

Severe Refractory Vasoplegic Shock Syndrome after OPCABG Successfully Treated with Hydroxycobalamin: A Case Report and Review of the Literature

 , and
, and 
Abstract
1. Introduction
2. Relevant Sections
2.1. Case Report Description
2.2. Literature Review
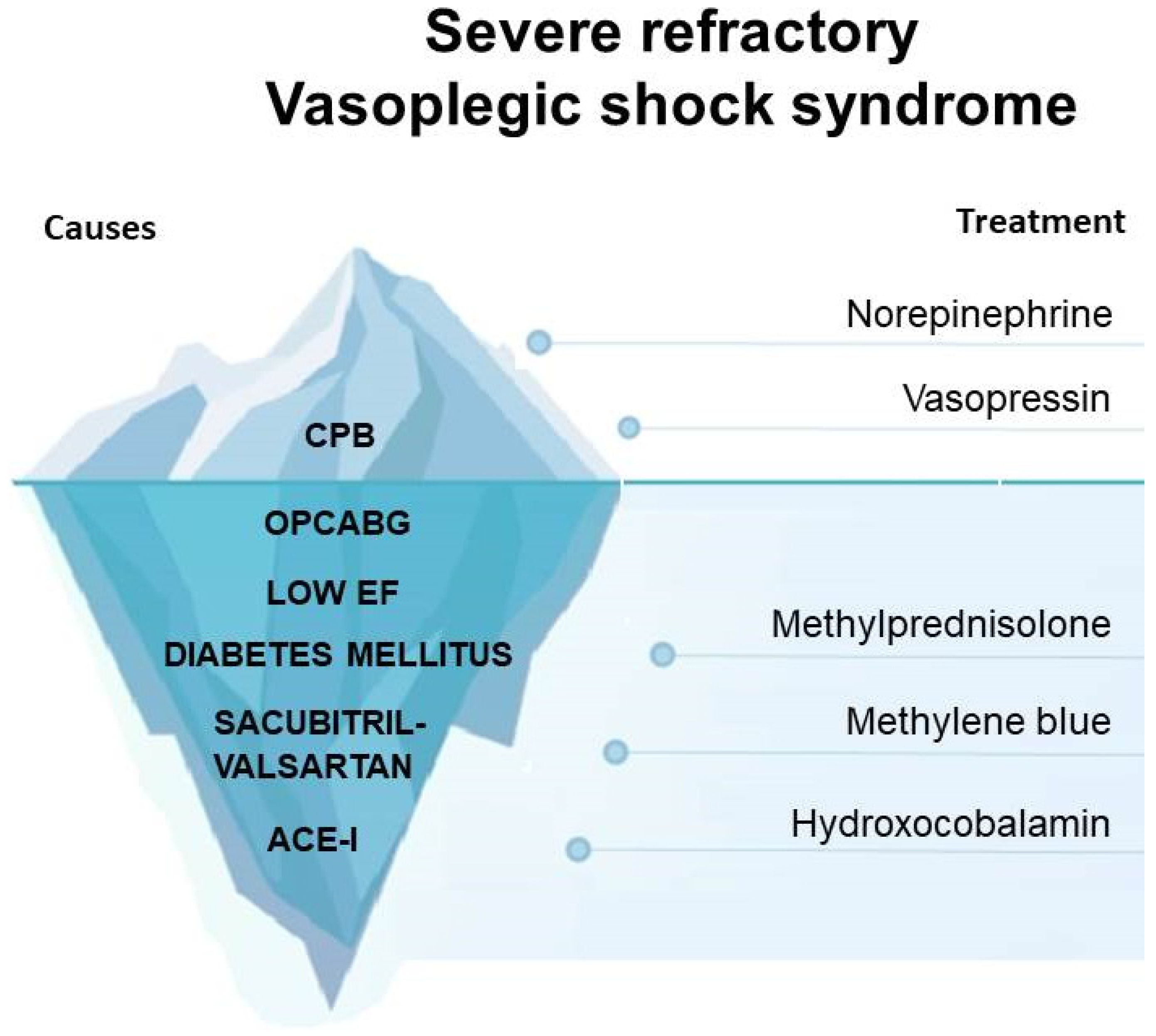
3. Discussion

{kind=link}
{kind=link}
| Study Author | Year of the Study | Type of the Study | Patients Included | Treatment |
|---|---|---|---|---|
| Sun et al. [3] | 2008 | comparative | 10 | - |
| Gomes et al. [16] | 2003 | retrospective | 4 | Norepinephrine |
| Raja et al. [20] | 2004 | case report | 1 | Norepinephrine and vasopressin |
| Vaidyanathan et al. | 2017 | case report | 1 | Norepinephrine and vasopressin |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ltaief, Z.; Ben-Hamouda, N.; Rancati, V.; Gunga, Z.; Marcucci, C.; Kirsch, M.; Liaudet, L. Vasoplegic Syndrome after Cardiopulmonary Bypass in Cardiovascular Surgery: Pathophysiology and Management in Critical Care. J. Clin. Med. 2022, 11, 6407. [Google Scholar] [CrossRef] [PubMed]
- Ortoleva, J.P.; Cobey, F.C. A systematic approach to the treatment of vasoplegia based on recent advances in pharmacotherapy. J. Cardiothorac. Vasc. Anesth. 2019, 33, 1310–1314. [Google Scholar] [CrossRef] [PubMed]
- Gomes, W.J.; Carvalho, A.C.; Palma, J.H.; Gonçalves, I., Jr.; Buffolo, E. Vasoplegic syndrome: A new dilemma. J. Thorac. Cardiovasc. Surg. 1994, 107, 942–943. [Google Scholar] [CrossRef] [PubMed]
- Levin, M.A.; Lin, H.M.; Castillo, J.G.; Adams, D.H.; Reich, D.L.; Fischer, G.W. Early on-cardiopulmonary bypass hypotension and other factors associated with vasoplegic syndrome. Circulation 2009, 120, 1664–1671. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Zhang, L.; Hill, P.C.; Lowery, R.; Lee, A.T.; Molyneaux, R.E.; Corso, P.J.; Boyce, S.W. Is incidence of postoperative vasoplegic syndrome different between off-pump and on-pump coronary artery bypass grafting surgery? Eur. J. Cardiothorac. Surg. 2008, 34, 820–825. [Google Scholar] [CrossRef] [PubMed]
- Burgdorff, A.M.; Bucher, M.; Schumann, J. Vasoplegia in patients with sepsis and septic shock: Pathways and mechanisms. J. Int. Med. Res. 2018, 46, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Busse, L.W.; Barker, N.; Petersen, C. Vasoplegic syndrome following cardiothoracic surgery-review of pathophysiology and update of treatment options. Crit. Care 2020, 24, 36. [Google Scholar] [CrossRef]
- Ni Choileain, N.; Redmond, H.P. Cell response to surgery. Ni Choileain, N.; Redmond HP. Arch. Surg. 2006, 141, 1132–1140. [Google Scholar] [CrossRef]
- Muhammad, R.; Dharmadjati, B.B.; Mulia, E.P.B.; Rachmi, D.A. Vasoplegia: Mechanism and Management Following Cardiopulmonary Bypass. Eurasian J. Med. 2022, 54, 92–99. [Google Scholar] [CrossRef]
- Papazisi, O.; Bruggemans, E.F.; Berendsen, R.R.; Hugo, J.D.V.; Lindeman, J.H.N.; Beeres, S.L.M.A.; Arbous, M.S.; van den Hout, W.B.; Mertens, B.J.A.; Ince, C.; et al. Prevention of vasoplegia with CytoSorb in heart failure patients undergoing cardiac surgery (CytoSorb-HF trial): Protocol for a randomised controlled trial. BMJ Open 2022, 12, e061337. [Google Scholar] [CrossRef]
- Haider, L.; Hugon-Vallet, E.; Constantin, J.P.; Riad, Z.; Sebbag, L.; Mewton, N. ARNI Pre-Operative Use and Vasoplegic Syndrome in Patients Undergoing Heart Transplantation or Left Ventricular Assist Device Surgery. Med. Sci. 2021, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Almufleh, A.; Mielniczuk, L.M.; Zinoviev, R.; Moeller, A.; Davies, R.A.; Stadnick, E.; Chan, V.; Chih, S. Profound Vasoplegia During Sacubitril/Valsartan Treatment After Heart Transplantation. Can. J. Cardiol. 2018, 34, 343.e5–343.e7. [Google Scholar] [CrossRef] [PubMed]
- Domínguez, J.M.; García-Romero, E.; Pàmies, J.; Mirabet, S.; González-Costello, J.; Spitaleri, G.; Perez-Villa, F.; Farrero, M. Incidence of vasoplegic syndrome after cardiac transplantation in patients treated with sacubitril/valsartan. Clin. Transplant. 2020, 34, e13994. [Google Scholar] [CrossRef]
- Kobalava, Z.; Kotovskaya, Y.; Averkov, O.; Pavlikova, E.; Moiseev, V.; Albrecht, D.; Chandra, P.; Ayalasomayajula, S.; Prescott, M.F.; Pal, P.; et al. Pharmacodynamic and Pharmacokinetic Profiles of Sacubitril/Valsartan (LCZ696) in Patients with Heart Failure and Reduced Ejection Fraction. Cardiovasc. Ther. 2016, 34, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Ozal, E.; Kuralay, E.; Yildirim, V.; Kilic, S.; Bolcal, C.; Kücükarslan, N.; Günay, C.; Demirkilic, U.; Tatar, H. Preoperative methylene blue administration in patients at high risk for vasoplegic syndrome during cardiac surgery. Ann. Thorac. Surg. 2005, 79, 1615–1619. [Google Scholar] [CrossRef] [PubMed]
- Gomes, W.J.; Erlichman, M.R.; Batista-Filho, M.L.; Knobel, M.; Almeida, D.R.; Carvalho, A.C.; Catani, R.; Buffolo, E. Vasoplegic syndrome after off-pump coronary artery bypass surgery. Eur. J. Cardiothorac. Surg. 2003, 23, 165–169. [Google Scholar] [CrossRef][Green Version]
- Andrei, S.; Bar, S.; Nguyen, M.; Bouhemad, B.; Guinot, P.G. Effect of norepinephrine on the vascular waterfall and tissue perfusion in vasoplegic hypotensive patients: A prospective, observational, applied physiology study in cardiac surgery. Intensive Care Med. Exp. 2023, 11, 52. [Google Scholar] [CrossRef]
- Hajjar, L.A.; Vincent, J.L.; Barbosa Gomes Galas, F.R.; Rhodes, A.; Landoni, G.; Osawa, E.A.; Melo, R.R.; Sundin, M.R.; Grande, S.M.; Gaiotto, F.A.; et al. Vasopressin versus Norepinephrine in Patients with Vasoplegic Shock after Cardiac Surgery: The VANCS Randomized Controlled Trial. Anesthesiology 2017, 126, 85–93. [Google Scholar] [CrossRef]
- Hartmann, C.; Radermacher, P.; Wepler, M.; Nussbaum, B. Non-Hemodynamic Effects of Catecholamines. Shock 2017, 48, 390–400. [Google Scholar] [CrossRef]
- Raja, S.G.; Dreyfus, G.D. Vasoplegic syndrome after off-pump coronary artery bypass surgery: An unusual complication. Tex. Heart Inst. J. 2004, 31, 421–424. [Google Scholar]
- Omar, S.; Zedan, A.; Nugent, K. Cardiac vasoplegia syndrome: Pathophysiology, risk factors and treatment. Am. J. Med. Sci. 2015, 349, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Papazisi, O.; Palmen, M.; Danser, A.H. The use of angiotensin II for the treatment of post-cardiopulmonary bypass vasoplegia. Cardiovasc. Drugs Ther. 2022, 36, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.; English, S.W.; Wang, X.S.; Ham, K.; Tumlin, J.; Szerlip, H.; Busse, L.W.; Altaweel, L.; Albertson, T.E.; Mackey, C.; et al. Angiotensin II for the treatment of vasodilatory shock. N. Engl. J. Med. 2017, 377, 419430. [Google Scholar] [CrossRef] [PubMed]
- Bellissant, E.; Annane, D. Effect of hydrocortisoneon phenylephrine mean arterial pressure dose-response relationship in septic shock. Clin. Pharmacol. Ther. 2000, 68, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.M.; Makheja, A.N.; Pash, J.; Verma, M. Corticosteroids suppress cyclooxygenase messenger RNA levels and prostanoid synthesis in cultured vascular cells. Biochem. Biophys. Res. Commun. 1988, 157, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Marik, E.; Khangoora, V.; Rivera, R.; Hooper, M.H.; Catravas, J. Hydrocortisone, vitamin C, and thiamine for the treatment of severe sepsis and septic shock: A retrospective before-after study. Chest 2017, 151, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Biston, P.; Devriendt, J.; Madl, C.; Chochrad, D.; Aldecoa, C.; Brasseur, A.; Defrance, P.; Gottignies, P.; Vincent, J.L.; et al. Comparison of dopamine and norepinephrine in the treatment of shock. N. Engl. J. Med. 2010, 362, 779–789. [Google Scholar] [CrossRef]
- Abril, M.K.; Khanna, A.K.; Kroll, S.; Mc Namara, C.; Handisides, D.; Busse, L.W. Regional differences in the treatment of refractory vasodilatory shock using angiotensin II in high output shock (ATHOS-3) data. J. Crit. Care 2019, 50, 188–194. [Google Scholar] [CrossRef]
- Shah, R.; Wenger, R.K.; Patel, P.A.; Davis, S.; Ha, B.; Feinman, J.W.; Patel, S.; Pulton, D.; Weiss, S.J.; Restrepo-Cardenas, J.; et al. Severe Vasoplegic Shock During Coronary Artery Bypass Surgery: Therapeutic challenges and Dilemmas in Hemodynamic Rescue. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1341–1347. [Google Scholar] [CrossRef]
- Wieruszewski, P.M.; Khanna, A.K. Vasopressor Choice and Timing in Vasodilatory Shock. Crit. Care 2022, 26, 76. [Google Scholar] [CrossRef]
- Oz, M.; Lorke, D.E.; Hasan, M.; Petroianu, G.A. Cellular and molecular actions of Methylene Blue in the nervous system. Med. Res. Rev. 2011, 31, 93–117. [Google Scholar] [CrossRef] [PubMed]
- Roderique, J.D.; VanDyck, K.; Holman, B.; Tang, D.; Chui, B.; Spiess, B.D. The use of high-dose hydroxycobalamin for vasoplegic syndrome. Ann. Thorac. Surg. 2014, 97, 1785–1786. [Google Scholar] [CrossRef] [PubMed]
- Charles, F.G.; Murray, L.J.; Giordano, C.; Spiess, B.D. Vitamin B12 for the treatment of vasoplegia in cardiac surgery and liver transplantation: A narrative review of cases and potential biochemical mechanisms. Can. J. Anaesth. 2019, 66, 1501–1513. [Google Scholar] [CrossRef] [PubMed]
- Seelhammer, T.G.; Plack, D.; Nei, S.; Wittwer, E.; Nelson, J.; Nabzdyk, C.G. Extended duration infusion of high-dose hydroxocobalamin for vasoplegic syndrome following cardiac surgery. Heart Lung 2021, 50, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Levin, R.L.; Degrange, M.A.; Bruno, G.F.; Del Mazo, C.D.; Taborda, D.J.; Griotti, J.J.; Boullon, F.J. Methylene blue reduces mortality and morbidity in vasoplegic patients after cardiac surgery. Ann. Thorac. Surg. 2004, 77, 496–499. [Google Scholar] [CrossRef]
- Shah, P.; Reynolds, P.; Pal, N. Hydroxocobalamin for the treatment of cardiac-associated vasoplegia: A case series. Can. J. Anaesth. 2018, 65, 560–568. [Google Scholar]
- Shapeton, A.D.; Mahmood, F.; Ortoleva, J.P. Hydroxocobalamin for the Treatment of Vasoplegia: A Review of Current Literature and Considerations for Use. J. Cardiothorac. Vasc. Anesth. 2019, 33, 894–901. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bacchi, B.; Cabrucci, F.; Chiarello, B.; Dokollari, A.; Bonacchi, M. Severe Refractory Vasoplegic Shock Syndrome after OPCABG Successfully Treated with Hydroxycobalamin: A Case Report and Review of the Literature. J. Clin. Med. 2024, 13, 169. https://doi.org/10.3390/jcm13010169
Bacchi B, Cabrucci F, Chiarello B, Dokollari A, Bonacchi M. Severe Refractory Vasoplegic Shock Syndrome after OPCABG Successfully Treated with Hydroxycobalamin: A Case Report and Review of the Literature. Journal of Clinical Medicine. 2024; 13(1):169. https://doi.org/10.3390/jcm13010169
Chicago/Turabian StyleBacchi, Beatrice, Francesco Cabrucci, Bruno Chiarello, Aleksander Dokollari, and Massimo Bonacchi. 2024. "Severe Refractory Vasoplegic Shock Syndrome after OPCABG Successfully Treated with Hydroxycobalamin: A Case Report and Review of the Literature" Journal of Clinical Medicine 13, no. 1: 169. https://doi.org/10.3390/jcm13010169
APA StyleBacchi, B., Cabrucci, F., Chiarello, B., Dokollari, A., & Bonacchi, M. (2024). Severe Refractory Vasoplegic Shock Syndrome after OPCABG Successfully Treated with Hydroxycobalamin: A Case Report and Review of the Literature. Journal of Clinical Medicine, 13(1), 169. https://doi.org/10.3390/jcm13010169