
Outer Retinal and Choroidal Changes in Adolescents with Long-Lasting Type 1 Diabetes

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
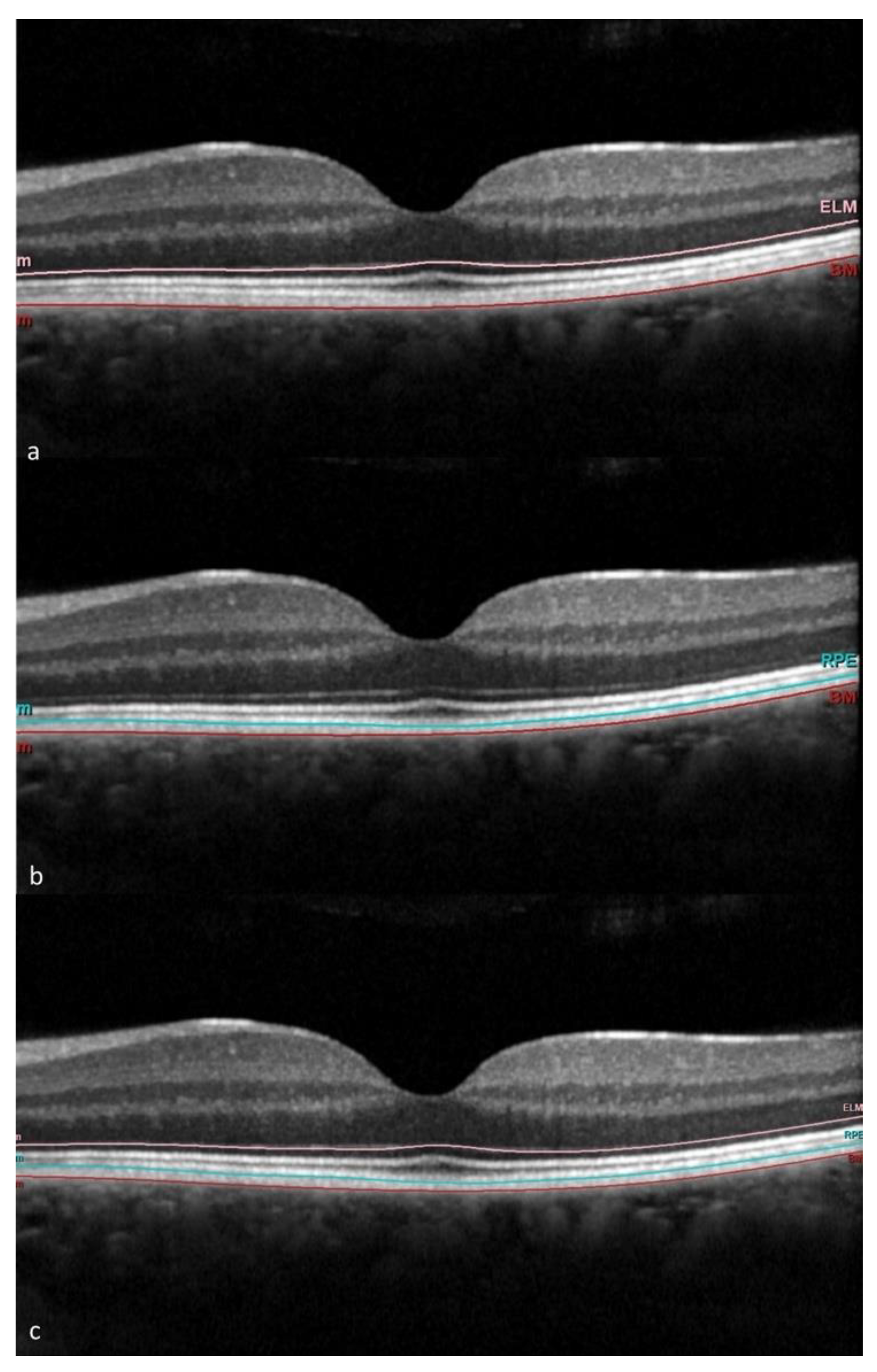
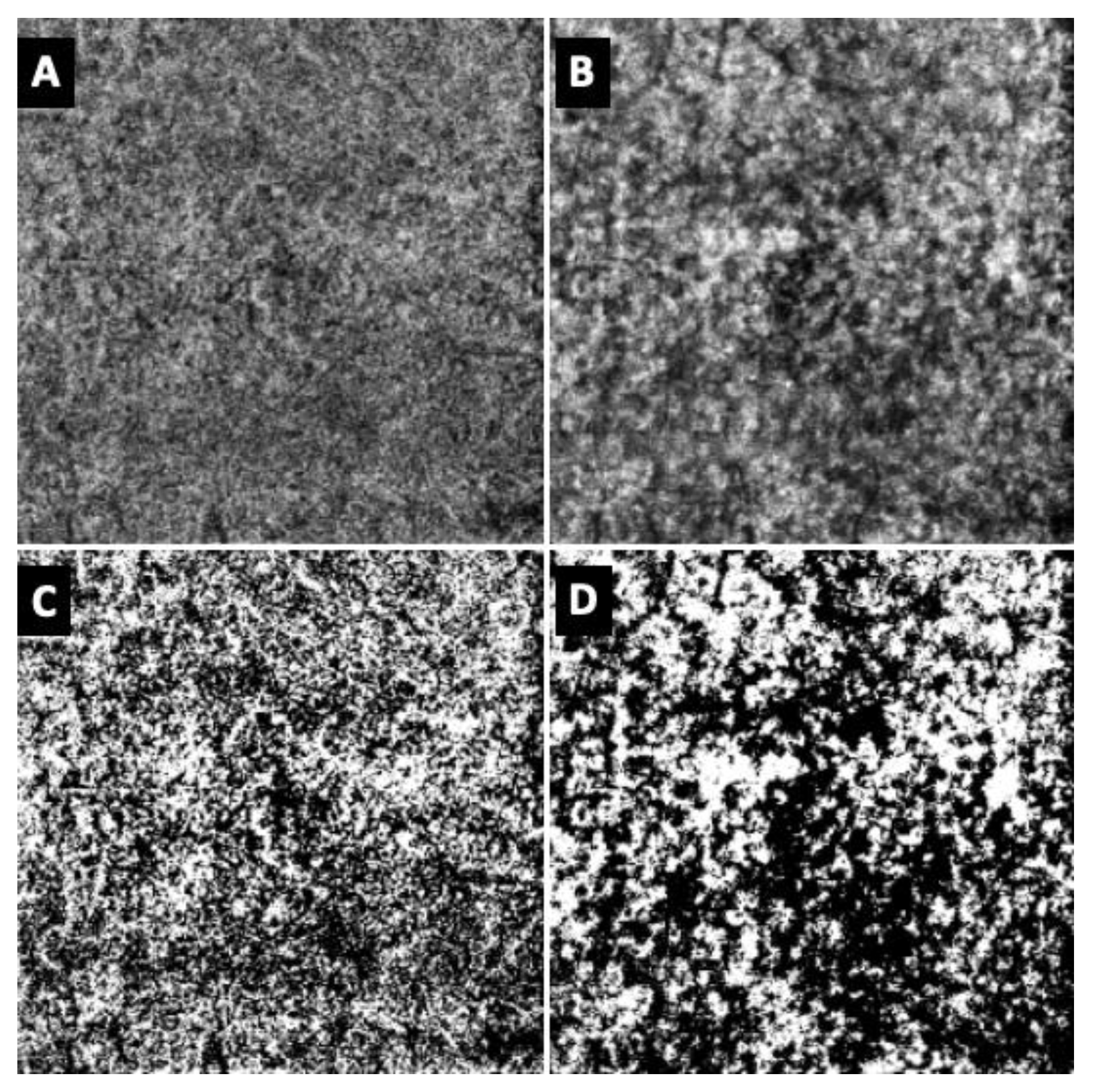
2.2. Imaging
2.3. Systemic Parameters
2.4. Statistical Analysis
3. Results
3.1. Population Features
3.2. OCT and OCTA Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nian, S.; Lo, A.C.Y.; Mi, Y.; Ren, K.; Yang, D. Neurovascular Unit in Diabetic Retinopathy: Pathophysiological Roles and Potential Therapeutical Targets. Eye Vis. 2021, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Antonetti, D.A.; Klein, R.; Gardner, T.W. Diabetic Retinopathy. N. Engl. J. Med. 2012, 366, 1227–1239. [Google Scholar] [CrossRef] [PubMed]
- Duh, E.J.; Sun, J.K.; Stitt, A.W. Diabetic Retinopathy: Current Understanding, Mechanisms, and Treatment Strategies. JCI Insight 2017, 2, e93751. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Midena, E. Retinal Layers Changes in Human Preclinical and Early Clinical Diabetic Retinopathy Support Early Retinal Neuronal and Müller Cells Alterations. J. Diabetes Res. 2013, 2013, 905058. [Google Scholar] [CrossRef]
- Pilotto, E.; Torresin, T.; Leonardi, F.; Gutierrez De Rubalcava Doblas, J.; Midena, G.; Moretti, C.; Midena, E. Retinal Microvascular and Neuronal Changes Are Also Present, Even If Differently, in Adolescents with Type 1 Diabetes without Clinical Diabetic Retinopathy. J. Clin. Med. 2022, 11, 3982. [Google Scholar] [CrossRef] [PubMed]
- Mameli, C.; Invernizzi, A.; Bolchini, A.; Bedogni, G.; Giani, E.; MacEdoni, M.; Zuccotti, G.; Preziosa, C.; Pellegrini, M. Analysis of Retinal Perfusion in Children, Adolescents, and Young Adults with Type 1 Diabetes Using Optical Coherence Tomography Angiography. J. Diabetes Res. 2019, 2019, 5410672. [Google Scholar] [CrossRef] [PubMed]
- Ebihara, S.; Machida, S.; Hara, Y.; Tada, A.; Ishizuka, M.; Gonmori, M.; Nishimura, T. Relationships between the Vascular Structure and Neural Function of the Macula in Patients with Diabetes Mellitus. Jpn. J. Ophthalmol. 2021, 65, 77–88. [Google Scholar] [CrossRef]
- Midena, E.; Torresin, T.; Longhin, E.; Midena, G.; Pilotto, E.; Frizziero, L. Early Microvascular and Oscillatory Potentials Changes in Human Diabetic Retina: Amacrine Cells and the Intraretinal Neurovascular Crosstalk. J. Clin. Med. 2021, 10, 4035. [Google Scholar] [CrossRef]
- Parravano, M.; Oddone, F.; Mineo, D.; Centofanti, M.; Borboni, P.; Lauro, R.; Tanga, L.; Manni, G. The Role of Humphrey Matrix Testing in the Early Diagnosis of Retinopathy in Type 1 Diabetes. Br. J. Ophthalmol. 2008, 92, 1656–1660. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- World Health Organization. Use of Glycated Haemoglobin (HbA1c) in the Diagnosis of Diabetes Mellitus. Available online: https://pubmed.ncbi.nlm.nih.gov/26158184/ (accessed on 22 January 2023).
- Wilkinson, C.P.; Ferris, F.L.; Klein, R.E.; Lee, P.P.; Agardh, C.D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J.T.; et al. Proposed International Clinical Diabetic Retinopathy and Diabetic Macular Edema Disease Severity Scales. Ophthalmology 2003, 110, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, M.V.; Rabiolo, A.; Marchese, A.; De Vitis, L.; Carnevali, A.; Querques, L.; Bandello, F.; Querques, G. Choroid Morphometric Analysis in Non-Neovascular Age-Related Macular Degeneration by Means of Optical Coherence Tomography Angiography. Br. J. Ophthalmol. 2017, 101, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Énzsöly, A.; Szabó, A.; Kántor, O.; Dávid, C.; Szalay, P.; Szabó, K.; Szél, Á.; Németh, J.; Lukáts, Á. Pathologic Alterations of the Outer Retina in Streptozotocin-Induced Diabetes. Invest. Ophthalmol. Vis. Sci. 2014, 55, 3686–3699. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, G.; Bucolo, C.; Drago, F.; Rossi, S.; Di Rosa, M.; Imbesi, R.; D’Agata, V.; Giunta, S. Attenuation of High Glucose-Induced Damage in RPE Cells through P38 MAPK Signaling Pathway Inhibition. Front. Pharmacol. 2021, 12, 684680. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xi, X.; Mei, Y.; Zhao, X.; Zhou, L.; Ma, M.; Liu, S.; Zha, X.; Yang, Y. High-Glucose Induces Retinal Pigment Epithelium Mitochondrial Pathways of Apoptosis and Inhibits Mitophagy by Regulating ROS/PINK1/Parkin Signal Pathway. Biomed. Pharmacother. 2019, 111, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Kim, D., II; Park, M.J.; Choi, J.H.; Lim, S.K.; Choi, H.J.; Park, S.H. Hyperglycemia-Induced GLP-1R Downregulation Causes RPE Cell Apoptosis. Int. J. Biochem. Cell Biol. 2015, 59, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Tonade, D.; Kern, T.S. Photoreceptor Cells and RPE Contribute to the Development of Diabetic Retinopathy. Prog. Retin. Eye Res. 2021, 83, 100919. [Google Scholar] [CrossRef]
- Willermain, F.; Scifo, L.; Weber, C.; Caspers, L.; Perret, J.; Delporte, C. Potential Interplay between Hyperosmolarity and Inflammation on Retinal Pigmented Epithelium in Pathogenesis of Diabetic Retinopathy. Int. J. Mol. Sci. 2018, 19, 1056. [Google Scholar] [CrossRef]
- Decanini, A.; Karunadharma, P.R.; Nordgaard, C.L.; Feng, X.; Olsen, T.W.; Ferrington, D.A. Human Retinal Pigment Epithelium Proteome Changes in Early Diabetes. Diabetologia 2008, 51, 1051–1061. [Google Scholar] [CrossRef]
- Barber, A.J.; Baccouche, B. Neurodegeneration in Diabetic Retinopathy: Potential for Novel Therapies. Vision Res. 2017, 139, 82–92. [Google Scholar] [CrossRef]
- Bresnick, G.H. Diabetic Retinopathy Viewed as a Neurosensory Disorder. Arch. Ophthalmol. 1986, 104, 989–990. [Google Scholar] [CrossRef] [PubMed]
- Gastinger, M.J.; Singh, R.S.J.; Barber, A.J. Loss of Cholinergic and Dopaminergic Amacrine Cells in Streptozotocin-Diabetic Rat and Ins2Akita-Diabetic Mouse Retinas. Invest. Ophthalmol. Vis. Sci. 2006, 47, 3143–3150. [Google Scholar] [CrossRef] [PubMed]
- Ly, A.; Yee, P.; Vessey, K.A.; Phipps, J.A.; Jobling, A.I.; Fletcher, E.L. Early Inner Retinal Astrocyte Dysfunction during Diabetes and Development of Hypoxia, Retinal Stress, and Neuronal Functional Loss. Invest. Ophthalmol. Vis. Sci. 2011, 52, 9316–9326. [Google Scholar] [CrossRef] [PubMed]
- Kern, T.S.; Barber, A.J. Retinal Ganglion Cells in Diabetes. J. Physiol. 2008, 586, 4401–4408. [Google Scholar] [CrossRef] [PubMed]
- Barber, A.J.; Gardner, T.W.; Abcouwer, S.F. The Significance of Vascular and Neural Apoptosis to the Pathology of Diabetic Retinopathy. Invest. Ophthalmol. Vis. Sci. 2011, 52, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Pilotto, E.; Bini, S.; Midena, E. Is Diabetic Retinopathy an Inflammatory Disease? Minerva Ophthalmol. 2018, 60, 26–35. [Google Scholar] [CrossRef]
- Kern, T.S.; Berkowitz, B.A. Photoreceptors in Diabetic Retinopathy. J. Diabetes Investig. 2015, 6, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Orduna-Hospital, E.; Sanchez-Cano, A.; Perdices, L.; Acha, J.; Lopez-Alaminos, E.M.; Pinilla, I. Changes in Retinal Layers in Type 1 Diabetes Mellitus without Retinopathy Measured by Spectral Domain and Swept Source OCTs. Sci. Rep. 2021, 11, 10427. [Google Scholar] [CrossRef]
- Pemp, B.; Palkovits, S.; Howorka, K.; Pumprla, J.; Sacu, S.; Garhöfer, G.; Bayerle-Eder, M.; Schmetterer, L.; Schmidt-Erfurth, U. Correlation of Retinal Neurodegeneration with Measures of Peripheral Autonomic Neuropathy in Type 1 Diabetes. Acta Ophthalmol. 2018, 96, e804. [Google Scholar] [CrossRef]
- Tan, W.; Wright, T.; Rajendran, D.; Garcia-Sanchez, Y.; Finkelberg, L.; Kisilak, M.; Campbell, M.; Westall, C.A. Cone-Photoreceptor Density in Adolescents With Type 1 Diabetes. Invest. Ophthalmol. Vis. Sci. 2015, 56, 6339–6343. [Google Scholar] [CrossRef]
- Lombardo, M.; Parravano, M.; Lombardo, G.; Varano, M.; Boccassini, B.; Stirpe, M.; Serrao, S. Adaptive Optics Imaging of Parafoveal Cones in Type 1 Diabetes. Retina 2014, 34, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, P.; Costanzo, E.; Giannini, D.; Fragiotta, S.; De Geronimo, D.; Giorno, P.; Picconi, F.; Frontoni, S.; Varano, M.; Parravano, M. In Vivo Assessment of Associations between Photoreceptors Structure and Macular Perfusion in Type 1 Diabetes. Br. J. Ophthalmol. 2023, 107, 1672–1679. [Google Scholar] [CrossRef] [PubMed]
- Arden, G.B.; Sivaprasad, S. Hypoxia and Oxidative Stress in the Causation of Diabetic Retinopathy. Curr. Diabetes Rev. 2011, 7, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Arden, G.B.; Sivaprasad, S. The Pathogenesis of Early Retinal Changes of Diabetic Retinopathy. Doc. Ophthalmol. 2012, 124, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; McLeod, D.S.; Merges, C.A.; Lutty, G.A. Choriocapillaris Degeneration and Related Pathologic Changes in Human Diabetic Eyes. Arch. Ophthalmol. 1998, 116, 589–597. [Google Scholar] [CrossRef]
- Lutty, G.A. Diabetic Choroidopathy. Vision Res. 2017, 139, 161–167. [Google Scholar] [CrossRef]
- Parravano, M.; Ziccardi, L.; Borrelli, E.; Costanzo, E.; Frontoni, S.; Picconi, F.; Parisi, V.; Sacconi, R.; Di Renzo, A.; Varano, M.; et al. Outer Retina Dysfunction and Choriocapillaris Impairment in Type 1 Diabetes. Sci. Rep. 2021, 11, 15183. [Google Scholar] [CrossRef]
- Wang, W.; Cheng, W.; Yang, S.; Chen, Y.; Zhu, Z.; Huang, W. Choriocapillaris Flow Deficit and the Risk of Referable Diabetic Retinopathy: A Longitudinal SS-OCTA Study. Br. J. Ophthalmol. 2023, 107, 1319–1323. [Google Scholar] [CrossRef]
- Tan, B.; Lim, N.A.; Tan, R.; Gan, A.T.L.; Chua, J.; Nusinovici, S.; Cheung, C.M.G.; Chakravarthy, U.; Wong, T.Y.; Schmetterer, L.; et al. Combining Retinal and Choroidal Microvascular Metrics Improves Discriminative Power for Diabetic Retinopathy. Br. J. Ophthalmol. 2023, 107, 993–999. [Google Scholar] [CrossRef]
- Ghassemi, F.; Fadakar, K.; Berijani, S.; Babeli, A.; Gholizadeh, A.; Sabour, S. Quantitative Assessment of Vascular Density in Diabetic Retinopathy Subtypes with Optical Coherence Tomography Angiography. BMC Ophthalmol. 2021, 21, 82. [Google Scholar] [CrossRef]
- Borrelli, E.; Palmieri, M.; Viggiano, P.; Ferro, G.; Mastropasqua, R. Photoreceptor damage in diabetic choroidopathy. Retina 2020, 40, 1062–1069. [Google Scholar] [CrossRef] [PubMed]
- Gołȩbiewska, J.; Olechowski, A.; Wysocka-Mincewicz, M.; Baszyńska-Wilk, M.; Groszek, A.; Czeszyk-Piotrowicz, A.; Szalecki, M.; Hautz, W. Choroidal Thickness and Ganglion Cell Complex in Pubescent Children with Type 1 Diabetes without Diabetic Retinopathy Analyzed by Spectral Domain Optical Coherence Tomography. J. Diabetes Res. 2018, 2018, 5458015. [Google Scholar] [CrossRef] [PubMed]
- Sayin, N.; Kara, N.; Pirhan, D.; Vural, A.; Ersan, H.B.A.; Onal, H.; Cinar, S. Evaluation of Subfoveal Choroidal Thickness in Children with Type 1 Diabetes Mellitus: An EDI-OCT Study. Semin. Ophthalmol. 2014, 29, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Q.; Jeppesen, P.; Larsen, M.; Munch, I.C. Subfoveal Choroidal Thickness in 1323 Children Aged 11 to 12 Years and Association with Puberty: The Copenhagen Child Cohort 2000 Eye Study. Invest. Ophthalmol. Vis. Sci. 2014, 55, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Xiong, S.; He, X.; Zhang, B.; Deng, J.; Wang, J.; Lv, M.; Zhu, J.; Zou, H.; Xu, X. Changes in Choroidal Thickness Varied by Age and Refraction in Children and Adolescents: A 1-Year Longitudinal Study. Am. J. Ophthalmol. 2020, 213, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Marta, W.M.; Andrzej, O.; Marta, B.W.; Aleksandra, B.; Joanna, G. Choroidal Thickness in Children with Type 1 Diabetes Depending on the Pubertal Status and Metabolic Parameters Analyzed by Optical Coherence Tomography. Sci. Rep. 2021, 11, 19677. [Google Scholar] [CrossRef]
- Ahmed, J.; Braun, R.D.; Dunn, R.; Lisenmeier, R.A. Oxygen Distribution in the Macaque Retina. Invest. Ophthalmol. Vis. Sci. 1993, 34, 516–521. [Google Scholar]
- Yi, J.; Liu, W.; Chen, S.; Backman, V.; Sheibani, N.; Sorenson, C.M.; Fawzi, A.A.; Linsenmeier, R.A.; Zhang, H.F. Visible Light Optical Coherence Tomography Measures Retinal Oxygen Metabolic Response to Systemic Oxygenation. Light. Sci. Appl. 2015, 4, e334. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameter | DR Group (N = 5) | noDR Group (N = 31) | HC Group (N = 15) |
|---|---|---|---|
| Sex (males:females) | 2:3 | 13:18 | 4:11 |
| Mean age ± SD (years) | 17.0 ± 1.6 | 17.2 ± 2.0 | 17.3 ± 3.1 |
| T1D mean duration ± SD (years) | 10.6 ± 4.07 | 13.0 ± 2.80 | n.a. |
| Parameter | DR Group | noDR Group | p-Value |
|---|---|---|---|
| Mean glucose ± SD (mg/dL) | 179.6 ± 14.0 | 178.2 ± 30.9 | 0.864 |
| Glycemic variability (SD) ± SD (mg/dL) | 84.4 ± 7.0 | 80.0 ± 14.7 | 0.339 |
| TIR ± SD (%) | 48.3 ± 3.9 | 46.6 ± 11.2 | 0.549 |
| TBR ± SD (%) | 9.3 ± 4.7 | 9.7 ± 6.9 | 0.880 |
| HbA1c ± SD (%) | 7.7 ± 0.9 | 7.6 ± 1.0 | 0.773 |
| Weight (kg) | 64.4 ± 10.3 | 62.9 ± 11.3 | 0.783 |
| BMI (kg/m2) | 23.7 ± 3.1 | 21.2 ± 2.57 | 0.066 |
| Total insulin daily dose (IU/die) | 61.8 ± 28.0 | 53.2 ± 14.5 | 0.296 |
| Insulin daily dose adjusted for weight (IU/kg/die) | 0.95 ± 0.3 | 0.85 ± 0.21 | 0.377 |
| Basal insulin over total (%) | 47.4 ± 16.3 | 54.8 ± 12.7 | 0.251 |
| Insulin bolus over total (%) | 52.6 ± 16.3 | 45.1 ± 12.7 | 0.251 |
| Sector | HC Group Mean ± SD (n = 30 Eyes) | DR Group Mean ± SD (n = 10 Eyes) | noDR Group Mean ± SD (n = 62 Eyes) | p-Value DR vs. noDR | p-Value DR vs. HC | p-Value noDR vs. HC |
|---|---|---|---|---|---|---|
| Global | 67.2 ± 1.7 | 68.4 ± 1.9 | 67.6 ± 1.9 | 0.241 | 0.202 | 0.492 |
| Central | 74.7 ± 3.8 | 75.6 ± 5.1 | 75.8 ± 3.7 | 0.631 | 0.481 | 0.113 |
| IS | 66.7 ± 2.0 | 67.8 ± 1.8 | 67.1 ± 2.2 | 0.439 | 0.374 | 0.612 |
| IN | 68.5 ± 2.6 | 68.7 ± 1.4 | 68.8 ± 2.6 | 0.761 | 0.956 | 0.707 |
| II | 66.5 ± 1.9 | 67.1 ± 2.0 | 66.8 ± 3.2 | 0.784 | 0.670 | 0.742 |
| IT | 68.2 ± 2.4 | 68.6 ± 1.6 | 68.4 ± 2.5 | 0.902 | 0.762 | 0.764 |
| OS | 65.5 ± 2.2 | 67.1 ± 2.4 | 65.9 ± 2.0 | 0.159 | 0.158 | 0.540 |
| ON | 65.5 ± 2.0 | 67.5 ± 3.4 | 66.0 ± 2.2 | 0.078 | 0.045 * | 0.437 |
| OI | 63.8 ± 2.3 | 66.0 ± 3.4 | 64.3 ± 2.1 | 0.040 * | 0.045 * | 0.535 |
| OT | 65.2 ± 2.0 | 67.1 ± 3.2 | 65.3 ± 2.2 | 0.030 * | 0.104 | 0.969 |
| Sector | HC Group Mean ± SD (n = 30 Eyes) | DR Group Mean ± SD (n = 10 Eyes) | noDR Group Mean ± SD (n = 62 Eyes) | p-Value DR vs. noDR | p-Value DR vs. HC | p-Value noDR vs. HC |
|---|---|---|---|---|---|---|
| Global | 14.8 ± 1.1 | 15.6 ± 1.7 | 15.5 ± 1.1 | 0.967 | 0.353 | 0.083 |
| Central | 18.5 ± 1.7 | 18.5 ± 2.3 | 18.5 ± 1.8 | 0.152 | 0.350 | 0.960 |
| IS | 14.9 ± 1.4 | 15.6 ± 1.8 | 15.8 ± 1.4 | 0.419 | 0.471 | 0.038 * |
| IN | 15.8 ± 1.6 | 16.6 ± 1.8 | 16.4 ± 1.3 | 0.937 | 0.391 | 0.172 |
| II | 14.7 ± 1.5 | 15.7 ± 2.2 | 15.4 ± 2.3 | 0.684 | 0.239 | 0.118 |
| IT | 14.3 ± 1.8 | 15.5 ± 2.1 | 15.4 ± 1.5 | 0.943 | 0.159 | 0.014 * |
| OS | 14.0 ± 1.3 | 14.9 ± 1.4 | 14.6 ± 1.4 | 0.700 | 0.277 | 0.153 |
| ON | 14.7 ± 1.4 | 15.1 ± 2.0 | 14.9 ± 1.4 | 0.824 | 0.690 | 0.665 |
| OI | 13.6 ± 1.1 | 14.6 ± 1.5 | 14.5 ± 1.4 | 0.864 | 0.221 | 0.024 * |
| OT | 12.8 ± 1.6 | 14.0 ± 1.9 | 13.5 ± 1.5 | 0.357 | 0.146 | 0.139 |
| Parameter | HC Group Mean ± SD (n = 30 Eyes) | T1D Group Mean ± SD (n = 72 Eyes) | DR Group Mean ± SD (n = 10 Eyes) | noDR Group Mean ± SD (n = 62 Eyes) | p-Value T1D vs. HC | p-Value DR vs. noDR | p-Value DR vs. HC | p-Value noDR vs. HC |
|---|---|---|---|---|---|---|---|---|
| CC VD | 0.434 ± 0.038 | 0.423 ± 0.035 | 0.418 ± 0.031 | 0.424 ± 0.036 | 0.2794 | 0.577 | 0.185 | 0.219 |
| CC SD | 0.566 ± 0.038 | 0.577 ± 0.035 | 0.582 ± 0.031 | 0.576 ± 0.036 | 0.2794 | 0.577 | 0.185 | 0.219 |
| CC V/S ratio | 0.775 ± 0.115 | 0.741 ± 0.107 | 0.723 ± 0.093 | 0.744 ± 0.110 | 0.2617 | 0.537 | 0.159 | 0.202 |
| Ch VD | 0.376 ± 0.052 | 0.374 ± 0.056 | 0.398 ± 0.047 | 0.365 ± 0.054 | 0.9266 | 0.067 | 0.208 | 0.380 |
| Ch SD | 0.624 ± 0.052 | 0.626 ± 0.056 | 0.602 ± 0.047 | 0.635 ± 0.054 | 0.9266 | 0.067 | 0.208 | 0.380 |
| Ch V/S ratio | 0.612 ± 0.138 | 0.610 ± 0.141 | 0.671 ± 0.132 | 0.587 ± 0.129 | 0.9498 | 0.084 | 0.239 | 0.375 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilotto, E.; Cosmo, E.; Torresin, T.; Coppola, M.; Gutierrez De Rubalcava Doblas, J.; Midena, G.; Moretti, C.; Midena, E. Outer Retinal and Choroidal Changes in Adolescents with Long-Lasting Type 1 Diabetes. J. Clin. Med. 2024, 13, 229. https://doi.org/10.3390/jcm13010229
Pilotto E, Cosmo E, Torresin T, Coppola M, Gutierrez De Rubalcava Doblas J, Midena G, Moretti C, Midena E. Outer Retinal and Choroidal Changes in Adolescents with Long-Lasting Type 1 Diabetes. Journal of Clinical Medicine. 2024; 13(1):229. https://doi.org/10.3390/jcm13010229
Chicago/Turabian StylePilotto, Elisabetta, Eleonora Cosmo, Tommaso Torresin, Marco Coppola, Joaquin Gutierrez De Rubalcava Doblas, Giulia Midena, Carlo Moretti, and Edoardo Midena. 2024. "Outer Retinal and Choroidal Changes in Adolescents with Long-Lasting Type 1 Diabetes" Journal of Clinical Medicine 13, no. 1: 229. https://doi.org/10.3390/jcm13010229
APA StylePilotto, E., Cosmo, E., Torresin, T., Coppola, M., Gutierrez De Rubalcava Doblas, J., Midena, G., Moretti, C., & Midena, E. (2024). Outer Retinal and Choroidal Changes in Adolescents with Long-Lasting Type 1 Diabetes. Journal of Clinical Medicine, 13(1), 229. https://doi.org/10.3390/jcm13010229