
Lumenless and Stylet-Driven Leads for Left Bundle Branch Area Pacing: Materials, Techniques, Benefits, and Trade-Offs of the Two Approaches



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. LBBP Lead Placement Technique
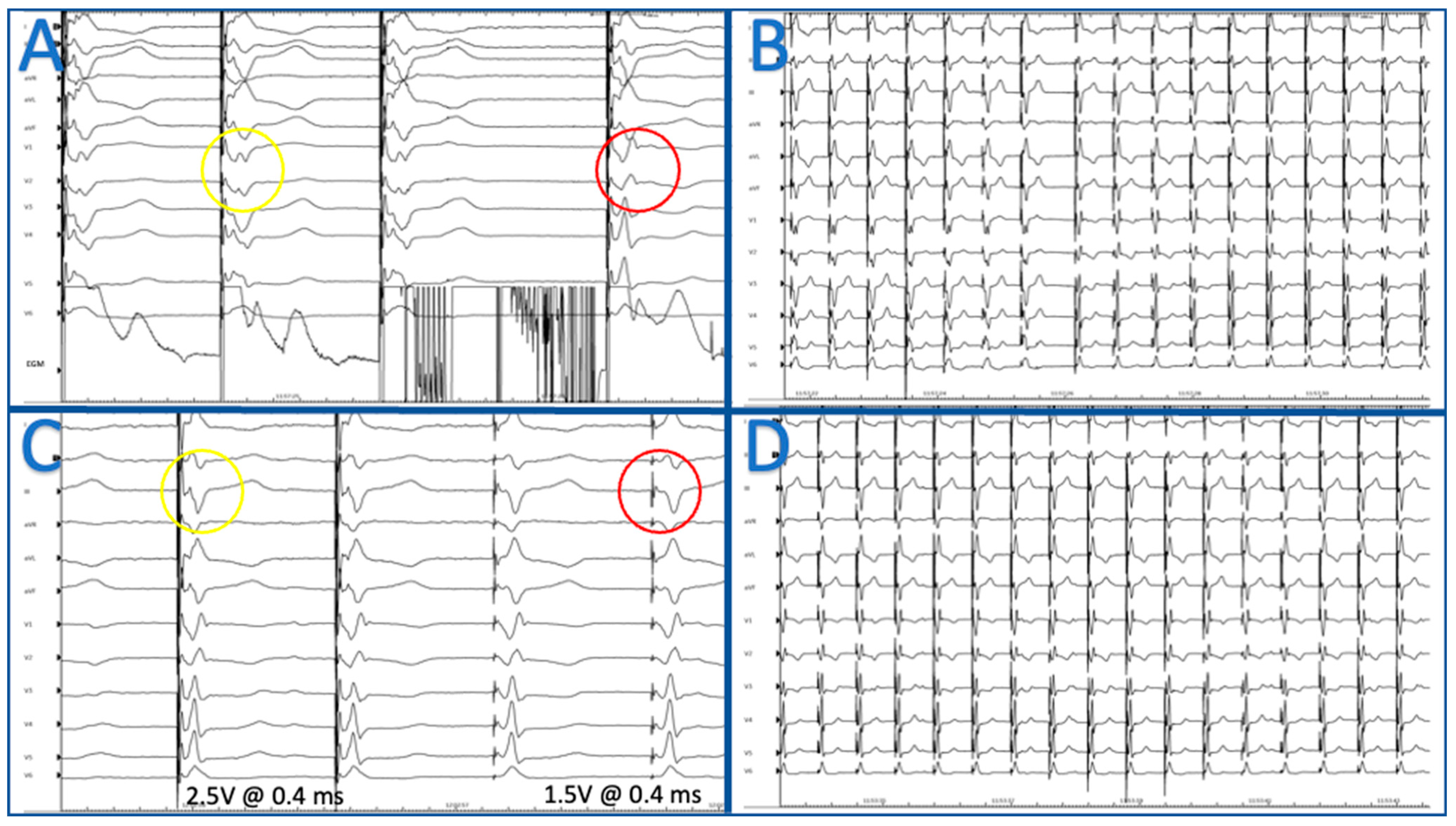
- QRS transition morphology during pacing thresholds;
- R wave peak time in V6 (V6RWPT) < 75 ms in case of native narrow QRS or RBBB; <80 ms in case of LBBB or asystole, or intra ventricular conduction delay with RBBB and fascicular block; in patients with severely dilated LV or conduction system disease, the accepted cutoff may be <90 ms;
- Measurement of V6–V1 inter-peak interval > 44 ms;
- -
- absence of local ventricular EGM capture into stimulus artifact with discrete isoe-lectric components on the paced bipole pair and immediately adjacent bipole pairs (2-mm interspacing) at EGM.
- -
- presence of an isoelectric interval between the pacing spike and ECG QRS complex.
- -
- the pacing spike–QRS interval closely approximates the left Purkinje potential to QRS interval.
- -
- direct capture of the local ventricular EGM into the pacing stimulus artifact with recruitment of ventricular components on the immediately adjacent bipole pairs (2-mm interspacing).
- -
- absence of isoelectric interval between the pacing spike and ECG QRS complex [8].
3. Lumenless Lead
3.1. Medtronic
3.2. Advantages
3.3. Limitations
4. Stylet-Driven Leads
4.1. Advantages
4.2. Limitations
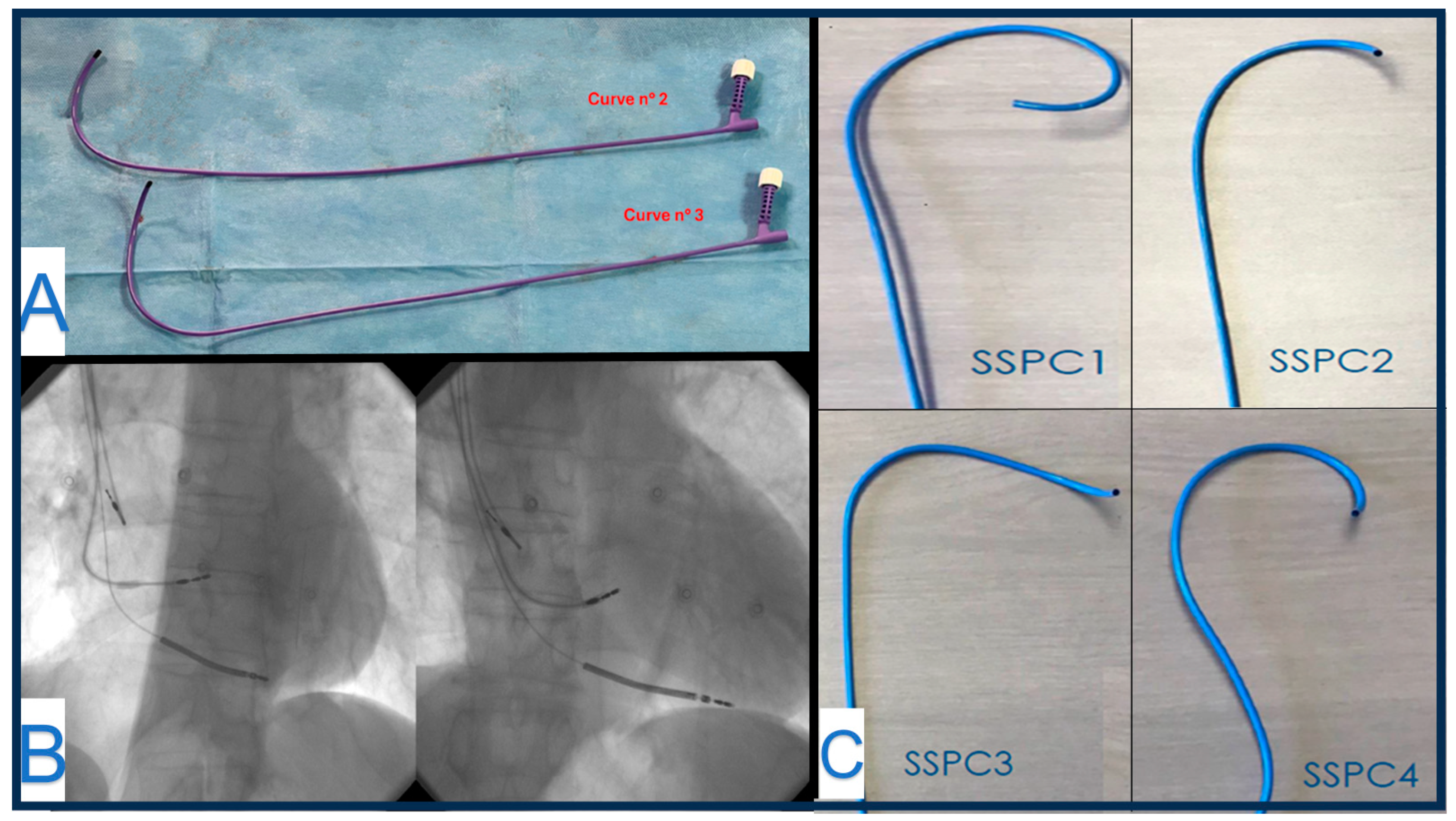
4.3. Solia S (Biotronik)
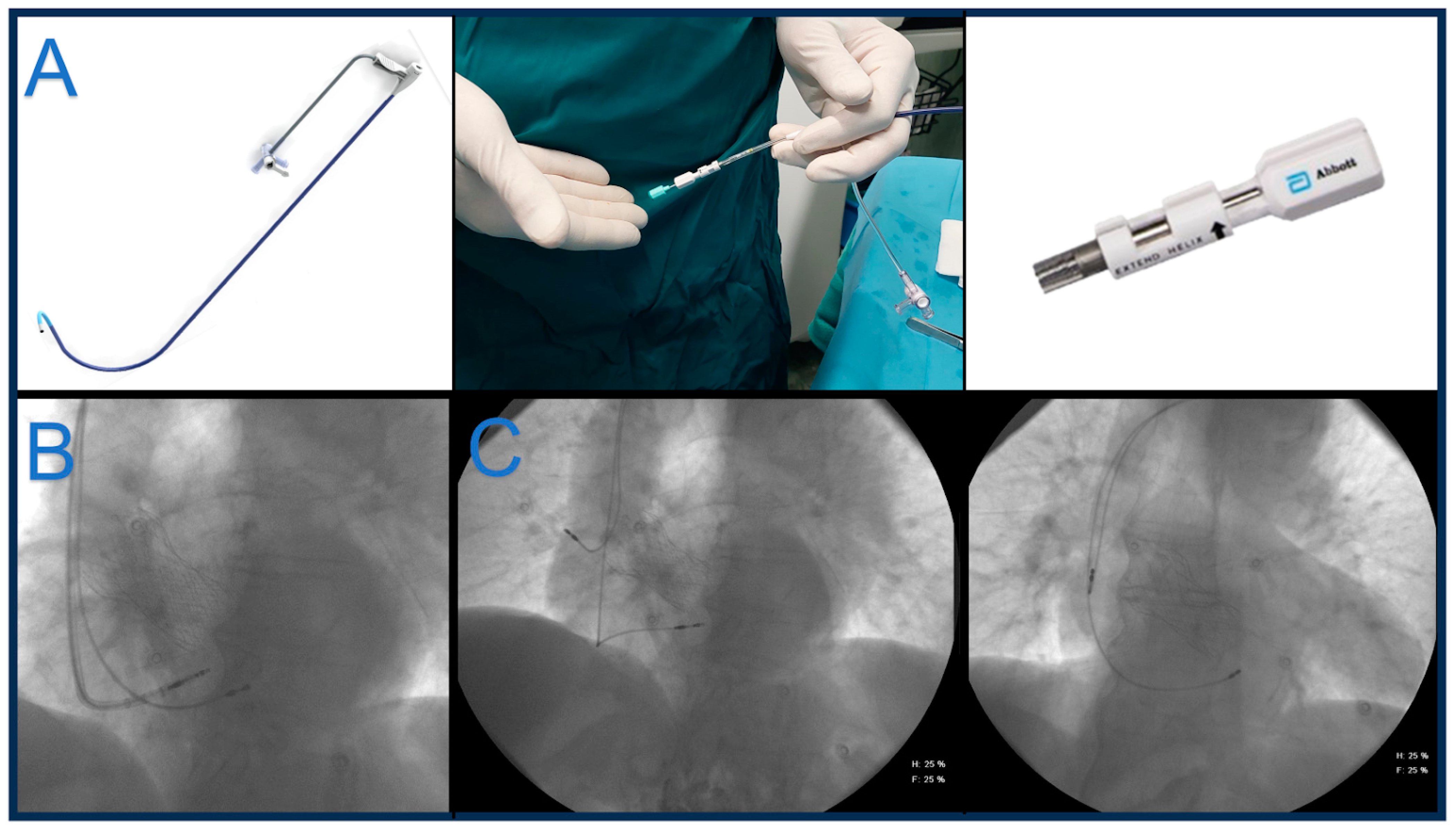
4.4. Tendril™ STS 2088TC (Abbott)
4.5. Ingevity + (Boston Scientific)
5. Potential Complications in LBBPa
- Septal perforation. Septal perforation is a common complication and is reported in up to 10.2% of LLL and 11.6% of SDL. The procedural outcome and follow-up of SDL compared with LLL for LBBPa can be diagnosed after a marked fall in the current of injury (COI) amplitude associated with a “QS” morphology, along with a drop in pacing impedance to <450 Ω. In the case of perforation, the lead can be advanced in the left ventricle and can evoke left ventricular ectopy. Pacing thresholds can rise.
- Macrodislodgment. Macroscopic dislodgment of the lead should be addressed as a technical problem during lead implantation (i.e., drill effect during screwing) and may lead to loss of capture. Lead displacement can be both in the right ventricle or left ventricle in the case of concomitant septal perforation.
- Microdislodgment. Per-operative microdislodgments are diagnosed in case of a change in morphology at surface 12 lead ECG, with a loss of terminal R’/r’ deflection in V1 and/or widening of the QRS.
- Lead rupture. Subtricuspidal friction of the lead may lead to lead rupture. The most common point of rupture is between the lead body and the ring [18,19]. LLL can be affected, too, and fractured leads in atypical locations can suggest that multiple attempts during initial lead implantation may be at a higher risk of lead fracture [20].
- Helix damage. Endocardium entanglement or deep septal penetration in thick myocardium can hamper tissue advancement, and counterclock rotations to retract the helix can be ineffective. Repositioning maneuvers are often necessary during LBBPa and can be a source of possible complications. In rare cases, helix elongation can precede helix rupture into the interventricular septum [13].
- Chest pain and ST elevation. Acute coronary events are rare occurrences during LBBPa implants (<1% of implants). They generally present with intraprocedural chest pain and possible ST elevation. Helix and lead retraction usually leads to symptom resolution. Coronary angiography is negative when performed in these cases. However, persistent ST elevation should also prompt suspicion of coronary vasospasm.
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hua, W.; Fan, X.; Li, X.; Niu, H.; Gu, M.; Ning, X.; Hu, Y.; Gold, M.R.; Zhang, S. Comparison of Left Bundle Branch and His Bundle Pacing in Bradycardia Patients. JACC Clin. Electrophysiol. 2020, 6, 1291–1299. [Google Scholar] [CrossRef] [PubMed]
- Cano, Ó.; Navarrete-Navarro, J.; Zalavadia, D.; Jover, P.; Osca, J.; Bahadur, R.; Izquierdo, M.; Navarro, J.; Subzposh, F.A.; Ayala, H.D.; et al. Acute performance of stylet driven leads for left bundle branch area pacing: A comparison with lumenless leads. Heart Rhythm O2 2023, 4, 765–776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sritharan, A.; Kozhuharov, N.; Masson, N.; Bakelants, E.; Valiton, V.; Burri, H. Procedural outcome and follow-up of stylet-driven leads compared with lumenless leads for left bundle branch area pacing. Europace 2023, 25, euad295. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, X.; Wei, L.; Bai, J.; Wang, W.; Qin, S.; Wang, J.; Liang, Y.; Su, Y.; Ge, J. Procedure-Related Complications of Left Bundle Branch Pacing: A Single-Center Experience. Front. Cardiovasc. Med. 2021, 8, 645947. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, J.; Wang, Z.; Zu, L.; Cheng, L.; Su, R.; Wang, X.; Liang, Z.; Chen, J.; Hang, F.; Du, J.; et al. Simplifying physiological left bundle branch area pacing using a new nine-partition method. Can. J. Cardiol. 2021, 37, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.K.; Ellenbogen, K.A. Left bundle branch pacing is the best approach to physiological pacing. Heart Rhythm O2 2020, 1, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, G.A. QRS morphologies in V1 and V6 during left bundle branch area pacing: Assessing the patterns. Europace 2023, 25, euad284. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Burri, H.; Jastrzebski, M.; Cano, Ó.; Čurila, K.; de Pooter, J.; Huang, W.; Israel, C.; Joza, J.; Romero, J.; Vernooy, K.; et al. EHRA clinical consensus statement on conduction system pacing implantation: Endorsed by the Asia Pacific Heart Rhythm Society (APHRS), Canadian Heart Rhythm Society (CHRS), and Latin American Heart Rhythm Society (LAHRS). Europace 2023, 25, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Upadhyay, G.A.; Tung, R. Influence of Capture Selectivity and Left Intrahisian Block on QRS Characteristics During Left Bundle Branch Pacing. JACC Clin Electrophysiol. 2022, 8, 635–647. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Chen, X.; Su, L.; Wu, S.; Xia, X.; Vijayaraman, P. A beginner’s guide to permanent left bundle branch pacing. Heart Rhythm 2019, 16, 1791–1796. [Google Scholar] [CrossRef] [PubMed]
- Ponnusamy, S.S.; Vijayaraman, P. My preferred approach to left bundle branch pacing: Lumenless leads. Heart Rhythm O2 2022, 4, 147–153. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zou, J.; Chen, K.; Liu, X.; Xu, Y.; Jiang, L.; Dai, Y.; Lin, J.; Hou, X.; Qiu, Y.; Himes, A.; et al. Clinical use conditions of lead deployment and simulated lead fracture rate in left bundle branch area pacing. J. Cardiovasc. Electrophysiol. 2023, 34, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Migliore, F.; Pittorru, R.; De Lazzari, M.; Tarzia, V.; Pastore, G.; Marcantoni, L.; Catanzariti, D.; Gerosa, G.; Zanon, F. Transvenous lead extraction of lumenless 3830 pacing lead in conduction system pacing: A single-center experience. J. Interv. Card. Electrophysiol. 2024, 67, 175–182. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Le Polain de Waroux, J.B.; Wielandts, J.Y.; Gillis, K.; Hilfiker, G.; Sorgente, A.; Capulzini, L.; Geerts, B.; Knecht, S.; Duytschaever, M.; Tavernier, R. Repositioning and extraction of stylet-driven pacing leads with extendable helix used for left bundle branch area pacing. J. Cardiovasc. Electrophysiol. 2021, 32, 1464–1466. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraman, P.; Subzposh, F.A.; Naperkowski, A. Extraction of the permanent His bundle pacing lead: Safety outcomes and feasibility of reimplantation. Heart Rhythm 2019, 16, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Zanon, F.; Marcantoni, L.; Pastore, G.; Baracca, E. Left bundle branch pacing by standard stylet-driven lead: Preliminary experience of two case reports. Heart Rhythm Case Rep. 2020, 6, 614–617. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- De Pooter, J.; Wauters, A.; Van Heuverswyn, F.; Le Polain de Waroux, J.B. A Guide to Left Bundle Branch Area Pacing Using Stylet-Driven Pacing Leads. Front. Cardiovasc. Med. 2022, 9, 844152. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Özpak, E.; Van Heuverswyn, F.; Timmermans, F.; De Pooter, J. Lead performance of stylet-driven leads in left bundle branch area pacing: Results from a large single-center cohort and insights from in-vitro bench testing. Heart Rhythm 2024, 21, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Thaler, R.; Sinner, M.F.; Joghetaei, N.; Fichtner, S. Early sudden distal conductor fracture of a stylet-driven lead implanted for left bundle branch area pacing. Heart Rhythm Case Rep. 2022, 9, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Rangaswamy, V.V.; Ponnusamy, S.S. Late distal conductor fracture of the lumenless pacing lead after left bundle branch area pacing. Heart Rhythm 2024, 21, 490–491. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taddeucci, S.; Mirizzi, G.; Santoro, A. Lumenless and Stylet-Driven Leads for Left Bundle Branch Area Pacing: Materials, Techniques, Benefits, and Trade-Offs of the Two Approaches. J. Clin. Med. 2024, 13, 4758. https://doi.org/10.3390/jcm13164758
Taddeucci S, Mirizzi G, Santoro A. Lumenless and Stylet-Driven Leads for Left Bundle Branch Area Pacing: Materials, Techniques, Benefits, and Trade-Offs of the Two Approaches. Journal of Clinical Medicine. 2024; 13(16):4758. https://doi.org/10.3390/jcm13164758
Chicago/Turabian StyleTaddeucci, Simone, Gianluca Mirizzi, and Amato Santoro. 2024. "Lumenless and Stylet-Driven Leads for Left Bundle Branch Area Pacing: Materials, Techniques, Benefits, and Trade-Offs of the Two Approaches" Journal of Clinical Medicine 13, no. 16: 4758. https://doi.org/10.3390/jcm13164758
APA StyleTaddeucci, S., Mirizzi, G., & Santoro, A. (2024). Lumenless and Stylet-Driven Leads for Left Bundle Branch Area Pacing: Materials, Techniques, Benefits, and Trade-Offs of the Two Approaches. Journal of Clinical Medicine, 13(16), 4758. https://doi.org/10.3390/jcm13164758