

High-Flow Nasal Cannula Therapy as an Adjuvant Therapy for Respiratory Support during Endoscopic Techniques: A Narrative Review

 ,
,
Abstract
:1. Introduction
- -
- Sedation, necessary for patient toleration of the technique, may induce respiratory depression, requiring airway interventions such as mandibular traction, oropharyngeal airway device insertion, non-invasive ventilation (NIV), and even orotracheal intubation (OTI) and invasive mechanical ventilation.
- -
- Other circumstances that arise during fiberoptic bronchoscopy (FOB) include:
- The effective airway diameter is reduced when advancing the bronchoscope beyond the glottis; suctioning during FOB can result in alveolar recruitment loss and atelectasis formation.
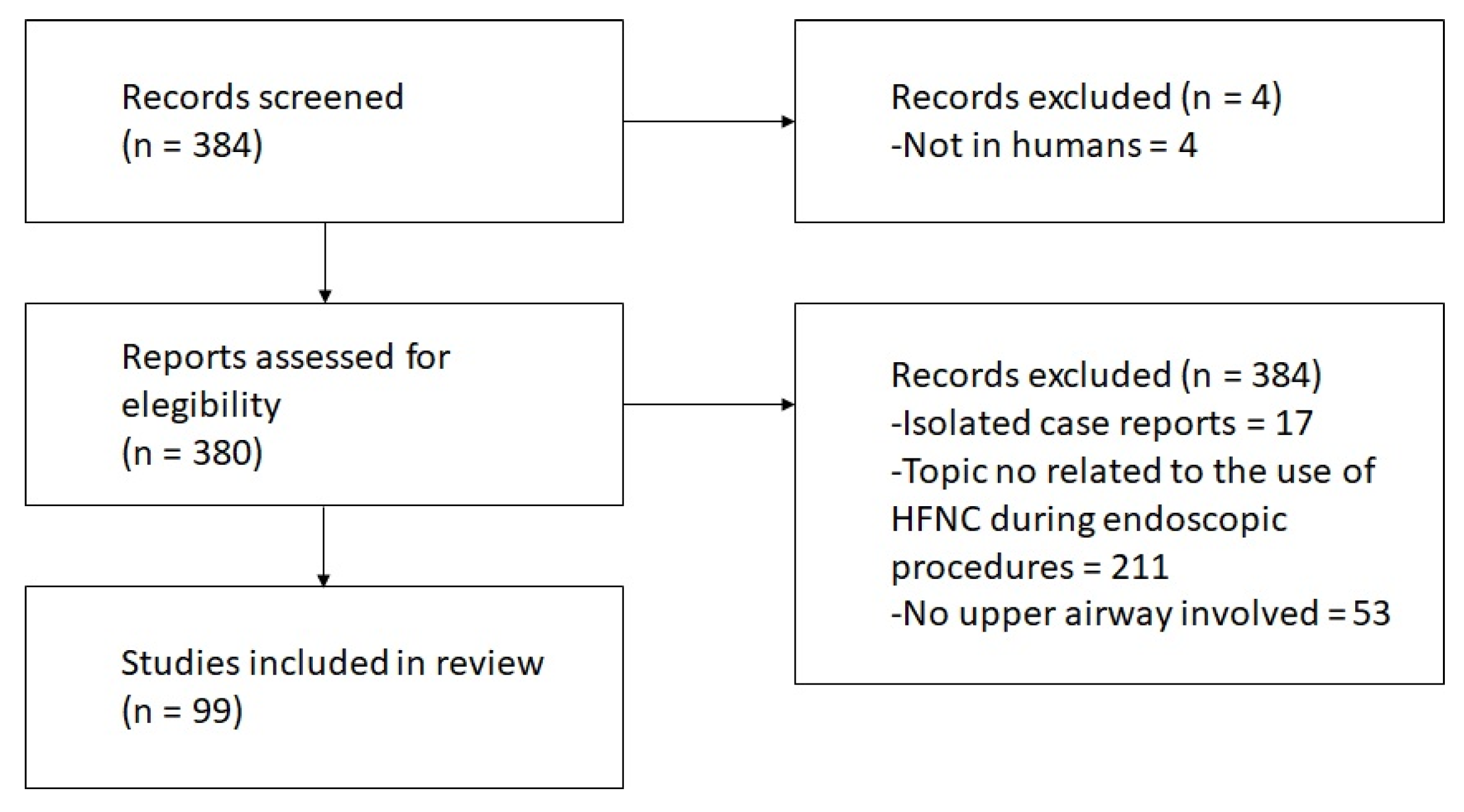
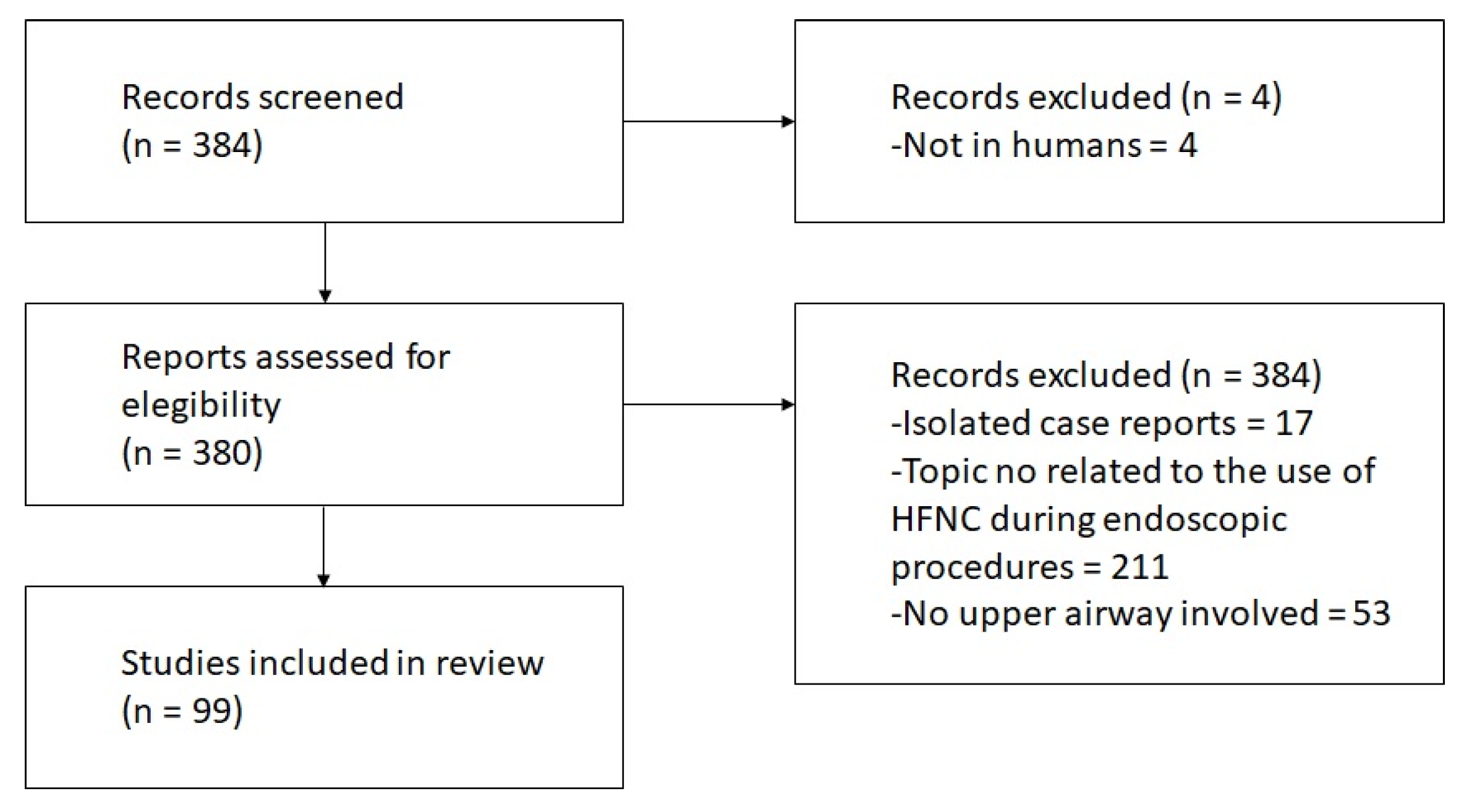
2. Materials and Methods
- Title: Do not consider it a systematic review, as our intention was to perform a narrative review;
- No risk bias assessment nor effect measurements were performed, as we did not intend to perform a meta-analysis.
3. Search Results and Main Findings of Included Trials
4. HFNC in FOB
4.1. HFNC vs. Other Oxygen Supply Systems during FOB
4.1.1. HFNC vs. COT
4.1.2. HFNC vs. CPAP/NIV
4.2. HFNC in Special Procedures and Situations
5. HFNC in Upper Gastrointestinal Endoscopy
5.1. HFNC vs. COT in Hypoxemia Prevention
5.2. HFNC and Hyperoxia Management
5.3. HFNC vs. COT in Hypercapnia Management
5.4. HFNC vs. COT in a High-Risk Population
6. HFNC in Surgical Procedures
6.1. Laryngeal Surgery
6.2. Thoracic Surgery
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ischaki, E.; Pantazopoulos, I.; Zakynthinos, S. Nasal high flow therapy: A novel treatment rather than a more expensive oxygen device. Eur. Respir. Rev. 2017, 26, 170028. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, R.F.; Hart, N.; Kaltsakas, G. High-flow therapy: Physiological effects and clinical applications. Breathe 2020, 16, 200224. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M.; Meade, S.; Summers, C.; McAuley, D.F.; Proudfoot, A.; Baladia, M.M.; Dark, P.M.; Diomede, K.; Finney, S.J.; Forni, L.G.; et al. RAND appropriateness panel to determine the applicability of UK guidelines on the management of acute respiratory distress syndrome (ARDS) and other strategies in the context of the COVID-19 pandemic. Thorax 2022, 77, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Oczkowski, S.; Ergan, B.; Bos, L.; Chatwin, M.; Ferrer, M.; Gregoretti, C.; Heunks, L.; Frat, J.-P.; Longhini, F.; Nava, S.; et al. ERS clinical practice guidelines: High-flow nasal cannula in acute respiratory failure. Eur. Respir. J. 2022, 59, 2101574. [Google Scholar] [CrossRef] [PubMed]
- Stahl, D.L.; Richard, K.M.; Papadimos, T.J. Complications of bronchoscopy: A concise synopsis. Int. J. Crit. Illn. Inj. Sci. 2015, 5, 189–195. [Google Scholar] [PubMed]
- Pelaia, C.; Bruni, A.; Garofalo, E.; Rovida, S.; Arrighi, E.; Cammarota, G.; Navalesi, P.; Pelaia, G.; Longhini, F. Oxygenation strategies during flexible bronchoscopy: A review of the literature. Respir. Res. 2021, 22, 253. [Google Scholar] [CrossRef]
- Roy, A.; Khanna, P.; Chowdhury, S.R.; Haritha, D.; Sarkar, S. The Impact of High-flow Nasal Cannula vs Other Oxygen Delivery Devices during Bronchoscopy under Sedation: A Systematic Review and Meta-analyses. Indian J. Crit. Care Med. 2022, 26, 1131–1140. [Google Scholar]
- Sampsonas, F.; Karamouzos, V.; Karampitsakos, T.; Papaioannou, O.; Katsaras, M.; Lagadinou, M.; Zarkadi, E.; Malakounidou, E.; Velissaris, D.; Stratakos, G.; et al. High-Flow vs. Low-Flow Nasal Cannula in Reducing Hypoxemic Events During Bronchoscopic Procedures: A Systematic Review and Meta-Analysis. Front. Med. 2022, 9, 815799. [Google Scholar] [CrossRef]
- Su, C.L.; Chiang, L.L.; Tam, K.W.; Chen, T.T.; Hu, M.C. High-flow nasal cannula for reducing hypoxemic events in patients undergoing bronchoscopy: A systematic review and meta-analysis of randomized trials. PLoS ONE 2021, 16, e0260716. [Google Scholar] [CrossRef]
- Thiruvenkatarajan, V.; Sekhar, V.; Wong, D.T.; Currie, J.; Van Wijk, R.; Ludbrook, G.L. Effect of high-flow nasal oxygen on hypoxaemia during procedural sedation: A systematic review and meta-analysis. Anaesthesia 2023, 78, 81–92. [Google Scholar] [CrossRef]
- Page, M.J.; E McKenzie, J.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; A Akl, E.; E Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Arias-Sanchez, P.P.; Ledesma, G.; Cobos, J.; Tirape, H.; Jaramillo, B.; Ruiz, J.; Pacheco, L.; Martinez, J.; Maldonado, R.; Andrade, L.; et al. Changes in Oxygen Saturation During Fiberoptic Bronchoscopy: High-Flow Nasal Cannula versus Standard Oxygen Therapy. Respir. Care 2023, 68, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, J.L.; Fu, S.; Zhou, J.M.; Zhu, Y.J.; Cai, S.N.; Fang, J.; Xie, K.-J.; Chen, X.-Z. Incidence of oxygen desaturation using a high-flow nasal cannula versus a facemask during flexible bronchoscopy in patients at risk of hypoxemia: A randomised controlled trial. BMC Pulm. Med. 2022, 22, 389. [Google Scholar]
- Longhini, F.; Pelaia, C.; Garofalo, E.; Bruni, A.; Placida, R.; Iaquinta, C.; Arrighi, E.; Perri, G.; Procopio, G.; Cancelliere, A.; et al. High-flow nasal cannula oxygen therapy for outpatients undergoing flexible bronchoscopy: A randomised controlled trial. Thorax 2022, 77, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Braune, S.; Frings, D.; Wiontzek, A.K.; Klose, H.; Kluge, S. High-flow nasal cannula oxygen versus non-invasive ventilation in patients with acute hypoxaemic respiratory failure undergoing flexible bronchoscopy—A prospective randomised trial. Crit. Care 2014, 18, 712. [Google Scholar] [CrossRef]
- Douglas, N.; Ng, I.; Nazeem, F.; Lee, K.; Mezzavia, P.; Krieser, R.; Steinfort, D.; Irving, L.; Segal, R. A randomised controlled trial comparing high-flow nasal oxygen with standard management for conscious sedation during bronchoscopy. Anaesthesia 2018, 73, 169–176. [Google Scholar] [CrossRef]
- Mazzeffi, M.A.; Petrick, K.M.; Magder, L.; Greenwald, B.D.; Darwin, P.; Goldberg, E.M.; Bigeleisen, P.; Chow, J.H.; Anders, M.; Boyd, C.M.; et al. High-Flow Nasal Cannula Oxygen in Patients Having Anesthesia for Advanced Esophagogastroduodenoscopy: HIFLOW-ENDO, a Randomized Clinical Trial. Anesth. Analg. 2021, 132, 743–751. [Google Scholar] [CrossRef]
- Thiruvenkatarajan, V.; Dharmalingam, A.; Arenas, G.; Wahba, M.; Liu, W.M.; Zaw, Y.; Steiner, R.; Tran, A.; Currie, J. Effect of high-flow vs. low-flow nasal plus mouthguard oxygen therapy on hypoxaemia during sedation: A multicentre randomised controlled trial. Anaesthesia 2022, 77, 46–53. [Google Scholar] [CrossRef]
- Zhang, W.; Yin, H.; Xu, Y.; Fang, Z.; Wang, W.; Zhang, C.; Shi, H.; Wang, X. The effect of varying inhaled oxygen concentrations of high-flow nasal cannula oxygen therapy during gastroscopy with propofol sedation in elderly patients: A randomized controlled study. BMC Anesthesiol. 2022, 22, 335. [Google Scholar] [CrossRef]
- Sawase, H.; Ozawa, E.; Yano, H.; Ichinomiya, T.; Yano, R.; Miyaaki, H.; Komatsu, N.; Ayuse, T.; Kurata, S.; Sato, S.; et al. Respiratory support with nasal high flow without supplemental oxygen in patients undergoing endoscopic retrograde cholangiopancreatography under moderate sedation: A prospective, randomized, single-center clinical trial. BMC Anesthesiol. 2023, 23, 156. [Google Scholar] [CrossRef]
- Kim, S.H.; Bang, S.; Lee, K.-Y.; Park, S.W.; Park, J.Y.; Lee, H.S.; Oh, H.; Oh, Y.J. Comparison of high flow nasal oxygen and conventional nasal cannula during gastrointestinal endoscopic sedation in the prone position: A randomized trial. Can. J. Anaesth. 2021, 68, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.Y.; Lin, F.S.; Shih, C.C.; Sung, Y.J.; Chen, A.Y.; Piao, Y.C.; Chen, J.-S.; Cheng, Y.-C. Comparisons on the intraoperative desaturation and postoperative outcomes in non-intubated video-assisted thoracic surgery with supraglottic airway devices or high-flow nasal oxygen: A retrospective study. J. Formos. Med. Assoc. 2023, 122, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Flach, S.; Elhoweris, A.; Majumdar, S.; Crawley, S.; Manickavasagam, J. Transoral laser microsurgery using high-flow nasal cannula oxygenation: Our experience of 21 cases. Clin. Otolaryngol. 2019, 44, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Ke, H.H.; Hsu, P.K.; Tsou, M.Y.; Ting, C.K. Nonintubated video-assisted thoracic surgery with high-flow oxygen therapy shorten hospital stay. J. Chin. Med. Assoc. 2020, 83, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Benninger, M.S.; Zhang, E.S.; Chen, B.; Tierney, W.S.; Abdelmalak, B.; Bryson, P.C. Utility of Transnasal Humidified Rapid Insufflation Ventilatory Exchange for Microlaryngeal Surgery. Laryngoscope 2021, 131, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.J.; Yeh, K.C.; Wang, M.L.; Tai, W.H.; Cheng, Y.J. Heated humidified high-flow nasal oxygen prevents intraoperative body temperature decrease in non-intubated thoracoscopy. J Anesth. 2018, 32, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Du Rand, I.A.; Blaikley, J.; Booton, R.; Chaudhuri, N.; Gupta, V.; Khalid, S.; Mandal, S.; Martin, J.; Mills, J.; Navani, N.; et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: Accredited by NICE. Thorax 2013, 68 (Suppl. S1), i1–i44. [Google Scholar] [CrossRef] [PubMed]
- Leone, M.; Einav, S.; Chiumello, D.; Constantin, J.M.; De Robertis, E.; de Abreu, M.G.; Gregoretti, C.; Jaber, S.; Maggiore, S.M.; Pelosi, P.; et al. Noninvasive respiratory support in the hypoxaemic peri-operative/periprocedural patient: A joint ESA/ESICM guideline. Eur. J. Anaesthesiol. 2020, 37, 265–279. [Google Scholar] [CrossRef]
- Golpe, R.; Mateos, A. Supplemental oxygen during flexible bronchoscopy. Chest 2002, 121, 663–664. [Google Scholar] [CrossRef]
- Kim, E.J.; Jung, C.Y.; Kim, K.C. Effectiveness and Safety of High-Flow Nasal Cannula Oxygen Delivery during Bronchoalveolar Lavage in Acute Respiratory Failure Patients. Tuberc. Respir. Dis. 2018, 81, 319–329. [Google Scholar] [CrossRef]
- La Combe, B.; Messika, J.; Labbé, V.; Razazi, K.; Maitre, B.; Sztrymf, B.; Dreyfuss, D.; Fartoukh, M.; Ricard, J.-D. High-flow nasal oxygen for bronchoalveolar lavage in acute respiratory failure patients. Eur. Respir. J. 2016, 47, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Maitre, B.; Jaber, S.; Maggiore, S.M.; Bergot, E.; Richard, J.C.; Bakthiari, H.; Housset, B.; Boussignac, G.; Brochard, L. Continuous positive airway pressure during fiberoptic bronchoscopy in hypoxemic patients. A randomized double-blind study using a new device. Am. J. Respir. Crit. Care Med. 2000, 162 3 Pt 1, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, M.; Conti, G.; Rocco, M.; Arcangeli, A.; Cavaliere, F.; Proietti, R.; Meduri, G.U. Noninvasive positive-pressure ventilation vs. conventional oxygen supplementation in hypoxemic patients undergoing diagnostic bronchoscopy. Chest 2002, 121, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Saksitthichok, B.; Petnak, T.; So-Ngern, A.; Boonsarngsuk, V. A prospective randomized comparative study of high-flow nasal cannula oxygen and non-invasive ventilation in hypoxemic patients undergoing diagnostic flexible bronchoscopy. J. Thorac. Dis. 2019, 11, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- Ben-Menachem, E.; McKenzie, J.; O’Sullivan, C.; Havryk, A.P. High-flow Nasal Oxygen Versus Standard Oxygen During Flexible Bronchoscopy in Lung Transplant Patients: A Randomized Controlled Trial. J. Bronchol. Interv. Pulmonol. 2020, 27, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Irfan, M.; Ahmed, M.; Breen, D. Assessment of High Flow Nasal Cannula Oxygenation in Endobronchial Ultrasound Bronchoscopy: A Randomized Controlled Trial. J. Bronchol. Interv. Pulmonol. 2021, 28, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Abdel Twab, S.M.; Abdo, F.F.; El Derh, M.S. High-flow nasal cannula oxygenation in comparison with apnoeic oxygenation during foreign body removal by rigid bronchoscopy: A randomised controlled trial. Indian J. Anaesth. 2022, 66, 344–349. [Google Scholar] [CrossRef]
- Waddingham, W.; Kamran, U.; Kumar, B.; Trudgill, N.J.; Tsiamoulos, Z.P.; Banks, M. Complications of diagnostic upper Gastrointestinal endoscopy: Common and rare—Recognition, assessment and management. BMJ Open Gastroenterol. 2022, 9, e000688. [Google Scholar] [CrossRef]
- Patel, A.; Nouraei, S.A. Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE): A physiological method of increasing apnoea time in patients with difficult airways. Anaesthesia 2015, 70, 323–329. [Google Scholar] [CrossRef]
- Lin, Y.; Zhang, X.; Li, L.; Wei, M.; Zhao, B.; Wang, X.; Pan, Z.; Tian, J.; Yu, W.; Su, D. High-flow nasal cannula oxygen therapy and hypoxia during gastroscopy with propofol sedation: A randomized multicenter clinical trial. Gastrointest. Endosc. 2019, 90, 591–601. [Google Scholar] [CrossRef]
- Nay, M.-A.; Fromont, L.; Eugene, A.; Marcueyz, J.-L.; Mfam, W.-S.; Baert, O.; Remerand, F.; Ravry, C.; Auvet, A.; Boulain, T. High-flow nasal oxygenation or standard oxygenation for gastrointestinal endoscopy with sedation in patients at risk of hypoxaemia: A multicentre randomised controlled trial (ODEPHI trial). Br. J. Anaesth. 2021, 127, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Doulberis, M.; Sampsonas, F.; Papaefthymiou, A.; Karamouzos, V.; Lagadinou, M.; Karampitsakos, T.; Lagadinou, M.; Karampitsakos, T.; Stratakos, G.; Kuntzen, T.; et al. High-flow versus conventional nasal cannula oxygen supplementation therapy and risk of hypoxia in gastrointestinal endoscopies: A systematic review and meta-analysis. Expert. Rev. Respir. Med. 2022, 16, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Hung, K.-C.; Chang, Y.-J.; Chen, I.-W.; Soong, T.-C.; Ho, C.-N.; Hsing, C.-H.; Chu, C.-C.; Chen, J.-Y.; Sun, C.-K. Efficacy of high flow nasal oxygenation against hypoxemia in sedated patients receiving gastrointestinal endoscopic procedures: A systematic review and meta-analysis. J. Clin. Anesth. 2022, 77, 110651. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.X.; He, X.X.; Chen, Y.P.; Yang, S. The effectiveness of high-flow nasal cannula during sedated digestive endoscopy: A systematic review and meta-analysis. Eur. J. Med. Res. 2022, 27, 30. [Google Scholar] [CrossRef] [PubMed]
- Khanna, P.; Haritha, D.; Das, A.; Sarkar, S.; Roy, A. Utility of high-flow nasal oxygen in comparison to conventional oxygen therapy during upper gastrointestinal endoscopic procedures under sedation: A systematic review and meta-analyses. Indian J. Gastroenterol. 2023, 42, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Ju, T.R.; Lai, P.C.; Lin, H.T.; Huang, Y.T. Should We Use High-Flow Nasal Cannula in Patients Receiving Gastrointestinal Endoscopies? Critical Appraisals through Updated Meta-Analyses with Multiple Methodologies and Depiction of Certainty of Evidence. J. Clin. Med. 2022, 11, 3860. [Google Scholar] [CrossRef] [PubMed]
- Shukla, K.; Parikh, B.; Kumar, A.; Nakra, M. Comparative evaluation of efficacy of oxygenation using high flow nasal cannula vs. conventional nasal cannula during procedural sedation for endoscopic ultrasound: A pilot study. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 648–654. [Google Scholar]
- Kallet, R.H.; Matthay, M.A. Hyperoxic acute lung injury. Respir. Care 2013, 58, 123–141. [Google Scholar] [CrossRef]
- Lee, M.J.; Cha, B.; Park, J.S.; Kim, J.S.; Cho, S.Y.; Han, J.H.; Park, M.H.; Yang, C.; Jeong, S. Impact of High-Flow Nasal Cannula Oxygenation on the Prevention of Hypoxia During Endoscopic Retrograde Cholangiopancreatography in Elderly Patients: A Randomized Clinical Trial. Dig. Dis. Sci. 2022, 67, 4154–4160. [Google Scholar] [CrossRef]
- Ji, J.Y.; Kim, E.H.; Lee, J.H.; Jang, Y.E.; Kim, H.S.; Kwon, S.K. Pediatric airway surgery under spontaneous respiration using high-flow nasal oxygen. Int. J. Pediatr. Otorhinolaryngol. 2020, 134, 110042. [Google Scholar] [CrossRef]
- Fan, Y.; Chi, X.; Zhu, D.; Yin, J.; Liu, Y.; Su, D. Non-intubated deep paralysis: A new anaesthesia strategy for vocal cord polypectomy. Perioper. Med. 2023, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Samad, I.; Phelps, M.; Pandian, V.; Best, S.R.; Akst, L.M.; Jaberi, M.; Stonemetz, J.; Hillel, A. High-flow oxygen, a primary oxygenation technique for endolaryngeal airway surgery: Our experience with 10 patients. Clin. Otolaryngol. 2016, 41, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, I.M.; Lodenius, A.; Tunelli, J.; Ullman, J.; Jonsson Fagerlund, M. Apnoeic oxygenation in adults under general anaesthesia using Transnasal Humidified Rapid-Insufflation Ventilatory Exchange (THRIVE)—A physiological study. Br. J. Anaesth. 2017, 118, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, S.; Rosen, D.; Housden, T.; Taylor, J.; Schibler, A. Nasal high-flow oxygen delivery in children with abnormal airways. Paediatr. Anaesth. 2017, 27, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Syamal, M.N.; Hanisak, J.; Macfarlan, J.; Ortega, B.; Sataloff, R.T.; Benninger, M.S. To Tube, or Not to Tube: Comparing Ventilation Techniques in Microlaryngeal Surgery. Laryngoscope 2021, 131, 2773–2781. [Google Scholar] [CrossRef] [PubMed]
- Riddell, Z.; Pressler, N.; Siau, K.; Mulder, C.J.J.; Shalmani, H.M.; Downs, A.; Gait, A.; Ishaq, S. Feasibility of high-flow nasal oxygen therapy and two-stage sedation during endoscopic hypopharyngeal therapy. JGH Open 2020, 4, 743–748. [Google Scholar] [CrossRef]
- Tsou, K.C.; Hsu, H.H.; Tsai, T.M.; Chen, K.C.; Chen, J.S. Clinical outcome of subcentimeter non-small cell lung cancer after VATS resection: Single institute experience with 424 patients. J. Formos. Med. Assoc. 2020, 119 1 Pt 3, 399–405. [Google Scholar] [CrossRef]
- Liu, H.Y.; Chiang, X.H.; Hung, M.H.; Wang, M.L.; Lin, M.W.; Cheng, Y.J.; Hsu, H.H.; Chen, J.S. Nonintubated uniportal thoracoscopic segmentectomy for lung cancer. J. Formos. Med. Assoc. 2020, 119, 1396–1404. [Google Scholar] [CrossRef]
- Shih, C.C.; Liang, P.C.; Chuang, Y.H.; Huang, Y.J.; Lin, P.J.; Wu, C.Y. Effects of high-flow nasal oxygen during prolonged deep sedation on postprocedural atelectasis: A randomised controlled trial. Eur. J. Anaesthesiol. 2020, 37, 1025–1031. [Google Scholar] [CrossRef]

{kind=link}
| References Author, Year | Study Design/Sample Size | Population and Type of Intervention | Sedation Methods | Respiratory Support Type | Main Results Summary |
|---|---|---|---|---|---|
| Arias-Sanchez, 2023 [12] | SC 40 | Adult patients in acute care with a presumptive diagnosis of pneumonia receiving oxygen and undergoing FOB | Dexmedetomidine, Hydrochloride, Topical Anesthesia (Lidocaine 2%) | HFNC: Flow 60 lpm, Tª 35 °C, and FiO2 40% vs. COT: FiO2 40% through a nasal cannula | HFNC vs. COT has a smaller decrease in SpO2 levels during the procedure (94% vs. 90%; p = 0.40); and less variation between SpO2 before FOB and the lowest SpO2 during FOB: 2% vs. 4.5%; p = 0.01. |
| Zhang, 2022 [13] | RCT 176 | Adults at risk of hypoxemia with a STOP-BANG score ≥ 3 during FOB under deep sedation | Propofol, Opioids | HFNC: Flow 60 lpm and FiO2 100% vs. COT: Flow 6 lpm through a tight-fitting facemask | HFNC vs. COT reduces the incidence of oxygen desaturation (4.6% vs. 29.2%; p < 0.001) and the airway intervention (5.7% vs. 48.3%; p < 0.001). |
| Longhini, 2022 [14] | RCT 36 | Adult outpatients undergoing FOB with BAL | Topical anaesthesia | HFNC: Flow 60 lpm, Tª 31 °C, and FiO2 21% if SpO2 > 95% or set to reach SpO2 > 95% vs. COT to maintain SpO2 > 94%. | HFNC improves gas exchange (56% of desaturation with COT vs. 11% with HFNC; p < 0.001), avoids loss of end-expiratory lung volume, and prevents an increase in diaphragm activation. |
| Simon, 2014 [15] | RCT 40 | Critically ill patients with acute hypoxaemic respiratory failure undergoing FOB | Propofol, Topical anaesthesia (lidocaine 0.8%) | HFNC: Flow 50 lpm vs. NIV: PEEP 3–10 cm H2O and IPAP 15–20 cm H2O. Full face mask. | NIV was superior to HFNC regarding oxygenation before, during, and after FOB in patients with moderate to severe hypoxaemia |
| Douglas, 2018 [16] | RCT 60 | Adults undergoing EBUS with conscious sedation | Propofol, Midazolam, Opioids, Topical 2% lidocaine | HFNC: Flow 30–70 lpm and FiO2 100% vs. COT at 10–15 lpm via a bite block | Higher SpO2 after pre-oxygenation and during the procedure with HFNC vs. COT (100% vs. 98% and 97.5 vs. 92%, respectively; p < 0.001). |
| Mazzeffi, 2021 [17] | RCT 262 | Adults with moderate to high risk for hypoxemia during advanced EGD | Propofol, Fentanyl or Midazolam | HFNC: Flow at 20 lpm vs. COT at 6 lpm | HFNC is associated with fewer desaturation episodes and hypoxia. There is no difference in the incidence of hypercarbia. Post-hoc analyses showed that patients with COPD who received HFNC had a significantly higher incidence of hypercarbia without differences in hypoxemia. |
| Thiruvenkatarajan, 2021 [18] | RTC 132 | Adults with moderate to high risk for hypoxemia: BMI > 30 or OSA or ASA classification of III–IV undergoing ERCP. | Propofol, Fentanyl | HFNC: Flow 30–60 lpm and FiO2 100% vs. COT through nasal cannula at 4 lpm + 4 lpm through mouthguard. | HFNC vs. COT did not significantly decrease hypoxemia, hypercarbia, the need for airway interventions, the requirement of a chin lift/jaw thrust, nasopharyngeal airway insertion, bag-mask ventilation, or OTI. |
| Zhang, 2022 [19] | RCT 369 | Elderly patients; ASA classification of I–II; and BMI < 30 kg/m2 undergoing gastroscopy | Propofol | HFNC: Flow 30 lpm and FiO2 at 50% (H50) or 100% (H100) vs. COT at 8 lpm | The incidence of hypoxia was lower in both the H50 and H100 groups than in the COT group. No significant differences were seen in the incidence of hypoxia between the H50 and H100 groups. |
| Sawase, 2023 [20] | RCT 75 | Adult patients (20–82 years) undergoing ERCP | Midazolam, Pethidine, hydrochloride | HFNC: Flow 40–60 lpm and FiO2 21% vs. COT at 1–2 lpm. | HFNC with room air vs. COT did not reduce marked hypercapnia during ERCP under sedation. There was no significant difference in the occurrence of hypoxemia between the HFNC group and the COT group. |
| Kim, 2021 [21] | RCT 72 | Adults with moderate to high risk for hypoxemia are undergoing ERCP in the prone position. | Propofol, Fentanyl | HFNC: Flow 50 lpm and FiO2 100% vs. COT at 5 lpm | HFNC provided a better nadir SpO2 level under sedation and less procedural interruption. |
| Lin, 2023 [22] | SC 294 | Adults undergoing anatomical resections, lymph node biopsy, and staging through uniportal VATS | Fentanyl, Propofol, Desflurane or Sevoflurane are inhaled | Airway management was performed with i-gel (Intersurgical Ltd.) or HFNC Optiflow (Fisher & Paykel). | HFNC had a significantly higher desaturation event rate, lower nadir SpO2, and longer hospitalisation compared to the i-gel group. However, propensity score matching analysis revealed no significant between-group difference in the desaturation rate. |
| Flach, 2019 [23] | SC 21 | Transoral laser microsurgery for subglottic stenosis, cordectomy, excision of a laryngeal papilloma, or vocal cord lesion. | Propofol, Remifentanil | HFNC: Flow 70 lpm and FiO2 100%. | No intra- or immediate post-operative complications were recorded, and adequate surgical access was achieved. No airway fires or similar adverse events, such as flaring, were mentioned. |
| Ke, 2020 [24] | SC 160 | Adults undergoing resection VATS | Propofol, Fentanyl, Midazolam. | HFNC: Flow 50 lpm and FiO2 100 vs. OTI (double-lumen endotracheal tube). | OTI had a significantly longer mean induction and operative time, suffered greater intraoperative blood loss, had longer postoperative hospital stays, and had an increased chest tube retention time vs. HFNC. |
| Benninger, 2021 [25] | SC 53 | Patients with subglottic stenosis, vocal cord lesions, and vocal cord paralysis through microlaryngoscopy. | Propofol, Remifentanil | THRIVE: Flow 70 lpm and FiO2 100%. | The median apnea time was 16 min, the median end tidal CO2 was 50 mmHg, and the median minimum SpO2 was 95%. Six cases required supplementation of THRIVE with OTI for sustained oxygen desaturation. |
| Lai, 2018 [26] | SC 256 | VATS for lung biopsy, wedge resection, segmentectomy, lobectomy, mediastinal tumour excision, and bullectomy. | Propofol to achieve BIS level 40–60. | THRIVE: Flow 20 lpm and FiO2 indicated before anaesthesia vs. COT through conventional O2 mask | Postoperative temperatures were significantly higher in patients using THRIVE vs. COT. Significantly less intraoperative temperature decrease was shown in the THRIVE group. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corral-Blanco, M.; Sayas-Catalán, J.; Hernández-Voth, A.; Rey-Terrón, L.; Villena-Garrido, V. High-Flow Nasal Cannula Therapy as an Adjuvant Therapy for Respiratory Support during Endoscopic Techniques: A Narrative Review. J. Clin. Med. 2024, 13, 81. https://doi.org/10.3390/jcm13010081
Corral-Blanco M, Sayas-Catalán J, Hernández-Voth A, Rey-Terrón L, Villena-Garrido V. High-Flow Nasal Cannula Therapy as an Adjuvant Therapy for Respiratory Support during Endoscopic Techniques: A Narrative Review. Journal of Clinical Medicine. 2024; 13(1):81. https://doi.org/10.3390/jcm13010081
Chicago/Turabian StyleCorral-Blanco, Marta, Javier Sayas-Catalán, Ana Hernández-Voth, Laura Rey-Terrón, and Victoria Villena-Garrido. 2024. "High-Flow Nasal Cannula Therapy as an Adjuvant Therapy for Respiratory Support during Endoscopic Techniques: A Narrative Review" Journal of Clinical Medicine 13, no. 1: 81. https://doi.org/10.3390/jcm13010081
APA StyleCorral-Blanco, M., Sayas-Catalán, J., Hernández-Voth, A., Rey-Terrón, L., & Villena-Garrido, V. (2024). High-Flow Nasal Cannula Therapy as an Adjuvant Therapy for Respiratory Support during Endoscopic Techniques: A Narrative Review. Journal of Clinical Medicine, 13(1), 81. https://doi.org/10.3390/jcm13010081