
Is a Low Dosage of Medical Cannabis Effective for Treating Pain Related to Fibromyalgia? A Pilot Study and Systematic Review

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
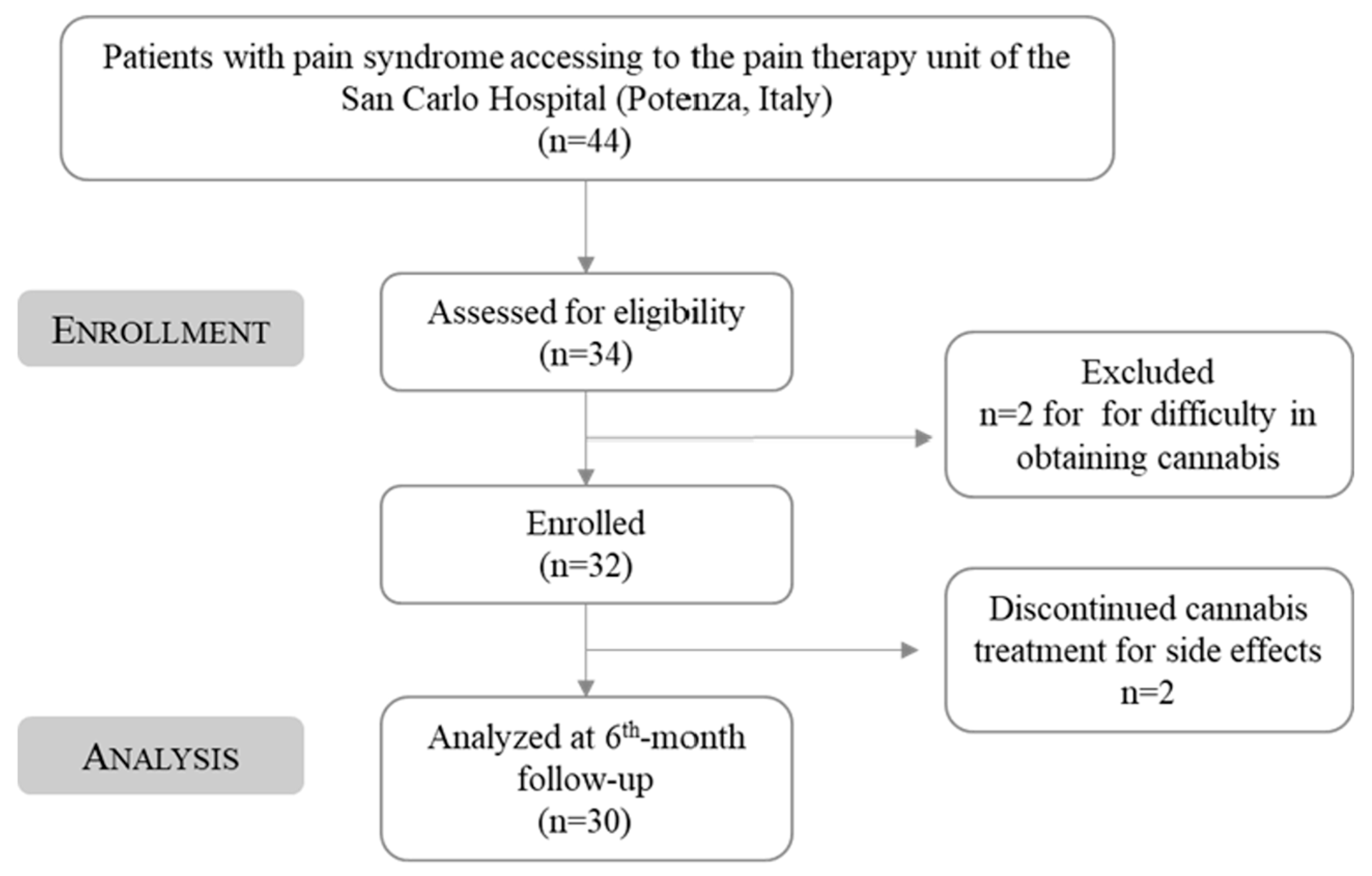
2.1. Study Design, Setting, and Outcomes
2.2. Treatment Regimen
2.3. Statistical Analysis
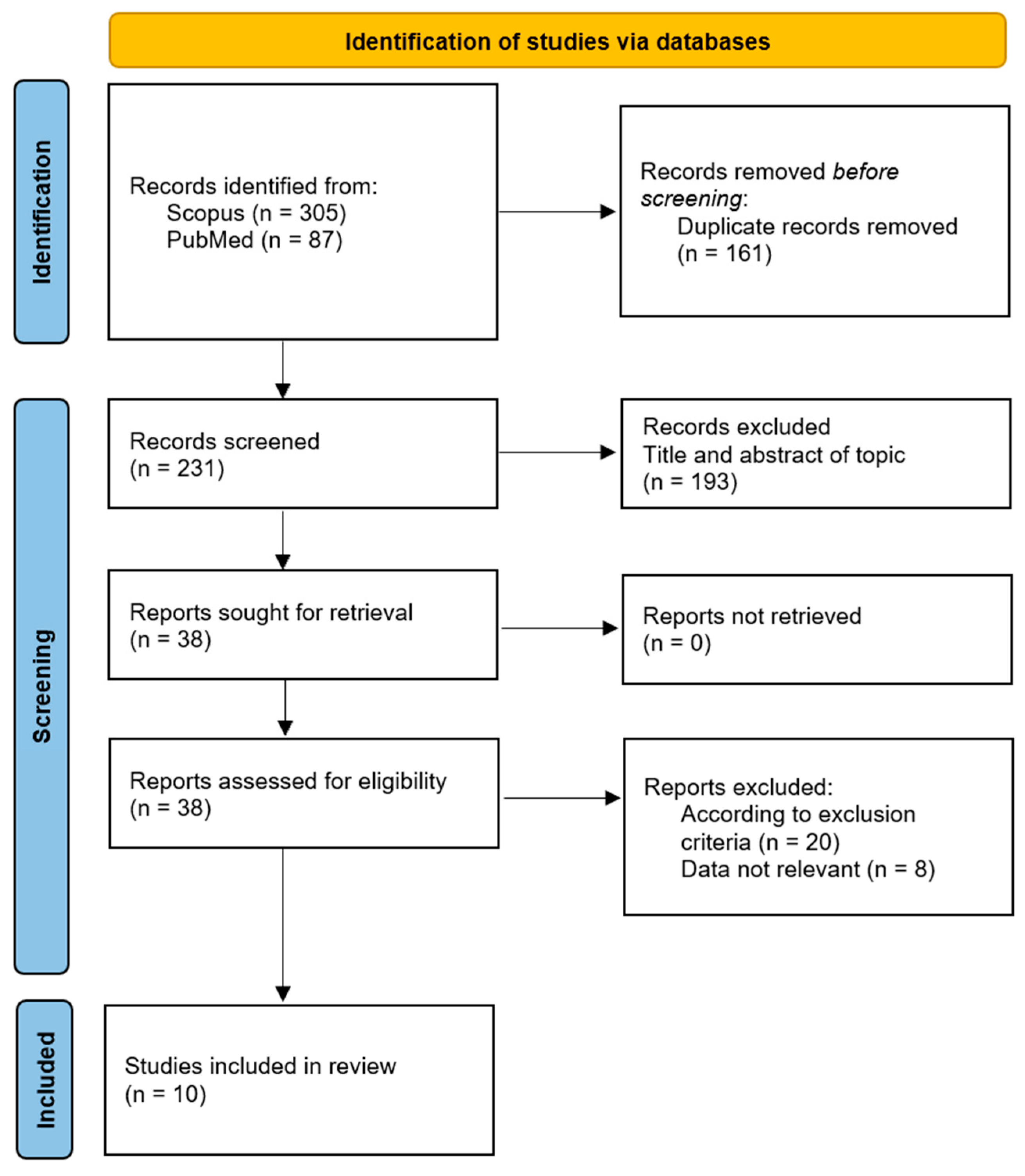
2.4. Systematic Review
Methodological Quality Assessment
3. Results
3.1. Patients Characteristics
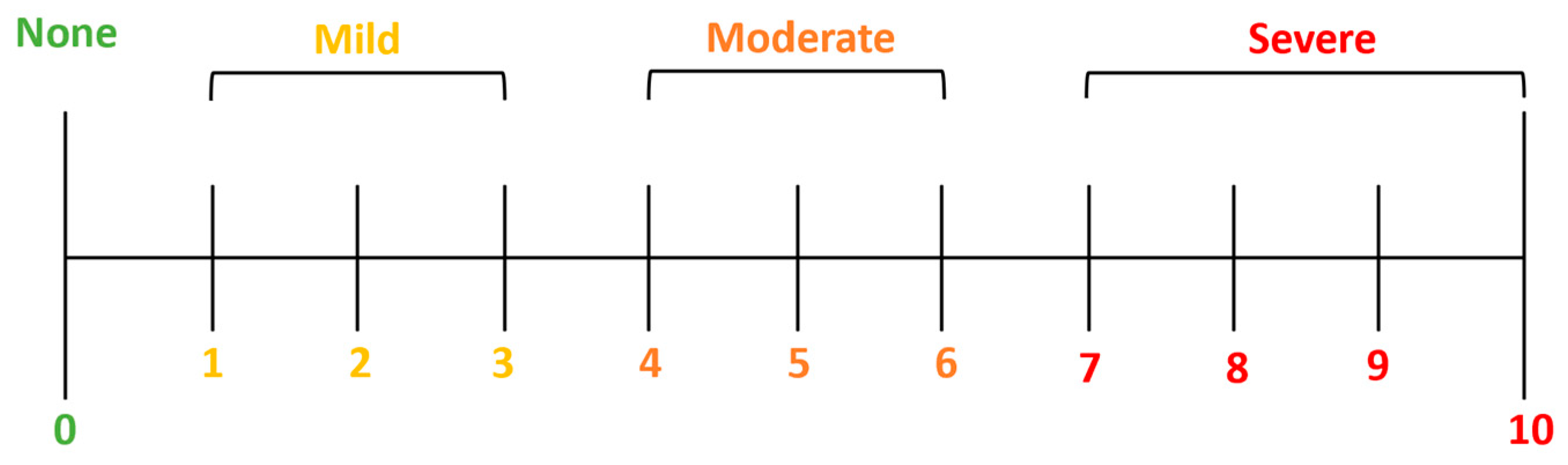
3.2. Numerical Pain Rating Scale (NRS)
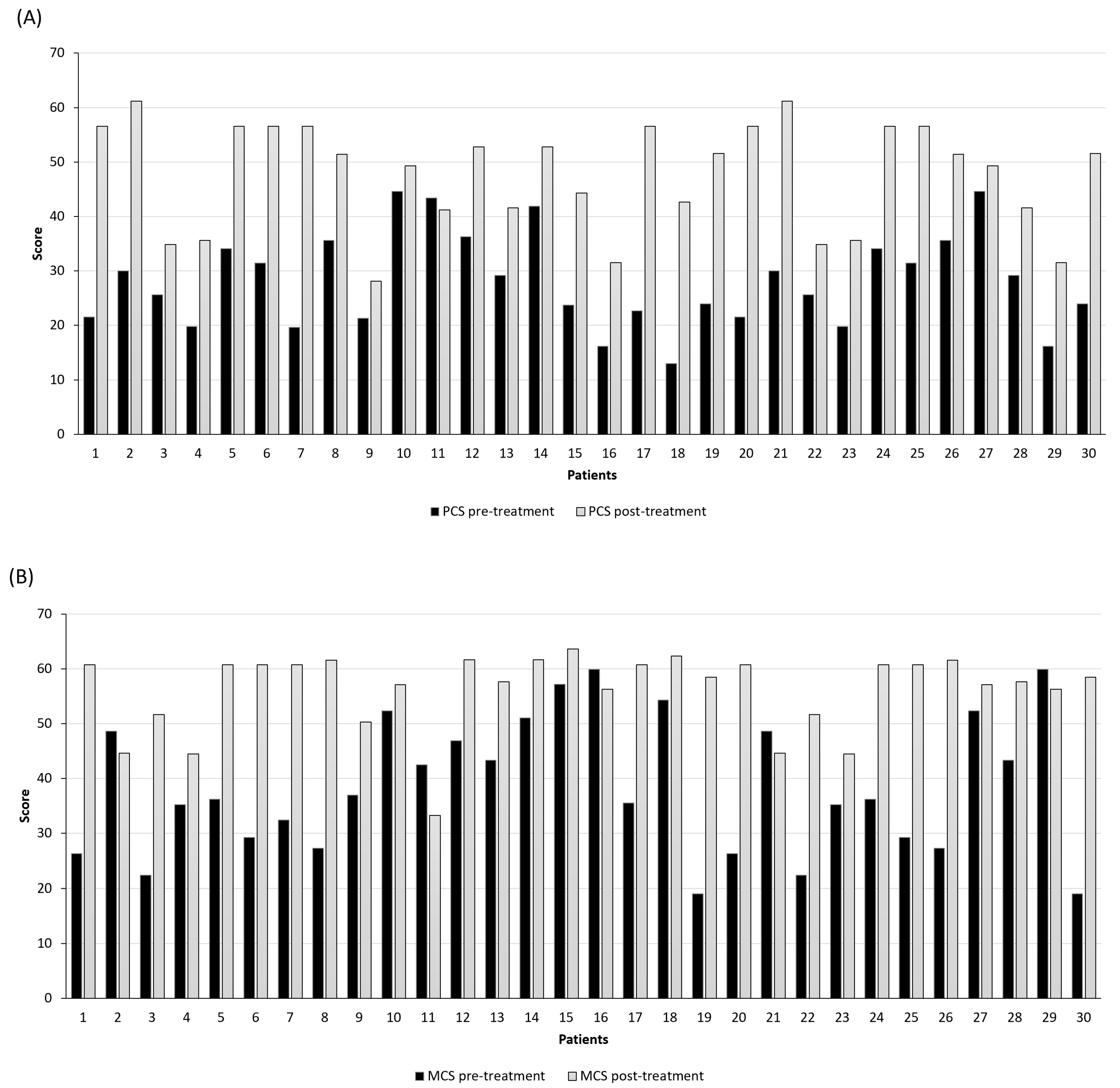
3.3. Short-Form Health Survey (SF-12)
3.4. Collateral Effects
3.5. Systematic Review
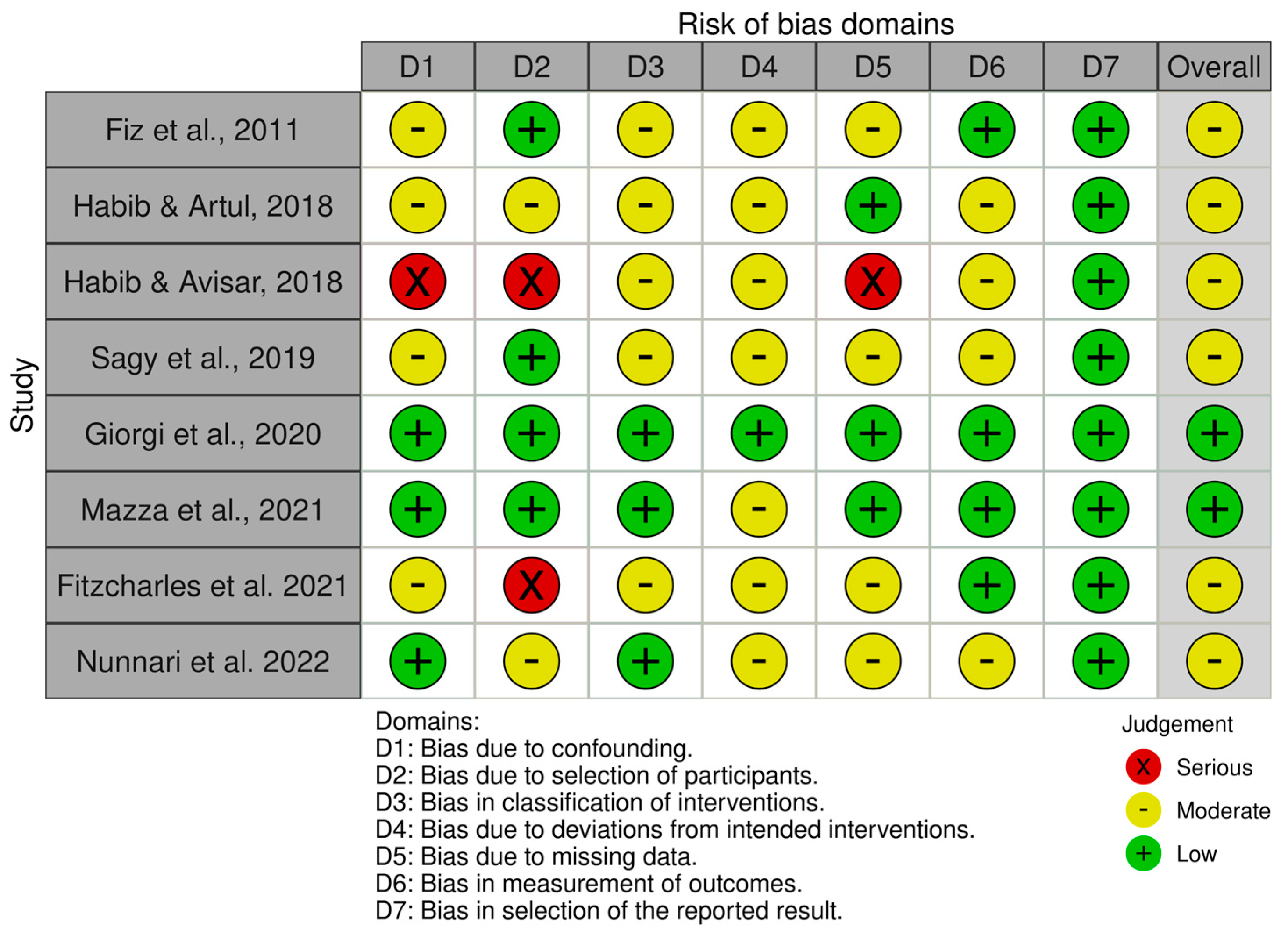
Risk of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al Sharie, S.; Varga, S.J.; Al-Husinat, L.i.; Sarzi-Puttini, P.; Araydah, M.; Bal’awi, B.R.; Varrassi, G. Unraveling the Complex Web of Fibromyalgia: A Narrative Review. Medicina 2024, 60, 272. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, ITC33–ITC48. [Google Scholar] [CrossRef] [PubMed]
- Choy, E.; Perrot, S.; Leon, T.; Kaplan, J.; Petersel, D.; Ginovker, A.; Kramer, E. A patient survey of the impact of fibromyalgia and the journey to diagnosis. BMC Health Serv. Res. 2010, 10, 102. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.A.; Wiffen, P.J.; Derry, S.; Rice, A.S. Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database Syst. Rev. 2014, 6, CD007938. [Google Scholar] [CrossRef]
- Aster, H.; Evdokimov, D.; Braun, A.; Üçeyler, N.; Sommer, C. Analgesic Medication in Fibromyalgia Patients: A Cross-Sectional Study. Pain Res. Manag. J. Can. Pain Soc. 2022, 2022, 1217717. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.E.; Guimarães, I. Fibromyalgia—Are there any new approaches? Best Pract. Res. Clin. Rheumatol. 2024, 101933. [Google Scholar] [CrossRef] [PubMed]
- Argenbright, C.M.; Bertlesman, A.M.; Russell, I.M.; Greer, T.L.; Peng, Y.B.; Fuchs, P.N. The Fibromyalgia Pain Experience: A Scoping Review of the Preclinical Evidence for Replication and Treatment of the Affective and Cognitive Pain Dimensions. Biomedicines 2024, 12, 778. [Google Scholar] [CrossRef] [PubMed]
- Häuser, W.; Walitt, B.; Fitzcharles, M.-A.; Sommer, C. Review of pharmacological therapies in fibromyalgia syndrome. Arthritis Res. Ther. 2014, 16, 201. [Google Scholar] [CrossRef] [PubMed]
- Melnikovova, I.; Russo, D.; Fait, T.; Kolarova, M.; Tauchen, J.; Kushniruk, N.; Falabella, R.; Milella, L.; Fernández Cusimamani, E. Evaluation of the effect of Lepidium meyenii Walpers in infertile patients: A randomized, double-blind, placebo-controlled trial. Phytother. Res. 2021, 35, 6359–6368. [Google Scholar] [CrossRef] [PubMed]
- Campesi, I.; Milella, L.; Palermo, M.; Sotgiu, G.; Reggiardo, G.; Franconi, F. Cigarette smoking affects the differences between male and female phenotypes. Am. J. Transl. Res. 2020, 12, 2998. [Google Scholar] [PubMed]
- Melnikovova, I.; Fait, T.; Kolarova, M.; Fernandez, E.C.; Milella, L. Effect of Lepidium meyenii Walp. on semen parameters and serum hormone levels in healthy adult men: A double-blind, randomized, placebo-controlled pilot study. Evid.-Based Complement. Altern. Med. 2015, 2015, 324369. [Google Scholar] [CrossRef] [PubMed]
- Alciati, A.; Nucera, V.; Masala, I.F.; Giallanza, M.; La Corte, L.; Giorgi, V.; Sarzi-Puttini, P.; Atzeni, F. One year in review 2021: Fibromyalgia. Clin. Exp. Rheumatol. 2021, 39, S3–S12. [Google Scholar] [CrossRef] [PubMed]
- Boehnke, K.F.; Litinas, E.; Clauw, D.J. Medical cannabis use is associated with decreased opiate medication use in a retrospective cross-sectional survey of patients with chronic pain. J. Pain 2016, 17, 739–744. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.R.; Romero-Sandoval, A.; Schatman, M.; Wallace, M.; Fanciullo, G.; McCarberg, B.; Ware, M. Cannabis in pain treatment: Clinical and research considerations. J. Pain 2016, 17, 654–668. [Google Scholar] [CrossRef] [PubMed]
- Fischedick, J.T.; Hazekamp, A.; Erkelens, T.; Choi, Y.H.; Verpoorte, R. Metabolic fingerprinting of Cannabis sativa L., cannabinoids and terpenoids for chemotaxonomic and drug standardization purposes. Phytochemistry 2010, 71, 2058–2073. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.B. Taming THC: Potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br. J. Pharmacol. 2011, 163, 1344–1364. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, A.G.; Serafini, M.R.; Quintans-Júnior, L.J. Terpenes and derivatives as a new perspective for pain treatment: A patent review. Expert Opin. Ther. Pat. 2014, 24, 243–265. [Google Scholar] [CrossRef] [PubMed]
- Apolone, G.; Mosconi, P.; Quattrociocchi, L.; Gianicolo, E.; Groth, N.; Ware, J. Questionario Sullo Stato di Salute SF-12. Versione Italiana; SF-12 questionnaire; Italian Version; IRFMN: Milano, Italy, 2005. [Google Scholar]
- Higgins, J.P.T.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Chapter 8: Assessing risk of bias in included studies. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017. [Google Scholar]
- Sterne, J.A.C.; Higgins, J.; Reeves, B.C. A Cochrane Risk Of Bias Assessment Tool: For Non Randomized Studies of Interventions (ACROBAT-NRSI). Version 2014, 1, 24. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Atakan, Z.; Martin-Santos, R.; Crippa, J.A.; Kambeitz, J.; Prata, D.; Williams, S.; Brammer, M.; Collier, D.A.; McGuire, P.K. Preliminary report of biological basis of sensitivity to the effects of cannabis on psychosis: AKT1 and DAT1 genotype modulates the effects of δ-9-tetrahydrocannabinol on midbrain and striatal function. Mol. Psychiatry 2012, 17, 1152–1155. [Google Scholar] [CrossRef] [PubMed]
- Istituto Nazionale di Statistica (ISTAT). Stato di Salute. 2011. Available online: https://www.istat.it/it/files/2011/02/metadati.pdf (accessed on 15 April 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Lerose, V.; Ponticelli, M.; Benedetto, N.; Carlucci, V.; Lela, L.; Tzvetkov, N.T.; Milella, L. Withania somnifera (L.) Dunal, a Potential Source of Phytochemicals for Treating Neurodegenerative Diseases: A Systematic Review. Plants 2024, 13, 771. [Google Scholar] [CrossRef]
- Fiz, J.; Durán, M.; Capellà, D.; Carbonell, J.; Farré, M. Cannabis use in patients with fibromyalgia: Effect on symptoms relief and health-related quality of life. PLoS ONE 2011, 6, e18440. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Artul, S. Medical cannabis for the treatment of fibromyalgia. JCR J. Clin. Rheumatol. 2018, 24, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Avisar, I. The consumption of cannabis by fibromyalgia patients in Israel. Pain Res. Treat. 2018, 2018, 7829427. [Google Scholar] [CrossRef] [PubMed]
- Sagy, I.; Bar-Lev Schleider, L.; Abu-Shakra, M.; Novack, V. Safety and efficacy of medical cannabis in fibromyalgia. J. Clin. Med. 2019, 8, 807. [Google Scholar] [CrossRef] [PubMed]
- Van de Donk, T.; Niesters, M.; Kowal, M.A.; Olofsen, E.; Dahan, A.; van Velzen, M. An experimental randomized study on the analgesic effects of pharmaceutical-grade cannabis in chronic pain patients with fibromyalgia. Pain 2019, 160, 860. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, V.; Bongiovanni, S.; Atzeni, F.; Marotto, D.; Di Carlo, M.; Galli, M.; Giovanioni, A.; Salaffi, F.; Sarzi-Puttini, P. Adding medical cannabis to standard analgesic treatment for fibromyalgia: A prospective observational study. Clin. Exp. Rheumatol. 2020, 38, 53–59. [Google Scholar] [PubMed]
- Chaves, C.; Bittencourt, P.C.T.; Pelegrini, A. Ingestion of a THC-rich cannabis oil in people with fibromyalgia: A randomized, double-blind, placebo-controlled clinical trial. Pain Med. 2020, 21, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Mazza, M. Medical cannabis for the treatment of fibromyalgia syndrome: A retrospective, open-label case series. J. Cannabis Res. 2021, 3, 35. [Google Scholar] [CrossRef] [PubMed]
- Fitzcharles, M.-A.; Rampakakis, E.; Sampalis, J.; Shir, Y.; Cohen, M.; Starr, M.; Häuser, W. Use of medical cannabis by patients with fibromyalgia in Canada after cannabis legalisation: A cross-sectional study. Clin. Exp. Rheumatol. 2021, 39, S115–S119. [Google Scholar] [CrossRef] [PubMed]
- Nunnari, P.; Ladiana, N.; Ceccarelli, G.; Notaro, P. Long-term Cannabis-based oil therapy and pain medications prescribing patterns: An Italian observational study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1224–1234. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, L.P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 2013, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Walitt, B.; Klose, P.; Fitzcharles, M.-A.; Phillips, T.; Haeuser, W. Cannabinoids for fibromyalgia. Cochrane Database Syst. Rev. 2016, 7, CD011694. [Google Scholar] [CrossRef] [PubMed]
- Skrabek, R.Q.; Galimova, L.; Ethans, K.; Perry, D. Nabilone for the treatment of pain in fibromyalgia. J. Pain 2008, 9, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Pezzilli, R.; Morselli-Labate, A.; Frulloni, L.; Cavestro, G.; Ferri, B.; Comparato, G.; Gullo, L.; Corinaldesi, R. The quality of life in patients with chronic pancreatitis evaluated using the SF-12 questionnaire: A comparative study with the SF-36 questionnaire. Dig. Liver Dis. 2006, 38, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Ware, M.A.; Fitzcharles, M.-A.; Joseph, L.; Shir, Y. The effects of nabilone on sleep in fibromyalgia: Results of a randomized controlled trial. Anesth. Analg. 2010, 110, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, P.; Pichini, S.; Pacifici, R.; Busardò, F.P.; Del Rio, A. Herbal preparations of medical cannabis: A vademecum for prescribing doctors. Medicina 2020, 56, 237. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Problem | Mild | Moderate | Severe | |
|---|---|---|---|---|
| Difficulty thinking or remembering | 0 | 1 | 2 | 3 |
| Awakening tired (not rested) | 0 | 1 | 2 | 3 |
| Fatigue | 0 | 1 | 2 | 3 |
| Class | |
|---|---|
| FDA approved drug | |
| Duloxetine | Serotonin–Norepinephrine Reuptake Inhibitor (SNRI) |
| Milnacipram | Serotonin–Norepinephrine Reuptake Inhibitor (SNRI) |
| Pregabalin | Anticonvulsant/Neuropathic Pain Agent |
| Commonly used drug | |
| Amitriptyline | Tricyclic Antidepressant (TCA) |
| Cyclobenzaprine | Muscle Relaxant |
| Gabapentin | Anticonvulsant/Neuropathic Pain Agent |
| Naltrexone | Opioid Antagonist |
| Acetaminophen | Analgesic |
| Parameters | n = 30 | |||
|---|---|---|---|---|
| Gender | Male | 20% | ||
| Female | 80% | |||
| Mediana | IQR | Mean ± SD | 95% CI | |
| Age | 50.50 | 45.75 | 53.17 ± 13.07 | 48.49–57.84 |
| Weight | 70.00 | 67.75 | 73.40 ± 10.28 | 69.72–77.08 |
| BMI (kg/m2) | 26.14 | 24.77 | 26.80 ± 3.89 | 25.41–28.19 |
| WPI | 8.00 | 6.00 | 7.53 ± 2.16 | 6.76–8.31 |
| SS | 7.00 | 5.00 | 7.10 ± 1.88 | 6.43–7.77 |
| Comorbidities | Pain Syndrome Associated with FM | ||||
|---|---|---|---|---|---|
| Patients | % | Patients | % | ||
| Hypertension | 6 | 20 | Polydistrict pain | 12 | 40 |
| Hypothyroidism | 3 | 10 | Migraine | 2 | 6.67 |
| Hereditary thrombophilia | 1 | 3.33 | Arthrosis | 1 | 3.33 |
| Convers syndrome | 1 | 3.33 | Rhizarthrosis | 1 | 3.33 |
| Hypercholesterol | 1 | 3.33 | Insomnia | 1 | 3.33 |
| Migraine | 1 | 3.33 | Trigeminal pain | 1 | 3.33 |
| Dyspeptic syndrome | 1 | 3.33 | Headache | 1 | 3.33 |
| Obesity | 1 | 3.33 | FBSS | 1 | 3.33 |
| Heart disease | 1 | 3.33 | |||
| Scleroderma | 1 | 3.33 | |||
| Raynaud’s disease | 1 | 3.33 |
| NRS | SF-12 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| PCS-12 | MCS-12 | ||||||||
| Prior MC | After MC | p-Value | Prior MC | After MC | p-Value | Prior MC | After MC | p-Value | |
| Median | 8.00 | 4.00 | <0.001 | 27.40 | 51.46 | <0.001 | 36.22 | 58.46 | <0.001 |
| IQR | 7.00 | 2.00 | 21.49 | 39.80 | 27.29 | 51.65 | |||
| Mean | 8.10 | 4.03 | 28.21 | 47.62 | 38.56 | 56.09 | |||
| ±SD | 1.24 | 2.11 | 8.72 | 9.81 | 12.41 | 7.28 | |||
| 95% CI | 7.66–8.54 | 3.28–4.79 | 25.09–31.33 | 44.11–51.13 | 34.12–43.00 | 53.48–58.69 | |||
| Author and Reference | Type of Study | Duration of the Study | Number of Investigated Subjects | Type of Cannabis Administered | Route of Administration | Evaluation Modality | Outcomes |
|---|---|---|---|---|---|---|---|
| Fiz et al., 2011 [29] | Observational (cross-sectional survey) | 1 day Data were taken at baseline and after 2 h of cannabis administration | 28 93% women | Not tirtrated cannabis | Smoked (54%), oral (46%) combined (43%). | VAS FIQ PSQI SF-36 | VAS score pain and stiffness relaxation feeling well being SF-36 mental component ~SF-36 phisical component ~FIQ ~PSQI |
| Habib and Artul, 2018 [30] | Observational (Retrospective) | 2 months | 26 73% women | Not tirtrated cannabis 26 ± 8.2 g/month | Smoked (58%) Vaporized (23%) Vaporized + Smoked (14%) Oral oil drop + Smoked (8%) | Revised FIQ | Improvement of all parameters evaluated with the revised FIQ |
| Habib and Avisar, 2018 [31] | Observational (Retrospective) | Not specified | 383 85% women | Not titrated cannabis 31.4 ± 16.3 g/month | Smoked with tobacco 63% Smoked pure cannabis 17% Sublingual oil drop 5% Vaporized 15% | Evaluation of daily activity, pain relief, slip quality, anxiety, and depression | Improvement of all evaluated parameters |
| Sagy et al., 2019 [32] | Observational | 6 month | 211 | THC- or CBD-rich strains 670 mg/day of cannabis at the beginning and 700 to 1000 mg at six months Median THC at six months 140 mg/day Madian CBD at six months 39 mg/day | Oil drops Inflorescence Capsules Cigarettes (the specific percentage of patients that used one or the other mode of administration was not specified) | NRS 5 and 8 point Linkert scale | Sleep problems Depression Quality life |
| Van de Donk Kowal, 2019 [33] | Randomised Placebo-Controlled 4-Way Crossover Trial | Not specified (patients received 1 of the 4 available type of cannabis with a minimum 2-week interval between visits) | 25 female patients | Bedrocan®: 22.4 mg THC, <1 mg CBD Bediol®: 13.4 mg THC, 17.8 mg CBD. Bedrolite® (Bedrocan International): <1 mg THC, 18.4 mg CBD. Placebo One inhalation. | Vaporization | Pressure pain test Electrical pain test Bowdle questionnaire Bond and Lader questionnaire | pressure pain threshold for cannabis variety containing THC pain score of 30% for Bediol compared to placebo |
| Giorgi et al., 2020 [34] | Observational (Perspective) | 6 month | 102 91% women | Bedrocan®: 22% THC, <1% CBD Bediol®: 6.3% THC, 8% CBD. | Oil oral drops | FAS Revised FIQ PSQI SAPS ZSR-D ZSR-A FACIT | PSQI in 44% of subjects FIQ score in 33% of patients Moderate improvement in ZSR-D and ZRS-A in 50% of subjects |
| Chaves et al., 2020 [35] | Randomised Double Bling Placebo-Controlled Clinical trial | 8 weeks | 17 female patients | White Widow variety - 48:1 THC:CBD Placebo 1 drop/day | Sublingual oil drop | FIQ | FIQ score in cannabis group compared to placebo |
| Mazza et al., 2021 [36] | Observational (Retrospective) | 12 months | 38 95% women | FM2 5–8% THC, 7.5–12% CBD Bediol 6% THC, 8% CBD FM1 13–20% THC, <1% CBD Bedrocan 22% THC, < 1% CBD Pedanios 17–26% THC, <1% CBD THC-dominant variety minimum 50 mg/day; maximum 600 mg/day Hybrid cannabis variety minimum 100 mg/day, maximum 600 mg/day | Oral decoction Sublingual oil drop Vaporized | ODI HADS SyS | 1 month follow up NRS, ODI, WPI and severity score 3 months follow up NRS, ODI, WPI 12 months follow up NRS, ODI, and severity score |
| Fitzcharles et al., 2021 [37] | Observational | 2 months | 117 91.5% women | Prescribed and not prescribed cannabis For inhaled cannabis 0.5 to 2 g per day, mostly | Smoked Vaporized Oil | VAS PtGA PGA | Pain syndrome relief |
| Nunnari et al., 2022 [38] | Observational (Retrospective) | The median duration of cannabis consumption is 12 months | 56 73.2% women | Bedrocan 78.5% of patients Bediol 17.9% of patients FM2 3.6% of patients | Cannabis oil | Effect of cannabis administration on pain medication discontinuation | Reduction in opioid users |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giardina, A.; Palmieri, R.; Ponticelli, M.; Antonelli, C.; Carlucci, V.; Colangelo, M.; Benedetto, N.; Di Fazio, A.; Milella, L. Is a Low Dosage of Medical Cannabis Effective for Treating Pain Related to Fibromyalgia? A Pilot Study and Systematic Review. J. Clin. Med. 2024, 13, 4088. https://doi.org/10.3390/jcm13144088
Giardina A, Palmieri R, Ponticelli M, Antonelli C, Carlucci V, Colangelo M, Benedetto N, Di Fazio A, Milella L. Is a Low Dosage of Medical Cannabis Effective for Treating Pain Related to Fibromyalgia? A Pilot Study and Systematic Review. Journal of Clinical Medicine. 2024; 13(14):4088. https://doi.org/10.3390/jcm13144088
Chicago/Turabian StyleGiardina, Antonio, Rocco Palmieri, Maria Ponticelli, Carlo Antonelli, Vittorio Carlucci, Monica Colangelo, Nadia Benedetto, Aldo Di Fazio, and Luigi Milella. 2024. "Is a Low Dosage of Medical Cannabis Effective for Treating Pain Related to Fibromyalgia? A Pilot Study and Systematic Review" Journal of Clinical Medicine 13, no. 14: 4088. https://doi.org/10.3390/jcm13144088
APA StyleGiardina, A., Palmieri, R., Ponticelli, M., Antonelli, C., Carlucci, V., Colangelo, M., Benedetto, N., Di Fazio, A., & Milella, L. (2024). Is a Low Dosage of Medical Cannabis Effective for Treating Pain Related to Fibromyalgia? A Pilot Study and Systematic Review. Journal of Clinical Medicine, 13(14), 4088. https://doi.org/10.3390/jcm13144088