
Management of Teeth with Grade 3 Endo-Periodontal Lesions by Combined Endodontic and Regenerative Periodontal Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
- Grade 3 endo-periodontal lesion;
- Endodontic treatment was performed first and followed by periodontal regenerative surgery;
- One- or two-wall intra-bony defects suitable for periodontal regenerative surgery;
- Adequate oral hygiene and control of inflammation: full-mouth plaque score (FMPS) of ≤20% and full-mouth bleeding score (FMBS) of ≤20%;
- Clinical and radiographic data of a consecutive follow-up of at least 1 year after regenerative therapy.
- Exclusion criteria for the analysis were as follows:
- Non-compliance;
- Incomplete probing or radiographic data;
- Heavy smokers > 10 cigarettes per day;
- Resective periodontal surgery on target tooth;
- Teeth with fractures, external or internal resorption;
- Additional periodontal or maxillofacial treatment in the areas of interest;
- Systemic diseases (e.g., uncontrolled diabetes).
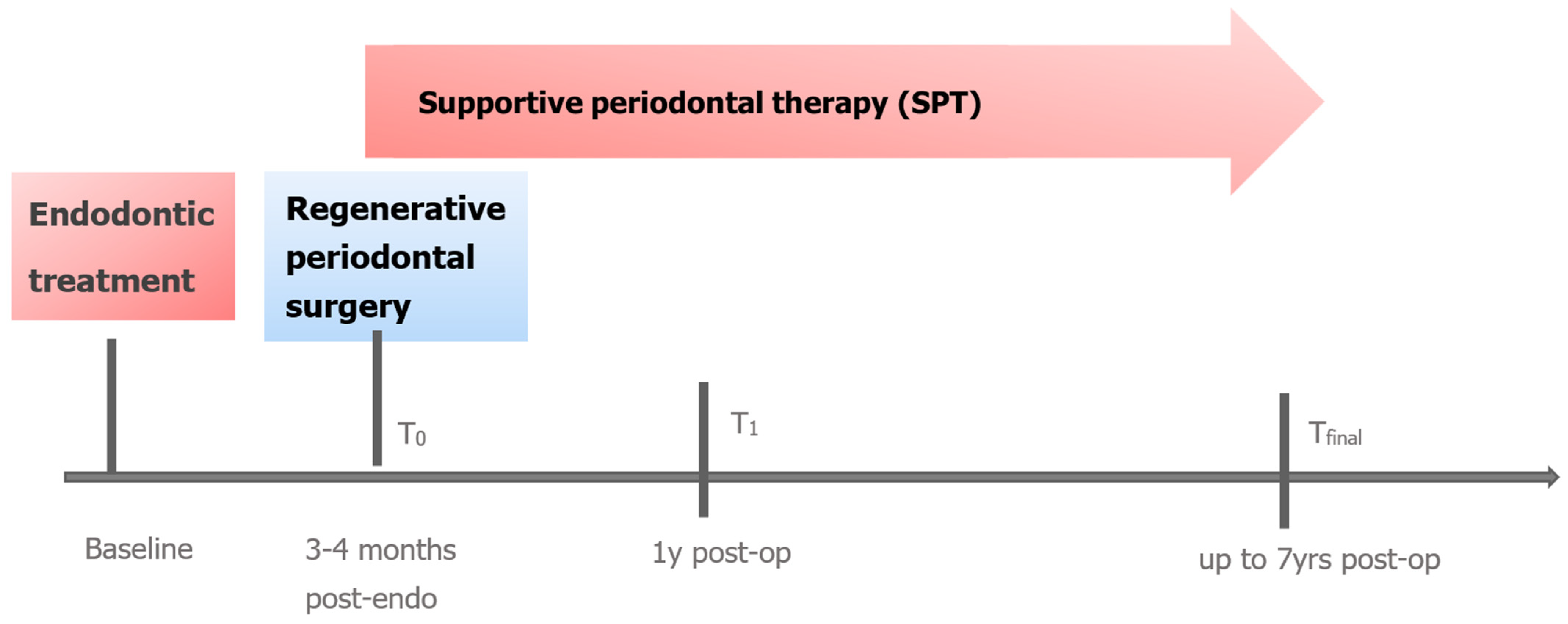
2.2. Treatment
2.2.1. Endodontic Therapy
2.2.2. Regenerative Periodontal Surgery
2.2.3. Supportive Periodontal Therapy
2.3. Clinical and Radiographic Assessments
- Probing pocket depth (PPD) at 6 sites per tooth;
- Full-mouth plaque scores (FMPS), Full mouth bleeding scores (FMBS);
- Tooth mobility (Miller, 1938) [27].
2.4. Statistical Analysis
3. Results
3.1. Patient and Defect Characteristics
3.2. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrera, D.; Retamal-Valdes, B.; Alonso, B.; Feres, M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), 578–594. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. 20), 162–170. [Google Scholar] [CrossRef] [PubMed]
- Ruetters, M.; Gehrig, H.; Kronsteiner, D.; Schuessler, D.L.; Kim, T.S. Prevalence of endo-perio lesions according to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Disease in a university hospital. Quintessence Int. 2022, 53, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Stalpers, G.; Mollo, A.; Tonetti, M.S. Periodontal regeneration versus extraction and prosthetic replacement of teeth severely compromised by attachment loss to the apex: 5-year results of an ongoing randomized clinical trial. J. Clin. Periodontol. 2011, 38, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Stalpers, G.; Mollo, A.; Tonetti, M.S. Periodontal regeneration versus extraction and dental implant or prosthetic replacement of teeth severely compromised by attachment loss to the apex: A randomized controlled clinical trial reporting 10-year outcomes, survival analysis and mean cumulative cost of recurrence. J. Clin. Periodontol. 2020, 47, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berghlund, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49 (Suppl. 24), 4–71. [Google Scholar] [CrossRef]
- Zehnder, M.; Gold, S.I.; Hasselgren, G. Pathologic interactions in pulpal and periodontal tissues. J. Clin. Periodontol. 2002, 29, 663–671. [Google Scholar] [CrossRef]
- Schmidt, J.C.; Walter, C.; Amato, M.; Weiger, R. Treatment of periodontal-endodontic lesions—A systematic review. J. Clin. Periodontol. 2014, 41, 779–790. [Google Scholar] [CrossRef]
- Ruetters, M.; Kim, T.S.; Krisam, J.; El-Sayed, S.; El Sayed, N. Effect of endodontic treatment on periodontal healing of grade 3 endo-periodontal lesions without root damage in periodontally compromised patients—A retrospective pilot study. Clin. Oral Investig. 2021, 25, 2373–2380. [Google Scholar] [CrossRef]
- Gupta, S.; Tewari, S.; Tewari, S.; Mittal, S. Effect of Time Lapse between Endodontic and Periodontal Therapies on the Healing of Concurrent Endodontic-Periodontal Lesions without Communication: A Prospective Randomized Clinical Trial. J. Endod. 2015, 41, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Dong, T.; Zhang, Y.; Li, X. Time-lapse between periodontal regeneration surgery and root canal therapy in severe combined periodontal-endodontic lesions. Saudi Dent J. 2023, 35, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Tonetti, M.S. Clinical concepts for regenerative therapy in intrabony defects. Periodontol 2000 2015, 68, 282–307. [Google Scholar] [CrossRef] [PubMed]
- Bröseler, F.; Tietmann, C.; Hinz, A.; Jepsen, S. Long-term results of periodontal regenerative therapy: A retrospective practice-based cohort study. J. Clin. Periodontol. 2017, 44, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Sun, C.; Akcalı, A.; Yeh, Y.-C.; Tu, Y.; Donos, N. The effect of horizontal and vertical furcation involvement on molar survival: A retrospective study. J. Clin. Periodontol. 2017, 45, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Koidou, V.; Nieri, M.; Barbato, L.; Pagliaro, U.; Cairo, F. Regenerative surgery versus access flap for the treatment of intrabony periodontal defects. A systematic review and meta-analysis. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 320–351. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos, A.; Bertl, K.; Spinelli, L.; Sculean, A.; Cortellini, P.; Tonetti, M.S. Medium- and long-term clinical benefits of periodontal regenerative/reconstructive procedures in intrabony defects: Systematic review and network meta-analysis of randomized controlled clinical studies. J. Clin. Periodontol. 2021, 48, 410–430. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, C.; Virzì, M.; Schupbach, P.; Broccaioli, A.; Simion, M. Treatment of combined endodontic-periodontic lesions using guided tissue regeneration: Clinical case and histology. Int. J. Periodontics Restorative Dent. 2012, 32, 433–439. [Google Scholar]
- Aksel, H.; Serper, A. A case series associated with different kinds of endo-perio lesions. J. Clin. Exp. Dent. 2014, 6, e91–e95. [Google Scholar] [CrossRef]
- Pico-Blanco, A.; Castelo-Baz, P.; Caneiro-Queija, L.; Liñares-González, A.; Martin-Lancharro, P.; Blanco-Carrión, J. Saving Single-rooted Teeth with Combined Endodontic-periodontal Lesions. J. Endod. 2016, 42, 1859–1864. [Google Scholar] [CrossRef]
- Arx, T.; Bosshardt, D. The use of Enamel Matrix Derivative (Emd) for Treatment of Combined Apicomarginal Lesions in Apical Surgery: A Retrospecitve Analysis. Eur. Endod. J. 2018, 3, 146–152. [Google Scholar]
- AlJasser, R.; Bukhary, S.; AlSarhan, M.; Alotaibi, D.; AlOraini, S.; Habib, S.R. Regenerative Therapy Modality for Treatment of True Combined Endodontic-Periodontal Lesions: A Randomized Controlled Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 6220. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Chung, S.H.; Han, J.Y. Periodontal regenerative therapy in endo-periodontal lesions: A retrospective study over 5 years. J. Periodont. Impl. Sci. 2019, 49, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Hamp, S.; Nyman, S.; Lindhe, J. Periodontal treatment of multirooted teeth. Results after 5 years. J. Clin. Periodontol. 1975, 49, 225–237. [Google Scholar]
- Tarnow, D.; Fletcher, P. Classification of the vertical component of furcation involvement. J. Periodontol. 1984, 55, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, K.; Sculean, A.; Jepsen, S. Complications and treatment errors related to regenerative periodontal surgery. Periodontol 2000 2023, 92, 120–134. [Google Scholar] [CrossRef] [PubMed]
- Miller, S. Textbook of Periodontia; Blakiston Company: Philadelphia, PA, USA, 1950. [Google Scholar]
- Rosner, B.; Glynn, R.; Lee, M.L. The Wilcoxon signed rank test for paired comparisons of clustered data. Biometrics 2006, 62, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.; Satten, G.A. A signed-Rank Test for Clustered Data. Biometrics 2008, 64, 501–507. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 23 December 2022).
- Hothorn, T.; Hornik, K.; van den Weil, M.A.; Zeileis, A. Implementing a class of permutation tests: The coin package. J. Stat. Softw. 2008, 28, 1–23. [Google Scholar] [CrossRef]
- López-Valverde, I.; Vignoletti, F.; Vignoletti, G.; Martin, C.; Sanz, M. Long-term tooth survival and success following primary root canal treatment: A 5-to 37-year retrospective observation. Clin. Oral Investig. 2023, 27, 3233–3244. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Christiansen, A.L.; Cortellini, P. Vertical subclassification predicts survival of molars with class II furcation involvement during supportive periodontal care. J. Clin. Periodontol. 2017, 44, 1140–1144. [Google Scholar] [CrossRef]
- Cortellini, P.; Cortellini, S.; Tonetti, M.S. Papilla preservation flaps for periodontal regeneration of molars severely compromised by combined furcation and intrabony defects: Retrospective analysis of a registry-based cohort. J. Periodontol. 2020, 91, 165–173. [Google Scholar] [CrossRef]
- Salvi, G.; Mischler, D.; Schmidlin, K.; Matuliene, G.; Pjetursson, B.; Brägger, U.; Lang, N.P. Risk factors associated with the longevity of multi-rooted teeth. Long-term outcomes after active and supportive periodontal therapy. J. Clin. Periodontol. 2014, 41, 701–707. [Google Scholar] [CrossRef]
- Jepsen, S.; Gennai, S.; Hirschfeld, S.; Kalemai, Z.; Buti, J.; Graziani, F. Regenerative surgical treatment of furcation defects: A systematic review and Bayesian network meta-analysis of randomized clinical trials. J. Clin Periodontol. 2020, 47 (Suppl. 22), 352–374. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Demographic Characteristics (n = 35) | |
|---|---|
| Female gender | 22/62.9% |
| Male gender | 13/37.1% |
| Age (mean ± SD/range) | 63.7 ± 9.06 (47–83 yrs) |
| Smokers | 8/22.8% |
| Time between endodontic and regenerative therapy (mean ± SD month) | 3.89 ± 3.84 |
| Defect characteristics (n = 39) | |
| Single-rooted | 13 |
| Multi-rooted (2 premolars, 24 molars) | 26 |
| Mandibular molars with/without furcation involvement | 11/6 |
| Maxillary molars with/without furcation involvement | 7/0 |
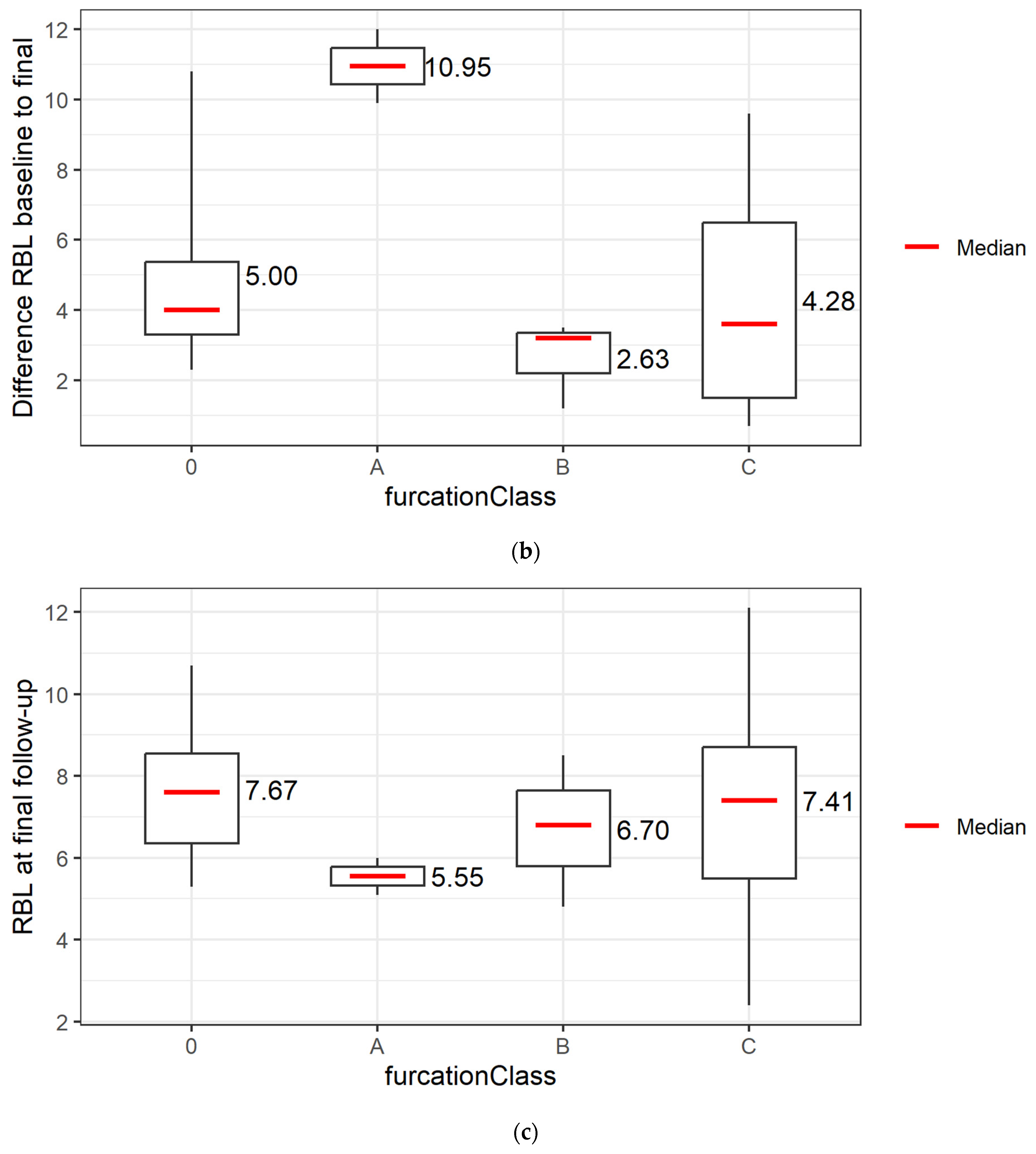
| Molars with horizontal furcation class I/II/III * | 4/13/1 |
| Molars with furcation involvement—subclass A** | 2 |
| Molars with furcation involvement—subclass B ** | 3 |
| Molars with furcation involvement—subclass C ** | 13 |
| Probing pocket depth at deepest site (mean ± SD/mm) | 9.21 ± 2.15 |
| Bone level (CEJ to bottom of defect intrasurgically) at deepest site (mean ± SD/mm) | 12.54 ± 3.44 |
| Follow-up time (mean ± SD / months) baseline | 31.41 ± 21.92 |
| Occlusal wear (teeth %) | 48.7% |
| Full Mouth Bleeding Score (mean ± SD/%) | 23.16 ± 16.67 |
| Full Mouth Plaque Score (mean ± SD/%) | 28.80 ± 13.30 |
| (a) | |||||
| N | T0 | T1 | Tfinal | ||
| rBL per tooth | 39 | 12.54 ± 3.36 | 7.95 ± 2.65 | NA | |
| rBL per tooth with final follow-up > 12 months | 23 | 13.09 ± 3.12 | 8.21 ± 3.08 | 8.39 ± 3.70 | |
| (b) | |||||
| T0.T1 | T0.Tfinal | T1.Tfinal | |||
| rBL per tooth for all 39 teeth | 1.00 × 10−7 | 1.00 × 10−7 | NA | ||
| rBL per tooth for 23 teeth with final follow-up > 12 months | 3.35 × 10−5 | 3.83 × 10−5 | 0.78 | ||
| (c) | |||||
| N | T0 | T1 | Tfinal | ||
| PPD per tooth | 39 | 9.21 ± 2.15 | 5.21 ± 1.79 | NA ± | |
| PPD per tooth with final follow-up > 12 months | 23 | 9.74 ± 2.05 | 5.04 ± 1.61 | 4.87 ± 2.32 | |
| (d) | |||||
| PPD (mm) | Baseline T0 | T1 | Tfinal | ||
| ≤4 | 0 (0.00%) | 8 (34.78%) | 12 (52.17%) | ||
| 5 | 0 (0.00%) | 6 (26.09%) | 4 (17.39%) | ||
| 6 | 0 (0.00%) | 4 (17.39%) | 2 (8.70%) | ||
| 7 | 2 (8.70%) | 4 (17.39%) | 2 (8.70%) | ||
| 8 | 4 (17.39%) | 1 (4.35%) | 1 (4.35%) | ||
| 9 | 4 (17.39%) | 0 (0.00%) | 0 (0.00%) | ||
| 10 | 5 (21.74%) | 0 (0.00%) | 2 (8.70%) | ||
| 11 | 1 (4.35%) | 0 (0.00%) | 0 (0.00%) | ||
| 12 | 7 (30.43%) | 0 (0.00%) | 0 (0.00%) | ||
| (e) | |||||
| comparison | p-value | ||||
| pc0–pc1 | 0.0122 | ||||
| pc0–pcfinal | 0.0050 | ||||
| Pc1–pcfinal | 0.3742 | ||||
| (a) | |||
| Molars with/without horizontal furcation class (n = 24) * | T0 | T1 | Tfinal |
| N = 24 | N = 24 | N = 16 | |
| 0 | 6 (25%) | 10 (42%) | 7 (44%) |
| I | 4 (17%) | 11 (46%) | 7 (44%) |
| II | 13 (54%) | 3 (13%) | 2 (12%) |
| III | 1 (4%) | 0 (0%) | 0 (0%) |
| Conversion of horizontal furcation class | N = 14 | ||
| → FII FI | 10 | ||
| → FI F0 | 2 | ||
| → FII F0 | 1 | ||
| → FIII FI | 1 | ||
| No conversion of horizontal furcation class | N = 4 | ||
| FI = FI | 2 | 7 | |
| FII = FII | 2 | 2 | |
| F0 = F0 | - | 7 | |
| (b) | |||
| Vertical furcation subclass ** (n = 18) | T0 | T1 | Tfinal |
| N = 18 | N = 18 | N = 16 | |
| A | 2 (11%) | 7 (39%) | 7 (44%) |
| B | 3 (17%) | 11 (61%) | 9 (56%) |
| C | 13 (72%) | 0 (0%) | 0 (0%) |
| Conversion of vertical furcation subclass | |||
| → B A | ./. | 2 | 1 |
| → C B | ./. | 10 | 1 |
| → C A | ./. | 3 | 2 |
| → B C → A B | 7 | 0 | 1 extraction 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tietmann, C.; Tezer, I.; Youssef, E.; Jepsen, S.; Jepsen, K. Management of Teeth with Grade 3 Endo-Periodontal Lesions by Combined Endodontic and Regenerative Periodontal Therapy. J. Clin. Med. 2024, 13, 93. https://doi.org/10.3390/jcm13010093
Tietmann C, Tezer I, Youssef E, Jepsen S, Jepsen K. Management of Teeth with Grade 3 Endo-Periodontal Lesions by Combined Endodontic and Regenerative Periodontal Therapy. Journal of Clinical Medicine. 2024; 13(1):93. https://doi.org/10.3390/jcm13010093
Chicago/Turabian StyleTietmann, Christina, Ivet Tezer, Emad Youssef, Søren Jepsen, and Karin Jepsen. 2024. "Management of Teeth with Grade 3 Endo-Periodontal Lesions by Combined Endodontic and Regenerative Periodontal Therapy" Journal of Clinical Medicine 13, no. 1: 93. https://doi.org/10.3390/jcm13010093
APA StyleTietmann, C., Tezer, I., Youssef, E., Jepsen, S., & Jepsen, K. (2024). Management of Teeth with Grade 3 Endo-Periodontal Lesions by Combined Endodontic and Regenerative Periodontal Therapy. Journal of Clinical Medicine, 13(1), 93. https://doi.org/10.3390/jcm13010093