

Performance of the First-Trimester Cervical Consistency Index to Predict Preterm Birth

 , ,
, ,  ,
,  ,
,  and
and
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Recruitment
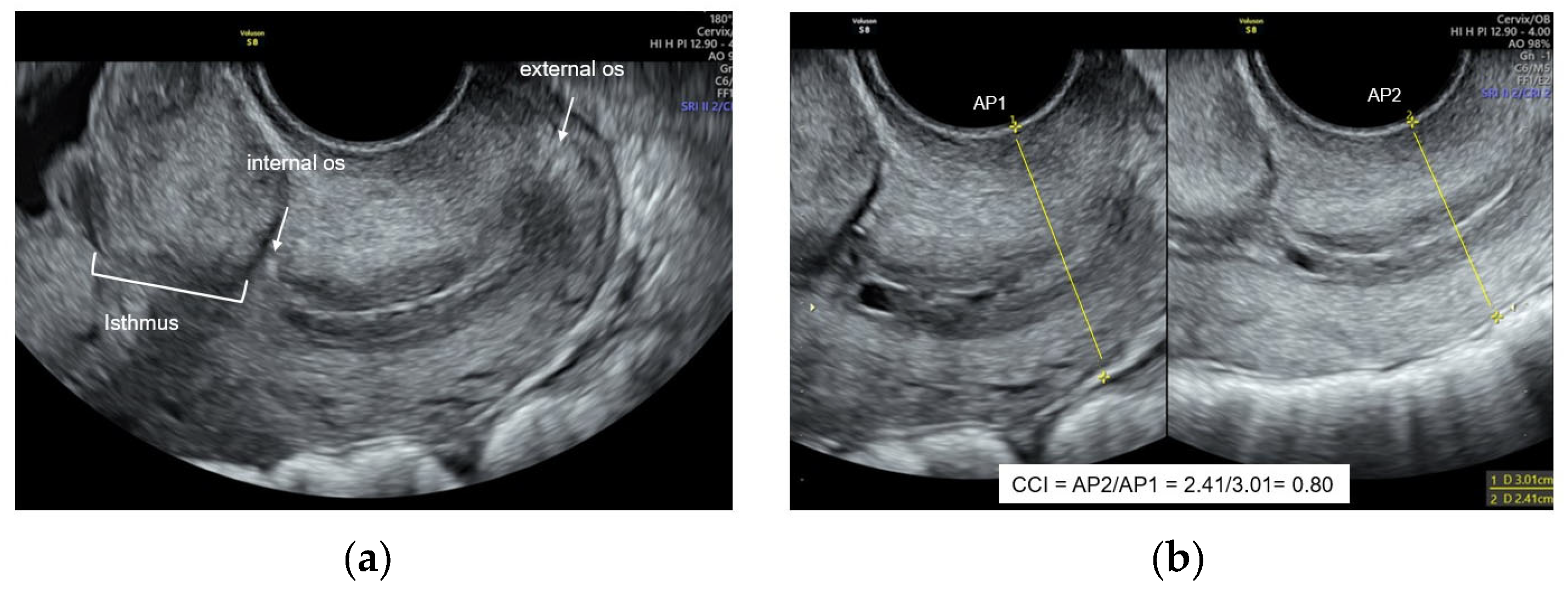
2.3. Ultrasound Evaluation
2.4. Follow Up
2.5. Data Collection
2.6. Outcomes
2.7. Statistical Analysis
3. Results
3.1. Description of the Cohort and Characteristics of the Study Population
3.2. Cervical Consistency Index as Predictor of sPTB
3.3. Cervical Consistency Index as Predictor of sPTB According to History of sPTB
3.4. Association between sPTB, CCI, Cervical Length, and History of PTB
3.5. Intraobserver and Interobserver Agreement of the Cervical Consistency Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- March of Dimes, pmNch, Save the Children, WHO. Born Too Soon: The Global Action Report on Preterm Birth. eds cp howson, mV Kinney, Je lawn. World Health Organization. Geneva. 2012. Available online: https://apps.who.int/iris/bitstream/handle/10665/44864/9789241503433_eng.pdf;jsessionid=C221360BA148E228A7A079C1EE4261E8?sequence=1 (accessed on 15 June 2024).
- De Costa, A.; Moller, A.B.; Blencowe, H.; Johansson, E.W.; Hussain-Alkhateeb, L.; Ohuma, E.O.; Okwaraji, Y.B.; Cresswell, J.; Requejo, J.H.; Bahl, R.; et al. Study protocol for WHO and UNICEF estimates of global, regional, and national preterm birth rates for 2010 to 2019. PLoS ONE 2021, 16, e0258751. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035, published correction appears in Lancet 2017, 389, 1884. [Google Scholar] [CrossRef] [PubMed]
- Celik, E.; To, M.; Gajewska, K.; Smith, G.C.; Nicolaides, K.H.; Fetal Medicine Foundation Second Trimester Screening Group. Cervical length and obstetric history predict spontaneous preterm birth: Development and validation of a model to provide individualized risk assessment. Ultrasound Obstet. Gynecol. 2008, 31, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Gudicha, D.W.; Romero, R.; Kabiri, D.; Hernandez-Andrade, E.; Pacora, P.; Erez, O.; Kusanovic, J.P.; Jung, E.; Paredes, C.; Berry, S.M.; et al. Personalized assessment of cervical length improves prediction of spontaneous preterm birth: A standard and a percentile calculator. Am. J. Obstet. Gynecol. 2021, 224, 288.e1–288.e17. [Google Scholar] [CrossRef] [PubMed]
- Parra-Saavedra, M.; Gómez, L.; Barrero, A.; Parra, G.; Vergara, F.; Navarro, E. Prediction of preterm birth using the cervical consistency index. Ultrasound Obstet. Gynecol. 2011, 38, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Baños, N.; Murillo-Bravo, C.; Julià, C.; Migliorelli, F.; Perez-Moreno, A.; Ríos, J.; Gratacós, E.; Valentin, L.; Palacio, M. Mid-trimester sonographic cervical consistency index to predict spontaneous preterm birth in a low-risk population. Ultrasound Obstet. Gynecol. 2018, 51, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Baños, N.; Julià, C.; Lorente, N.; Ferrero, S.; Cobo, T.; Gratacos, E.; Palacio, M. Mid-Trimester Cervical Consistency Index and Cervical Length to Predict Spontaneous Preterm Birth in a High-Risk Population. AJP Rep. 2018, 8, e43–e50. [Google Scholar] [CrossRef] [PubMed]
- van der Merwe, J.; Couck, I.; Russo, F.; Burgos-Artizzu, X.P.; Deprest, J.; Palacio, M.; Lewi, L. The Predictive Value of the Cervical Consistency Index to Predict Spontaneous Preterm Birth in Asymptomatic Twin Pregnancies at the Second-Trimester Ultrasound Scan: A Prospective Cohort Study. J. Clin. Med. 2020, 9, 1784. [Google Scholar] [CrossRef] [PubMed]
- Wharton, L.K.; Anumba, D.O.C. Techniques for detecting cervical remodeling as a predictor for spontaneous preterm birth: Current evidence and future research avenues in patients with multiple pregnancies. J. Matern. Fetal Neonatal Med. 2023, 36, 2262081. [Google Scholar] [CrossRef] [PubMed]
- Sonek, J.; Shellhaas, C. Cervical sonography: A review. Ultrasound Obstet. Gynecol. 1998, 11, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Becerra-Mojica, C.H.; Parra-Saavedra, M.A.; Diaz-Martinez, L.A.; Martinez-Portilla, R.J.; Rincon Orozco, B. Cohort profile: Colombian Cohort for the Early Prediction of Preterm Birth (COLPRET): Early prediction of preterm birth based on personal medical history, clinical characteristics, vaginal microbiome, biophysical characteristics of the cervix and maternal serum biochemical markers. BMJ Open 2022, 12, e060556. [Google Scholar] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Faris, I.; Callejas, A. Histobiomechanical Remodeling of the Cervix during Pregnancy: Proposed Framework. Math. Probl. Eng. 2019, 2019, 5957432. [Google Scholar] [CrossRef]
- McFarlin, B.L.; Bigelow, T.A.; Laybed, Y.; O’Brien, W.D.; Oelze, M.L.; Abramowicz, J.S. Ultrasonic attenuation estimation of the pregnant cervix: A preliminary report. Ultrasound Obstet. Gynecol. 2010, 36, 218–225. [Google Scholar] [CrossRef]
- Conoscenti, G.; Meir, Y.J.; D’Ottavio, G.; Rustico, M.A.; Pinzano, R.; Fischer-Tamaro, L.; Stampalija, T.; Natale, R.; Maso, G.; Mandruzzato, G. Does cervical length at 13–15 weeks’ gestation predict preterm delivery in an unselected population? Ultrasound Obstet. Gynecol. 2003, 21, 128–134. [Google Scholar] [CrossRef]
- Carvalho, M.H.; Bittar, R.E.; Brizot, M.L.; Maganha, P.P.; Borges da Fonseca, E.S.; Zugaib, M. Cervical length at 11–14 weeks’ and 22-24 weeks’ gestation evaluated by transvaginal sonography, and gestational age at delivery. Ultrasound Obstet. Gynecol. 2003, 21, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Berghella, V.; Talucci, M.; Desai, A. Does transvaginal sonographic measurement of cervical length before 14 weeks predict preterm delivery in high-risk pregnancies? Ultrasound Obstet. Gynecol. 2003, 21, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Antsaklis, P.; Daskalakis, G.; Pilalis, A.; Papantoniou, N.; Mesogitis, S.; Antsaklis, A. The role of cervical length measurement at 11–14 weeks for the prediction of preterm delivery. J. Matern. Fetal Neonatal Med. 2011, 24, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Souka, A.P.; Papastefanou, I.; Michalitsi, V.; Papadopoulos, G.K.; Kassanos, D. A predictive model of short cervix at 20–24 weeks using first-trimester cervical length measurement and maternal history. Prenat. Diagn. 2011, 31, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Greco, E.; Lange, A.; Ushakov, F.; Calvo, J.R.; Nicolaides, K.H. Prediction of spontaneous preterm delivery from endocervical length at 11 to 13 weeks. Prenat. Diagn. 2011, 31, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Souka, A.P.; Papastefanou, I.; Michalitsi, V.; Salambasis, K.; Chrelias, C.; Salamalekis, G.; Kassanos, D. Cervical length changes from the first to second trimester of pregnancy, and prediction of preterm birth by first-trimester sonographic cervical measurement. J. Ultrasound Med. 2011, 30, 997–1002, published correction appears in J. Ultrasound Med. 2011, 30, 1753. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Chaemsaithong, P.; Duan, H.; Ju, X.; Appiah, K.; Shen, L.; Wang, X.; Tai, Y.; Leung, T.Y.; Poon, L.C. Screening for spontaneous preterm birth by cervical length and shear-wave elastography in the first trimester of pregnancy. Am. J. Obstet. Gynecol. 2022, 227, 500.e1–500.e14. [Google Scholar] [CrossRef] [PubMed]
- Feltovich, H.; Carlson, L. New techniques in evaluation of the cervix. Semin. Perinatol. 2017, 41, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Andrade, E.; Maymon, E.; Luewan, S.; Bhatti, G.; Mehrmohammadi, M.; Erez, O.; Pacora, P.; Done, B.; Hassan, S.S.; Romero, R. A soft cervix, categorized by shear-wave elastography, in women with short or with normal cervical length at 18–24 weeks is associated with a higher prevalence of spontaneous preterm delivery. J. Perinat. Med. 2018, 46, 489–501. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Term Birth n = 606 | sPTB < 37 Weeks n = 61 | p-Value |
|---|---|---|---|
| Maternal age (years) * | 28 (24–32) | 27(25–32) | 0.118 |
| Preterm birth history | 41 (6.8%) | 13 (21.3%) | <0.001 |
| Smoking history | 70 (11.5%) | 4 (6.6%) | 0.244 |
| Body mass index * | 25.3 (22.6–28.1) | 26.5 (23.4–29.7) | 0.224 |
| GA at scan (weeks) * | 13.1(12.5–13.5) | 13.2 (12.5–13.5) | 0.671 |
| Cervical length (mm) * | 35 (35–38) | 35 (33–37) | 0.845 |
| CCI * | 0.83 (0.78–0.87) | 0.80 (0.76–0.85) | 0.003 |
| GA at delivery(weeks) * | 38.6 (38–39.4) | 36.2(34.5–36.4) | <0.001 |
| Without previous pregnancies | 223 (37%) | 16 (26.2%) | 0.097 |
| Health care system Subsidized Contributive Special Not in the system | 78 (28.2%) 172 (62.1%) 16 (5.8%) 11 (3.1%) | 10 (29.4%) 17 (50.0%) 5 (14.7%) 2 (5.9%) | 0.537 0.146 0.677 |
| Marital status Married Live with partner Single | 189 (31.2%) 334 (55.1%) 83 (13.7%) | 13(21.3%) 44 (72.1%) 4 (6.5%) | 0.480 0.544 |
| Residence place Metropolitan area Outside | 460 (76.0%) 145(24.0%) | 42(68.8%) 19 (31.2%) | 0.217 |
| Nationality Colombian Venezuelan | 576 (95.1%) 30 (4.9%) | 58 (95.1%) 3 (4.9%) | 0.991 |
| Cut-Off | Sensitivity % (n/N) | Specificity % (n/N) | PPV % (n/N) | NPV % (n/N) | LR+ 95% CI | LR− 95% CI |
|---|---|---|---|---|---|---|
| sPTB < 37 weeks | ||||||
| CCI (centile) | ||||||
| 0.71 (5th) | 9.8 (6/61) | 95.4 (576/604) | 17.6 (6/34) | 76.2 (576/631) | 2.12 (0.91–4.92) | 0.95 (0.85–1.06) |
| 0.74 (10th) | 19.7 (12/61) | 90.4 (546/604) | 17.1 (12/70) | 91.8(546/595) | 2.05 (1.17–3.60) | 0.89 (0.77–1.03) |
| 0.76 (15th) | 24.6 (15/61) | 85.9 (519/604) | 15.0(15/100) | 91.9 (519/565) | 1.75 (1.08–2.83) | 0.88 (0.75–1.03) |
| CCI < 0.70 * | 9.8 (6/34) | 96.2 (581/604) | 20.7 (23/29) | 91.4 (581/636) | 3.40 (1.09–6.10) | 0.87 (0.84–1.05) |
| sPTB < 34 weeks | ||||||
| CCI (centile) | ||||||
| 0.71 (5th) | 16.7 (2/12) | 95.1 (621/653) | 5.9 (2/34) | 98.4 (621/631) | 3.40 (0.92–12.60) | 0.88 (0.67–1.14) |
| 0.74 (10th) | 33.3 (4/12) | 90.0 (588/653) | 5.8 (4/69) | 98.7 (588/596) | 3.35 (1.46–7.70) | 0.74 (0.49–1.11) |
| 0.76 (15th) | 50.0 (6/12) | 85.6 (559/653) | 6.0 (6/100) | 98.9 (559/565) | 3.47 (1.91–6.30) | 0.58 (0.33–1.03) |
| CCI < 0.69 * | 16.7 (2/12) | 96.3 (629/653) | 7.7(2/26) | 98.4 (629/639) | 4.53 (1.21–17.06) | 0.87 (0.66–1.13) |
| No History of sPTB | Sensitivity % (n/N) | Specificity % (n/N) | PPV % (n/N) | NPV % (n/N) | LR+ | LR− |
|---|---|---|---|---|---|---|
| sPTB < 37 weeks | ||||||
| CCI at 10th percentile | 15 (7/48) | 91 (516/565) | 13/7/49) | 93 (516/557) | 1.68 | 0.94 |
| sPTB < 34 weeks | ||||||
| CCI at 10th percentile | 22 (2/9) | 91 (550/604) | 4 (2/56) | 99 (550/557) | 2.49 | 0.85 |
| History of sPTB | ||||||
| sPTB < 37 weeks | ||||||
| CCI at 10th percentile | 39 (5/13) | 90 (37/41) | 56 (5/9) | 82 (37/45) | 3.94 | 0.68 |
| sPTB < 34 weeks | ||||||
| CCI at 10th percentile | 67 (2/3) | 82 (44/51) | 22 (2/9) | 98 (44/45) | 4.86 | 0.40 |
| PTB < 37 Weeks | OR | 5% CI | 95% CI | p-Value | AUC |
|---|---|---|---|---|---|
| CCI <10th percentile | 2.55 | 1.28 | 5.10 | 0.008 | 0.55 (0.50–0.60) |
| Cervical Length | 1.00 | 0.95 | 1.06 | 0.843 | 0.50 (0.43–0.58) |
| History of PTB | 3.73 | 1.87 | 7.44 | <0.001 | 0.57 (0.52–0.62) |
| PTB < 34 weeks | |||||
| CCI < 10th percentile | 4.87 | 1.42 | 16.63 | 0.012 | 0.62 (0.48–0.76) |
| Cervical Length | 0.95 | 0.83 | 1.08 | 0.475 | 0.41 (0.22–0.60) |
| History of PTB | 3.94 | 1.03 | 15.09 | 0.044 | 0.58 (0.45–0.71) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becerra-Mojica, C.H.; Parra-Saavedra, M.A.; Martínez-Vega, R.A.; Díaz-Martínez, L.A.; Martínez-Portilla, R.J.; Torres-Torres, J.; Rincon-Orozco, B. Performance of the First-Trimester Cervical Consistency Index to Predict Preterm Birth. J. Clin. Med. 2024, 13, 3906. https://doi.org/10.3390/jcm13133906
Becerra-Mojica CH, Parra-Saavedra MA, Martínez-Vega RA, Díaz-Martínez LA, Martínez-Portilla RJ, Torres-Torres J, Rincon-Orozco B. Performance of the First-Trimester Cervical Consistency Index to Predict Preterm Birth. Journal of Clinical Medicine. 2024; 13(13):3906. https://doi.org/10.3390/jcm13133906
Chicago/Turabian StyleBecerra-Mojica, Carlos H., Miguel A. Parra-Saavedra, Ruth A. Martínez-Vega, Luis A. Díaz-Martínez, Raigam J. Martínez-Portilla, Johnatan Torres-Torres, and Bladimiro Rincon-Orozco. 2024. "Performance of the First-Trimester Cervical Consistency Index to Predict Preterm Birth" Journal of Clinical Medicine 13, no. 13: 3906. https://doi.org/10.3390/jcm13133906
APA StyleBecerra-Mojica, C. H., Parra-Saavedra, M. A., Martínez-Vega, R. A., Díaz-Martínez, L. A., Martínez-Portilla, R. J., Torres-Torres, J., & Rincon-Orozco, B. (2024). Performance of the First-Trimester Cervical Consistency Index to Predict Preterm Birth. Journal of Clinical Medicine, 13(13), 3906. https://doi.org/10.3390/jcm13133906