, −5.82% to 4.11%) in the proportion of patients receiving desired care. This result showed considerable heterogeneity (I2 = 91.9%). One study characteristic (co-intervention, education) correlated with larger effects. Although including co-intervention in multivariable meta-regression was significant, it did not diminish heterogeneity. The reported reach varied and was not high, while the uptake was relatively high. Most studies did not explicitly address feasibility, though some statements implied its evaluation. Conclusions: The current literature on the impact of DHIs in community-based CKD care is limited. The studies suggest a non-significant effect of DHIs on enhancing CKD management in community settings, marked by significant heterogeneity. Future research should focus on rigorous, methodologically sound implementations to better assess the effectiveness of DHIs in the primary care management of CKD.
1. Introduction
Chronic kidney disease (CKD) is a leading public health problem worldwide. In 2017, the Global Burden Disease (GBD) project identified 697.5 million cases of all-stage CKD, with a prevalence of 9.1% (8.5–9.8). CKD has become a prominent noncommunicable cause of mortality worldwide [1]. By 2022, a joint statement indicated that the current number of individuals affected by CKD was estimated to be 843.6 million [2], approximately double the number of people living with diabetes (422 million) [3].
The significance of timely identification and early intervention in CKD cannot be overstated, as the advancement of CKD is associated with devastating clinical consequences such as end-stage kidney disease (ESKD), cardiovascular outcome, and increased death rates [4]. However, at present, there is no accepted systematic approach for the early management of CKD in primary care settings. CKD is usually insidious, with most affected individuals remaining asymptomatic until the disease becomes advanced. Furthermore, patients at high risk of disease development have a limited time window for therapeutic intervention before being referred to nephrology. This is because certain disease-modifying medications can only delay the progression of the disease, rather than prevent it entirely, consequently leading to higher rates of complications and mortality.
Moreover, kidney health receives significantly less focus compared to primary upstream risk factors such as diabetes and hypertension, both from public health authorities and the general population [5,6]. Primary care providers may be under-aware of current CKD treatment guidelines, potentially leading to a failure to meet quality-of-care indicators [7].
The primary healthcare system serves as a health gatekeeper and provides a foundation for policy and practice improvements to ensure the efficient delivery of high-quality primary healthcare. However, the focus on primary prevention and management for CKD remains suboptimal, especially in screening and care processes [8,9].
Digital health interventions (DHIs) [10] are technologies centered on delivering health services and information through digital and communication tools. They include a wide range of applications such as mobile health apps, wearable devices, telehealth or telemedicine services, and e-prescriptions. These interventions aim to improve patient care, support health professionals, enhance public health services, and optimize health system management. Their scope ranges from providing direct patient care and support to managing data and resources in healthcare settings. The widespread use of electronic health records (EHRs) in recent decades has led to the delivery of DHIs through information technology to improve the quality, safety, and efficiency of healthcare, particularly in primary care [10].
Previous reviews [11] have assessed the efficacy of digital health in the management of CKD. However, these reviews have not specifically addressed the impact on improving the process of care for CKD within a community setting, nor have they examined implementation indicators such as reach, uptake, and feasibility at the practical level.
To the best of our knowledge, this systematic review and meta-analysis is the first to synthesize the evidence on the effectiveness of DHIs for managing CKD in primary care settings. Our research aimed to evaluate the effectiveness of DHIs in the process of care and report on their reach, uptake, and feasibility.
2. Methods
2.1. Search Strategy and Selection Criteria
Our systematic review protocol, registered in PROSPERO (CRD42023449098), follows the 2020 PRISMA guidelines [12]. We conducted searches on PubMed, Embase, Cochrane Central Register of Controlled Trials, Web of Science, and ClinicalTrials.gov on 30 June 2023, using MeSH terms and broad search terms. We also manually searched the reference lists of related reviews on digital health interventions. The complete search is detailed in Supplementary Appendix S1.
Duplicates among the retrieved citations were removed using EndNote 20 (Thomson ResearchSoft, Stamford, CT, USA). The remaining full articles were then imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Two independent researchers (D.Z. and L.Y.) screened the titles and abstracts of the identified articles based on the predefined strategies. The full inclusion and exclusion criteria are listed in Supplementary Table S1. We considered randomized controlled trials (RCTs), cluster RCTs, pilot RCTs, and prospective RCTs conducted in adults within primary care settings that implemented digital health interventions (e.g., screening, diagnostic, medication adherence, and clinical outcome) and published in English from 1 January 2009 to 30 June 2023. Studies involving permanent dialysis treatment were excluded. Trials with control groups receiving substantial digital tool interventions were also excluded. Considering the relatively recent widespread adoption of digital health applications, the start date was set to 2009 to reflect contemporary practice [13]. The full texts of potentially relevant articles were independently assessed by the two reviewers. Discrepancies were resolved by arbitration from a third reviewer.
2.2. Outcomes
The Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) model framework guided our evaluation of implementation research [14]. We defined adoption or uptake as the reported action of using the intervention or health promotion program [14,15]. Our focus was primarily on the effectiveness in processes of care, such as testing, documentation, and medication use (e.g., renin–angiotensin–aldosterone system inhibitors (RAASi), referrals). However, we also recorded clinical outcomes, including intermediate endpoints like serum creatinine and blood pressure, when reported.
2.3. Data Extraction
The data extraction form, based on the Cochrane Handbook for Systematic Reviews of Interventions [16], was completed using Covidence systematic review software. For eligible articles, two reviewers independently extracted details including publication data, author information (names, affiliations, funding, and conflicts of interest), study characteristics (start and end date, country, design, purpose, blinding and randomization method, retention rate, and statistical analyses), participant demographics (condition of kidney disease, severity of disease, comorbidities, inclusion and exclusion criteria, sample size, recruitment process, and demographics), intervention (type, duration, frequency, and primary and secondary outcomes) and comparison, results (timepoint for follow-up, and primary and secondary outcomes), and conclusions.
2.4. Quality Assessment
The risk of bias in the included studies was independently assessed by two reviewers using the Cochrane risk-of-bias version 2 tool. Considerations included the randomization process, deviations from intended interventions, missing outcome data, the measurement of outcomes, and the selection of reported result. We used the pertinent versions of the tool to appraise the quality in included RCTs and cluster RCTs. Discrepancies were resolved through discussion and consensus.
2.5. Evaluation of Reach, Uptake, and Feasibility of Interventions
Data on reach, uptake, and feasibility were extracted from studies reporting relevant information. Reach was defined as the intended audience’s contact with the intervention [17]. Feasibility encompassed acceptability, adherence, cost-effectiveness likelihood, and provider capacity to deliver the intervention [18]. Based on the Reach, Effectiveness, Adoption, Implementation, and Maintenance (RE-AIM) framework, adoption or uptake was defined as the reported action of taking up or making use of the intervention or health promotion program [14]. We considered reach and uptake at the individual intervention participant level.
2.6. Data Analysis
We used a multilevel meta-analysis to estimate absolute improvements in care processes between intervention and control groups, accounting for study heterogeneity and the clustering of multiple outcomes from the same patients. Clustered designs, which means assigning intervention levels to the provider group rather than to the individual patient, did not always report cluster-adjusted estimates. Our study considered clustering through multiplying the standard error of risk differences by the square root of the design effect [19]. For studies without reported intraclass correlation coefficients (ICCs), ICCs were imputed from a published database [20]. We calculated the median ICCs for process measures across the 139 studies in this database and applied the relevant value to a given study.
Univariate and multivariable meta-regression analyses were conducted to examine effects based on study characteristics. These analyses estimated the difference in absolute improvements reported between studies with and without each intervention. Furthermore, a meta-regression model was fitted, including covariates with a p value less than 0.1 from the univariate analyses. This was done to identify study and intervention features that predicted larger effects and to determine if heterogeneity could be reduced. We used the I2 statistic to summarize statistical heterogeneity. With regard to clinical endpoints, we performed a meta-analysis of changes in systolic blood pressure, which was the most commonly reported continuous clinical endpoint.
All statistical analyses were conducted using R Software, version 4.2.2 (R Foundation for Statistical Computing, Vienna, Australia). The Rma.mv function from the “metafor” library was utilized to fit all multilevel models.
3. Results
This study identified 679 records, comprising 669 from the database searches and 10 manually sourced from relevant systematic review citations. After eliminating 88 duplicates, title and abstract screening led to the exclusion of 591 records. Of the 61 records subjected to full-text examination, 1 was unavailable in full text. Screening the full text of 60 articles resulted in 48 exclusions, leaving 12 for inclusion in the review. These comprised six studies (encompassing seven trials) reporting on process of care outcome indicators (Figure 1).
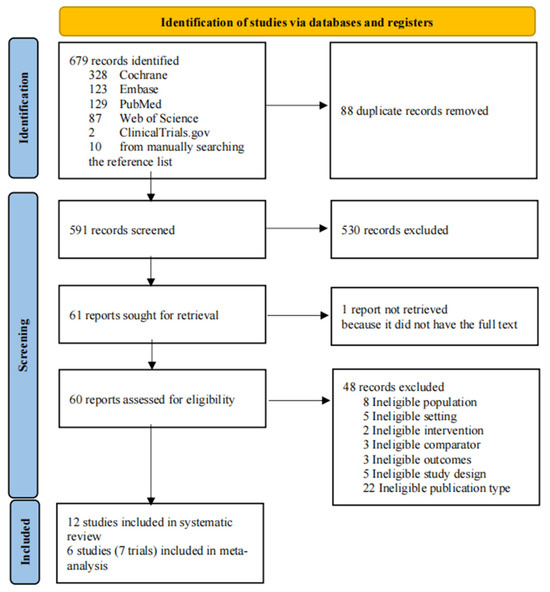
Figure 1.
Flow of studies through the review process.
The 12 studies primarily originated from the USA (n = 8), followed by 3 in Europe and 1 in Bangladesh. A majority (10 studies) were conducted from 2013 onwards, with the remaining 2 between 2009 and 2012. All studies utilized RCT designs, including one parallel, three cluster, and two 2 × 2 factorial designs. Interventions focused on patients in six studies, on providers in five, and on both in one study. Detailed information regarding the studies included in the analysis is presented in Supplementary Table S2.
Employing a multilevel meta-analysis model (Figure 2), we analyzed incremental improvements in the literature. The findings indicated that DHIs led to a non-significant overall absolute improvement of −0.85% (95% CI, −5.82% to 4.11%) in optimal process of care among patients compared to control groups. In terms of specific process of care characteristics, the referral rate showed a −3.14% difference (95% CI, −11.60% to 5.31%), the testing rates improved by 0.35% (95% CI, −7.21% to 6.50%), the CKD documentation by 5.49% (95% CI, −13.73% to 24.72%), and the medication use decreased by −2.66% (95% CI, −5.49% to 0.17%). Supplementary Figure S2 details models for each category.
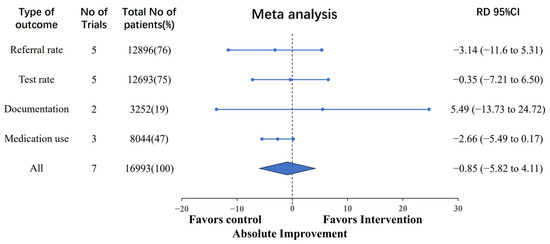
Figure 2.
Absolute changes in process of care by different categories of clinical care. Note. The “Referral rate” refers to the frequency of nephrology referrals. The “Test rate” encompasses assessments such as proteinuria evaluation, eGFR testing, hemoglobin measurement, serum phosphorus analysis, 25-Hydroxy vitamin D assessment, and parathyroid hormone measurement. The “Documentation” pertains to the recording of CKD information within the EMR. The “Medication use” signifies the prescription and utilization of ACE inhibitors/ARBs and statins.
The univariate meta-regression analyses (Table 1) revealed a 4.58% improvement (95% CI, −0.71% to 9.87%) in processes of care when education was a co-intervention, compared to a −4.69% change (95% CI, −9.42% to 0.04%) in studies without this aspect, a statistically significant difference (p = 0.01).

Table 1.
Absolute changes in process of care by study feature.
The multivariable regression analysis (Table 2), including co-intervention and follow-up time (both with p < 0.1 in the univariate regression), identified co-intervention (p = 0.03) as a significantly impacting process of care change. However, high heterogeneity persisted; the initial I2 was 91.9% and remained high at I2 = 87.3% even after accounting for co-intervention and follow-up time. Systolic blood pressure, the most reported continuous clinical endpoint [21,22,23,24], changed insignificantly by 2.32 mmHg (95%CI, −0.60 to 5.25) (Figure 3).
Table 2.
Multivariable meta-regression model for absolute changes in process of care by study feature.
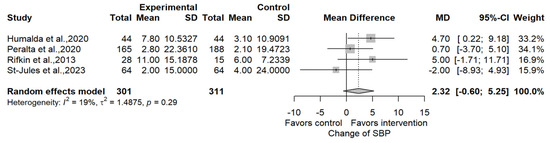
Figure 3.
Change in systolic blood pressure [21,22,23,24].
Sensitivity analyses using odds ratios instead of risk differences showed an overall odds ratio of 0.98 (95%CI, 0.77 to 1.25), underscoring the stability and robustness of conclusions when using odds ratios [25].
Regarding reach, uptake, and feasibility, six studies reported intervention reach with a median of 24.6% (range: 6.2–45), while four reported a median of 50% (range: 31.5–63.8) assigned to intervention groups (two studies did not report applicable reach) (Table 3). Intervention uptake, reported in five studies, had a median of 74% (range: 41–100). Although eight studies did not explicitly deem their interventions feasible, they reported effectiveness, reliability, high satisfaction, research participation willingness, and adherence. The authors’ interpretations of feasibility varied among studies, reflecting differences in feasibility measurement components.
Table 3.
Reach, uptake, and feasibility of the included studies.
4. Discussion
This systematic review synthesized evidence from 12 studies on the effectiveness, reach, uptake, and feasibility of DHIs in managing the care process of 23,945 patients with CKD in community settings. The meta-analysis of seven trials indicated no statistically significant difference in overall and specific care process elements compared to control groups. The reported reach was relatively low, and data on uptake were scarce.
Co-intervention (education) showed statistical significance in both the univariate and multivariate regression analyses. However, this factor did not fully account for the observed heterogeneity across studies. The overall heterogeneity was high at 91.9%, remaining substantial at 87.3% even after the multivariate regression. This suggests the presence of potential wide and non-random variations, the specific reasons for which are currently unknown.
A similar high level of heterogeneity was noted in other systematic reviews. Siopis et al. and Kwan et al. [34,35], who examined the impact of a clinical decision support system (CDSS) on desired care, reported substantial heterogeneity (I2 = 76% to 89%), with subgroup analyses unable to clarify the underlying causes. Other reviews [11,36] also failed to identify the origins of significant variations through subgroup analyses.
Several factors might explain the limited efficacy of DHIs. First, some studies [26,30] indicate that the intervention type employed is passive alert, wherein users can only access alert information by clicking on the relevant page, leading to the less frequent clicks and negative pronounced intervention effect. Conversely, pop-up alerts might cause user fatigue, impeding workflow integration. Second, the limited sample size and the patients of early stage CKD may have resulted in too small a number of patients progressing to the advanced stage, hence yielding no significant differences during the intervention monitoring period [22]. Therefore, it is recommended that future research should be undertaken to address the issues of sample size. Third, studies with patients mostly in CKD stages 3–5 [30] showed that referrals often focused on comorbidities rather than nephrology, suggesting a need to consider potential attrition when considering referrals. Fourth, two studies [29,32] indicated limited potential for enhancing DHI management due to high initial examination and medication levels in populations affiliated with university hospitals or general clinics with extensive eGFR implementation. Fifth, the limited CKD knowledge among users, especially primary care providers (PCPs), might lead to an underestimation of alerts and impact medical decision making [35]. Consequently, this can impact the communication between PCPs and patients during medical decision-making processes. Additionally, the active involvement of patients in the intervention process of a DHI is often contingent upon their knowledge of CKD management. As mentioned before, the meta-regression analysis identified potential predictors of Co-intervention (education), which aligns with the findings of a previous systematic review [35] emphasizing the significance of educating users during DHIs.
Lastly, within the community context, the efficacy of the DHIs is limited by various external circumstances. For instance, community-based DHIs face challenges like early CKD diagnosis and treatment awareness, adherence to guidelines, and time constraints for patient education [37,38].
The findings align with other scholarly sources. Stevenson et al. [11] and Galbraith et al. [39] found diverse eHealth intervention concepts and technologies, leading to insufficient evidence for efficacy recommendations. Kwan et al. [35] reported a modest increase in desired care element receipt due to CDSS, with education emerging as a significant predictive factor.
For future research and practical application, it is recommended to integrate alert systems effectively with user workflows. Second, future study should avoid restricting study populations to those with higher baseline levels. Third, when implementing the DHIs, it is crucial to prioritize the education of primary care providers (PCPs) and patients on the management of CKD. Fourth, further investigation should examine and resolve potential obstacles to the implementation of DHIs in a community-based context.
The limitations of the included studies must be acknowledged. First, there is significant heterogeneity among the studies, with differences in intervention types, objectives, and target populations. Second, most studies focused on short-term clinical parameters such as blood pressure and serum creatinine rather than longer term outcomes like hospitalization and mortality, due to the short duration of the RCTs. Third, the assessment of reach, uptake, and feasibility is not comprehensive, with future research needed to explore these aspects more thoroughly and develop robust evaluation frameworks. Additionally, it is important to acknowledge that the limited number of studies incorporated in the meta-analysis and meta-regression within this review may impact the power of the data analysis findings. Therefore, it is advisable to interpret the conclusions of this study with caution.
In conclusion, the current literature on DHIs in community-based CKD care suggests limited efficacy and considerable heterogeneity. Future research should focus on methodologically sound implementations to assess the effectiveness of DHIs in primary care CKD management more rigorously.
In terms of the risk of bias of the studies, three studies were classified at high risk of bias, five at moderate risk, and four at low risk (Supplementary Figure S1). Two studies [24,30] were high-risk due to unblinded intervention allocation, and one study [28] was high-risk due to unblinded outcome measurement. Four studies had moderate risk due to potential randomization process issues, and four either lacked or did not mention blinding in the allocation process.
5. Conclusions
The literature on the impact of DHIs in community-based CKD care is limited. Existing studies indicate that the efficacy of DHIs in enhancing CKD management is not significant and exhibits considerable heterogeneity. Future research should undertake rigorous and methodologically sound investigations to examine DHIs’ effectiveness in CKD management within primary care more effectively.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcm13020364/s1.
Author Contributions
Conceptualization, M.H. and J.L.; methodology, M.H. and D.Z.; software, M.H., D.Z. and L.Y. (Lili Ye); validation, D.Z., L.Y. (Lili Ye) and M.H.; formal analysis, L.Y. (Lili Ye) and D.Z.; investigation, D.Z., L.Y. (Lili Ye) and M.H.; resources, M.H.; data curation, D.Z.; writing—original draft preparation, D.Z. and M.H.; writing—review and editing, M.H. and D.Z.; visualization, L.Y. (Lili Ye), D.Z. and M.H.; supervision, M.H.; project administration, M.H.; funding acquisition, J.L. and L.Y. (Li Yang) All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by grants from the Beijing Nova Program (2021051), the Fundamental Research Funds for the Central Universities, Peking University Clinical Scientists Program (BMU2023PYJH023), the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-046), the Beijing Young Scientist Program (BJJWZYJH01201910001006) and the Capital Health Development Scientific Research Project (2022-1-4071).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article and Supplementary Material, further inquiries can be directed to the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Report on Diabetes: World Health Organization; Report No.: 9789241565257; WHO: Geneva, Switzerland, 2016.
- Matsushita, K.; Coresh, J.; Sang, Y.; Chalmers, J.; Fox, C.; Guallar, E.; Jafar, T.; Jassal, S.K.; Landman, G.W.D.; Muntner, P.; et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: A collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2015, 3, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Tummalapalli, S.L.; Vittinghoff, E.; Crews, D.C.; Cushman, M.; Gutiérrez, O.M.; Judd, S.E.; Kramer, H.J.; Peralta, C.A.; Tuot, D.S.; Shlipak, M.G.; et al. Chronic Kidney Disease Awareness and Longitudinal Health Outcomes: Results from the reasons for Geographic And Racial Differences in Stroke Study. Am. J. Nephrol. 2020, 51, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.D.; McCulloch, C.E.; Banerjee, T.; Pavkov, M.E.; Gillespie, B.W.; Saran, R.; Shlipak, M.G.; Powe, N.R.; Tuot, D.S.; Shahinian, V.; et al. CKD Awareness Among US Adults by Future Risk of Kidney Failure. Am. J. Kidney Dis. 2020, 76, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Bello, A.K.; Ronksley, P.E.; Tangri, N.; Kurzawa, J.; Osman, M.A.; Singer, A.; Grill, A.K.; Nitsch, D.; Queenan, J.A.; Wick, J.; et al. Quality of Chronic Kidney Disease Management in Canadian Primary Care. JAMA Netw. Open 2019, 2, e1910704. [Google Scholar] [CrossRef] [PubMed]
- Stempniewicz, N.; Vassalotti, J.A.; Cuddeback, J.K.; Ciemins, E.; Storfer-Isser, A.; Sang, Y.; Matsushita, K.; Ballew, S.H.; Chang, A.R.; Levey, A.S.; et al. Chronic Kidney Disease Testing Among Primary Care Patients With Type 2 Diabetes Across 24 U.S. Health Care Organizations. Diabetes Care 2021, 44, 2000–2009. [Google Scholar] [CrossRef]
- Alfego, D.; Ennis, J.; Gillespie, B.; Lewis, M.J.; Montgomery, E.; Ferrè, S.; Vassalotti, J.A.; Letovsky, S. Chronic Kidney Disease Testing Among At-Risk Adults in the U.S. Remains Low: Real-World Evidence From a National Laboratory Database. Diabetes Care 2021, 44, 2025–2032. [Google Scholar] [CrossRef]
- Sheikh, A.; Anderson, M.; Albala, S.; Casadei, B.; Franklin, B.D.; Richards, M.; Taylor, D.; Tibble, H.; Mossialos, E. Health information technology and digital innovation for national learning health and care systems. Lancet Digit. Health 2021, 3, e383–e396. [Google Scholar] [CrossRef]
- Stevenson, J.K.; Campbell, Z.C.; Webster, A.C.; Chow, C.K.; Tong, A.; Craig, J.C.; Campbell, K.L.; Lee, V.W.S. eHealth interventions for people with chronic kidney disease. Cochrane Database Syst. Rev. 2019, 8, Cd012379. [Google Scholar] [CrossRef]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; A Akl, E.; E Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Dicianno, B.E.; Parmanto, B.; Fairman, A.D.; Crytzer, T.M.; Yu, D.X.; Pramana, G.; Coughenour, D.; Petrazzi, A.A. Perspectives on the evolution of mobile (mHealth) technologies and application to rehabilitation. Phys. Ther. 2015, 95, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Harden, S.M.; Gaglio, B.; Rabin, B.; Smith, M.L.; Porter, G.C.; Ory, M.G.; Estabrooks, P.A. RE-AIM Planning and Evaluation Framework: Adapting to New Science and Practice With a 20-Year Review. Front. Public Health 2019, 7, 64. [Google Scholar] [CrossRef]
- Proctor, E.; Silmere, H.; Raghavan, R.; Hovmand, P.; Aarons, G.; Bunger, A.; Griffey, R.; Hensley, M. Outcomes for implementation research: Conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health 2011, 38, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0. 2019. Available online: https://training.cochrane.org/handbook/archive/v6 (accessed on 18 November 2022).
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed]
- Skivington, K.; Matthews, L.; Simpson, S.; Craig, P.; Baird, J.; Blazeby, J.; Boyd, K.; Craig, N.; French, D.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4. Available online: https://www.training.cochrane.org/handbook (accessed on 2 August 2023).
- University of Aberdeen Health Services Research Unit Research Tools. Database of Intra-Correlation coe0 Cients (ICCs). Available online: https://www.abdn.ac.uk/hsru/what-we-do/tools/index.php (accessed on 21 March 2019).
- Humalda, J.K.; Klaassen, G.; de Vries, H.; Meuleman, Y.; Verschuur, L.C.; Straathof, E.J.; Laverman, G.D.; Bos, W.J.W.; van der Boog, P.J.; Vermeulen, K.M.; et al. A Self-management Approach for Dietary Sodium Restriction in Patients With CKD: A Randomized Controlled Trial. Am. J. Kidney Dis. 2020, 75, 847–856. [Google Scholar] [CrossRef]
- Peralta, C.A.; Livaudais-Toman, J.; Stebbins, M.; Lo, L.; Robinson, A.; Pathak, S.; Scherzer, R.; Karliner, L.S. Electronic Decision Support for Management of CKD in Primary Care: A Pragmatic Randomized Trial. Am. J. Kidney Dis. 2020, 76, 636–644. [Google Scholar] [CrossRef]
- Rifkin, D.E.; Abdelmalek, J.A.; Miracle, C.M.; Low, C.; Barsotti, R.; Rios, P.; Stepnowsky, C.; Agha, Z. Linking clinic and home: A randomized, controlled clinical effectiveness trial of real-time, wireless blood pressure monitoring for older patients with kidney disease and hypertension. Blood Press. Monit. 2013, 18, 8–15. [Google Scholar] [CrossRef]
- St-Jules, D.E.; Hu, L.; Woolf, K.; Wang, C.; Goldfarb, D.S.; Katz, S.D.; Popp, C.; Williams, S.K.; Li, H.; Jagannathan, R.; et al. An Evaluation of Alternative Technology-Supported Counseling Approaches to Promote Multiple Lifestyle Behavior Changes in Patients With Type 2 Diabetes and Chronic Kidney Disease. J. Ren. Nutr. 2023, 33, 35–44. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Guyatt, G.H.; Griffith, L.E. Griffith Can we individualize the ‘number needed to treat’? An empirical study of summary effect measures in meta-analyses. Int. J. Epidemiol. 2002, 31, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Kader, K.; Fischer, G.S.; Li, J.; Moore, C.G.; Hess, R.; Unruh, M.L. Automated clinical reminders for primary care providers in the care of CKD: A small cluster-randomized controlled trial. Am. J. Kidney Dis. 2011, 58, 894–902. [Google Scholar] [CrossRef]
- Bhardwaja, B.; Carroll, N.M.; Raebel, M.A.; Chester, E.A.; Korner, E.J.; Rocho, B.E.; Brand, D.W.; Magid, D.J. Improving Prescribing Safety in Patients with Renal Insufficiency in the Ambulatory Setting: The Drug Renal Alert Pharmacy (DRAP) Program. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2011, 31, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Blakeman, T.; Blickem, C.; Kennedy, A.; Reeves, D.; Bower, P.; Gaffney, H.; Gardner, C.; Lee, V.; Jariwala, P.; Dawson, S.; et al. Effect of information and telephone-guided access to community support for people with chronic kidney disease: Randomised controlled trial. PLoS ONE 2014, 9, e109135. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, S.D.; Jolly, S.E.; Schold, J.D.; Arrigain, S.; Nakhoul, G.; Konig, V.; Hyland, J.; Burrucker, Y.K.; Dann, P.D.; Tucky, B.H.; et al. Pragmatic Randomized, Controlled Trial of Patient Navigators and Enhanced Personal Health Records in CKD. Clin. J. Am. Soc. Nephrol. 2017, 12, 1418–1427. [Google Scholar] [CrossRef] [PubMed]
- Samal, L.; D’amore, J.D.; Gannon, M.P.; Kilgallon, J.L.; Charles, J.-P.; Mann, D.M.; Siegel, L.C.; Burdge, K.; Shaykevich, S.; Lipsitz, S.; et al. Impact of Kidney Failure Risk Prediction Clinical Decision Support on Monitoring and Referral in Primary Care Management of CKD: A Randomized Pragmatic Clinical Trial. Kidney Med. 2022, 4, 100493. [Google Scholar] [CrossRef] [PubMed]
- Sarker, M.H. A CKD Awareness Campaign and mHealth Education to Improve Knowledge and Quality of Life Among CKD Patients in Bangladesh: A Randomized Controlled Trial. J. Am. Soc. Nephrol. 2022, 33, 48–49. [Google Scholar]
- Sequist, T.D.; Holliday, A.M.; Orav, E.J.; Bates, D.W.; Denker, B.M. Physician and patient tools to improve chronic kidney disease care. Am. J. Manag. Care 2018, 24, e107–e114. [Google Scholar]
- van Gelder, V.A.; Scherpbier-de Haan, N.D.; van Berkel, S.; Akkermans, R.P.; de Grauw, I.S.; Adang, E.M.; Assendelft, P.J.; de Grauw, W.J.C.; Biermans, M.C.J.; Wetzels, J.F.M. Web-based consultation between general practitioners and nephrologists: A cluster randomized controlled trial. Fam. Pract. 2017, 34, 430–436. [Google Scholar] [CrossRef]
- Siopis, G.; Moschonis, G.; Eweka, E.; Jung, J.; Kwasnicka, D.; Asare, B.Y.-A.; Kodithuwakku, V.; Willems, R.; Verhaeghe, N.; Annemans, L.; et al. Effectiveness, reach, uptake, and feasibility of digital health interventions for adults with hypertension: A systematic review and meta-analysis of randomised controlled trials. Lancet Digit. Health 2023, 5, e144–e159. [Google Scholar] [CrossRef]
- Kwan, J.L.; Lo, L.; Ferguson, J.; Goldberg, H.; Diaz-Martinez, J.P.; Tomlinson, G.; Grimshaw, J.M.; Shojania, K.G. Computerised clinical decision support systems and absolute improvements in care: Meta-analysis of controlled clinical trials. BMJ 2020, 370, m3216. [Google Scholar] [CrossRef] [PubMed]
- Moschonis, G.; Siopis, G.; Jung, J.; Eweka, E.; Willems, R.; Kwasnicka, D.; Asare, B.Y.-A.; Kodithuwakku, V.; Verhaeghe, N.; Vedanthan, R.; et al. Effectiveness, reach, uptake, and feasibility of digital health interventions for adults with type 2 diabetes: A systematic review and meta-analysis of randomised controlled trials. Lancet Digit. Health 2023, 5, e125–e143. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, M.; Jiang, M.-Y.; Song, R.; Mothi, S.S.; Bellou, S.; Polding, L.C.; Li, J.; Cho, A.; Hsiao, L.-L. High Prevalence and Low Awareness of Albuminuria in the Community Setting in the KDSAP. Kidney Int. Rep. 2020, 5, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Dorgelo, A.; Oostrom, T.A.J. An integrated approach towards a public health perspective on chronic kidney disease. Nat. Rev. Nephrol. 2022, 18, 131–132. [Google Scholar] [CrossRef]
- Galbraith, L.; Jacobs, C.; Hemmelgarn, B.R.; Donald, M.; Manns, B.J.; Jun, M. Chronic disease management interventions for people with chronic kidney disease in primary care: A systematic review and meta-analysis. Nephrol. Dial. Transpl. 2018, 33, 112–121. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).