
Beliefs about Medicines and the Level of Intentional Non-Adherence to Treatment among Patients with Multiple Sclerosis Treated with First-Line Drugs

Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
- (1)
- Fulfilled the McDonald’s criteria;
- (2)
- Treatment with DMT therapy;
- (3)
- Signed informed consent.
2.2. Questionnaires
- The Intentional Non-Adherence Scale (INAS) is a scale to assess intentional non-adherence to prescribed medications [9]. The questionnaire consists of 22-item scale scored on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). The final score ranges between 22 and 110, and higher scores indicate poorer adherence.
2.3. Ethical Consideration
2.4. Statistical Methods
3. Results
3.1. Sociodemographic and Clinical Characteristics
3.2. Level of Intentional Non-Adherence (INAS Scores) and Beliefs about Medication (BMQ Scores)
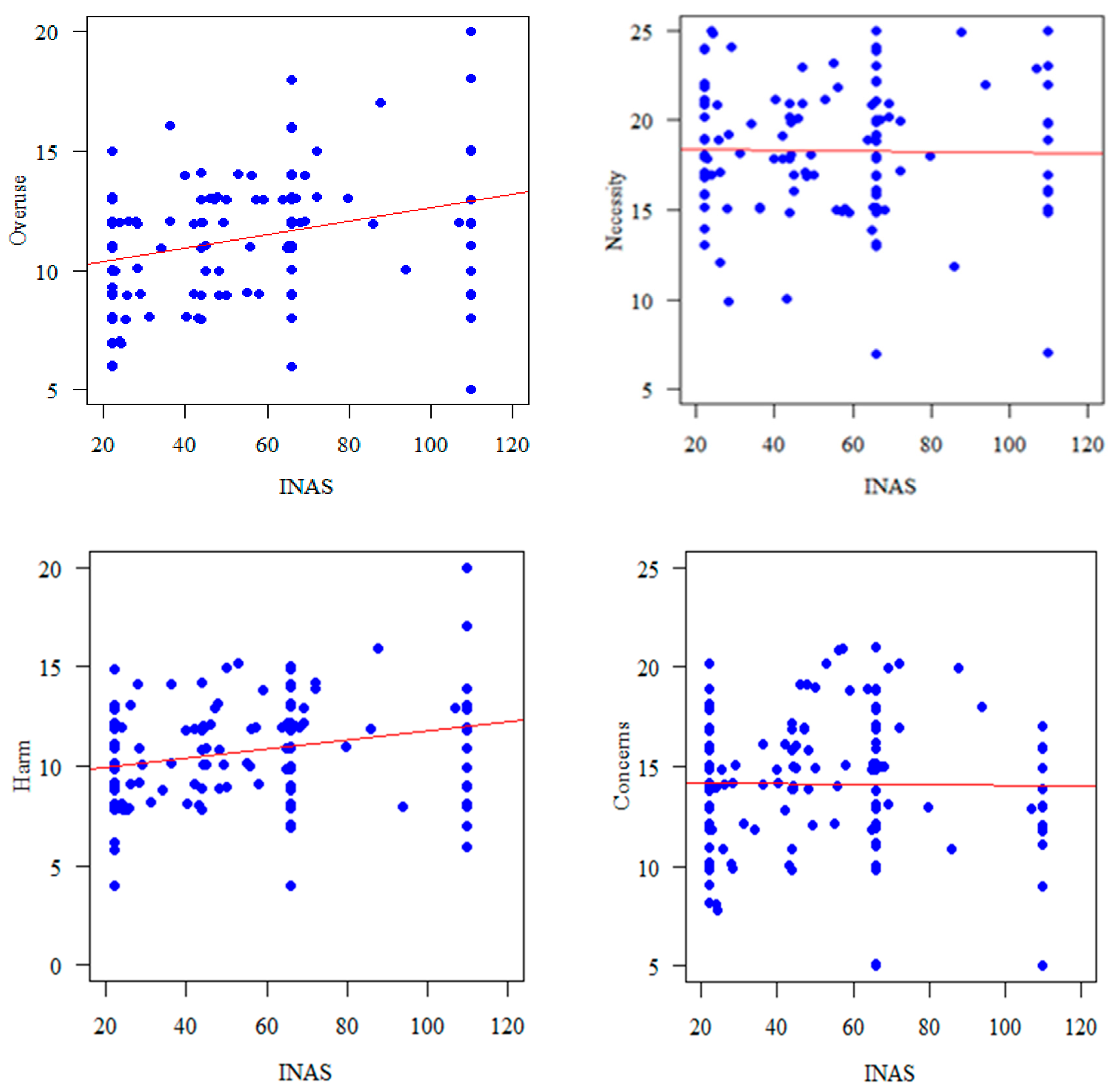
3.3. Correlation between Non-Adherence and Beliefs about Medication
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Steiner, J.F.; Prochazka, A.V. The assessment of refill compliance using pharmacy records: Methods, validity, and applications. J. Clin. Epidemiol. 1997, 50, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Li, S.C. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther. Clin. Risk Manag. 2008, 4, 269–286. [Google Scholar] [CrossRef] [PubMed]
- Haynes, R.B.; McDonald, H.P.; Garg, A.X. Helping Patients Follow Prescribed Treatment: Clinical Applications. JAMA 2002, 288, 2880. [Google Scholar] [CrossRef] [PubMed]
- Danner, U.N.; Aarts, H.; Vries, N.K. Habit vs. intention in the prediction of future behaviour: The role of frequency, context stability and mental accessibility of past behaviour. Br. J. Soc. Psychol. 2008, 47, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Phillips, L.A.; Cohen, J.; Burns, E.; Abrams, J.; Renninger, S. Self-management of chronic illness: The role of ‘habit’ versus reflective factors in exercise and medication adherence. J. Behav. Med. 2016, 39, 1076–1091. [Google Scholar] [CrossRef] [PubMed]
- Leventhal, H.; Phillips, L.A.; Burns, E. The Common-Sense Model of Self-Regulation (CSM): A dynamic framework for understanding illness self-management. J. Behav. Med. 2016, 39, 935–946. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; Chapman, S.C.E.; Parham, R.; Freemantle, N.; Forbes, A.; Cooper, V. Understanding Patients’ Adherence-Related Beliefs about Medicines Prescribed for Long-Term Conditions: A Meta-Analytic Review of the Necessity-Concerns Framework. PLoS ONE 2013, 8, e80633. [Google Scholar] [CrossRef]
- Weinman, J.; Graham, S.; Canfield, M.; Kleinstäuber, M.; Perera, A.I.; Dalbeth, N.; Petrie, K.J. The Intentional Non-Adherence Scale (INAS): Initial development and validation. J. Psychosom. Res. 2018, 115, 110–116. [Google Scholar] [CrossRef]
- Hauser, S.L.; Cree, B.A.C. Treatment of Multiple Sclerosis: A Review. Am. J. Med. 2020, 133, 1380–1390.e2. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J.; Hankins, M. The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- Karbownik, M.S.; Jankowska-Polańska, B.; Horne, R.; Górski, K.M.; Kowalczyk, E.; Szemraj, J. Adaptation and validation of the Polish version of the Beliefs about Medicines Questionnaire among cardiovascular patients and medical students. PLoS ONE 2020, 15, e0230131. [Google Scholar] [CrossRef] [PubMed]
- Gatt, I.; West, L.M.; Calleja, N.; Briffa, C.; Cordina, M. Psychometric properties of the Belief about Medicines Questionnaire (BMQ) in the Maltese language. Pharm. Pract. 2017, 15, 886. [Google Scholar] [CrossRef] [PubMed]
- Pardo, G.; Pineda, E.D.; Ng, C.D.; Sheinson, D.; Bonine, N.G. The Association Between Persistence and Adherence to Disease-Modifying Therapies and Healthcare Resource Utilization and Costs in Patients With Multiple Sclerosis. J. Health Econ. Outcomes Res. 2022, 9, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Yermakov, S.; Davis, M.; Calnan, M.; Fay, M.; Cox-Buckley, B.; Sarda, S.; Duh, M.S.; Iyer, R. Impact of increasing adherence to disease-modifying therapies on healthcare resource utilization and direct medical and indirect work loss costs for patients with multiple sclerosis. J. Med. Econ. 2015, 18, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Nicholas, J.A.; Edwards, N.C.; Edwards, R.A.; Dellarole, A.; Grosso, M.; Phillips, A.L. Real-world adherence to, and persistence with, once- and twice-daily oral disease-modifying drugs in patients with multiple sclerosis: A systematic review and meta-analysis. BMC Neurol. 2020, 20, 281. [Google Scholar] [CrossRef]
- Menzin, J.; Caon, C.; Nichols, C.; White, L.A.; Friedman, M.; Pill, M.W. Narrative Review of the Literature on Adherence to Disease-Modifying Therapies Among Patients with Multiple Sclerosis. J. Manag. Care Pharm. 2013, 19, S24–S40. [Google Scholar] [CrossRef] [PubMed]
- Morillo Verdugo, R.; Ramírez-Herráiz, E.; Fernández-Del Olmo, R.; Roig Bonet, M.; Valdivia Garcia, M. Adherence to disease-modifying treatments in patients with multiple sclerosis in Spain. Patient Prefer. Adherence 2019, 13, 261–272. [Google Scholar] [CrossRef]
- Haas, J.; Firzlaff, M. Twenty-four-month comparison of immunomodulatory treatments—A retrospective open label study in 308 RRMS patients treated with beta interferons or glatiramer acetate (Copaxone®). Eur. J. Neurol. 2005, 12, 425–431. [Google Scholar] [CrossRef]
- Hansen, K.; Schüssel, K.; Kieble, M.; Werning, J.; Schulz, M.; Friis, R.; Pöhlau, D.; Schmitz, N.; Kugler, J. Adherence to Disease Modifying Drugs among Patients with Multiple Sclerosis in Germany: A Retrospective Cohort Study. PLoS ONE 2015, 10, e0133279. [Google Scholar] [CrossRef]
- Burks, J.; Marshall, T.; Ye, X. Adherence to disease-modifying therapies and its impact on relapse, health resource utilization, and costs among patients with multiple sclerosis. ClinicoEconomics Outcomes Res. 2017, 9, 251–260. [Google Scholar] [CrossRef]
- Gadkari, A.S.; McHorney, C.A. Unintentional non-adherence to chronic prescription medications: How unintentional is it really? BMC Health Serv. Res. 2012, 12, 98. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Zivadinov, R. Risk factors for and management of cognitive dysfunction in multiple sclerosis. Nat. Rev. Neurol. 2011, 7, 332–342. [Google Scholar] [CrossRef]
- Munsell, M.; Frean, M.; Menzin, J.; Phillips, A.L. An evaluation of adherence in patients with multiple sclerosis newly initiating treatment with a self-injectable or an oral disease-modifying drug. Patient Prefer. Adherence 2016, 11, 55–62. [Google Scholar] [CrossRef]
- Gerber, B.; Cowling, T.; Chen, G.; Yeung, M.; Duquette, P.; Haddad, P. The impact of treatment adherence on clinical and economic outcomes in multiple sclerosis: Real world evidence from Alberta, Canada. Mult. Scler. Relat. Disord. 2017, 18, 218–224. [Google Scholar] [CrossRef]
- Marrero, R.J.; Fumero, A.; De Miguel, A.; Peñate, W. Psychological factors involved in psychopharmacological medication adherence in mental health patients: A systematic review. Patient Educ. Couns. 2020, 103, 2116–2131. [Google Scholar] [CrossRef]
- Thach, A.V.; Brown, C.M.; Herrera, V.; Sasane, R.; Barner, J.C.; Ford, K.C.; Lawson, K.A. Associations Between Treatment Satisfaction, Medication Beliefs, and Adherence to Disease-Modifying Therapies in Patients with Multiple Sclerosis. Int. J. MS Care 2018, 20, 251–259. [Google Scholar] [CrossRef]
- Pust, G.E.; Untiedt, B.; Randerath, J.; Barabasch, A.; Köpke, S.; Rahn, A.C.; Hansen, H.; Heesen, C. Exploring Adherence to First-Line and Second-Line Immunotherapies in Multiple Sclerosis. Int. J. MS Care 2020, 22, 219–225. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 1999, 47, 555–567. [Google Scholar] [CrossRef]
- Świątoniowska-Lonc, N.; Polański, J.; Mazur, G.; Jankowska-Polańska, B. Impact of Beliefs about Medicines on the Level of Intentional Non-Adherence to the Recommendations of Elderly Patients with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 2825. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.; Pereira, C.; Monteiro, M.J.; Santos, C. Patients’ beliefs about medicines and adherence to medication in ischemic heart disease. Aten. Primaria 2014, 46, 101–106. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Jamous, R.; Sweileh, W.; El-Deen Abu Taha, A.; Zyoud, S. Beliefs about medicines and self-reported adherence among patients with chronic illness: A study in Palestine. J. Fam. Med. Prim. Care 2014, 3, 224. [Google Scholar]
- Neter, E.; Glass-Marmor, L.; Wolkowitz, A.; Lavi, I.; Miller, A. Beliefs about medication as predictors of medication adherence in a prospective cohort study among persons with multiple sclerosis. BMC Neurol. 2021, 21, 136. [Google Scholar] [CrossRef]
- Štrosová, D.; Tužil, J.; Turková, B.V.; Pilnáčková, B.F.; de Souza, L.L.; Doležalová, H.; Rašková, M.; Dufek, M.; Doležal, T. Relationship between Patient Preferences, Attitudes to Treatment, Adherence, and Quality of Life in New Users of Teriflunomide. Pharmaceuticals 2022, 15, 1248. [Google Scholar] [CrossRef]
- Yazdi-Feyzabadi, V.; Nakhaee, N.; Mehrolhassani, M.H.; Naghavi, S.; Homaie Rad, E. Development and validation of a questionnaire to determine medical orders non-adherence: A sequential exploratory mixed-method study. BMC Health Serv. Res. 2021, 21, 136. [Google Scholar] [CrossRef]
- Bischoff, C.; Schreiber, H.; Bergmann, A. Background information on multiple sclerosis patients stopping ongoing immunomodulatory therapy: A multicenter study in a community-based environment. J. Neurol. 2012, 259, 2347–2353. [Google Scholar] [CrossRef]
- Castelan, A.; Nellen, J.F.; Van Der Valk, M.; Nieuwkerk, P.T. Intentional-but not Unintentional Medication Non-adherence was Related with Beliefs about Medicines Among a Multi-Ethnic Sample of People with HIV. AIDS Behav. 2023, 27, 1045–1054. [Google Scholar] [CrossRef]


{kind=link}
| Variables | (n = 148) | |
|---|---|---|
| Age [years] | mean ± SD | 43.9 ± 10.19 |
| median | 42 | |
| quartiles | 37–50 | |
| EDSS [score] | mean ± SD | 2.38 ± 1.27 |
| median | 2 | |
| quartiles | 1.5–3 | |
| Duration of the disease [years] | mean ± SD | 12.07 ± 6.35 |
| median | 11.5 | |
| quartiles | 7–17 | |
| Number of relapses in the last two years? | mean ± SD | 0.62 ± 1.08 |
| median | 0 | |
| quartiles | 0–1 | |
| Duration of DMTs use (years) | mean ± SD | 6.22 ± 3.67 |
| median | 6 | |
| quartiles | 0.3–9 | |
| Gender, n (%) | Female | 100 (67.57%) |
| Male | 48 (32.43%) | |
| Form of the medicine, n (%) | Injections | 61 (41.22%) |
| Tablets | 87 (58.78%) | |
| Place of residence, n (%) | Village | 35 (23.65%) |
| City < 50 thousand residents | 40 (27.03%) | |
| City 50–500 thousand residents | 20 (13.51%) | |
| City > 500 thousand residents | 53 (35.81%) | |
| Education, n (%) | Basic or vocational education | 23 (15.54%) |
| Secondary education | 55 (37.16%) | |
| Higher education | 70 (47.30%) | |
| Marital status, n (%) | Single | 30 (20.27%) |
| Married | 101 (68.24%) | |
| Divorced | 16 (10.81%) | |
| Widowed | 1 (0.68%) | |
| Occupational activity, n (%) | Active/working | 101 (68.24%) |
| Retired | 12 (8.11%) | |
| Pension | 23 (15.54%) | |
| Unemployed | 10 (6.76%) | |
| Student | 2 (1.35%) | |
| Complains, n (%) | Speech disorders | 19 (12.84%) |
| Hypertonia | 33 (22.30%) | |
| Mood disorders | 44 (29.73%) | |
| Sensory disorders | 32 (21.62%) | |
| Mobility and balance disorders | 84 (56.76%) | |
| Sexual disorders | 39 (26.35%) | |
| Vision disorders | 73 (49.32%) | |
| Sphincter disorders | 52 (35.14%) | |
| Dysphagia | 12 (8.11%) | |
| Fatigability | 105 (0.95%) | |
| Mean | SD | Median | Min | Max | Q1 | Q3 | ||
|---|---|---|---|---|---|---|---|---|
| INAS | 51.41 | 27.83 | 47.0 | 22 | 110 | 22.00 | 66 | |
| BMQ | Overuse | 11.28 | 2.50 | 11.5 | 5 | 20 | 9.25 | 13 |
| BMQ | Harm | 10.69 | 2.55 | 11.0 | 4 | 20 | 9.00 | 12 |
| BMQ | Necessity | 18.30 | 3.41 | 18.0 | 7 | 25 | 16.00 | 21 |
| BMQ | Concerns | 14.17 | 3.29 | 14.0 | 5 | 21 | 12.00 | 16 |
| Variable | Parametr | 95% CI | p | ||
|---|---|---|---|---|---|
| Gender | Female | ref. | |||
| Male | 7.406 | −2.129 | 16.941 | 0.13 | |
| Age [years] | 0.348 | −0.091 | 0.788 | 0.123 | |
| Form of the medicine | Injections | ref. | |||
| Tablets | 7.648 | −1.408 | 16.703 | 0.1 | |
| EDSS score | 0.142 | −3.406 | 3.69 | 0.938 | |
| Place of residence | Village | ref. | |||
| City < 50 thousand residents | 6.718 | −5.94 | 19.375 | 0.3 | |
| City 50–500 thousand residents | −1.207 | −16.536 | 14.122 | 0.878 | |
| City > 500 thousand residents | −1.387 | −13.299 | 10.524 | 0.82 | |
| Education | Basic or vocational education | ref. | |||
| Secondary education | −0.236 | −13.741 | 13.27 | 0.973 | |
| Higher education | −7.859 | −20.931 | 5.213 | 0.241 | |
| Marital status | Single | ref. | |||
| Married | −2.477 | −13.778 | 8.824 | 0.668 | |
| Divorced, Widowed | 10.184 | −6.315 | 26.684 | 0.228 | |
| Occupational activity | Active/working, student | ref. | |||
| Retired | 16.141 | −0.374 | 32.657 | 0.057 | |
| Pension | 9.388 | −3.099 | 21.875 | 0.143 | |
| Unemployed | 1.775 | −16.159 | 19.709 | 0.846 | |
| Disease duration (years) | 0.098 | −0.612 | 0.808 | 0.787 | |
| Number of relapses in the last two years? | 1.101 | −3.083 | 5.285 | 0.607 | |
| Duration of DMTs use (years) | 0.339 | −0.978 | 1.657 | 0.614 | |
| Speech disorders | No | ref. | |||
| Yes | 4.055 | −9.378 | 17.488 | 0.555 | |
| Hypertonia | No | ref. | |||
| Yes | 0.215 | −10.593 | 11.024 | 0.969 | |
| Mood disorders | No | ref. | |||
| Yes | −4.82 | −14.631 | 4.992 | 0.337 | |
| Sensory disorders | No | ref. | |||
| Yes | −6.342 | −17.222 | 4.538 | 0.255 | |
| Mobility and balance disorders | No | ref. | |||
| Yes | −1.446 | −10.524 | 7.632 | 0.755 | |
| Sexual disorders | No | ref. | |||
| Yes | −3.515 | −13.711 | 6.681 | 0.5 | |
| Vision disorders | No | ref. | |||
| Yes | −8.277 | −17.175 | 0.621 | 0.07 | |
| Sphincter disorders | No | ref. | |||
| Yes | −1.551 | −10.972 | 7.869 | 0.747 | |
| Dysphagia | No | ref. | |||
| Yes | 2.634 | −13.842 | 19.11 | 0.754 | |
| Fatigability | No | ref. | |||
| Yes | −3.907 | −13.796 | 5.981 | 0.44 | |
| Variable | Parametr | 95%CI | p | ||
|---|---|---|---|---|---|
| Gender | Female | ref. | |||
| Male | 8.599 | −0.68 | 17.877 | 0.072 | |
| Age | [years] | 0.137 | −0.347 | 0.622 | 0.58 |
| Form of the medicine | Injections | ref. | |||
| Tablets | 7.896 | −1.041 | 16.834 | 0.086 | |
| Occupational activity | Active/working, student | ref. | |||
| Retired | 11.632 | −6.272 | 29.537 | 0.205 | |
| Pension | 7.226 | −5.24 | 19.693 | 0.258 | |
| Unemployed | 5.642 | −11.469 | 22.753 | 0.519 | |
| Vision disorders | No | ref. | |||
| Yes | −6.497 | −15.22 | 2.226 | 0.147 | |
| BMQ: Overuse | 4.204 | 0.997 | 7.411 | 0.011 * | |
| BMQ: Harm | −0.001 | −3.223 | 3.222 | 1 | |
| BMQ: Necessity | 0.244 | −1.05 | 1.538 | 0.712 | |
| BMQ: Concerns | −1.365 | −2.866 | 0.136 | 0.077 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kołtuniuk, A.; Chojdak-Łukasiewicz, J. Beliefs about Medicines and the Level of Intentional Non-Adherence to Treatment among Patients with Multiple Sclerosis Treated with First-Line Drugs. J. Clin. Med. 2024, 13, 182. https://doi.org/10.3390/jcm13010182
Kołtuniuk A, Chojdak-Łukasiewicz J. Beliefs about Medicines and the Level of Intentional Non-Adherence to Treatment among Patients with Multiple Sclerosis Treated with First-Line Drugs. Journal of Clinical Medicine. 2024; 13(1):182. https://doi.org/10.3390/jcm13010182
Chicago/Turabian StyleKołtuniuk, Aleksandra, and Justyna Chojdak-Łukasiewicz. 2024. "Beliefs about Medicines and the Level of Intentional Non-Adherence to Treatment among Patients with Multiple Sclerosis Treated with First-Line Drugs" Journal of Clinical Medicine 13, no. 1: 182. https://doi.org/10.3390/jcm13010182
APA StyleKołtuniuk, A., & Chojdak-Łukasiewicz, J. (2024). Beliefs about Medicines and the Level of Intentional Non-Adherence to Treatment among Patients with Multiple Sclerosis Treated with First-Line Drugs. Journal of Clinical Medicine, 13(1), 182. https://doi.org/10.3390/jcm13010182