
The Management of Postoperative Recurrence in Crohn’s Disease


 ,
,
Abstract
:1. Introduction
2. Methods
3. Monitoring
3.1. Endoscopy

{kind=link}
{kind=link}
| Score | Endoscopic Findings | |
|---|---|---|
| Endoscopic Postoperative Remission | i0 | no lesions |
| i1 | ≤5 aphthous ulcers | |
| Endoscopic Postoperative Recurrence | i2 | >5 aphthous ulcers with normal mucosa in-between or large lesions limited to anastomosis |
| i2a (mRS) | lesions limited to the ileocolonic anastomosis (with/without anastomotic stenosis) | |
| i2b (mRS) | >5 aphthous ulcers or larger lesions with normal mucosa in-between the neoterminal ileum (with/without anastomotic stenosis) | |
| i3 | aphthous ileitis with diffusely inflamed mucosa | |
| i4 | diffuse inflammation with large ulcers, nodules and/or strictures |
3.2. Cross-Sectional Image
3.3. Biomarkers
3.3.1. Fecal Calprotectin
3.3.2. Serum Biomarkers
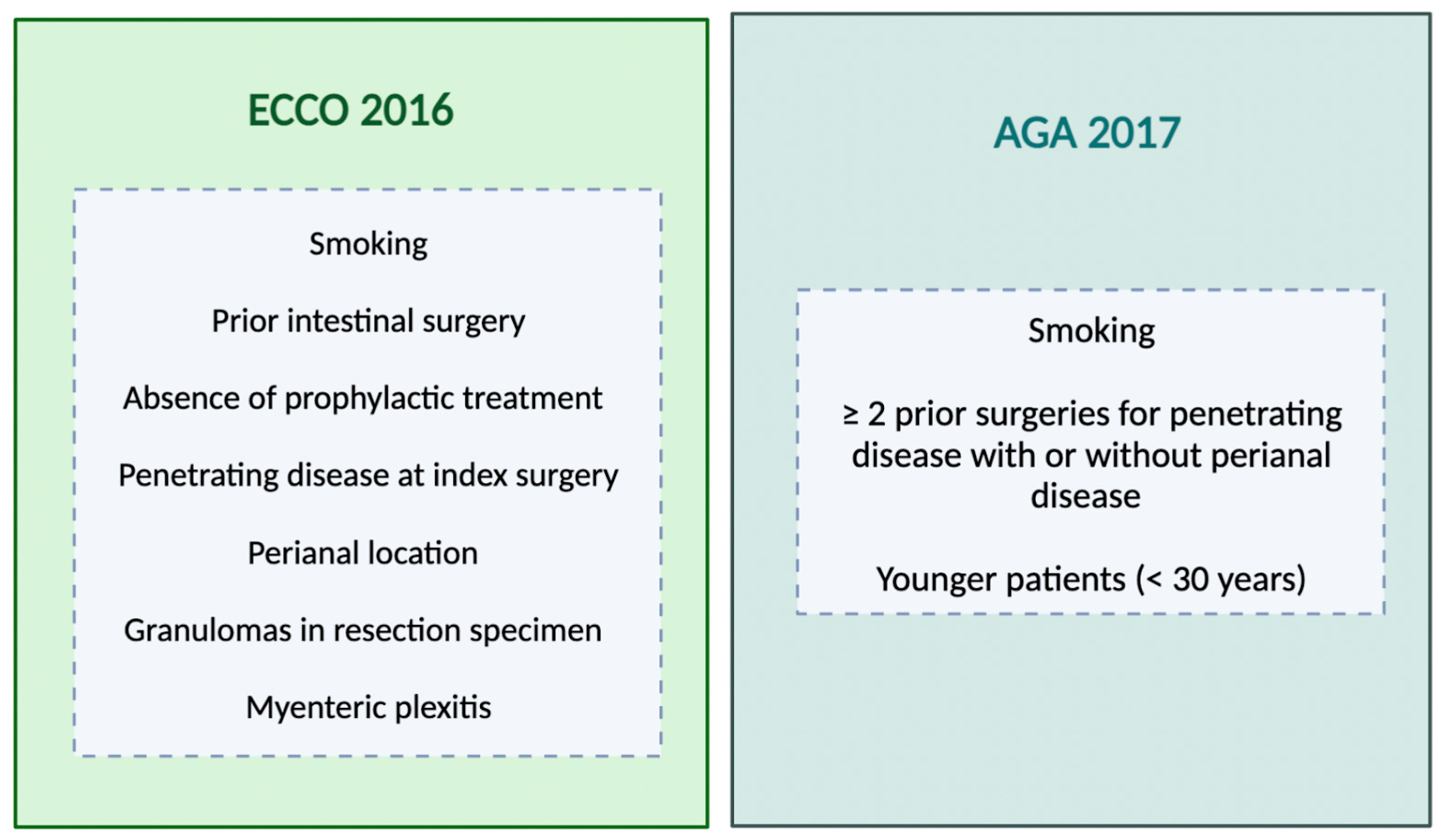
4. Risk Factors for Postoperative Recurrence
5. Prophylaxis of Postoperative Recurrence
5.1. Antibiotics
5.2. Mesalazine
5.3. Corticosteroids
5.4. Immunomodulators
5.5. Anti-Tumor Necrosis Factor
5.6. Vedolizumab and Ustekinumab
| Authors | Drug | Study Design | Population | AGE | Sex (M/F) | Risk Factors | Outcomes | Results |
|---|---|---|---|---|---|---|---|---|
| Herfarth et al. (2013) [92] | Ciprofloxacin vs. placebo | RCT | 33 patients | 30 (18–70) | 18/15 | Smo = 12% nR = 18% Str = 54% | Endoscopic POR 6 months (65% vs. 69%, p < 0.805) | Ineffective |
| Rutgeerts et al. (2005) [91] | Ornidazole vs. placebo | RCT | 78 patients | 33 (18–70) | 42/16 | Smo = 17% nR = 24% Str = 18% | Clinical POR 1 year (8% vs. 38%, p = 0.046); Endoscopic POR 1 year (79% vs. 54%, p = 0.037) | Effective |
| Rutgeerts et al. (1995) [90] | Metronidazole vs. placebo | RCT | 60 patients | 25 | NA | nR = 41% Str = 58% | Endoscopic POR 3 months (52% vs. 75%, p = 0.09); Histological POR 3 months (17% vs. 54%, p = 0.008) | Effective |
| Hellers et al. (1999) [95] | Budesonide 6 mg/d vs. placebo | RCT | 129 patients | 35 (17–81) | 62/67 | nR = 28% | Endoscopic POR 3 months (52% vs. 31%, p = NA); Endoscopic POR 12 months (58% vs. 52%, p = NA) | Ineffective |
| Ewe et al. (1999) [96] | Budesonide 3 mg/3 d vs. placebo | RCT | 62 patients | 34 (23–47) | 37/46 | nR = 62% | Clinical and/or endoscopic POR 1 year 1 (57% vs. 70%) | Ineffective |
| NA | MTX | NA | NA | NA | NA | NA | NA | No data |
| Gjuladin-Hellon et al. (2019) [102] | Thiopurines vs. placebo | Meta-analysis 3 studies | 408 patients | NA | NA | NA | Reduction endoscopic POR 12–36 months (67% vs. 75%, RR 0.85, 95% CI 0.64–1.13); Reduction clinical POR 12–36 months (51% vs. 64%, RR 0.79, 95% CI 0.67–0.92) | Effective |
| Peyrin-Biroulet et al. (2009) [101] | Thiopurines vs. placebo/ metronidazole/ 5-ASA | Meta-analysis 4 studies | 433 patients | NA | NA | NA | Reduction endoscopic POR (mean difference 15%, 95% CI 1.8–29%, p = 0.026); Reduction clinical POR (mean difference 8%, 95% CI: 1–15%, p = 0.021) | Effective |
| Reguiero et al. (2016) [103] | IFX vs. placebo | RCT | 297 patients | 36 (18–73) | 158/139 | nR = 42% Str = 57% | Clinical POR 76 weeks (12.9% vs. 20%, p = 0.097); endoscopic POR 76 weeks (30.6% vs. 60%, p < 0.002) | Effective |
| De Cruz et al. (2015) [13] | Metronidazole+ Thiopurines/ ADA vs. Metronidazole | RCT | 118 patients | 36 (26–47) | 19/33 | Smo = 31% nR = 31% Str = 40% | Endoscopic POR 6 months (52% vs. 75%, p = 0.03) | Effective |
| Buisson et al. (2021) [118] | UST vs. AZA | Observational Retrospective | 63 patients UST (32); AZA (31) | 37 | 15/48 | Smo = 38% | Endoscopic POR 6 months (28% vs. 54.5%, p = 0.029) | Uncertain |
| Yanai et al. (2022) [116] | UST/VDZ vs. Anti-TNF | Observational Retrospective | 297 patients UST (34)/VDZ (39) vs. anti-TNF (224) | 24 (IQR 19–32) | 166/131 | Smo = 36% nR = 2% Str = 64% | Endoscopic POR 1 year 41.8%; UST and anti-TNF (OR 1.86, 95% CI 0.79–4.38) | Uncertain |
| Mañosa et al. (2022) [117] | UST | Observational Retrospective | 40 patients | 34 (24–55) | 25/15 | Smo = 22% nR = 42% Str = 37% | Clinical POR 12 months in 32%; Endoscopic POR 18 months in 42% | Uncertain |
| Yamada et al. (2018) [119] | VDZ vs. anti-TNF | Observational Retrospective | 80 patients VDZ (22); anti-TNF (58) | 33 | 38/42 | Smo = 12% Str = 42% | Endoscopic remission 6–12 months (25% vs. 66%, p = 0.01) | Uncertain |
| Mañosa et al. (2022) [117] | VDZ | Observational Retrospective | 25 patients | 38 (31–62) | 15/10 | Smo = 16% nR = 40% Str = 52% | Clinical POR 12 months in 30%; endoscopic POR 18 months in 40% | Uncertain |
6. Medical Treatment of Postoperative Recurrence
6.1. Antibiotics
6.2. Mesalazine
6.3. Corticosteroids
6.4. Immunomodulators
6.5. Anti-Tumor Necrosis Factor
6.6. Ustekinumab
6.7. Vedolizumab
| Authors | Drug | Study Design | Population | AGE | Sex (M/F) | Risk Factors | Outcomes | Results |
|---|---|---|---|---|---|---|---|---|
| NA | ANTIBIOTICS | NA | NA | NA | NA | NA | NA | No data |
| NA | STEROIDS | NA | NA | NA | NA | NA | NA | No data |
| NA | MTX | NA | NA | NA | NA | NA | NA | No data |
| Reinisch et al. (2010) [122] | 5-ASA vs. AZA | RCT | 78 endoscopic POR | 35 (17–81) | 62/67 | nR = 28% | Treatment failure at 1 year (11% vs. 22%, p = 0.19); endoscopic improvement (34.4% vs. 63.3%, p = 0.023); clinical POR more often with mesalazine | Uncertain |
| Orlando et al. (2020) [123] | 5-ASA vs. AZA | RCT | 48 endoscopic POR | 34 (23–47) | 30/36 | Smo = 43% Str = 87% | Treatment failure at 1 year (21% vs. 14%, p = 0.7); endoscopic improvement (8.3% vs. 36.4%, p = 0.035); clinical POR more often with mesalazine | Uncertain |
| Carla-Moreau et al. (2015) [105] | IFX vs. AZA/5-ASA | Meta-analysis | 50 endoscopic POR | 36 | NA | NA | IFX is more effective for endoscopic POR (OR 16.6; 95% CI 2.5–110.2) | >> IFX |
| Cañete et al. 2020 [129] | IFX or ADA | Retrospective cohort | 83 IFX, 96 ADA | NA | 98/81 | Smo = 49% Str = 44% | Endoscopic improvement in 61%; Endoscopic remission in 42%; Thiopurines + IFX >> ADA | Effective |
| Tursi et al. (2021) [131] | UST | Retrospective case-series | 15 clinical and endoscopic cohort | 42 (37–52) | 9/6 | Smo = 13% | Endoscopic remission (11/11); Clinical remission 6 months (12/15) | Uncertain |
| Macaluso et al. (2023) [132] | UST | Retrospective cohort | 44 endoscopic POR | 47.3 (±15.0) | 18/26 | Smo = 42% Str = 84% nR = 6.8% | Endoscopic improvement in 50%; Endoscopic remission in 27%; No endoscopic response in 27% | Uncertain |
| Macaluso et al. (2022) [134] | VDZ | Retrospective cohort | 58 endoscopic POR | 36 (18–73) | 158/139 | nR = 42% Str = 57% | Endoscopic improvement 16 months in 48%; clinical failure 1 year in 19%; new surgery in 12% | Uncertain |
6.8. Non-Pharmacological Treatment
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peyrin-Biroulet, L.; Cieza, A.; Sandborn, W.J.; Coenen, M.; Chowers, Y.; Hibi, T.; Kostanjsek, N.; Stucki, G.; Colombel, J.-F.; the International Programme to Develop New Indexes for Crohn’s Disease (IPNIC) group. Development of the First Disability Index for Inflammatory Bowel Disease Based on the International Classification of Functioning, Disability and Health. Gut 2012, 61, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Fiorino, G.; Peyrin-Biroulet, L. Early Intervention in Crohn’s Disease: Towards Disease Modification Trials. Gut 2017, 66, 2179–2187. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s Disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, F.; Peyrin-Biroulet, L.; Danese, S.; Fiorino, G. New Drugs in the Pipeline for the Treatment of Inflammatory Bowel Diseases: What Is Coming? Curr. Opin. Pharmacol. 2020, 55, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Peyrin-Biroulet, L.; Loftus, E.V.; Colombel, J.-F.; Sandborn, W.J. The Natural History of Adult Crohn’s Disease in Population-Based Cohorts. Am. J. Gastroenterol. 2010, 105, 289–297. [Google Scholar] [CrossRef]
- Roda, G.; Chien Ng, S.; Kotze, P.G.; Argollo, M.; Panaccione, R.; Spinelli, A.; Kaser, A.; Peyrin-Biroulet, L.; Danese, S. Crohn’s Disease. Nat. Rev. Dis. Primers 2020, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Bemelman, W.A.; Warusavitarne, J.; Sampietro, G.M.; Serclova, Z.; Zmora, O.; Luglio, G.; de Buck van Overstraeten, A.; Burke, J.P.; Buskens, C.J.; Francesco, C.; et al. ECCO-ESCP Consensus on Surgery for Crohn’s Disease. J. Crohns Colitis 2017, 12, 1–16. [Google Scholar] [CrossRef]
- Frolkis, A.D.; Lipton, D.S.; Fiest, K.M.; Negrón, M.E.; Dykeman, J.; deBruyn, J.; Jette, N.; Frolkis, T.; Rezaie, A.; Seow, C.H.; et al. Cumulative Incidence of Second Intestinal Resection in Crohn’s Disease: A Systematic Review and Meta-Analysis of Population-Based Studies. Am. J. Gastroenterol. 2014, 109, 1739–1748. [Google Scholar] [CrossRef]
- Burr, N.E.; Lord, R.; Hull, M.A.; Subramanian, V. Decreasing Risk of First and Subsequent Surgeries in Patients With Crohn’s Disease in England From 1994 through 2013. Clin. Gastroenterol. Hepatol. 2019, 17, 2042–2049.e4. [Google Scholar] [CrossRef]
- Beelen, E.M.J.; van der Woude, C.J.; Pierik, M.J.; Hoentjen, F.; de Boer, N.K.; Oldenburg, B.; van der Meulen, A.E.; Ponsioen, C.I.J.; Dijkstra, G.; Bruggink, A.H.; et al. Decreasing Trends in Intestinal Resection and Re-Resection in Crohn’s Disease: A Nationwide Cohort Study. Ann. Surg. 2021, 273, 557–563. [Google Scholar] [CrossRef]
- Kalman, T.D.; Everhov, Å.H.; Nordenvall, C.; Sachs, M.C.; Halfvarson, J.; Ekbom, A.; Ludvigsson, J.F.; Myrelid, P.; Olén, O. Decrease in Primary but Not in Secondary Abdominal Surgery for Crohn’s Disease: Nationwide Cohort Study, 1990–2014. Br. J. Surg. 2020, 107, 1529–1538. [Google Scholar] [CrossRef] [PubMed]
- Nones, R.B.; Fleshner, P.R.; Queiroz, N.S.F.; Cheifetz, A.S.; Spinelli, A.; Danese, S.; Peyrin-Biroulet, L.; Papamichael, K.; Kotze, P.G. Therapeutic Drug Monitoring of Biologics in IBD: Essentials for the Surgical Patient. J. Clin. Med. 2021, 10, 5642. [Google Scholar] [CrossRef] [PubMed]
- De Cruz, P.; Kamm, M.A.; Hamilton, A.L.; Ritchie, K.J.; Krejany, E.O.; Gorelik, A.; Liew, D.; Prideaux, L.; Lawrance, I.C.; Andrews, J.M.; et al. Crohn’s Disease Management after Intestinal Resection: A Randomised Trial. Lancet 2015, 385, 1406–1417. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, A.; Sacchi, M.; Fiorino, G.; Danese, S.; Montorsi, M. Risk of Postoperative Recurrence and Postoperative Management of Crohn’s Disease. World J. Gastroenterol. 2011, 17, 3213–3219. [Google Scholar] [PubMed]
- Dragoni, G.; Allocca, M.; Myrelid, P.; Noor, N.M.; Hammoudi, N.; the 8 th Scientific Workshop of the European Crohn’s and Colitis Organisation; Rivière, P.; Panis, Y.; Ferrante, M. Results of the Eighth Scientific Workshop of ECCO: Diagnosing Postoperative Recurrence of Crohn’s Disease after an Ileocolonic Resection with Ileocolonic Anastomosis. J. Crohns Colitis 2023, 17, 1373–1386. [Google Scholar] [CrossRef]
- Vespa, E.; Furfaro, F.; Allocca, M.; Fiorino, G.; Correale, C.; Gilardi, D.; Argollo, M.; Zilli, A.; Zacharopoulou, E.; Loy, L.; et al. Endoscopy after Surgery in Inflammatory Bowel Disease: Crohn’s Disease Recurrence and Pouch Surveillance. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 829–841. [Google Scholar] [CrossRef]
- Khanna, R.; Ma, C.; Jairath, V.; Vande Casteele, N.; Zou, G.; Feagan, B.G. Endoscopic Assessment of Inflammatory Bowel Disease Activity in Clinical Trials. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2022, 20, 727–736.e2. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Geboes, K.; Vantrappen, G.; Beyls, J.; Kerremans, R.; Hiele, M. Predictability of the Postoperative Course of Crohn’s Disease. Gastroenterology 1990, 99, 956–963. [Google Scholar] [CrossRef]
- Yamamoto, T.; Bamba, T.; Umegae, S.; Matsumoto, K. The Impact of Early Endoscopic Lesions on the Clinical Course of Patients Following Ileocolonic Resection for Crohn’s Disease: A 5-year Prospective Cohort Study. United Eur. Gastroenterol. J. 2013, 1, 294–298. [Google Scholar] [CrossRef]
- Ble, A.; Renzulli, C.; Cenci, F.; Grimaldi, M.; Barone, M.; Sedano, R.; Chang, J.; Nguyen, T.M.; Hogan, M.; Zou, G.; et al. The Relationship Between Endoscopic and Clinical Recurrence in Postoperative Crohn’s Disease: A Systematic Review and Meta-Analysis. J. Crohns Colitis 2022, 16, 490–499. [Google Scholar] [CrossRef]
- Marteau, P.; Laharie, D.; Colombel, J.-F.; Martin, L.; Coevoet, H.; Allez, M.; Cadiot, G.; Bourreille, A.; Carbonnel, F.; Bouhnik, Y.; et al. Interobserver Variation Study of the Rutgeerts Score to Assess Endoscopic Recurrence after Surgery for Crohn’s Disease. J. Crohns Colitis 2016, 10, 1001–1005. [Google Scholar] [CrossRef] [PubMed]
- Domènech, E.; Mañosa, M.; Bernal, I.; Garcia-Planella, E.; Cabré, E.; Piñol, M.; Lorenzo-Zúñiga, V.; Boix, J.; Gassull, M.A. Impact of Azathioprine on the Prevention of Postoperative Crohn’s Disease Recurrence: Results of a Prospective, Observational, Long-Term Follow-up Study. Inflamm. Bowel Dis. 2008, 14, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Rivière, P.; Pekow, J.; Hammoudi, N.; Wils, P.; De Cruz, P.; Wang, C.P.; Mañosa, M.; Ollech, J.; Allez, M.; Nachury, M.; et al. Comparison of the Risk of Crohn’s Disease Postoperative Recurrence Between Modified Rutgeerts Score I2a and I2b Categories: An Individual Patient Data Meta-Analysis. J. Crohns Colitis 2023, 17, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Gecse, K.; Lowenberg, M.; Bossuyt, P.; Rutgeerts, P.J.; Vermeire, S.; Stitt, L.; Vandervoort, M.K.; Sandborn, W.; Feagan, B.G.; Samaan, M.A.; et al. Sa1198 Agreement Among Experts in the Endoscopic Evaluation of Postoperative Recurrence in Crohn’s Disease Using the Rutgeerts Score. Gastroenterology 2014, 146, S-227. [Google Scholar] [CrossRef]
- Rivière, P.; Vermeire, S.; Irles-Depe, M.; Van Assche, G.; Rutgeerts, P.; De Buck Van Overstraeten, A.; Denost, Q.; Wolthuis, A.; D’Hoore, A.; Laharie, D.; et al. No Change in Determining Crohn’s Disease Recurrence or Need for Endoscopic or Surgical Intervention With Modification of the Rutgeerts’ Scoring System. Clin. Gastroenterol. Hepatol. 2019, 17, 1643–1645. [Google Scholar] [CrossRef] [PubMed]
- Ollech, J.E.; Aharoni-Golan, M.; Weisshof, R.; Normatov, I.; Sapp, A.R.; Kalakonda, A.; Israel, A.; Glick, L.R.; Karrison, T.; Dalal, S.R.; et al. Differential Risk of Disease Progression between Isolated Anastomotic Ulcers and Mild Ileal Recurrence after Ileocolonic Resection in Patients with Crohn’s Disease. Gastrointest. Endosc. 2019, 90, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Hammoudi, N.; Auzolle, C.; Tran Minh, M.-L.; Boschetti, G.; Bezault, M.; Buisson, A.; Pariente, B.; Treton, X.; Seksik, P.; Fumery, M.; et al. Postoperative Endoscopic Recurrence on the Neoterminal Ileum But Not on the Anastomosis Is Mainly Driving Long-Term Outcomes in Crohn’s Disease. Am. J. Gastroenterol. 2020, 115, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Bislenghi, G.; Vancoillie, P.-J.; Fieuws, S.; Verstockt, B.; Sabino, J.; Wolthuis, A.; D’Hoore, A. Effect of Anastomotic Configuration on Crohn’s Disease Recurrence after Primary Ileocolic Resection: A Comparative Monocentric Study of End-to-End versus Side-to-Side Anastomosis. Updat. Surg. 2023, 75, 1607–1615. [Google Scholar] [CrossRef]
- Gajendran, M.; Bauer, A.J.; Buchholz, B.M.; Watson, A.R.; Koutroubakis, I.E.; Hashash, J.G.; Ramos-Rivers, C.; Shah, N.; Lee, K.K.; Cruz, R.J.; et al. Ileocecal Anastomosis Type Significantly Influences Long-Term Functional Status, Quality of Life, and Healthcare Utilization in Postoperative Crohn’s Disease Patients Independent of Inflammation Recurrence. Am. J. Gastroenterol. 2018, 113, 576–583. [Google Scholar] [CrossRef]
- Kann, B.R. Anastomotic Considerations in Crohn’s Disease. Clin. Colon Rectal Surg. 2023, 36, 63–73. [Google Scholar] [CrossRef]
- Kavalukas, S.L.; Scheurlen, K.M.; Galandiuk, S. State-of-the-Art Surgery for Crohn’s Disease: Part I-Small Intestine/Ileal Disease. Langenbecks Arch. Surg. 2022, 407, 885–895. [Google Scholar] [CrossRef] [PubMed]
- Schmoyer, C.J.; Saidman, J.; Bohl, J.L.; Bierly, C.L.; Kuemmerle, J.F.; Bickston, S.J. The Pathogenesis and Clinical Management of Stricturing Crohn Disease. Inflamm. Bowel Dis. 2021, 27, 1839–1852. [Google Scholar] [CrossRef] [PubMed]
- Nardone, O.M.; Calabrese, G.; Barberio, B.; Giglio, M.C.; Castiglione, F.; Luglio, G.; Savarino, E.; Ghosh, S.; Iacucci, M. Rates of Endoscopic Recurrence In Postoperative Crohn’s Disease Based on Anastomotic Techniques: A Systematic Review And Meta-Analysis. Inflamm. Bowel Dis. 2023, izad252. [Google Scholar] [CrossRef]
- Scheurlen, K.M.; Parks, M.A.; Macleod, A.; Galandiuk, S. Unmet Challenges in Patients with Crohn’s Disease. J. Clin. Med. 2023, 12, 5595. [Google Scholar] [CrossRef] [PubMed]
- Rivière, P.; Bislenghi, G.; Vermeire, S.; Domènech, E.; Peyrin-Biroulet, L.; Laharie, D.; D’Hoore, A.; Ferrante, M. Postoperative Crohn’s Disease Recurrence: Time to Adapt Endoscopic Recurrence Scores to the Leading Surgical Techniques. Clin. Gastroenterol. Hepatol. 2022, 20, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- De Cruz, P.; Bernardi, M.-P.; Kamm, M.A.; Allen, P.B.; Prideaux, L.; Williams, J.; Johnston, M.J.; Keck, J.; Brouwer, R.; Heriot, A.; et al. Postoperative Recurrence of Crohn’s Disease: Impact of Endoscopic Monitoring and Treatment Step-up. Colorectal Dis. 2013, 15, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.C.; Loftus, E.V.; Hirano, I.; Falck–Ytter, Y.; Singh, S.; Sultan, S.; Flamm, S.L.; Lim, J.K.; Rubenstein, J.H.; Smalley, W.E.; et al. American Gastroenterological Association Institute Guideline on the Management of Crohn’s Disease after Surgical Resection. Gastroenterology 2017, 152, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, G.R.; Loftus, E.V.; Isaacs, K.L.; Regueiro, M.D.; Gerson, L.B.; Sands, B.E. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am. J. Gastroenterol. 2018, 113, 481–517. [Google Scholar] [CrossRef]
- Pouillon, L.; Remen, T.; Amicone, C.; Louis, E.; Maes, S.; Reenaers, C.; Germain, A.; Baumann, C.; Bossuyt, P.; Peyrin-Biroulet, L. Risk of Late Postoperative Recurrence of Crohn’s Disease in Patients in Endoscopic Remission After Ileocecal Resection, over 10 Years at Multiple Centers. Clin. Gastroenterol. Hepatol. 2021, 19, 1218–1225.e4. [Google Scholar] [CrossRef]
- Shen, B.; Kochhar, G.S.; Navaneethan, U.; Cross, R.K.; Farraye, F.A.; Iacucci, M.; Schwartz, D.A.; Gonzalez-Lama, Y.; Schairer, J.; Kiran, R.P.; et al. Endoscopic Evaluation of Surgically Altered Bowel in Inflammatory Bowel Disease: A Consensus Guideline from the Global Interventional Inflammatory Bowel Disease Group. Lancet Gastroenterol. Hepatol. 2021, 6, 482–497. [Google Scholar] [CrossRef]
- Domènech, E.; López-Sanromán, A.; Nos, P.; Vera, M.; Chaparro, M.; Esteve, M.; Gisbert, J.P.; Mañosa, M. Recomendaciones del Grupo Español de Trabajo en Enfermedad de Crohn y Colitis Ulcerosa (GETECCU) sobre la monitorización, prevención y tratamiento de la recurrencia posquirúrgica en la enfermedad de Crohn. Gastroenterol. Hepatol. 2017, 40, 472–483. [Google Scholar] [CrossRef]
- Allocca, M.; Dal Buono, A.; D’Alessio, S.; Spaggiari, P.; Garlatti, V.; Spinelli, A.; Faita, F.; Danese, S. Relationships Between Intestinal Ultrasound Parameters and Histopathologic Findings in a Prospective Cohort of Patients With Crohn’s Disease Undergoing Surgery. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2023, 42, 1717–1728. [Google Scholar] [CrossRef] [PubMed]
- Yung, D.E.; Har-Noy, O.; Tham, Y.S.; Ben-Horin, S.; Eliakim, R.; Koulaouzidis, A.; Kopylov, U. Capsule Endoscopy, Magnetic Resonance Enterography, and Small Bowel Ultrasound for Evaluation of Postoperative Recurrence in Crohn’s Disease: Systematic Review and Meta-Analysis. Inflamm. Bowel Dis. 2018, 24, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, M.; Laurent, V.; Grandmougin, A.; Vuitton, L.; Bourreille, A.; Luc, A.; Clerc-Urmes, I.; Orry, X.; Frampas, E.; De Billy, M.; et al. A Magnetic Resonance Imaging Index to Predict Crohn’s Disease Postoperative Recurrence: The MONITOR Index. Clin. Gastroenterol. Hepatol. 2022, 20, e1040–e1049. [Google Scholar] [CrossRef] [PubMed]
- Yebra Carmona, J.; Poza Cordón, J.; Suárez Ferrer, C.; Martín Arranz, E.; Lucas Ramos, J.; Andaluz García, I.; Sánchez Azofra, M.; Rueda García, J.L.; Martín Arranz, M.D. Correlación entre la endoscopia y la ecografía intestinal para la evaluación de la recurrencia posquirúrgica de la enfermedad de Crohn. Gastroenterol. Hepatol. 2022, 45, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Mocci, G.; Migaleddu, V.; Cabras, F.; Sirigu, D.; Scanu, D.; Virgilio, G.; Marzo, M. SICUS and CEUS Imaging in Crohn’s Disease: An Update. J. Ultrasound 2017, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rispo, A.; Imperatore, N.; Testa, A.; Nardone, O.M.; Luglio, G.; Caporaso, N.; Castiglione, F. Diagnostic Accuracy of Ultrasonography in the Detection of Postsurgical Recurrence in Crohn’s Disease: A Systematic Review with Meta-Analysis. Inflamm. Bowel Dis. 2018, 24, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.M.; Ripollés, T.; Cortés, X.; Moreno, N.; Martínez, M.J.; Bustamante-Balén, M.; Delgado, F.; Moreno-Osset, E. Contrast-Enhanced Ultrasonography: Usefulness in the Assessment of Postoperative Recurrence of Crohn’s Disease. J. Crohns Colitis 2013, 7, 192–201. [Google Scholar] [CrossRef]
- Furfaro, F.; D’Amico, F.; Zilli, A.; Craviotto, V.; Aratari, A.; Bezzio, C.; Spinelli, A.; Gilardi, D.; Radice, S.; Saibeni, S.; et al. Noninvasive Assessment of Postoperative Disease Recurrence in Crohn’s Disease: A Multicenter, Prospective Cohort Study on Behalf of the Italian Group for Inflammatory Bowel Disease. Clin. Gastroenterol. Hepatol. 2023, 21, 3143–3151. [Google Scholar] [CrossRef]
- Alfarone, L.; Dal Buono, A.; Craviotto, V.; Zilli, A.; Fiorino, G.; Furfaro, F.; D’Amico, F.; Danese, S.; Allocca, M. Cross-Sectional Imaging Instead of Colonoscopy in Inflammatory Bowel Diseases: Lights and Shadows. J. Clin. Med. 2022, 11, 353. [Google Scholar] [CrossRef]
- Boube, M.; Laharie, D.; Nancey, S.; Hebuterne, X.; Fumery, M.; Pariente, B.; Roblin, X.; Peyrin-biroulet, L.; Minet-quinard, R.; Pereira, B.; et al. Variation of Faecal Calprotectin Level within the First Three Months after Bowel Resection Is Predictive of Endoscopic Postoperative Recurrence in Crohn’s Disease. Dig. Liver Dis. 2020, 52, 740–744. [Google Scholar] [CrossRef] [PubMed]
- RØseth, A.G.; Fagerhol, M.K.; Aadland, E.; Schjønsby, H. Assessment of the Neutrophil Dominating Protein Calprotectin in Feces: A Methodologic Study. Scand. J. Gastroenterol. 1992, 27, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Menees, S.B.; Powell, C.; Kurlander, J.; Goel, A.; Chey, W.D. A Meta-Analysis of the Utility of C-Reactive Protein, Erythrocyte Sedimentation Rate, Fecal Calprotectin, and Fecal Lactoferrin to Exclude Inflammatory Bowel Disease in Adults with IBS. Am. J. Gastroenterol. 2015, 110, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Ricciuto, A.; Lewis, A.; D’Amico, F.; Dhaliwal, J.; Griffiths, A.M.; Bettenworth, D.; Sandborn, W.J.; Sands, B.E.; Reinisch, W.; et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target Strategies in IBD. Gastroenterology 2021, 160, 1570–1583. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, F.; Nancey, S.; Danese, S.; Peyrin-Biroulet, L. A Practical Guide for Faecal Calprotectin Measurement: Myths and Realities. J. Crohns Colitis 2021, 15, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Sipponen, T.; Savilahti, E.; Kolho, K.-L.; Nuutinen, H.; Turunen, U.; Färkkilä, M. Crohn’s Disease Activity Assessed by Fecal Calprotectin and Lactoferrin: Correlation with Crohn’s Disease Activity Index and Endoscopic Findings. Inflamm. Bowel Dis. 2008, 14, 40–46. [Google Scholar] [CrossRef]
- Ho, G.T.; Lee, H.M.; Brydon, G.; Ting, T.; Hare, N.; Drummond, H.; Shand, A.G.; Bartolo, D.C.; Wilson, R.G.; Dunlop, M.G.; et al. Fecal Calprotectin Predicts the Clinical Course of Acute Severe Ulcerative Colitis. Am. J. Gastroenterol. 2009, 104, 673–678. [Google Scholar] [CrossRef]
- Molander, P.; af Björkesten, C.-G.; Mustonen, H.; Haapamäki, J.; Vauhkonen, M.; Kolho, K.-L.; Färkkilä, M.; Sipponen, T. Fecal Calprotectin Concentration Predicts Outcome in Inflammatory Bowel Disease after Induction Therapy with TNFα Blocking Agents. Inflamm. Bowel Dis. 2012, 18, 2011–2017. [Google Scholar] [CrossRef]
- Lobatón, T.; López-García, A.; Rodríguez-Moranta, F.; Ruiz, A.; Rodríguez, L.; Guardiola, J. A New Rapid Test for Fecal Calprotectin Predicts Endoscopic Remission and Postoperative Recurrence in Crohn’s Disease. J. Crohns Colitis 2013, 7, e641–e651. [Google Scholar] [CrossRef]
- Theede, K.; Holck, S.; Ibsen, P.; Ladelund, S.; Nordgaard-Lassen, I.; Nielsen, A.M. Level of Fecal Calprotectin Correlates with Endoscopic and Histologic Inflammation and Identifies Patients With Mucosal Healing in Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2015, 13, 1929–1936.e1. [Google Scholar] [CrossRef]
- Theede, K.; Holck, S.; Ibsen, P.; Kallemose, T.; Nordgaard-Lassen, I.; Nielsen, A.M. Fecal Calprotectin Predicts Relapse and Histological Mucosal Healing in Ulcerative Colitis. Inflamm. Bowel Dis. 2016, 22, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Zittan, E.; Kelly, O.B.; Kirsch, R.; Milgrom, R.; Burns, J.; Nguyen, G.C.; Croitoru, K.; Van Assche, G.; Silverberg, M.S.; Steinhart, A.H. Low Fecal Calprotectin Correlates with Histological Remission and Mucosal Healing in Ulcerative Colitis and Colonic Crohn’s Disease. Inflamm. Bowel Dis. 2016, 22, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Walsh, A.; Kormilitzin, A.; Hinds, C.; Sexton, V.; Brain, O.; Keshav, S.; Uhlig, H.; Geddes, J.; Goodwin, G.; Peters, M.; et al. Defining Faecal Calprotectin Thresholds as a Surrogate for Endoscopic and Histological Disease Activity in Ulcerative Colitis—A Prospective Analysis. J. Crohns Colitis 2019, 13, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Tham, Y.S.; Yung, D.E.; Fay, S.; Yamamoto, T.; Ben-Horin, S.; Eliakim, R.; Koulaouzidis, A.; Kopylov, U. Fecal Calprotectin for Detection of Postoperative Endoscopic Recurrence in Crohn’s Disease: Systematic Review and Meta-Analysis. Ther. Adv. Gastroenterol. 2018, 11, 175628481878557. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Shiraki, M.; Bamba, T.; Umegae, S.; Matsumoto, K. Faecal Calprotectin and Lactoferrin as Markers for Monitoring Disease Activity and Predicting Clinical Recurrence in Patients with Crohn’s Disease after Ileocolonic Resection: A Prospective Pilot Study. United Eur. Gastroenterol. J. 2013, 1, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Lasson, A.; Strid, H.; Öhman, L.; Isaksson, S.; Olsson, M.; Rydström, B.; Ung, K.-A.; Stotzer, P.-O. Fecal Calprotectin One Year after Ileocaecal Resection for Crohn’s Disease—A Comparison with Findings at Ileocolonoscopy. J. Crohns Colitis 2014, 8, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Boschetti, G.; Laidet, M.; Moussata, D.; Stefanescu, C.; Roblin, X.; Phelip, G.; Cotte, E.; Passot, G.; Francois, Y.; Drai, J.; et al. Levels of Fecal Calprotectin Are Associated with the Severity of Postoperative Endoscopic Recurrence in Asymptomatic Patients with Crohn’s Disease. Am. J. Gastroenterol. 2015, 110, 865–872. [Google Scholar] [CrossRef]
- Lamb, C.A.; Mohiuddin, M.K.; Gicquel, J.; Neely, D.; Bergin, F.G.; Hanson, J.M.; Mansfield, J.C. Faecal Calprotectin or Lactoferrin Can Identify Postoperative Recurrence in Crohn’s Disease. Br. J. Surg. 2009, 96, 663–674. [Google Scholar] [CrossRef]
- Khakoo, N.S.; Lewis, A.; Roldan, G.A.; Al Khoury, A.; Quintero, M.A.; Deshpande, A.R.; Kerman, D.H.; Damas, O.M.; Abreu, M.T. Patient Adherence to Fecal Calprotectin Testing Is Low Compared to Other Commonly Ordered Tests in Patients with Inflammatory Bowel Disease. Crohns Colitis 360 2021, 3, otab028. [Google Scholar] [CrossRef]
- Veyre, F.; Boschetti, G.; Meunier, C.; Cuerq, C.; Gay, C.; Charlois, A.-L.; Duclaux-Loras, R.; Danion, P.; Cotte, E.; Kepenekian, V.; et al. Low Levels of Fecal Calprotectin 3 Months after Surgery Predict Subsequent Endoscopic Postoperative Remission in Crohn’s Disease. Dig. Dis. Sci. 2021, 66, 4429–4435. [Google Scholar] [CrossRef]
- D’Haens, G.; Kelly, O.; Battat, R.; Silverberg, M.S.; Laharie, D.; Louis, E.; Savarino, E.; Bodini, G.; Yarur, A.; Boland, B.S.; et al. Development and Validation of a Test to Monitor Endoscopic Activity in Patients with Crohn’s Disease Based on Serum Levels of Proteins. Gastroenterology 2020, 158, 515–526.e10. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.L.; De Cruz, P.; Wright, E.K.; Dervieux, T.; Jain, A.; Kamm, M.A. Non-Invasive Serological Monitoring for Crohn’s Disease Postoperative Recurrence. J. Crohns Colitis 2022, 16, 1797–1807. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Blanco, L.; Manlay, L.; Reymond, M.; Dapoigny, M.; Rouquette, O.; Dubois, A.; Pereira, B. Top-down Versus Step-up Strategies to Prevent Postoperative Recurrence in Crohn’s Disease. Inflamm. Bowel Dis. 2023, 29, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Argollo, M.; Kotze, P.G.; Lamonaca, L.; Gilardi, D.; Furfaro, F.; Yamamoto, T.; Danese, S. Prevention of Postoperative Recurrence in CD: Tailoring Treatment to Patient Profile. Curr. Drug Targets 2019, 20, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
- Piovani, D.; Danese, S.; Peyrin-Biroulet, L.; Nikolopoulos, G.K.; Lytras, T.; Bonovas, S. Environmental Risk Factors for Inflammatory Bowel Diseases: An Umbrella Review of Meta-Analyses. Gastroenterology 2019, 157, 647–659.e4. [Google Scholar] [CrossRef] [PubMed]
- Kuenzig, M.E.; Lee, S.M.; Eksteen, B.; Seow, C.H.; Barnabe, C.; Panaccione, R.; Kaplan, G.G. Smoking Influences the Need for Surgery in Patients with the Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis Incorporating Disease Duration. BMC Gastroenterol. 2016, 16, 143. [Google Scholar] [CrossRef] [PubMed]
- Reese, G.E.; Nanidis, T.; Borysiewicz, C.; Yamamoto, T.; Orchard, T.; Tekkis, P.P. The Effect of Smoking after Surgery for Crohn’s Disease: A Meta-Analysis of Observational Studies. Int. J. Colorectal Dis. 2008, 23, 1213–1221. [Google Scholar] [CrossRef]
- Gklavas, A. Risk Factors for Postoperative Recurrence of Crohn’s Disease with Emphasis on Surgical Predictors. Ann. Gastroenterol. 2017, 30, 598. [Google Scholar] [CrossRef]
- Sachar, D.B.; Lemmer, E.; Ibrahim, C.; Edden, Y.; Ullman, T.; Ciardulo, J.; Roth, E.; Greenstein, A.J.; Bauer, J.J. Recurrence Patterns after First Resection for Stricturing or Penetrating Crohn’s Disease. Inflamm. Bowel Dis. 2009, 15, 1071–1075. [Google Scholar] [CrossRef]
- Simillis, C.; Yamamoto, T.; Reese, G.E.; Umegae, S.; Matsumoto, K.; Darzi, A.W.; Tekkis, P.P. A Meta-Analysis Comparing Incidence of Recurrence and Indication for Reoperation after Surgery for Perforating versus Nonperforating Crohn’s Disease. Am. J. Gastroenterol. 2008, 103, 196–205. [Google Scholar] [CrossRef]
- McLeod, R.S.; Wolff, B.G.; Ross, S.; Parkes, R.; McKenzie, M. Recurrence of Crohn’s Disease after Ileocolic Resection Is Not Affected by Anastomotic Type: Results of a Multicenter, Randomized, Controlled Trial. Dis. Colon Rectum 2009, 52, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Arslan Lied, G.; Arebi, N.; Phillips, R.K.; Kamm, M.A. Clinical and Surgical Recurrence of Crohn’s Disease after Ileocolonic Resection in a Specialist Unit. Eur. J. Gastroenterol. Hepatol. 2009, 21, 551–557. [Google Scholar] [CrossRef]
- Gionchetti, P.; Dignass, A.; Danese, S.; Magro Dias, F.J.; Rogler, G.; Lakatos, P.L.; Adamina, M.; Ardizzone, S.; Buskens, C.J.; Sebastian, S.; et al. 3rd European Evidence-Based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 2: Surgical Management and Special Situations. J. Crohns Colitis 2017, 11, 135–149. [Google Scholar] [CrossRef] [PubMed]
- Simillis, C.; Jacovides, M.; Reese, G.E.; Yamamoto, T.; Tekkis, P.P. Meta-Analysis of the Role of Granulomas in the Recurrence of Crohn Disease. Dis. Colon Rectum 2010, 53, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Ertem, F.U.; Rivers, C.R.; Watson, A.R.; Tang, G.; Schwartz, M.; Johnston, E.; Barrie, A.; Harrison, J.; Dueker, J.M.; Hartman, D.; et al. Granuloma Presence at Initial Surgery Predicts Need for Repeat Surgery Independent of Rutgeerts Score in Crohn’s Disease. Inflamm. Bowel Dis. 2023, 29, 1895–1900. [Google Scholar] [CrossRef] [PubMed]
- Yzet, C.; Riault, C.; Brazier, F.; Grados, L.; Nguyen-Khac, E.; Chatelain, D.; Sabbagh, C.; Buisson, A.; Diouf, M.; Fumery, M. Positive Margins and Plexitis Increase the Risk of Recurrence after Ileocecal Resection: A Systematic Review and Meta-Analysis. Dig. Liver Dis. 2023, S1590865822008702. [Google Scholar] [CrossRef] [PubMed]
- Dragoni, G.; Castiglione, F.; Bezzio, C.; Pugliese, D.; Spagnuolo, R.; Viola, A.; Cocomazzi, F.; Aratari, A.; Savarino, E.V.; Balestrieri, P.; et al. Comparison of Two Strategies for the Management of Postoperative Recurrence in Crohn’s Disease Patients with One Clinical Risk Factor: A Multicentre IG-IBD Study. United Eur. Gastroenterol. J. 2023, 11, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.; Kanth, R.; Gazo, J.; Sorrentino, D. Management of Post-Operative Crohn’s Disease in 2017: Where Do We Go from Here? Expert Rev. Gastroenterol. Hepatol. 2016, 10, 1257–1269. [Google Scholar] [CrossRef]
- Vaughn, B.P. Prevention of Post-Operative Recurrence of Crohn’s Disease. World J. Gastroenterol. 2014, 20, 1147. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Hiele, M.; Geboes, K.; Peeters, M.; Penninckx, F.; Aerts, R.; Kerremans, R. Controlled Trial of Metronidazole Treatment for Prevention of Crohn’s Recurrence after Ileal Resection. Gastroenterology 1995, 108, 1617–1621. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Van Assche, G.; Vermeire, S.; D’Haens, G.; Baert, F.; Noman, M.; Aerden, I.; De Hertogh, G.; Geboes, K.; Hiele, M.; et al. Ornidazole for Prophylaxis of Postoperative Crohn’s Disease Recurrence: A Randomized, Double-Blind, Placebo-Controlled Trial. Gastroenterology 2005, 128, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Herfarth, H.H.; Katz, J.A.; Hanauer, S.B.; Sandborn, W.J.; Loftus, E.V.; Sands, B.E.; Galanko, J.A.; Walkup, D.; Isaacs, K.L.; Martin, C.F.; et al. Ciprofloxacin for the Prevention of Postoperative Recurrence in Patients with Crohn’s Disease: A Randomized, Double-Blind, Placebo-Controlled Pilot Study. Inflamm. Bowel Dis. 2013, 19, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- van Loo, E.S.; Dijkstra, G.; Ploeg, R.J.; Nieuwenhuijs, V.B. Prevention of Postoperative Recurrence of Crohn’s Disease. J. Crohns Colitis 2012, 6, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Gjuladin-Hellon, T.; Gordon, M.; Iheozor-Ejiofor, Z.; Akobeng, A.K. Oral 5-Aminosalicylic Acid for Maintenance of Surgically-Induced Remission in Crohn’s Disease. Cochrane Database Syst. Rev. 2019, 2019, CD008414. [Google Scholar] [CrossRef] [PubMed]
- Hellers, G.; Cortot, A.; Jewell, D.; Leijonmarck, C.E.; Löfberg, R.; Malchow, H.; Nilsson, L.-G.; Pallone, F.; Pena, S.; Persson, T.; et al. Oral Budesonide for Prevention of Postsurgical Recurrence in Crohn’s Disease. Gastroenterology 1999, 116, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Ewe, K.; Böttger, T.; Buhr, H.J.; Ecker, K.-W.; Otto, H.F. Low-Dose Budesonide Treatment for Prevention of Postoperative Recurrence of Crohn’s Disease: A Multicentre Randomized Placebo-Controlled Trial. Eur. J. Gastroenterol. Hepatol. 1999, 11, 277–282. [Google Scholar] [CrossRef]
- Ardizzone, S.; Maconi, G.; Sampietro, G.M.; Russo, A.; Radice, E.; Colombo, E.; Imbesi, V.; Molteni, M.; Danelli, P.G.; Taschieri, A.M.; et al. Azathioprine and Mesalamine for Prevention of Relapse after Conservative Surgery for Crohn’s Disease. Gastroenterology 2004, 127, 730–740. [Google Scholar] [CrossRef]
- Hanauer, S.B.; Korelitz, B.I.; Rutgeerts, P.; Peppercorn, M.A.; Thisted, R.A.; Cohen, R.D.; Present, D.H. Postoperative Maintenance of Crohn’s Disease Remission with 6-Mercaptopurine, Mesalamine, or Placebo: A 2-Year Trial. Gastroenterology 2004, 127, 723–729. [Google Scholar] [CrossRef]
- D’Haens, G.R.; Vermeire, S.; Van Assche, G.; Noman, M.; Aerden, I.; Van Olmen, G.; Rutgeerts, P. Therapy of Metronidazole with Azathioprine to Prevent Postoperative Recurrence of Crohn’s Disease: A Controlled Randomized Trial. Gastroenterology 2008, 135, 1123–1129. [Google Scholar] [CrossRef]
- Mowat, C.; Arnott, I.; Cahill, A.; Smith, M.; Ahmad, T.; Subramanian, S.; Travis, S.; Morris, J.; Hamlin, J.; Dhar, A.; et al. Mercaptopurine versus Placebo to Prevent Recurrence of Crohn’s Disease after Surgical Resection (TOPPIC): A Multicentre, Double-Blind, Randomised Controlled Trial. Lancet Gastroenterol. Hepatol. 2016, 1, 273–282. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L.; Deltenre, P.; Ardizzone, S.; D’Haens, G.; Hanauer, S.B.; Herfarth, H.; Lémann, M.; Colombel, J.-F. Azathioprine and 6-Mercaptopurine for the Prevention of Postoperative Recurrence in Crohn’s Disease: A Meta-Analysis. Am. J. Gastroenterol. 2009, 104, 2089–2096. [Google Scholar] [CrossRef] [PubMed]
- Gjuladin-Hellon, T.; Iheozor-Ejiofor, Z.; Gordon, M.; Akobeng, A.K. Azathioprine and 6-Mercaptopurine for Maintenance of Surgically-Induced Remission in Crohn’s Disease. Cochrane Database Syst. Rev. 2019, 2019, CD010233. [Google Scholar] [CrossRef] [PubMed]
- Regueiro, M.; Feagan, B.G.; Zou, B.; Johanns, J.; Blank, M.A.; Chevrier, M.; Plevy, S.; Popp, J.; Cornillie, F.J.; Lukas, M.; et al. Infliximab Reduces Endoscopic, but Not Clinical, Recurrence of Crohn’s Disease after Ileocolonic Resection. Gastroenterology 2016, 150, 1568–1578. [Google Scholar] [CrossRef] [PubMed]
- Savarino, E.; Bodini, G.; Dulbecco, P.; Assandri, L.; Bruzzone, L.; Mazza, F.; Frigo, A.C.; Fazio, V.; Marabotto, E.; Savarino, V. Adalimumab Is More Effective Than Azathioprine and Mesalamine at Preventing Postoperative Recurrence of Crohn’s Disease: A Randomized Controlled Trial. Am. J. Gastroenterol. 2013, 108, 1731–1742. [Google Scholar] [CrossRef] [PubMed]
- Carla-Moreau, A.; Paul, S.; Roblin, X.; Genin, C.; Peyrin-Biroulet, L. Prevention and Treatment of Postoperative Crohn’s Disease Recurrence with Anti-TNF Therapy: A Meta-Analysis of Controlled Trials. Dig. Liver Dis. 2015, 47, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Mao, R.; Chen, B.; He, Y.; Zeng, Z.; Chen, M. Systematic Review with Meta-Analysis of Prospective Studies: Anti-Tumour Necrosis Factor for Prevention of Postoperative Crohn’s Disease Recurrence. J. Crohns Colitis 2015, 9, 918–927. [Google Scholar] [CrossRef]
- Jain, S.R.; Ow, Z.G.W.; Chin, Y.H.; Lim, W.H.; Kong, G.; Tham, H.Y.; Wong, N.W.; Chong, C.S.; Foo, F.J.; Chan, W.P.W. Quantifying the Rate of Recurrence of POSTOPERATIVE Crohn’s Disease with Biological Therapy. A META-ANALYSIS. J. Dig. Dis. 2021, 22, 399–407. [Google Scholar] [CrossRef]
- Beelen, E.M.J.; Nieboer, D.; Arkenbosch, J.H.C.; Regueiro, M.D.; Satsangi, J.; Ardizzone, S.; López-Sanromán, A.; Savarino, E.; Armuzzi, A.; Janneke Van Der Woude, C.; et al. Risk Prediction and Comparative Efficacy of Anti-TNF vs Thiopurines, for Preventing Postoperative Recurrence in Crohn’s Disease: A Pooled Analysis of 6 Trials. Clin. Gastroenterol. Hepatol. 2022, 20, 2741–2752.e6. [Google Scholar] [CrossRef]
- Regueiro, M.; Kip, K.E.; Baidoo, L.; Swoger, J.M.; Schraut, W. Postoperative Therapy with Infliximab Prevents Long-Term Crohn’s Disease Recurrence. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2014, 12, 1494–1502.e1. [Google Scholar] [CrossRef]
- Gangwani, M.K.; Nawras, M.; Aziz, M.; Rani, A.; Priyanka, F.; Dahiya, D.S.; Ahmed, Z.; Sohail, A.H.; Karna, R.; Lee-Smith, W.; et al. Comparing Adalimumab and Infliximab in the Prevention of Postoperative Recurrence of Crohn’s Disease: A Systematic Review and Meta-Analysis. Ann. Gastroenterol. 2023, 36, 293–299. [Google Scholar] [CrossRef]
- Cohen, B.L.; Fleshner, P.; Kane, S.V.; Herfarth, H.H.; Palekar, N.; Farraye, F.A.; Leighton, J.A.; Katz, J.A.; Cohen, R.D.; Gerich, M.E.; et al. Prospective Cohort Study to Investigate the Safety of Preoperative Tumor Necrosis Factor Inhibitor Exposure in Patients with Inflammatory Bowel Disease Undergoing Intra-Abdominal Surgery. Gastroenterology 2022, 163, 204–221. [Google Scholar] [CrossRef] [PubMed]
- Fumery, M.; Seksik, P.; Auzolle, C.; Munoz-Bongrand, N.; Gornet, J.-M.; Boschetti, G.; Cotte, E.; Buisson, A.; Dubois, A.; Pariente, B.; et al. Postoperative Complications after Ileocecal Resection in Crohn’s Disease: A Prospective Study From the REMIND Group. Am. J. Gastroenterol. 2017, 112, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Payen, E.; Neuraz, A.; Zenzeri, L.; Talbotec, C.; Abi Nader, E.; Chatenoud, L.; Chhun, S.; Goulet, O.; Ruemmele, F.M.; Pigneur, B. Adalimumab Therapy in Pediatric Crohn Disease: A 2-Year Follow-Up Comparing “Top-Down” and “Step-Up” Strategies. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Jenkinson, P.W.; Plevris, N.; Siakavellas, S.; Lyons, M.; Arnott, I.D.; Wilson, D.; Watson, A.J.M.; Jones, G.-R.; Lees, C.W. Temporal Trends in Surgical Resection Rates and Biologic Prescribing in Crohn’s Disease: A Population-Based Cohort Study. J. Crohns Colitis 2020, 14, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Taxonera, C.; Lopez-Sanroman, A.; Nos Mateu, P.; Danese, S.; Armuzzi, A.; Roblin, X.; Peyrin-Biroulet, L.; West, R.; Witteman, B.; et al. OP14 Prevention of Postoperative Recurrence of Crohn’s Disease with Vedolizumab: First Results of the Prospective Placebo-Controlled Randomised Trial REPREVIO. J. Crohns Colitis 2023, 17, i19. [Google Scholar] [CrossRef]
- Yanai, H.; Kagramanova, A.; Knyazev, O.; Sabino, J.; Haenen, S.; Mantzaris, G.J.; Mountaki, K.; Armuzzi, A.; Pugliese, D.; Furfaro, F.; et al. Endoscopic Postoperative Recurrence in Crohn’s Disease after Curative Ileocecal Resection with Early Prophylaxis by Anti-TNF, Vedolizumab or Ustekinumab: A Real-World Multicentre European Study. J. Crohns Colitis 2022, 16, 1882–1892. [Google Scholar] [CrossRef] [PubMed]
- Mañosa, M.; Fernández-Clotet, A.; Nos, P.; Martín-Arranz, M.D.; Manceñido, N.; Carbajo, A.; Hinojosa, E.; Hernández-Camba, A.; Muñoz-Pérez, R.; Boscá-Watts, M.; et al. Ustekinumab and Vedolizumab for the Prevention of Postoperative Recurrence of Crohn’s Disease: Results from the ENEIDA Registry. Dig. Liver Dis. 2023, 55, 46–52. [Google Scholar] [CrossRef]
- Buisson, A.; Nancey, S.; Manlay, L.; Rubin, D.T.; Hebuterne, X.; Pariente, B.; Fumery, M.; Laharie, D.; Roblin, X.; Bommelaer, G.; et al. Ustekinumab Is More Effective than Azathioprine to Prevent Endoscopic Postoperative Recurrence in Crohn’s Disease. United Eur. Gastroenterol. J. 2021, 9, 552–560. [Google Scholar] [CrossRef]
- Yamada, A.; Komaki, Y.; Patel, N.; Komaki, F.; Pekow, J.; Dalal, S.; Cohen, R.D.; Cannon, L.; Umanskiy, K.; Smith, R.; et al. The Use of Vedolizumab in Preventing Postoperative Recurrence of Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 502–509. [Google Scholar] [CrossRef]
- D’Amico, F.; Tasopoulou, O.; Fiorino, G.; Zilli, A.; Furfaro, F.; Allocca, M.; Sileri, P.; Spinelli, A.; Peyrin-Biroulet, L.; Danese, S. Early Biological Therapy in Operated Crohn’s Disease Patients Is Associated with a Lower Rate of Endoscopic Recurrence and Improved Long-Term Outcomes: A Single-Center Experience. Inflamm. Bowel Dis. 2023, 29, 539–547. [Google Scholar] [CrossRef]
- Ferrante, M.; Pouillon, L.; Mañosa, M.; Savarino, E.; Allez, M.; Kapizioni, C.; Arebi, N.; Carvello, M.; Myrelid, P.; De Vries, A.C.; et al. Results of the Eighth Scientific Workshop of ECCO: Prevention and Treatment of Postoperative Recurrence in Patients with Crohn’s Disease Undergoing an Ileocolonic Resection with Ileocolonic Anastomosis. J. Crohns Colitis 2023, 17, 1707–1722. [Google Scholar] [CrossRef] [PubMed]
- Reinisch, W.; Angelberger, S.; Petritsch, W.; Shonova, O.; Lukas, M.; Bar-Meir, S.; Teml, A.; Schaeffeler, E.; Schwab, M.; Dilger, K.; et al. Azathioprine versus Mesalazine for Prevention of Postoperative Clinical Recurrence in Patients with Crohn’s Disease with Endoscopic Recurrence: Efficacy and Safety Results of a Randomised, Double-Blind, Double-Dummy, Multicentre Trial. Gut 2010, 59, 752–759. [Google Scholar] [CrossRef] [PubMed]
- Orlando, A.; Mocciaro, F.; Ventimiglia, M.; Renna, S.; Rispo, A.; Scribano, M.L.; Testa, A.; Aratari, A.; Bossa, F.; Angelucci, E.; et al. Azathioprine for prevention of clinical recurrence in Crohn’s disease patients with severe endoscopic recurrence: An IG-IBD randomized double-blind trial. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11356–11364. [Google Scholar] [CrossRef] [PubMed]
- Zabana, Y.; Mañosa, M.; Cabré, E.; Bernal, I.; Marín, L.; Lorenzo-Zúñiga, V.; Moreno, V.; Boix, J.; Domènech, E. Addition of Mesalazine for Subclinical Post-Surgical Endoscopic Recurrence of Crohn’s Disease despite Preventive Thiopurine Therapy: A Case-Control Study. J. Gastroenterol. Hepatol. 2014, 29, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- D’Haens, G.; Geboes, K.; Ponette, E.; Penninckx, F.; Rutgeerts, P. Healing of Severe Recurrent Ileitis with Azathioprine Therapy in Patients with Crohn’s Disease. Gastroenterology 1997, 112, 1475–1481. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, M.; Papamichael, K.; Duricova, D.; D’Haens, G.; Vermeire, S.; Archavlis, E.; Rutgeerts, P.; Bortlik, M.; Mantzaris, G.; Van Assche, G.; et al. Systematic versus Endoscopy-Driven Treatment with Azathioprine to Prevent Postoperative Ileal Crohn’s Disease Recurrence. J. Crohns Colitis 2015, 9, 617–624. [Google Scholar] [CrossRef] [PubMed]
- De Cruz, P.; Hamilton, A.L.; Burrell, K.J.; Gorelik, A.; Liew, D.; Kamm, M.A. Endoscopic Prediction of Crohn’s Disease Postoperative Recurrence. Inflamm. Bowel Dis. 2022, 28, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, K.; Archavlis, E.; Lariou, C.; Mantzaris, G.J. Adalimumab for the Prevention and/or Treatment of Post-Operative Recurrence of Crohn’s Disease: A Prospective, Two-Year, Single Center, Pilot Study. J. Crohns Colitis 2012, 6, 924–931. [Google Scholar] [CrossRef]
- Cañete, F.; Mañosa, M.; Pérez-Martínez, I.; Barreiro-de Acosta, M.; González-Sueyro, R.C.; Nos, P.; Iglesias-Flores, E.; Gutiérrez, A.; Bujanda, L.; Gordillo, J.; et al. Antitumor Necrosis Factor Agents to Treat Endoscopic Postoperative Recurrence of Crohn’s Disease: A Nationwide Study with Propensity-Matched Score Analysis. Clin. Transl. Gastroenterol. 2020, 11, e00218. [Google Scholar] [CrossRef]
- Allocca, M.; Landi, R.; Bonovas, S.; Fiorino, G.; Papa, A.; Spinelli, A.; Furfaro, F.; Peyrin-Biroulet, L.; Armuzzi, A.; Danese, S. Effectiveness of Mesalazine, Thiopurines and Tumour Necrosis Factor Antagonists in Preventing Post-Operative Crohn’s Disease Recurrence in a Real-Life Setting. Digestion 2017, 96, 166–172. [Google Scholar] [CrossRef]
- Tursi, A.; Mocci, G.; Picchio, M.; Elisei, W.; Maconi, G. Letter: Ustekinumab for the Treatment of Post-Surgical and Refractory Crohn’s Disease. Aliment. Pharmacol. Ther. 2021, 53, 859–860. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, F.S.; Grova, M.; Mocciaro, F.; Di Mitri, R.; Privitera, A.C.; Distefano, M.E.; Vitello, A.; Camilleri, S.; Ferracane, C.; Pluchino, D.; et al. Ustekinumab Is a Promising Option for the Treatment of Postoperative Recurrence of Crohn’s Disease. J. Gastroenterol. Hepatol. 2023, 38, 1503–1509. [Google Scholar] [CrossRef]
- Ahmed, W.; Mahtani, P.; Pan, Y.; Rajan, A.; Lai, D.; Gordon, B.L.; Smith, E.S.; Longman, R.; Lukin, D.J.; Scherl, E.; et al. S874 Comparative Efficacy of TNF Antagonists and Ustekinumab in Post-Operative Crohn’s Disease. Off. J. Am. Coll. Gastroenterol. ACG 2021, 116, S409. [Google Scholar] [CrossRef]
- Macaluso, F.S.; Cappello, M.; Crispino, F.; Grova, M.; Privitera, A.C.; Piccillo, G.; Magnano, A.; Ferracane, C.; Belluardo, N.; Giangreco, E.; et al. Vedolizumab May Be an Effective Option for the Treatment of Postoperative Recurrence of Crohn’s Disease. Dig. Liver Dis. 2022, 54, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Ellul, P.; Langhorst, J.; Mikocka-Walus, A.; Barreiro-de Acosta, M.; Basnayake, C.; Ding, N.J.S.; Gilardi, D.; Katsanos, K.; Moser, G.; et al. European Crohn’s and Colitis Organisation Topical Review on Complementary Medicine and Psychotherapy in Inflammatory Bowel Disease. J. Crohns Colitis 2019, 13, 673–685e. [Google Scholar] [CrossRef] [PubMed]
- Ferman, M.; Lim, A.H.; Hossain, M.; Siow, G.W.; Andrews, J.M. Multidisciplinary Team Meetings Appear to Be Effective in Inflammatory Bowel Disease Management: An Audit of Process and Outcomes. Intern. Med. J. 2018, 48, 1102–1108. [Google Scholar] [CrossRef]
- Gasparetto, M.; Angriman, I.; Guariso, G. The Multidisciplinary Health Care Team in the Management of Stenosis in Crohn’s Disease. J. Multidiscip. Healthc. 2015, 8, 167–179. [Google Scholar] [CrossRef]
- Angriman, I.; Buzzi, G.; Giorato, E.; Barbierato, M.; Cavallin, F.; Ruffolo, C.; Degasperi, S.; Mari, V.; De Simoni, O.; Campi, M.; et al. Crohn’s Disease-Related Stoma Complications and Their Impact on Postsurgical Course. Dig. Surg. 2022, 39, 83–91. [Google Scholar] [CrossRef]
- Maheshwari, P.; Bobb, A.; Stuart, A.; Dalessio, S.; Bernasko, N.; Tinsley, A.; Clarke, K.; Coates, M.D.; Williams, E. Impact of a Nurse Navigator on a Dedicated Inflammatory Bowel Disease-Focused Gastroenterology Clinic. Ann. Gastroenterol. 2021, 34, 675–679. [Google Scholar] [CrossRef]
- Kok, K.B.; Byrne, P.; Ibarra, A.R.; Martin, P.; Rampton, D.S. Understanding and Managing Psychological Disorders in Patients with Inflammatory Bowel Disease: A Practical Guide. Frontline Gastroenterol. 2023, 14, 78–86. [Google Scholar] [CrossRef]
- Magavi, P.R.; Beeken, L.A.; Matro, R.; Ally, M.; Ferrari, M.J.; Konijeti, G.G. Incorporating Nutrition-Based Strategies into IBD Treatment. Curr. Gastroenterol. Rep. 2022, 24, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Alrashed, F.; Almutairi, N.; Shehab, M. The Role of Clinical Pharmacists in Improving Quality of Care in Patients with Inflammatory Bowel Disease: An Evaluation of Patients’ and Physicians’ Satisfaction. Healthc. Basel Switz. 2022, 10, 1818. [Google Scholar] [CrossRef] [PubMed]
- Parigi, T.L.; D’Amico, F.; Abreu, M.T.; Dignass, A.; Dotan, I.; Magro, F.; Griffiths, A.M.; Jairath, V.; Iacucci, M.; Mantzaris, G.J.; et al. Difficult-to-Treat Inflammatory Bowel Disease: Results from an International Consensus Meeting. Lancet Gastroenterol. Hepatol. 2023, 8, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Panaccione, R. Anti-Adhesion Molecule Therapy for Inflammatory Bowel Disease. Ther. Adv. Gastroenterol. 2010, 3, 239–258. [Google Scholar] [CrossRef] [PubMed]
- D’Alessio, S.; Ungaro, F.; Noviello, D.; Lovisa, S.; Peyrin-Biroulet, L.; Danese, S. Revisiting Fibrosis in Inflammatory Bowel Disease: The Gut Thickens. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Argollo, M.; Gilardi, D.; Roda, G.; Fiorino, G.; Peyrin-Biroulet, L.; Danese, S. Anti-Fibrotic Drugs for Crohn’s Disease: Ready for Prime Time? Curr. Pharm. Des. 2019, 25, 47–56. [Google Scholar] [CrossRef]
- Rankin, A.; Baumann, A.; Downey, B.; Valaitis, R.; Montour, A.; Mandy, P. The Role of the Indigenous Patient Navigator: A Scoping Review. Can. J. Nurs. Res. Rev. Can. Rech. En Sci. Infirm. 2022, 54, 199–210. [Google Scholar] [CrossRef]
- Parigi, T.L.; Iacucci, M.; Ghosh, S. Blockade of IL-23: What Is in the Pipeline? J. Crohns Colitis 2022, 16, ii64–ii72. [Google Scholar] [CrossRef]
- Parigi, T.L.; Solitano, V.; Peyrin-Biroulet, L.; Danese, S. Do JAK Inhibitors Have a Realistic Future in Treating Crohn’s Disease? Expert Rev. Clin. Immunol. 2022, 18, 181–183. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasulo, E.; D’Amico, F.; Osorio, L.; Allocca, M.; Fiorino, G.; Zilli, A.; Parigi, T.L.; Danese, S.; Furfaro, F. The Management of Postoperative Recurrence in Crohn’s Disease. J. Clin. Med. 2024, 13, 119. https://doi.org/10.3390/jcm13010119
Fasulo E, D’Amico F, Osorio L, Allocca M, Fiorino G, Zilli A, Parigi TL, Danese S, Furfaro F. The Management of Postoperative Recurrence in Crohn’s Disease. Journal of Clinical Medicine. 2024; 13(1):119. https://doi.org/10.3390/jcm13010119
Chicago/Turabian StyleFasulo, Ernesto, Ferdinando D’Amico, Laura Osorio, Mariangela Allocca, Gionata Fiorino, Alessandra Zilli, Tommaso Lorenzo Parigi, Silvio Danese, and Federica Furfaro. 2024. "The Management of Postoperative Recurrence in Crohn’s Disease" Journal of Clinical Medicine 13, no. 1: 119. https://doi.org/10.3390/jcm13010119
APA StyleFasulo, E., D’Amico, F., Osorio, L., Allocca, M., Fiorino, G., Zilli, A., Parigi, T. L., Danese, S., & Furfaro, F. (2024). The Management of Postoperative Recurrence in Crohn’s Disease. Journal of Clinical Medicine, 13(1), 119. https://doi.org/10.3390/jcm13010119