

Building Bridges between People with Stroke, Families, and Health Professionals: Development of a Blended Care Program for Self-Management

 ,
,  , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
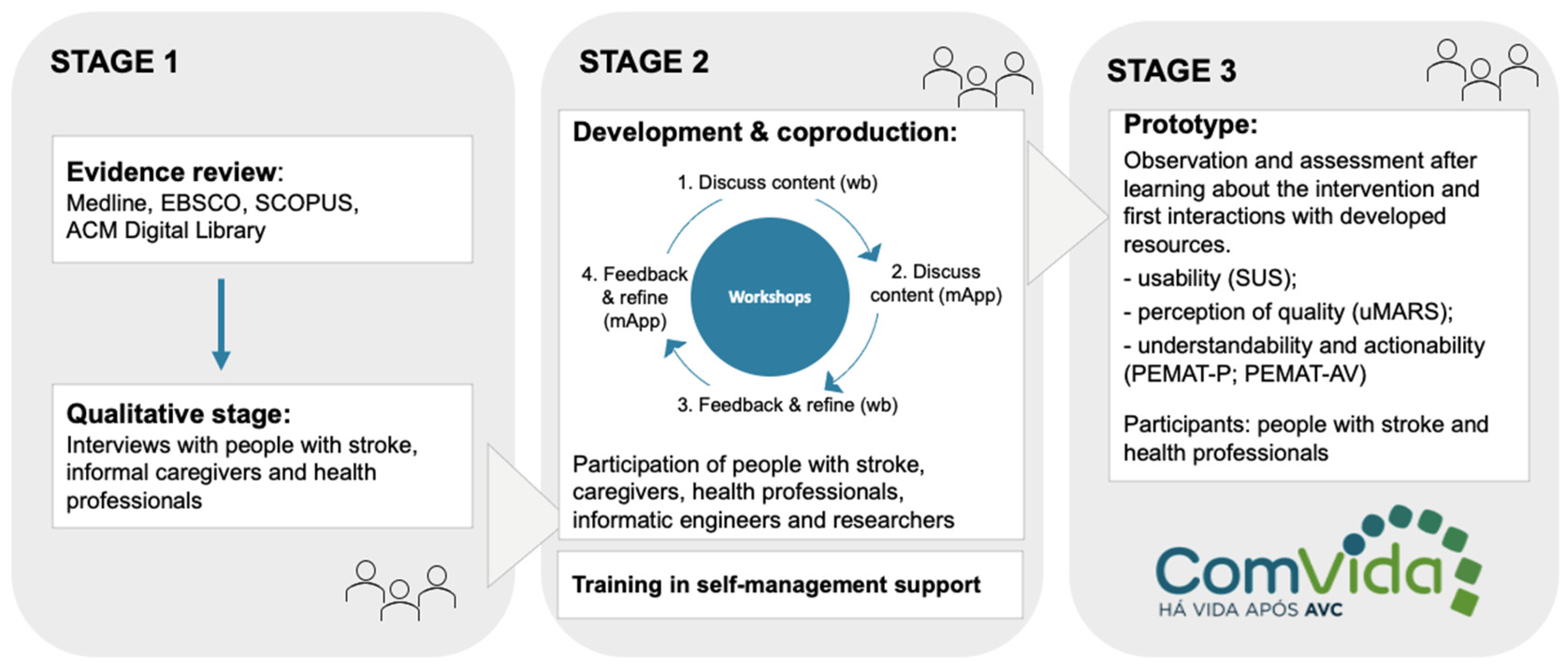
2.1. Study Design, Setting, and Participants
2.1.1. Stage 1: Evidence Review and Qualitative Study
2.1.2. Stage 2: Co-Production
2.1.3. Stage 3: Prototyping
2.2. Ethical Considerations
2.3. Data Analysis
3. Results
3.1. Stage 1
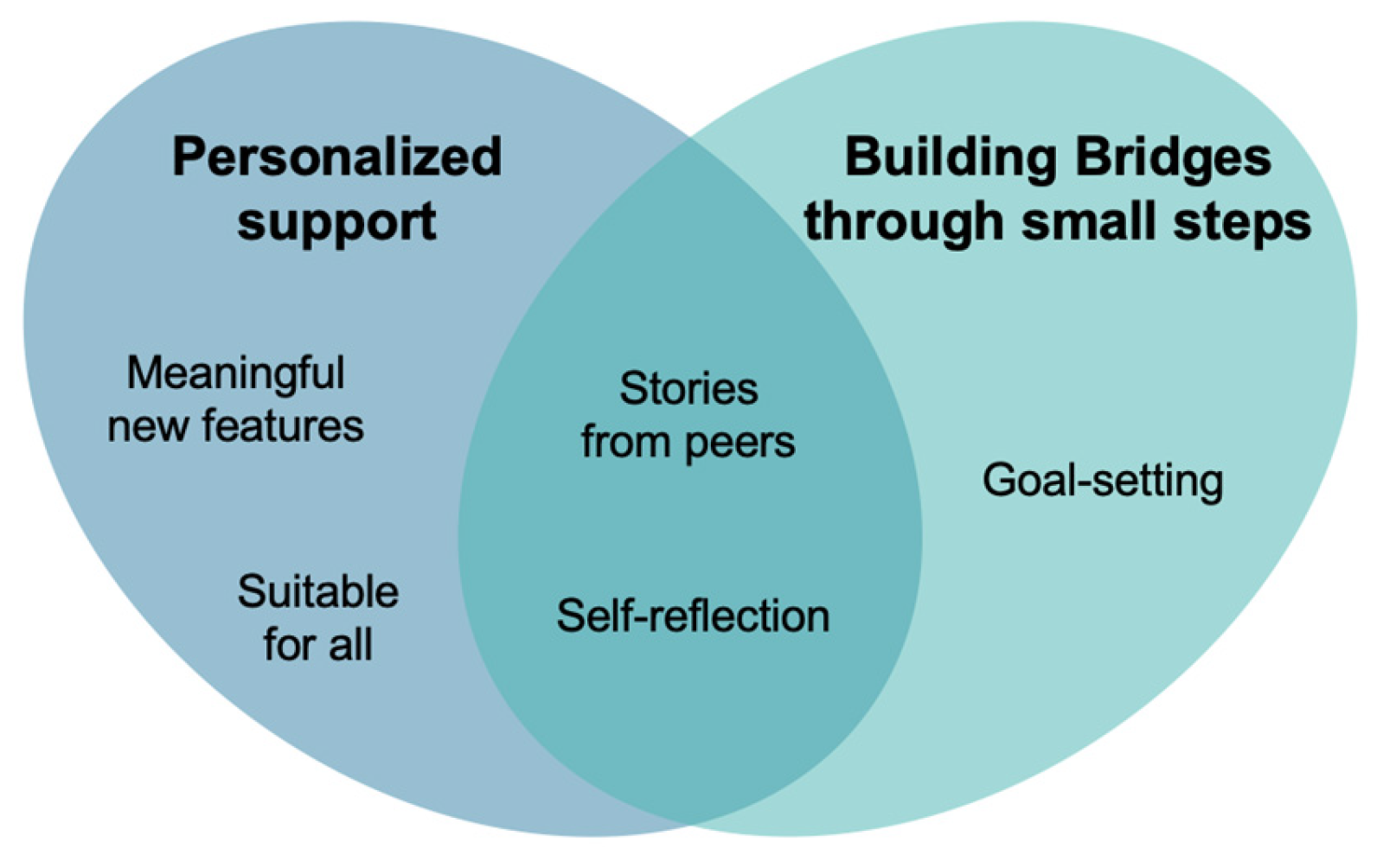
3.1.1. Thematic Analysis
Personalized Support
- Stories from Peers
“Look: “she also felt this like me, or I felt this too. After all, it’s normal”. We feel a little more normal, not so extra-terrestrial. It’s true, that helps.”(PwS#05)
“I spoke to a lot of people who had the same, and I asked them for advice, how they felt afterwards. That helped me a lot”(PwS#14)
“It would be a helpful tool [referring to the workbook] both for the person who had the stroke and for the family members who deal more directly with the situation”(C#11)
“I think that having stories from some people who have already gone through the same situation can be a good incentive to help them with their own rehabilitation.”(HP#13, Physiotherapist)
“People with stroke [from the workbook] do not look sick, which is good. However, it may also be important for people to realize that it is common to stay seriously weakened. This may help them to identify themselves with the stories presented”(HP#03, Physiotherapist)
“Other examples, including activities culturally adapted to our Portuguese contexts, such as going to the cafe, going to the supermarket, going for a walk with the dog, will contribute to a better adaptation of the workbook to our culture.”(HP#01, Physiotherapist)
- Meaningful New Features
“Older people forget the medication a lot and mix them all the time. I remember that my grandmother used to mix all the medications. Maybe it was quite useful something to manage the medication.”(PwS#01)
“So, if there was an option to do medication management in the app, I think it was important. One more agenda: the user’s agenda for the physiotherapy sessions, to remind exercises to do at home, or a space in the app where the therapist or health professional could put some specific tips.”(HP#04, Physiotherapist)
“For example, it was important to have a page with facts. Or… is not really a chat, but where people could ask questions, and someone could answer. I think that is also important.”(C#04)
“The disadvantage about the digital solutions, here in Portugal, is that some people do not know how to use technology. These kinds of technologies would be very useful for people, but some don’t know nothing about it. That was visible during the pandemic.”(PwS#06)
- Suitable for All
“New technologies are a useful tool, but it really depends on some personal factors. For very old people, who live in rural areas, who do not have access to technology, of course they will not make sense.”(HP#14, Social Worker)
“Would be useful having a blank page [referring to the workbook]. Let’s imagine this: there are contacts that may be specific to the region where the patient is hospitalized (…). In addition to national contacts, we could add some local contacts that may be useful.”(HP#10, Nurse)
“I think this workbook is very, very, very important for post-discharge. Going home is a dramatic shock.”(PwS#05)
“Really, the only thing I thought it would be important was that when he left [the hospital] he had some support. Because we had still almost two months at home without me having any support.”(C#09)
“It can’t happen a patient leaving the hospital and the family do not knowing how to dress that patient or how to lift the patient, or if the patient doesn’t get up, how to mobilize him.”(HP#14, Social Worker)
“There are several health professionals giving information at the same time, and families can’t understand all… it is the therapist, the social worker, the doctor, the nurse”(HP#17, Nurse)
Building Bridges through Small Steps
- Goal Setting
“The thing I found most interesting in the manual was that part where the person defines goals, I don’t say SMART goals, but almost creating SMART goals for themselves. See goals, let’s define after how long we are waiting for… (…) I think it could be interesting”(HP#02, Physiotherapist)
“I had a patient who had a stroke and came back from vacation showing me a video and saying: “see, I can swim, I can swim in the sea and in the pool.” And he showed me all the videos, so happy. That was our goal since the beginning.”(HP#01, Physiotherapist)
“She [the patient] was always seeing the glass as half empty, and I sometimes tried to help her see the glass as half full: “You were lying down, you wouldn’t get up, you can already lean against the back of the bed and you can sit up in bed for 5 min without feeling dizzy, without falling backwards”. It was a very progressive and exhaustive process (…). She put a lot of pressure on herself, on the goals she wanted to achieve, and that affected her psychologically”(C#05)
“If people do things just because, they will end demotivated. My mom was always saying: “I can’t, I can’t” [about communicating through writing]. I gave her a pen and a paper and I asked her to add carrots to the supermarket list. At first, she couldn’t, but at the second time she was already writing it. I think that the steps to achieve goals will depend on the person, on what is important for her.”(C#07)
“For example, for driving, I set small goals. First, I decided that my goal was to drive to the physiotherapy, which is two minutes distance. I did this for three weeks (…) then, I defined several levels to follow: I increased the distance, going to a commercial surface, then going to Setúbal and I started to broaden my horizons.”(PwS#05)
“It ends up being a motivation to set recovery goals. At this level, perhaps it may be a tool to stop people from giving up, based on the testimonies, some similar and others not so much.”(C#06)
- Self-Reflection
“It gives us a way to encourage the use of strategies for their recovery, to explore reflection or personal reflection.”(HP#01, Physiotherapist)
“Many of them do not have this ability of looking back and reflecting on their recovery. They say: oh, everything is wrong” (…). So, if we go back and look at the records, maybe if I go get to one of these old records and say: -Look here and look now. Can you see the difference? It is palpable.”(HP#06, Occupational therapist)
“I think it may be very interesting and of huge value to invite people to evaluate their own progress. This will help them to set goals and be proactive”(C#11)
“Thinking about what I’m feeling and what I want to do it is not easy. It is an intimate moment, being at home writing… I am fully aware that I speak openly about what I feel, which helps me. I do not have that fear, but it’s not easy for everyone.”(PwS#05)
3.2. Stage 2
3.3. Stage 3
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, E.; Wilson, L.; Wickramasinghe, K.; Bhatnagar, P.; Leal, J.; Luengo-Fernandez, R.; Burns, R.; Rayner, M.; Townsend, N. European Cardiovascular Disease Statistics 2017; European Heart Network Brussels: Brusells, Belgium, 2017. [Google Scholar]
- Chen, T.; Zhang, B.; Deng, Y.; Fan, J.C.; Zhang, L.; Song, F. Long-Term Unmet Needs after Stroke: Systematic Review of Evidence from Survey Studies. BMJ Open 2019, 9, e028137. [Google Scholar] [CrossRef] [PubMed]
- Della Vecchia, C.; Viprey, M.; Haesebaert, J.; Termoz, A.; Giroudon, C.; Dima, A.; Rode, G.; Préau, M.; Schott, A.M. Contextual Determinants of Participation after Stroke: A Systematic Review of Quantitative and Qualitative Studies. Disabil. Rehabil. 2021, 43, 1786–1798. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Xiao, L.D.; Chamberlain, D.; Newman, P. Enablers and Barriers in Hospital-to-Home Transitional Care for Stroke Survivors and Caregivers: A Systematic Review. J. Clin. Nurs. 2021, 30, 2786–2807. [Google Scholar] [CrossRef] [PubMed]
- Lou, S.; Carstensen, K.; Jørgensen, C.R.; Nielsen, C.P. Stroke Patients’ and Informal Carers’ Experiences with Life after Stroke: An Overview of Qualitative Systematic Reviews. Disabil. Rehabil. 2017, 39, 301–313. [Google Scholar] [CrossRef]
- Langhorne, P.; Baylan, S. Early Supported Discharge Services for People with Acute Stroke. Cochrane Database Syst. Rev. 2017, 7, CD000433. [Google Scholar] [CrossRef]
- Connor, E.O.; Dolan, E.; Horgan, F.; Galvin, R.; Robinson, K. A Qualitative Evidence Synthesis Exploring People after Stroke, Family Members, Carers and Healthcare Professionals’ Experiences of Early Supported Discharge (ESD) after Stroke. PLoS ONE 2023, 18, e0281583. [Google Scholar] [CrossRef]
- Pindus, D.M.; Mullis, R.; Lim, L.; Wellwood, I.; Rundell, A.V.; Aziz, N.A.A.; Mant, J. Stroke Survivors’ and Informal Caregivers’ Experiences of Primary Care and Community Healthcare Services—A Systematic Review and Meta-Ethnography. PLoS ONE 2018, 13, e0192533. [Google Scholar] [CrossRef]
- Fryer, C.E.; Luker, J.A.; McDonnell, M.N.; Hillier, S.L. Self Management Programmes for Quality of Life in People with Stroke. Cochrane Database Syst. Rev. 2016, 2016, CD010442. [Google Scholar] [CrossRef]
- Norrving, B.; Barrick, J.; Davalos, A.; Dichgans, M.; Cordonnier, C.; Guekht, A.; Kutluk, K.; Mikulik, R.; Wardlaw, J.; Richard, E.; et al. Action Plan for Stroke in Europe 2018–2030. Eur. Stroke J. 2018, 3, 309–336. [Google Scholar] [CrossRef]
- Pereira, C.M.; Greenwood, N.; Jones, F. From Recovery to Regaining Control of Life—The Perspectives of People with Stroke, Their Carers and Health Professionals. Disabil. Rehabil. 2021, 43, 2897–2908. [Google Scholar] [CrossRef]
- Pereira, C.M.; Greenwood, N.; Jones, F. “A Proof of Life” through Transition from Hospital to Home after a Stroke in a Portuguese Setting—A Multi-Perspective, Longitudinal Qualitative Study. Int. J. Qual. Stud. Health Well-Being 2023, 18, 2238986. [Google Scholar] [CrossRef] [PubMed]
- WHO. Health System Review- Portugal. Phase I Final Report; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- DGS. Manual de Boas Práticas Literacia Em Saúde: Capacitação Dos Profissionais de Saúde [Manual of Good Practices Health Literacy: Training of Health Professionals]; Direçao-Geral da Saúde: Lisboa, Portugal, 2019; ISBN 9789726752882. (In Portuguese) [Google Scholar]
- NICE. National Clinical Guidelines for Stroke- for the United Kingdom and Ireland; King’s College London: London, UK, 2023. [Google Scholar]
- Winstein, C.J.; Stein, J.; Arena, R.; Bates, B.; Cherney, L.R.; Cramer, S.C.; Deruyter, F.; Eng, J.J.; Fisher, B.; Harvey, R.L.; et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2016, 47, e98–e169. [Google Scholar] [CrossRef] [PubMed]
- Mountain, A.; Patrice Lindsay, M.; Teasell, R.; Salbach, N.M.; de Jong, A.; Foley, N.; Bhogal, S.; Bains, N.; Bowes, R.; Cheung, D.; et al. Canadian Stroke Best Practice Recommendations: Rehabilitation, Recovery, and Community Participation Following Stroke. Part Two: Transitions and Community Participation Following Stroke. Int. J. Stroke 2020, 15, 789–806. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Owolabi, M.O.; Feigin, V.L.; Abd-Allah, F.; Akinyemi, R.O.; Bhattacharjee, N.V.; Brainin, M.; Cao, J.; Caso, V.; Dalton, B.; et al. Pragmatic Solutions to Reduce the Global Burden of Stroke: A World Stroke Organization–Lancet Neurology Commission. Lancet Neurol. 2023, 22, 1160–1206. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Holman, H.R.; Med, A.B. Self-Management Education: History, Definition, Outcomes, and Mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Warner, G.; Packer, T.; Villeneuve, M.; Audulv, A.; Versnel, J. A Systematic Review of the Effectiveness of Stroke Self-Management Programs for Improving Function and Participation Outcomes: Self-Management Programs for Stroke Survivors. Disabil. Rehabil. 2015, 37, 2141–2163. [Google Scholar] [CrossRef]
- Parke, H.L.; Epiphaniou, E.; Pearce, G.; Taylor, S.J.C.; Sheikh, A.; Griffiths, C.J.; Greenhalgh, T.; Pinnock, H. Self-Management Support Interventions for Stroke Survivors: A Systematic Meta-Review. PLoS ONE 2015, 10, e0131448. [Google Scholar] [CrossRef]
- Moore, G.; Campbell, M.; Copeland, L.; Craig, P.; Movsisyan, A.; Hoddinott, P.; Littlecott, H.; O’Cathain, A.; Pfadenhauer, L.; Rehfuess, E.; et al. Adapting Interventions to New Contexts-the ADAPT Guidance. BMJ 2021, 374, n1679. [Google Scholar] [CrossRef]
- Klockar, E.; Kylén, M.; Gustavsson, C.; Finch, T.; Jones, F.; Elf, M. Self-Management from the Perspective of People with Stroke—An Interview Study. Patient Educ. Couns. 2023, 112, 107740. [Google Scholar] [CrossRef]
- Morton, K.; Dennison, L.; May, C.; Murray, E.; Little, P.; McManus, R.J.; Yardley, L. Using Digital Interventions for Self-Management of Chronic Physical Health Conditions: A Meta-Ethnography Review of Published Studies. Patient Educ. Couns. 2017, 100, 616–635. [Google Scholar] [CrossRef] [PubMed]
- Tighe, S.A.; Ball, K.; Kensing, F.; Kayser, L.; Rawstorn, J.C.; Maddison, R. Toward a Digital Platform for the Self-Management of Noncommunicable Disease: Systematic Review of Platform-Like Interventions. J. Med. Internet Res. 2020, 22, e16774. [Google Scholar] [CrossRef] [PubMed]
- Lavin, N.; Hellawell, M.; O’Brien, C. E-Health for Stroke Survivors and Their Carers. Br. J. Healthc. Manag. 2017, 23, 462–466. [Google Scholar] [CrossRef]
- Lau, S.C.L.; Bhattacharjya, S.; Fong, M.W.M.; Nicol, G.E.; Lenze, E.J.; Baum, C.; Hardi, A.; Wong, A.W.K. Effectiveness of Theory-Based Digital Self-Management Interventions for Improving Depression, Anxiety, Fatigue and Self-Efficacy in People with Neurological Disorders: A Systematic Review and Meta-Analysis. J. Telemed. Telecare 2020, 28, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Kamoen, O.; Maqueda, V.; Yperzeele, L.; Pottel, H.; Cras, P.; Vanhooren, G.; Vanacker, P. Stroke Coach: A Pilot Study of a Personal Digital Coaching Program for Patients after Ischemic Stroke. Acta Neurol. Belg. 2020, 120, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Feng, W.; Chhatbar, P.Y.; Liu, Y.; Ji, X.; Ovbiagele, B. Mobile Health as a Viable Strategy to Enhance Stroke Risk Factor Control: A Systematic Review and Meta-Analysis. J. Neurol. Sci. 2017, 378, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Cadilhac, D.A.; Busingye, D.; Li, J.C.; Andrew, N.E.; Kilkenny, M.F.; Thrift, A.G.; Thijs, V.; Hackett, M.L.; Kneebone, I.; Lannin, N.A.; et al. Development of an Electronic Health Message System to Support Recovery after Stroke: Inspiring Virtual Enabled Resources Following Vascular Events (IVERVE). Patient Prefer. Adherence 2018, 12, 1213–1224. [Google Scholar] [CrossRef]
- Hwang, N.-K.; Ji-Su, P.; Chang, M.-Y. Tele-Health Interventions to Support Self-Management in Stroke Survivers: A Systematic Review. Healthcare 2020, 9, 472. [Google Scholar] [CrossRef]
- Wong, A.W.K.; Fong, M.W.M.; Munsell, E.G.S.; Metts, C.L.; Lee, S.I.; Nicol, G.E.; DePaul, O.; Tomazin, S.E.; Kaufman, K.J.; Mohr, D.C. Using Intervention Mapping and Behavior Change Techniques to Develop a Digital Intervention for Self-Management in Stroke: Development Study. JMIR Hum. Factors 2023, 10, e45099. [Google Scholar] [CrossRef]
- Purvis, T.; Busingye, D.; Andrew, N.E.; Kilkenny, M.F.; Thrift, A.G.; Li, J.C.; Cameron, J.; Thijs, V.; Hackett, M.L.; Kneebone, I.; et al. Mixed Methods Evaluation to Explore Participant Experiences of a Pilot Randomized Trial to Facilitate Self-Management of People Living with Stroke: Inspiring Virtual Enabled Resources Following Vascular Events (IVERVE). Health Expect. 2022, 25, 2570–2581. [Google Scholar] [CrossRef]
- Cameron, J.; Lannin, N.A.; Harris, D.; Andrew, N.E.; Kilkenny, M.F.; Purvis, T.; Thrift, A.G.; Thayabaranathan, T.; Ellery, F.; Sookram, G.; et al. A Mixed-Methods Feasibility Study of a New Digital Health Support Package for People after Stroke: The Recovery-Focused Community Support to Avoid Readmissions and Improve Participation after Stroke (ReCAPS) Intervention. Pilot Feasibility Stud. 2022, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Creswell, D.J. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2018; ISBN 2013206534. [Google Scholar]
- Hawkins, J.; Madden, K.; Fletcher, A.; Midgley, L.; Grant, A.; Cox, G.; Moore, L.; Campbell, R.; Murphy, S.; Bonell, C.; et al. Development of a Framework for the Co-Production and Prototyping of Public Health Interventions. BMC Public Health 2017, 17, 689. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; et al. Improving the Content Validity of the Mixed Methods Appraisal Tool: A Modified e-Delphi Study. J. Clin. Epidemiol. 2019, 111, 49–59.e1. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Morrison, L.; Bradbury, K.; Muller, I. The Person-Based Approach to Intervention Development: Application to Digital Health-Related Behavior Change Interventions. J. Med. Internet Res. 2015, 17, e30. [Google Scholar] [CrossRef] [PubMed]
- Morrison, L.; Muller, I.; Yardley, L.; Bradbury, K. The Person-Based Approach to Planning, Optimising, Evaluating and Implementing Behavioural Health Interventions. Eur. Health Psychol. 2018, 20, 464–469. [Google Scholar]
- Mummah, S.A.; Robinson, T.N.; King, A.C.; Gardner, C.D.; Sutton, S. IDEAS (Integrate, Design, Assess, and Share): A Framework and Toolkit of Strategies for the Development of More Effective Digital Interventions to Change Health Behavior. J. Med. Internet Res. 2016, 18, e317. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.C.L.; Judycki, S.; Mix, M.; DePaul, O.; Tomazin, R.; Hardi, A.; Wong, A.W.K.; Baum, C. Theory-Based Self-Management Interventions for Community-Dwelling Stroke Survivors: A Systematic Review and Meta-Analysis. Am. J. Occup. Ther. 2022, 76, 7604205010. [Google Scholar] [CrossRef]
- Denzin, N.; Lincoln, Y. The SAGE Handbook of Qualitative Research, 5th ed.; Denzin, N., Lincoln, Y., Eds.; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2018; Volume 195, ISBN 9781483349800. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. One Size Fits All? What Counts as Quality Practice in (Reflexive) Thematic Analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: Toward a Unifying Theory of Behavioral Change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Brito, M. Avaliar Materiais de Comunicação Em Saúde Melhora Literacia Em Saúde: Tradução e Adaptação Transcultural Do Instrumento PEMAT Para Portugal. J. Investig. Médica 2021, 2, 005–024. [Google Scholar] [CrossRef]
- Shoemaker, S.J.; Wolf, M.; Brach, C. Developement of the Patient Education Material Assessment Tool (PEMAT). Patient Educ. Couns. 2014, 96, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.I.; Rosa, A.F.; Queirós, A.; Silva, A.; Rocha, N.P. European Portuguese Validation of the System Usability Scale (SUS). Procedia Comput. Sci. 2015, 67, 293–300. [Google Scholar] [CrossRef]
- Lewis, J.R. The System Usability Scale: Past, Present, and Future. Int. J. Hum. Comput. Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Gralha, S.R.; da Silva Bittencourt, O.N. Portuguese Translation and Validation of the User Rating Scale for Mobile Applications in the Health Area (UMARS). Res. Soc. Dev. 2023, 12, e8912642056. [Google Scholar] [CrossRef]
- Stoyanov, S.R.; Hides, L.; Kavanagh, D.J.; Wilson, H. Development and Validation of the User Version of the Mobile Application Rating Scale (UMARS). JMIR mHealth uHealth 2016, 4, e72. [Google Scholar] [CrossRef]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Clark, E.; MacCrosain, A.; Ward, N.S.; Jones, F. The Key Features and Role of Peer Support within Group Self-Management Interventions for Stroke? A Systematic Review. Disabil. Rehabil. 2018, 42, 307–316. [Google Scholar] [CrossRef]
- Jones, F.; Gage, H.; Drummond, A.; Bhalla, A.; Grant, R.; Lennon, S.; McKevitt, C.; Riazi, A.; Liston, M. Feasibility Study of an Integrated Stroke Self-Management Programme: A Cluster-Randomised Controlled Trial. BMJ Open 2016, 6, e008900. [Google Scholar] [CrossRef]
- McKenna, S.; Jones, F.; Glenfield, P.; Lennon, S. Bridges Self-Management Program for People with Stroke in the Community: A Feasibility Randomized Controlled Trial. Int. J. Stroke 2015, 10, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Kulnik, S.T.; Pöstges, H.; Townsend, R.; Micklethwaite, P.; Jones, F. A Gift from Experience: Co-Production and Co-Design in Stroke and Self-Management. Des. Health 2019, 3, 98–118. [Google Scholar] [CrossRef]
- Hale, L.; Jones, F.; Mulligan, H.; Levack, W.; Smith, C.; Claydon, L.; Milosavljevic, S.; Taylor, D.; Allan, J.; MacKenzie, N.; et al. Developing the Bridges Self-Management Programme for New Zealand Stroke Survivors: A Case Study. Int. J. Ther. Rehabil. 2014, 21, 381–388. [Google Scholar] [CrossRef]
- Hale, L.; McCulloch, M.; De Ruiter, S.; Wihongia, E.; Norlinga, E.M.; Gorczynski, D.; Linney, M.; Kennedy, P.; Jones, F. Implementing and Evaluating the Bridges Stroke Self-Management Programme into a New Zealand District Health Board Stroke Service: A Case Study. New Zeal. J. Physiother. 2021, 49, 58–69. [Google Scholar] [CrossRef]
- Singer, B.; Jones, F.; Lennon, S.; Singer, B. Adapting the Bridges Stroke Self-Management Programme for Use in Australia. Int. J. Ther. Rehabil. 2018, 25, 414–423. [Google Scholar] [CrossRef]
- Flutter. Available online: https://flutter.dev/ (accessed on 15 September 2023).
- Node.Js. Available online: https://nodejs.org/ (accessed on 29 September 2023).
- MongoDB. Available online: https://www.mongodb.com/ (accessed on 10 September 2023).
- Duncan Millar, J.; Mason, H.; Kidd, L. What Is Important in Supporting Self-Management in Community Stroke Rehabilitation? A Q Methodology Study. Disabil. Rehabil. 2023, 45, 2307–2315. [Google Scholar] [CrossRef]
- Pearce, G.; Pinnock, H.; Epiphaniou, E.; Parke, H.L.; Heavey, E.; Griffiths, C.J.; Greenhalgh, T.; Sheikh, A.; Taylor, S.J.C. Experiences of Self-Management Support Following a Stroke: A Meta-Review of Qualitative Systematic Reviews. PLoS ONE 2015, 10, e0141803. [Google Scholar] [CrossRef]
- Dekker, J.; de Groot, V.; ter Steeg, A.M.; Vloothuis, J.; Holla, J.; Collette, E.; Satink, T.; Post, L.; Doodeman, S.; Littooij, E. Setting Meaningful Goals in Rehabilitation: Rationale and Practical Tool. Clin. Rehabil. 2020, 34, 3–12. [Google Scholar] [CrossRef]
- Perski, O.; Short, C.E. Acceptability of Digital Health Interventions: Embracing the Complexity. Transl. Behav. Med. 2021, 11, 1473–1480. [Google Scholar] [CrossRef]
- Ozkaynak, M.; Sircar, C.M.; Frye, O.; Valdez, R.S. A Systematic Review of Design Workshops for Health Information Technologies. Informatics 2021, 8, 34. [Google Scholar] [CrossRef]
- Neves, R. A Avaliação de Uma Aplicação Móvel de Saúde Sob o Ponto de Vista Do Utilizador: O Caso Da App MySNS Carteira; Universidade Beira Interior: Covilhã, Portugal, 2021. [Google Scholar]
- Lambrecht, A.; Vuillerme, N.; Raab, C.; Simon, D.; Messner, E.M.; Hagen, M.; Bayat, S.; Kleyer, A.; Aubourg, T.; Schett, G.; et al. Quality of a Supporting Mobile App for Rheumatic Patients: Patient-Based Assessment Using the User Version of the Mobile Application Scale (UMARS). Front. Med. 2021, 8, 715345. [Google Scholar] [CrossRef] [PubMed]
- Agher, D.; Sedki, K.; Despres, S.; Albinet, J.P.; Jaulent, M.C.; Tsopra, R. Encouraging Behavior Changes and Preventing Cardiovascular Diseases Using the Prevent Connect Mobile Health App: Conception and Evaluation of App Quality. J. Med. Internet Res. 2022, 24, e25384. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population | Outcome | Results |
|---|---|---|
| People with Stroke (n = 17) | Gender (male) | 11 |
| Age (years: Mean ± SD; Min–Max) | 60.2 ± 2; 34–80 | |
| Time after stroke—months (Mean ± SD; Min–Max) | 6 ± 3.1; 2–11 | |
| Regular use of technology (yes) | 7 | |
| GSE scale (Mean ± SD; Min–Max) | 29.2 ± 4.6; 20–38 | |
| SIS 3.0 (Mean ± SD) | 52.1 ± 15.6; 25.2–74.2 | |
| e-Heals (Mean ± SD; Min–Max) | 25.8 ± 9.5; 5–37 | |
| HLS-EU-PT (Mean ± SD; Min–Max) | 34 ± 11.9; 4.8–49.5 | |
| Informal caregivers (n = 12) | Gender (female) | 11 |
| Age (years Mean ± SD; Min–Max) | 52.6 ± 9.8; 36–69 | |
| Laboral Situation (Employee) | 10 | |
| Regular use of technology (yes) | 10 | |
| Previous experience of caring (no) | 8 | |
| QASCI-vr (Mean ± SD; Min–Max) | 2.9 ± 0.4; 2.4–3.5 | |
| GSE scale (Mean ± SD; Min–Max) | 33.0 ± 3.6; 27–40 | |
| e-Heals (Mean ± SD; Min–Max) | 27.4 ± 7.1; 12–37 | |
| HLS-EU-PT (Mean ± SD; Min–Max) | 36.9 ± 7; 26.1–47.9 | |
| Health professionals (n = 18) | Gender (female) | 15 |
| Working experience with PwS-years (Mean ± SD; Min–Max) | 17.2 ± 8.9; 5–30 | |
| Professional setting (n) | Hospital (inpatient stroke unit and outpatient rehabilitation): 15 | |
| Primary health care: 1 | ||
| Community rehabilitation: 2 | ||
| Profession (n) | Physiotherapist: 7 | |
| Speech and language therapist: 2 | ||
| Occupational therapist: 2 | ||
| Medical doctor: 1 | ||
| Psychologist: 1 | ||
| Social worker: 1 | ||
| Nurse: 4 |
| Tool | Outcome | Results | ||
|---|---|---|---|---|
| Total Score | Score PwS | Score HP | ||
| Workbook ComVida | PEMAT-P | |||
| Understandability (%) | 97.4% | 95.8% | 98.9% | |
| Actionality (%) | 100% | 100% | 100% | |
| PEMAT-AV | ||||
| Understandability (%) | - | - | 96.8% | |
| Actionality (%) | - | - | 90.8% | |
| SUS Average (Mean ± SD) | - | 88.2 ± 14.03 | - | |
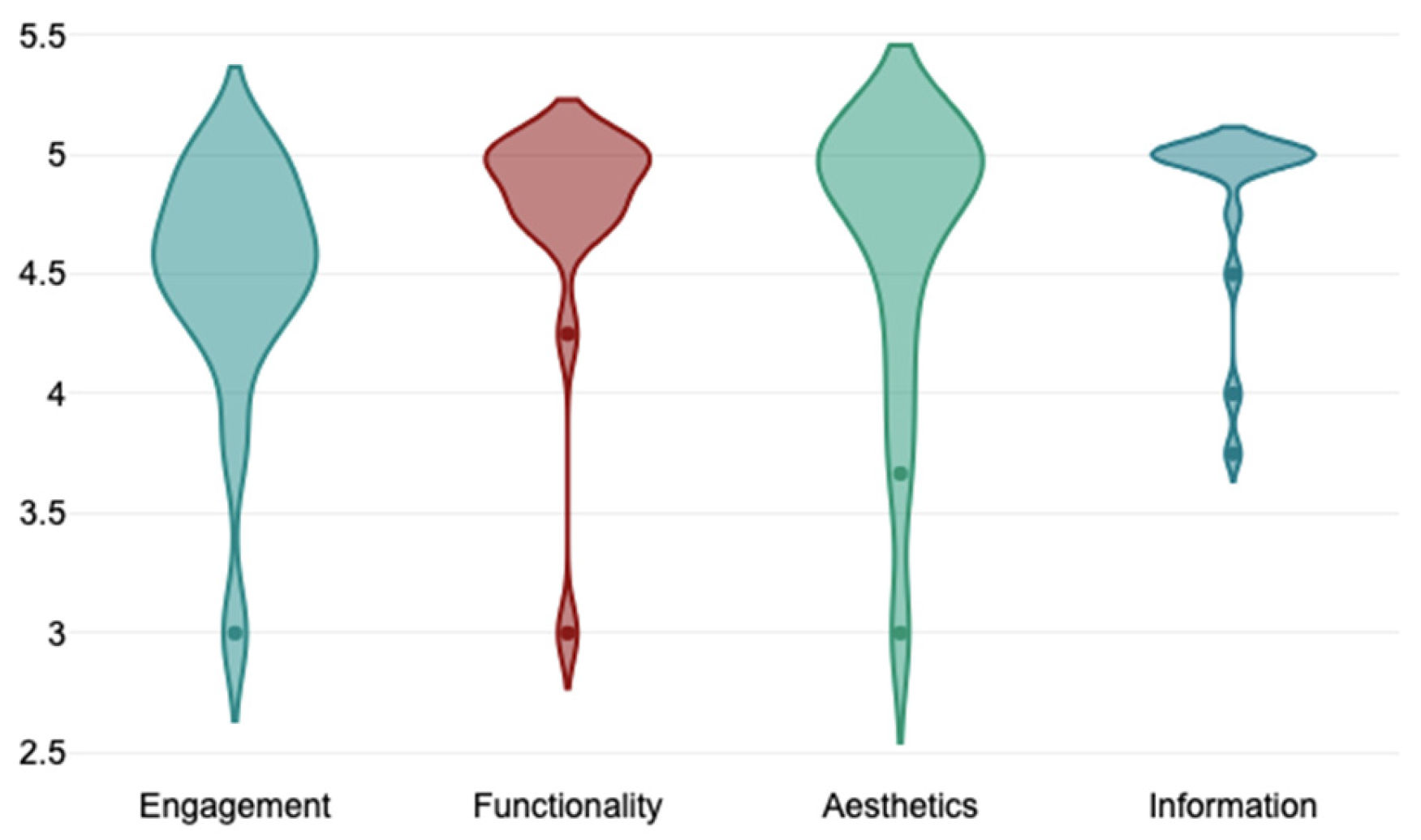
| Mobile App ComVida | uMARS total score (Mean ± SD) | - | 4.61 ± 0.48 | - |
| Objective quality of the App (Mean ± SD) | - | 4.66 ± 0.49 | - | |
| Subjective quality of the App (Mean ± SD) | - | 4.57 ± 0.53 | - | |
| Subjective quality of the App | - | 5 stars (1–5) | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendes Pereira, C.; Matos, M.; Carvalho, D.; Macedo, P.; Calheiros, J.M.; Alves, J.; Paulino Ferreira, L.; Dias, T.L.; Neves Madeira, R.; Jones, F. Building Bridges between People with Stroke, Families, and Health Professionals: Development of a Blended Care Program for Self-Management. J. Clin. Med. 2024, 13, 300. https://doi.org/10.3390/jcm13010300
Mendes Pereira C, Matos M, Carvalho D, Macedo P, Calheiros JM, Alves J, Paulino Ferreira L, Dias TL, Neves Madeira R, Jones F. Building Bridges between People with Stroke, Families, and Health Professionals: Development of a Blended Care Program for Self-Management. Journal of Clinical Medicine. 2024; 13(1):300. https://doi.org/10.3390/jcm13010300
Chicago/Turabian StyleMendes Pereira, Carla, Mara Matos, Daniel Carvalho, Patricia Macedo, José M. Calheiros, Janice Alves, Luís Paulino Ferreira, Teresa L. Dias, Rui Neves Madeira, and Fiona Jones. 2024. "Building Bridges between People with Stroke, Families, and Health Professionals: Development of a Blended Care Program for Self-Management" Journal of Clinical Medicine 13, no. 1: 300. https://doi.org/10.3390/jcm13010300
APA StyleMendes Pereira, C., Matos, M., Carvalho, D., Macedo, P., Calheiros, J. M., Alves, J., Paulino Ferreira, L., Dias, T. L., Neves Madeira, R., & Jones, F. (2024). Building Bridges between People with Stroke, Families, and Health Professionals: Development of a Blended Care Program for Self-Management. Journal of Clinical Medicine, 13(1), 300. https://doi.org/10.3390/jcm13010300