
Prognosis and Predictor Factors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: A Retrospective Analysis of the Post-Transcatheter Aortic Replacement Clairval Hospital Registry

 ,
,
Abstract
1. Introduction
2. Materials and Methods
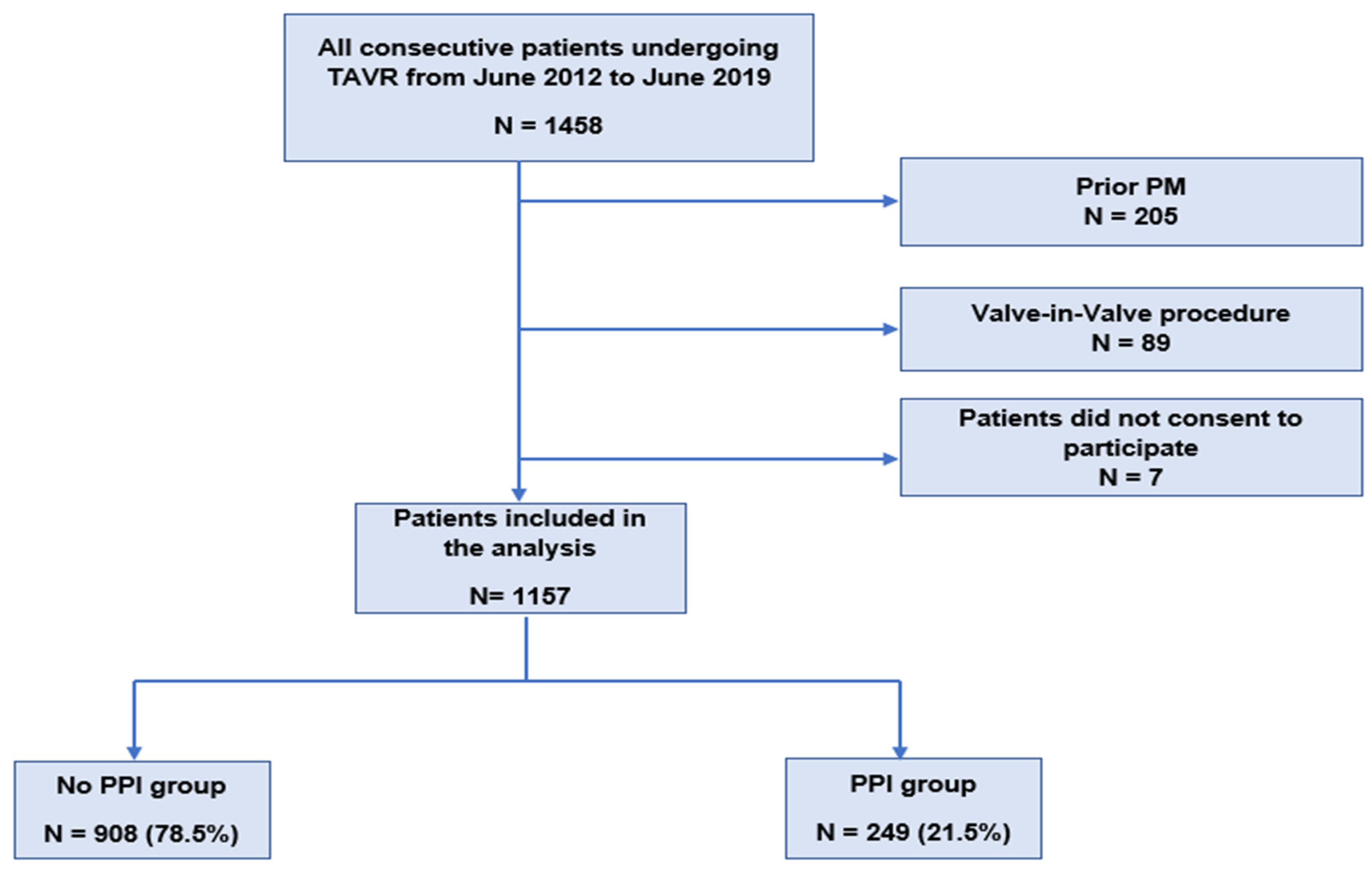
2.1. Study Population and Setting
2.2. Definitions and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Study Population and Procedural Characteristics
3.2. PPI and Predictive Factor
3.3. Change in Practices over Time
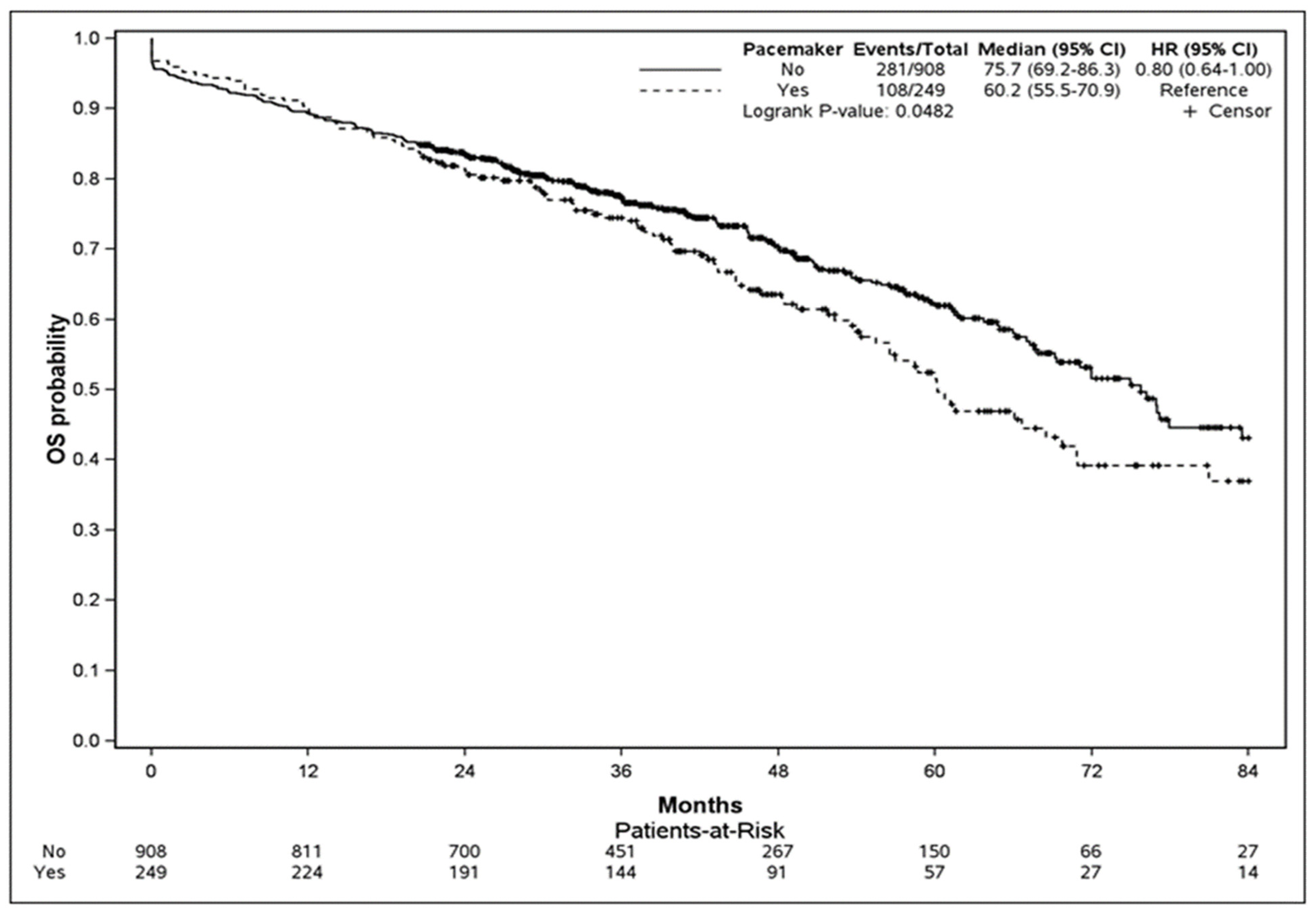
3.4. Survival Analysis
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Urena, M.; Webb, J.G.; Cheema, A.; Serra, V.; Toggweiler, S.; Barbanti, M.; Cheung, A.; Ye, J.; Dumont, E.; DeLarochellière, R.; et al. Impact of new-onset persistent left bundle branch block on late clinical outcomes in patients undergoing transcatheter aortic valve implantation with a balloon-expandable valve. JACC Cardiovasc. Interv. 2014, 7, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Gilard, M.; Eltchaninoff, H.; Iung, B.; Donzeau-Gouge, P.; Chevreul, K.; Fajadet, J.; Leprince, P.; Leguerrier, A.; Lievre, M.; Prat, A.; et al. Registry of Transcatheter Aortic-Valve Implantation in High-Risk Patients. N. Engl. J. Med. 2012, 366, 1705–1715. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Lefevre, T.; Van Belle, E.; Eltchaninoff, H.; Iung, B.; Koning, R.; Motreff, P.; Leprince, P.; Verhoye, J.P.; Manigold, T.; et al. Temporal Trends in Transcatheter Aortic Valve Replacement in France: FRANCE 2 to FRANCE TAVI. J. Am. Coll. Cardiol. 2017, 70, 42–55. [Google Scholar] [CrossRef] [PubMed]
- Ullah, W.; Zahid, S.; Zaidi, S.R.; Sarvepalli, D.; Haq, S.; Roomi, S.; Mukhtar, M.; Khan, M.A.; Gowda, S.N.; Ruggiero, N.; et al. Predictors of Permanent Pacemaker Implantation in Patients Undergoing Transcatheter Aortic Valve Replacement—A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e020906. [Google Scholar] [CrossRef] [PubMed]
- Lilly, S.M.; Deshmukh, A.J.; Epstein, A.E.; Ricciardi, M.J.; Shreenivas, S.; Velagapudi, P.; Wyman, J.F. 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 76, 2391–2411. [Google Scholar] [CrossRef] [PubMed]
- Rodés-Cabau, J.; Ellenbogen, K.A.; Krahn, A.D.; Latib, A.; Mack, M.; Mittal, S.; Muntané-Carol, G.; Nazif, T.M.; Sondergaard, L.; Urena, M.; et al. Management of Conduction Disturbances Associated with Transcatheter Aortic Valve Replacement: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2019, 74, 1086–1106. [Google Scholar] [CrossRef] [PubMed]
- Subramani, S.; Arora, L.; Krishnan, S.; Hanada, S.; Sharma, A.; Ramakrishna, H. Analysis of Conduction Abnormalities and Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Ki, Y.-J.; Kang, J.; Lee, H.S.; Chang, M.; Han, J.-K.; Yang, H.-M.; Park, K.W.; Kang, H.-J.; Koo, B.-K.; Kim, H.-S. Optimal Oversizing Index Depending on Valve Type and Leakage-Proof Function for Preventing Paravalvular Leakage after Transcatheter Aortic Valve Implantation. J. Clin. Med. 2020, 9, 3936. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.J.; Yan, C.J.; Lin, D.Q.; Cheng, Y.B.; Yu, S.J.; Li, J.; Zhang, X.P.; Cheng, W. Prognostic impact of new permanent pacemaker implantation following transcatheter aortic valve replacement. Catheter. Cardiovasc. Interv. 2023, 102, 743–750. [Google Scholar] [CrossRef]
- Panagides, V.; Cheema, A.N.; Urena, M.; Nombela-Franco, L.; Veiga-Fernandez, G.; Vilalta, V.; Regueiro, A.; Del Val, D.; Asmarats, L.; del Trigo, M.; et al. Optimal Degree of Balloon-Expandable Transcatheter Valve Oversizing in Patients With Borderline Aortic Annulus Measurements: Insights From a Multicenter Real-World Experience. Circ. Cardiovasc. Interv. 2023, 16, e012554. [Google Scholar] [CrossRef]
- Carroll, J.D.; Mack, M.J.; Vemulapalli, S.; Herrmann, H.C.; Gleason, T.G.; Hanzel, G.; Deeb, G.M.; Thourani, V.H.; Cohen, D.J.; Desai, N.; et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 76, 2492–2516. [Google Scholar] [CrossRef]
- Glikson, M.; Nielsen, J.C.; Kronborg, M.B.; Michowitz, Y.; Auricchio, A.; Barbash, I.M.; Barrabés, J.A.; Boriani, G.; Braunschweig, F.; Brignole, M.; et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur. Heart J. 2021, 42, 3427–3520. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Mangieri, A.; Lanzillo, G.; Bertoldi, L.; Jabbour, R.J.; Regazzoli, D.; Ancona, M.B.; Tanaka, A.; Mitomo, S.; Garducci, S.; Montalto, C.; et al. Predictors of Advanced Conduction Disturbances Requiring a Late (≥48 H) Permanent Pacemaker Following Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2018, 11, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Mauri, V.; Reimann, A.; Stern, D.; Scherner, M.; Kuhn, E.; Rudolph, V.; Rosenkranz, S.; Eghbalzadeh, K.; Friedrichs, K.; Wahlers, T.; et al. Predictors of Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement with the SAPIEN 3. JACC Cardiovasc. Interv. 2016, 9, 2200–2209. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Van der Boon, R.; de Nicolas, J.M.-M.; Dumonteil, N.; Chieffo, A.; de Jaegere, P.; Tchetche, D.; Marcheix, B.; Millischer, D.; Cassagneau, R.; et al. Impact of permanent pacemaker on mortality after transcatheter aortic valve implantation: The PRAGMATIC (Pooled Rotterdam-Milan-Toulouse in Collaboration) Pacemaker substudy. EuroIntervention 2016, 12, 1185–1193. [Google Scholar] [CrossRef] [PubMed]
- Auffret, V.; Puri, R.; Urena, M.; Chamandi, C.; Rodriguez-Gabella, T.; Philippon, F.; Rodés-Cabau, J. Conduction Disturbances After Transcatheter Aortic Valve Replacement: Current Status and Future Perspectives. Circulation 2017, 136, 1049–1069. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, T.; Yamanaka, F.; Shishido, K.; Moriyama, N.; Komatsu, I.; Yokoyama, H.; Miyashita, H.; Sato, D.; Sugiyama, Y.; Hayashi, T.; et al. Impact of High Implantation of Transcatheter Aortic Valve on Subsequent Conduction Disturbances and Coronary Access. JACC Cardiovasc. Interv. 2023, 16, 1192–1204. [Google Scholar] [CrossRef]
- Defaye, P.; Biffi, M.; El-Chami, M.; Boveda, S.; Glikson, M.; Piccini, J.; Vitolo, M. Cardiac pacing and lead devices management: 25 years of research at EP Europace journal. EP Eur. 2023, 25, euad202. [Google Scholar] [CrossRef]
- Ravaux, J.M.; Di Mauro, M.; Vernooy, K.; Hof, A.W.V.; Veenstra, L.; Kats, S.; Maessen, J.G.; Lorusso, R. Do Women Require Less Permanent Pacemaker After Transcatheter Aortic Valve Implantation? A Meta-Analysis and Meta-Regression. J. Am. Heart Assoc. 2021, 10, e019429. [Google Scholar] [CrossRef] [PubMed]
- MitMitacchione, G.; Schiavone, M.; Gasperetti, A.; Arabia, G.; Breitenstein, A.; Cerini, M.; Palmisano, P.; Montemerlo, E.; Ziacchi, M.; Gulletta, S.; et al. Outcomes of leadless pacemaker implantation following transvenous lead extraction in high-volume referral centers: Real-world data from a large international registry. Heart Rhythm. 2023, 20, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Alhuarrat, M.A.D.; Khawrawala, A.; Renjithlal, S.; Eid, M.M.; Varrias, D.; Mohammed, M.; Grushko, M.; Di Biase, L. Comparison of in-hospital outcomes and complications of leadless pacemaker and traditional transvenous pacemaker implantation. Europace 2023, 25, euad269. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Whole Cohort (n = 1157) | No PPI Group (n= 908) | PPI Group (n = 249) | p Value | |
|---|---|---|---|---|
| Age, y, mean ± SD | 82.02 ± 6.98 | 81.78 ± 6.97 | 82.89 ± 6.96 | 0.015 |
| Female, n (%) | 592 (52.1) | 479 (53.6) | 113 (46.3) | 0.042 |
| BMI, kg/m2, mean ± SD | 26.37 ± 4.58 | 26.33 ± 4.58 | 26.51 ± 4.60 | 0.825 |
| EuroSCORE, mean ± SD | 16.71 ± 11.06 | 16.51 ± 10.94 | 17.43 ± 11.50 | 0.249 |
| Cardiovascular risk factors | ||||
| Hypertension, n (%) | 736 (63.6) | 575 (63.3) | 161 (64.7) | 0.699 |
| Dyslipidaemia, n (%) | 404 (34.9) | 320 (35.2) | 84 (33.7) | 0.659 |
| Non-insulin-dependent diabetes mellitus, n (%) | 262 (22.6) | 202 (22.2) | 60 (24.1) | 0.537 |
| Insulin-dependent diabetes mellitus, n (%) | 75 (6.5) | 60 (6.6) | 15 (6) | 0.740 |
| Current smoker, n (%) | 40 (3.5) | 34 (3.7) | 6 (2.4) | 0.307 |
| Coexisting illnesses | ||||
| Chronic kidney disease (GFR < 60 mL/m2), n (%) | 334 (29) | 251 (27.8) | 83 (33.3) | 0.090 |
| Dialysis, n (%) | 33(2.9) | 31 (3.4) | 2 (0.8) | 0.0295 |
| Coronary artery disease, n (%) | 582 (51.1) | 445 (49.8) | 137 (55.7) | 0.104 |
| Chronic respiratory disease (VEMS < 50%), n (%) | 296 (26.1) | 231 (26) | 65 (26.4) | 0.897 |
| Percutaneous coronary intervention, n (%) | 454 (39.2) | 345 (38) | 109 (43.8) | 0.098 |
| Cerebrovascular disease, n (%) | 95 (8.2) | 73 (8.1) | 22 (8.8) | 0.696 |
| Obliterative arteriopathy in lower limbs, n (%) | 437 (38.5) | 345 (38.8) | 92 (37.6) | 0.720 |
| Atrial fibrillation, n (%) | 291 (25.3) | 216 (23.9) | 75 (30.4) | 0.038 |
| Mitral regurgitation (grade 3+), n (%) | 28 (2.4) | 25 (2.8) | 3 (1.2) | 0.241 |
| Coronary artery bypass surgery, n (%) | 72 (6.2) | 53 (5.8) | 19 (7.6) | 0.301 |
| Previous aortic valve valvuloplasty, n (%) | 183 (15.9) | 141 (15.6) | 42 (16.9) | 0.624 |
| LVEF, %, mean ± SD | 57 ± 11.8 | 57.3 ± 11.8 | 55.9 ± 11.8 | 0.052 |
| Cardiac symptoms, N (%) | ||||
| NYHA functional scale | ||||
| I–II | 296 (26.1) | 243 (27.3) | 53 (21.5) | 0.65 |
| III–IV | 839 (74) | 646 (72.6) | 193 (78.5) | 0.65 |
| Syncope | 45 (3.9) | 35 (3.9) | 10 (4) | 0.907 |
| Hearth failure | 6 (0.5) | 4 (0.4) | 2 (0.8) | 0.615 |
| Angina | 8 (0.7) | 7 (0.8) | 1 (0.4) | 1 |
| Pre-procedure electrocardiographic variables | ||||
| QRS duration, ms, mean ± SD | 99.9 ± 23.8 | 97.4± 22.6 | 108.9 ± 25.9 | <0.0001 |
| PR interval ms, mean ± SD | 176.8 ± 44.1 | 175.4 ± 42.5 | 181.8 ± 49.6 | 0.069 |
| Sinus rhythm, n (%) | 946 (81.8) | 747 (82.3) | 199 (79.9) | 0.395 |
| LVH, n (%) | 8 (0.7) | 7 (0.8) | 1 (0.4) | 1 |
| First-degree AVB, n (%) | 172 (14.9) | 128 (14.1) | 44 (17.7) | 0.160 |
| LBBB, n (%) | 107 (9.2) | 79 (8.7) | 28 (11.2) | 0.22 |
| RBBB, n (%) | 116 (10) | 61 (6.7) | 55 (22.1) | <0.001 |
| Left anterior hemiblock, n (%) | 57 (4.9) | 38 (4.2) | 19 (7.6) | 0.026 |
| Incomplete left bundle branch block, n (%) | 11 (1) | 6 (0.7) | 5 (2) | 0.052 |
| Atrial fibrillation, n (%) | 159 (13.7) | 113 (12.4) | 46 (18.5) | 0.014 |
| Atrial flutter, n (%) | 157 (13.6) | 111 (12.2) | 46 (18.5) | 0.0107 |
| Bradycardia, n (%) | 2 (0.2) | 1 (0.1) | 1 (0.4) | 0.384 |
| Pre-procedure echocardiographic variables | ||||
| Aortic-valve gradient, mmhg, mean ± SD | 50.5 ± 14.3 | 50.8 ± 14.3 | 49.6 ± 14.6 | 0.074 |
| Aortic-valve area, cm2, mean ± SD | 0.957 ± 3.967 | 1.017 ± 4.454 | 0.729 ± 0.473 | 0.594 |
| PAP, mmhg, mean ± SD | 24.9 ± 24.2 | 29.8 ± 35.9 | 26.0 ± 27.3 | 0.078 |
| Baseline treatment, N (%) | ||||
| Amiodarone | 174 (26.3) | 117 (22.9) | 57 (38) | <0.001 |
| β-blocker | 424 (46.5) | 331 (45.6) | 93 (50) | 0.282 |
| Digoxin | 15 (3) | 12 (2.9) | 3 (3.1) | 1 |
| Flecainide | 18 (3.6) | 16 (3.9) | 2 (2.1) | 0.547 |
| Calcium channel antagonists | 49 (9.1) | 39 (9) | 10 (9.7) | 0.818 |
| Whole Cohort (n = 1157) | No PPI Group (n= 908) | PPI Group (n = 249) | p Value | |
|---|---|---|---|---|
| Periprocedural characteristics, N (%) | ||||
| Access route | ||||
| Transfemoral access | 862 (74.6) | 669 (73.7) | 193 (77.8) | 0.107 |
| Trans aortic access | 154 (13.3) | 124 (13.7) | 30 (12.1) | 0.107 |
| Trans carotid access | 87 (7.5) | 76 (8.1) | 11 (4.4) | 0.107 |
| Transapical access | 52 (4.5) | 38 (4.2) | 14 (5.6) | 0.107 |
| Prosthetic valve type | ||||
| Balloon-expandable valve | 1025 (98.6) | 820 (90.4) | 205 (82.3) | <0.001 |
| Self-expandable valve | 131 (11.3) | 87 (9.5) | 44 (17.6) | <0.001 |
| Nominal area oversizing, %, mean ± SD | 12.89 ± 10.77 | 12.64 ± 10.32 | 13.77 ± 12.18 | 0.993 |
| Electrocardiographic variables post-TAVR | ||||
| QRS duration, ms, mean ± SD | 117.3 ± 52.9 | 109.4 ± 54.9 | 150.4 ± 23.6 | <0.0001 |
| PR interval, ms, mean ± SD | 186.4 ± 62.6 | 182.9 ± 56.8 | 202.5 ± 82.4 | <0.0001 |
| Complications N (%) | ||||
| Stroke | 20 (1.7) | 16 (1.8) | 4 (1.6) | 1 |
| Myocardial infarction | 6 (0.6) | 5 (0.6) | 1 (0.4) | 1 |
| Valve migration | 4 (100) | 4 | 0 | - |
| Periprosthetic regurgitation | ||||
| Grade 0 (no regurgitation) | 733 (64.8) | 567 (64.1) | 166 (67.5) | 0.627 |
| Grade 1 (Mild) | 346 (30.6) | 278 (31.4) | 68 (27.7) | 0.627 |
| Grade 2 (Moderate) | 48 (4.2) | 37 (4.2) | 11 (4.5) | 0.627 |
| Grade 3 and 4 (Severe) | 4 (0.4) | 3 (0.3) | 1 (0.4) | 0.627 |
| Severe vascular access complications according to VARC 3 criteria | 55 (5.2) | 42 (5) | 13 (5.8) | 0.634 |
| In-hospital death, n (%) | 42 (3.6) | 37 (4.1) | 5 (2) | 0.122 |
| Length of hospital stay, days, mean ± SD | 10.1 ± 6.3 | 9.6 ± 6.2 | 11.7 ± 6.4 | <0.0001 |
| Estimated one-year mortality (95%, IC), % | 11 (9–12) | 11 (9–13) | 10 (7–15) | 0.749 * |
| Estimated 7-year mortality (95%, IC), % | 58 (53–64) | 57 (50–65) | 63 (54–73) | 0.048 * |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Total Population | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Creatinine serum level | 1.001 (0.99–1.02) | 0.894 | ||
| History of AF | 1.38 (1.02–1.90) | 0.039 | ||
| Baseline electrocardiographic variables | ||||
| AF | 1.62 (1.11–2.37) | 0.011 | ||
| Flutter | 2 (1.42–2.81) | |||
| RBBB | 3.94 (2.64–5.85) | <0.0001 | 2.49 (1.4–4.30) | 0.001 |
| Left anterior hemiblock | 1.89 (1.07–3.34) | 0.028 | ||
| Longer baseline QRS duration | 1.019 (1.013–1.025) | <0.0001 | 1.01 (1.004–1.02) | 0.0028 |
| Echocardiographic and CT scan variables | ||||
| Aortic annulus diameter in Echocardiography | 1.104 (1.026–1.187) | 0.008 | ||
| Aortic annulus diameter in CT scan | 1.125 (1.054–1.202) | 0.0004 | ||
| Baseline treatment | ||||
| Preoperative amiodarone | 2.07 (1.4–3.05) | 0.0002 | ||
| Valve type | ||||
| Self-expandable valves | 2.02 (1.36–3.00) | 0.0004 | 1.82 (1.09–3.04) | 0.021 |
| Post-TAVR electrocardiographic variables | ||||
| QRS duration (ms) | 1.040 (1.03–1.05) | <0.0001 | ||
| PR interval (ms) | 1.005 (1.00–1.01) | 0.0003 | ||
| 2012–2014 (n = 220) | 2015–2017 (n = 528) | 2018–2019 (n = 409) | p Value | |
|---|---|---|---|---|
| Access route | ||||
| Transfemoral, n (%) | 127 (58) | 407 (77.5) | 327 (86.3) | - |
| Trans aortic, n (%) | 63 (28.8) | 80 (15.2) | 11 (2.9) | - |
| Trans carotid, n (%) | 0 (0) | 4 (0.8) | 19 (5) | - |
| Transapical, n (%) | 25 (11.4) | 21 (4) | 5 (1.3) | - |
| Type of valve | ||||
| Balloon-expandable valve, n (%) | 157 (71.4) | 503 (95.3%) | 365 (89.5) | <0.001 |
| Self-expandable valve, n (%) | 63 (28.6) | 25 (4.7) | 43 (10.6) | <0.001 |
| Nominal area oversizing, %, mean ± SD | 15.2 ± 16.7 | 13.7 ± 8.3 | 12.9 ± 10.7 | <0.0001 |
| PPI rate, n (%) | 65 (29.5) | 128 (24.2) | 56 (13.7) | <0.001 |
| PPI indication | ||||
| third-degree atrioventricular block, n (%) | 16 (32) | 63 (51.6) | 25 (48.1) | <0.001 |
| LBBB with pathological electrophysiologic exploration, n (%) | 9 (18) | 24 (19.7) | 22 (42.3) | <0.001 |
| LBBB without electrophysiologic exploration, n (%) | 18 (36) | 29 (23.8) | 1 (1.9) | <0.001 |
| Second-degree atrioventricular block, n (%) | 1 (2) | 3 (2.5) | 2 (3.8) | <0.001 |
| Others, n (%) | 4 (8) | 3 (2.5) | 1 (1.9) | <0.001 |
| Complications N (%) | ||||
| Stroke | 3 (1.4) | 11 (2.1) | 6 (1.5) | 0.80 |
| Myocardial infarction | 2 (0.9) | 3 (0.6) | 1 (0.3) | 0.43 |
| Valve migration | 0 | 3 (0.75) | 1 (0.25) | - |
| Periprosthetic regurgitation | ||||
| Grade 0 (no regurgitation) | 95 (44%) | 387 (73.6%) | 251 (64.5%) | <0.001 |
| Grade 1 (mild) | 100 (46.3%) | 130 (24.7%) | 116 (29.8%) | <0.001 |
| Grade 2 (moderate) | 20 (9.3%) | 8 (1.5%) | 20 (5.1%) | <0.001 |
| Grade 3 and 4 (Severe) | 1 (0.5%) | 1 (0.2%) | 2 (0.5%) | <0.001 |
| In-hospital death, n (%) | 14 (6.4) | 22 (4.2) | 6 (1.5) | 0.005 |
| Length of hospital stay, days, mean ± SD | 13.4 ± 9.2 | 9.5 ± 5 | 9 ± 5.1 | <0.0001 |
| Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| Total Population | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Age | 1.021 (1.003–1.04) | 0.023 | ||
| Female | 0.896 (0.7–1.15) | 0.382 | ||
| Coexisting illness | ||||
| Chronic kidney disease | 1.74 (1.33–2.26) | <0.0001 | 1.53 (1.11–2.12) | 0.01 |
| Chronic respiratory disease | 1.58 (1.2–2.08) | 0.001 | 1.45 (1.04–2.03) | 0.03 |
| Dialysis | 2.75 (1.36- 5.56) | 0.005 | ||
| Mitral regurgitation | 2.32 (1.09–4.93) | 0.028 | ||
| Obliterative arteriopathy in lower limbs | 1.39 (1.07–1.78) | 0.011 | 1.38 (1.02–1.87) | 0.04 |
| Cardiac symptoms | ||||
| NYHA functional disease | ||||
| I-II | 1.397 (0.626–3.116) | 0.414 | ||
| Syncope | 2.067 (0.990–4.356) | 0.053 | ||
| ECG variables at baseline | ||||
| Sinus Rhythm | 1.86 (1.37–2.52) | <0.0001 | ||
| Narrow QRS complex (<120 ms) | 1.61 (1.23–2.09) | 0.0005 | ||
| AF | 2 (1.43–2.78) | <0.0001 | 1.95 (1.4–2.71) | <0.001 |
| Access route | ||||
| Trans aortic | 3.768 (2.642–5.375) | <0.0001 | ||
| Trans carotid | 0.520 (0.175–1.545) | 0.239 | ||
| Transapical | 1.875 (1.057–3.327) | 0.032 | ||
| Valve type | ||||
| Balloon-expandable valve | 0.718 (0.495–1.042) | 0.0809 | ||
| Nominal area oversizing | 1.02 (0.97–1.07) | 0.527 | ||
| Need for PPI | 1.71 (1.28–2.28) | 0.0003 | 2.49 (1.4–4.3) | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panagides, V.; Sakka, E.; Cheneau, E.; Bouharaoua, A.; Vicat, J.; Leude-Vaillant, E.; Rochas, P.; Collet, F.; Giacomoni, M.-P. Prognosis and Predictor Factors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: A Retrospective Analysis of the Post-Transcatheter Aortic Replacement Clairval Hospital Registry. J. Clin. Med. 2024, 13, 3050. https://doi.org/10.3390/jcm13113050
Panagides V, Sakka E, Cheneau E, Bouharaoua A, Vicat J, Leude-Vaillant E, Rochas P, Collet F, Giacomoni M-P. Prognosis and Predictor Factors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: A Retrospective Analysis of the Post-Transcatheter Aortic Replacement Clairval Hospital Registry. Journal of Clinical Medicine. 2024; 13(11):3050. https://doi.org/10.3390/jcm13113050
Chicago/Turabian StylePanagides, Vassili, Emna Sakka, Edouard Cheneau, Ahmed Bouharaoua, Jacques Vicat, Elisabeth Leude-Vaillant, Philippe Rochas, Frédéric Collet, and Marie-Paule Giacomoni. 2024. "Prognosis and Predictor Factors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: A Retrospective Analysis of the Post-Transcatheter Aortic Replacement Clairval Hospital Registry" Journal of Clinical Medicine 13, no. 11: 3050. https://doi.org/10.3390/jcm13113050
APA StylePanagides, V., Sakka, E., Cheneau, E., Bouharaoua, A., Vicat, J., Leude-Vaillant, E., Rochas, P., Collet, F., & Giacomoni, M.-P. (2024). Prognosis and Predictor Factors of Permanent Pacemaker Implantation after Transcatheter Aortic Valve Replacement: A Retrospective Analysis of the Post-Transcatheter Aortic Replacement Clairval Hospital Registry. Journal of Clinical Medicine, 13(11), 3050. https://doi.org/10.3390/jcm13113050