

Functional and Mortality Outcomes with Medical and Surgical Therapy in Malignant Posterior Circulation Infarcts: A Systematic Review


 , ,
, ,  , and
, and
Abstract
1. Introduction
2. Methods
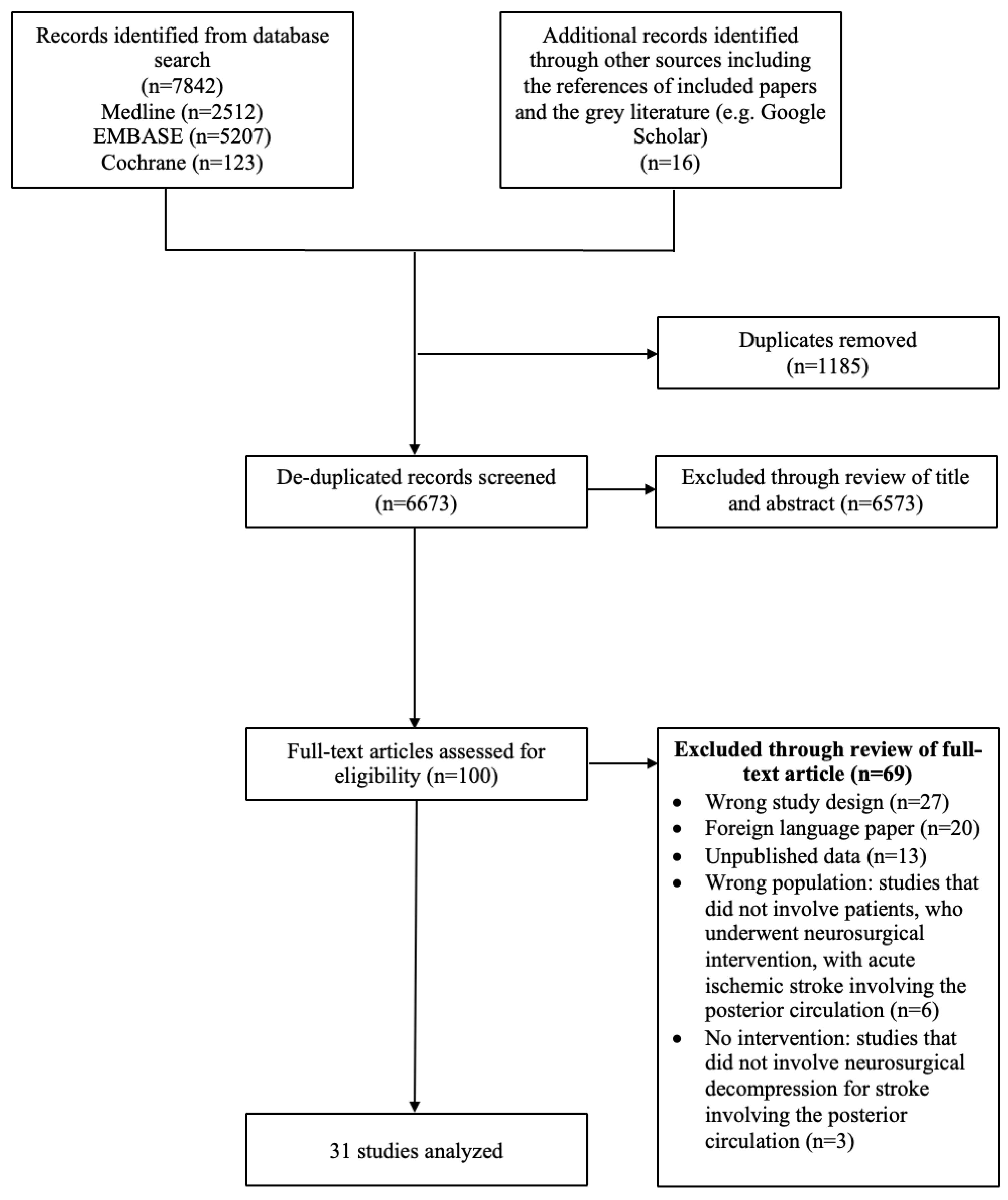
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Reporting Bias Assessment

{kind=link}
{kind=link}
| (A) | |||||||
|---|---|---|---|---|---|---|---|
| Study Title | Authors | Study Design | Country | Definition of Good Functional Outcome | Number of Patients Treated Surgically | Number of Patients Treated Medically | Follow-Up Duration (Months) |
| Cerebellar infarction with obstructive hydrocephalus | Taneda et al., 1982 [17] | Retrospective cohort study | Japan | Completely recovered | 10 | 5 | Unreported |
| Surgical and medical management of patients with massive cerebellar infarctions: results of the German–Austrian Cerebellar Infarction Study. | Jauss et al., 1999 [18] | Cohort study | Germany | mRS ≤ 2 | 48 | 36 | Mean: 3 |
| Space occupying cerebellar infarction | Hornig et al., 1994 [19] | Retrospective cohort study | Germany | mRS ≤ 1 | 36 | 16 | Unreported |
| Neurosurgical management of cerebellar haematoma and infarct | Mathew et al., 1995 [20] | Retrospective cohort study | UK | GOS: unspecified by author. Assumed to be GOS ≥ 4 | 16 | 34 | Unreported |
| Neuroimaging in deteriorating patients with cerebellar infarcts and mass effect | Koh et al., 2000 [21] | Retrospective cohort study | USA | mRS ≤ 2 | 9 | 26 | Median: 16 (range: 1–105) |
| Management of acute cerebellar infarction: one institution’s experience | Raco et al., 2003 [22] | Retrospective case series | Italy | GOS: unspecified by author. Assumed to be GOS ≥ 4 | 19 | 25 | Unreported |
| Neurosurgical management of massive cerebellar infarct outcome in 53 patients | Mostofi, 2013 [23] | Retrospective cohort study | French West Indies | Unreported by author. Unable to determine | 25 | 28 | Unreported |
| Predicting Surgical Intervention in Cerebellar Stroke: A Quantitative Retrospective Analysis | Taylor et al., 2020 [24] | Retrospective cohort study | USA | Unreported by author. Unable to determine | 21 | 65 | Unreported |
| (B) | |||||||
| Study Title | Authors | Study Design | Country | Definition of Good Functional Outcome | Number of Patients Treated Surgically | Follow-Up Duration (Months) | |
| Treatment of cerebellar infarction by decompressive suboccipital craniectomy | Chen et al., 1992 [25] | Case series | Germany | Barthel Index; unspecified by author. Assumed to be BI = 100 | 11 | Mean: 42.9 | |
| Management of cerebellar infarction with associated occlusive hydrocephalus | Bertalanffy et al., 1992 [26] | Case series | Germany | Unreported | 10 | Unreported | |
| Monitoring therapeutic efficacy of decompressive craniotomy in space occupying cerebellar infarcts using brain-stem auditory evoked potentials | Krieger et al., 1993 [27] | Case series | Germany | Unreported by author. Unable to determine | 11 | Unreported | |
| Is decompressive craniectomy for acute cerebral infarction of any benefit? | Koh et al., 2000 [28] | Case series | Singapore | GOS ≥ 4 | 3 | Mean: 7 (range: 3–17) | |
| Clinical outcome following surgical treatment for bilateral cerebellar infarction. | Tsitsopoulos et al., 2011 [13] | Case series | Denmark | mRS ≤ 2 | 10 | Median: 57.6 (range: 15–118) | |
| Endoscopic third ventriculostomy for occlusive hydrocephalus caused by cerebellar infarction | Baldauf et al., 2006 [29] | Case series | Germany | Unreported by author. Unable to determine | 10 | Mean: 43 | |
| Controversy of surgical treatment for severe cerebellar infarction | Kudo et al., 2007 [30] | Case series | Germany | GOS | 25 | Unreported | |
| Occlusive hydrocephalus associated with cerebellar infarction treated with endoscopic third ventriculostomy: report of 5 cases | Yoshimura, et al., 2007 [31] | Case series | USA | GOS; undefined. Assumed to be GOS ≥ 4 | 5 | Mean: 3 | |
| Long-term outcome after suboccipital decompressive craniectomy for malignant cerebellar infarction. | Pfefferkorn T et al., 2009 [32] | Case series | Germany | mRS ≤ 3 | 57 | Unreported | |
| Long-term outcome after surgical treatment for space-occupying cerebellar infarction: experience in 56 patients. | Jüttler et al., 2009 [33] | Case series | Germany | mRS ≤ 2 | 56 | Unreported | |
| Hydrocephalus in posterior fossa lesions: ventriculostomy and permanent shunt rates by diagnosis | Mangubat et al., 2009 [34] | Case series | USA | Unreported by author. Unable to determine | 4 | Unreported | |
| Endoscopic third ventriculostomy in patients with secondary triventricular hydrocephalus from a haemorrhage or ischaemia in the posterior cranial fossa | Vindigni et al., 2010 [35] | Case series | Italy | GOS; undefined. Assumed to be GOS ≥ 4 | 19 | Mean: 6 | |
| Surgical treatment of patients with unilateral cerebellar infarcts: clinical outcome and prognostic factors. | Tsitsopoulos et al., 2011 [36] | Case series | Germany | mRS ≤ 2 | 32 | Unreported | |
| Ventriculosubgaleal shunt in the management of obstructive hydrocephalus caused by cerebellar infarction | Moussa et al., 2013 [37] | Case series | Germany | Unreported by author. Unable to determine | 10 | Mean: 6 | |
| Lesions on DWI and the Outcome in Hyperacute Posterior Circulation Stroke | Lee et al., 2014 [38] | Case series | South Korea | mRS ≤ 2 | 9 | Mean: 3 | |
| Preventive suboccipital decompressive craniectomy for cerebellar infarction: a retrospective matched case control study | Kim et al., 2016 [39] | Case-control | South Korea | mRS ≤ 2 | 84 | Mean: 12 | |
| Neurologic Outcome After Decompressive Craniectomy: Predictors of Outcome in Different Pathologic Conditions | Goedemans et al., 2017 [40] | Case series | Amsterdam | GOS ≥4 | 10 | Mean: 12 | |
| Strokectomy and Extensive Cerebrospinal Fluid Drainage for the Treatment of Space-Occupying Cerebellar Ischemic Stroke | Tartara et al., 2018 [41] | Case series | Germany | mRS ≤ 2 | 11 | Mean: 33.8 (range 12–58) | |
| Long-term functional outcome after decompressive suboccipital craniectomyfor space-occupying cerebellar infarction | Lindeskog et al., 2019 [42] | Case series | Denmark | mRS ≤ 3 | 22 | Mean: 12 | |
| Evaluation of clinical significance of decompressive suboccipital craniectomy on the prognosis of cerebellar infarction | Suyama et al., 2019 [43] | Case series | Japan | mRS; unspecified by author. Assumed to be Mrs ≤ 2 | 14 | Mean: 3 | |
| Posterior Fossa Surgery for Stroke: Differences in Outcomes Between Cerebellar Hemorrhage and Infarcts | Lee et al., 2020 [10] | Case series | Germany | mRS ≤3 | 50 | Mean: 44.5 ± 33.9 | |
| Cerebellar Necrosectomy Instead of Suboccipital Decompression: A Suitable Alternative for Patients with Space-Occupying Cerebellar Infarction | Hernández-Durán et al., 2020 [44] | Case series | Germany | GOS ≥ 4 | 34 | Unreported | |
| The impact of emergent suboccipital craniectomy upon outcome and prognosis of massive cerebellar infarction: A single institutional study | Mattar et al., 2021 [45] | Case series | Egypt | mRS ≤ 2 | 42 | Mean: 3 | |
3. Results
3.1. Medical versus Surgical Treatment
3.1.1. Choice of Surgical Treatment vs. Medical Treatment
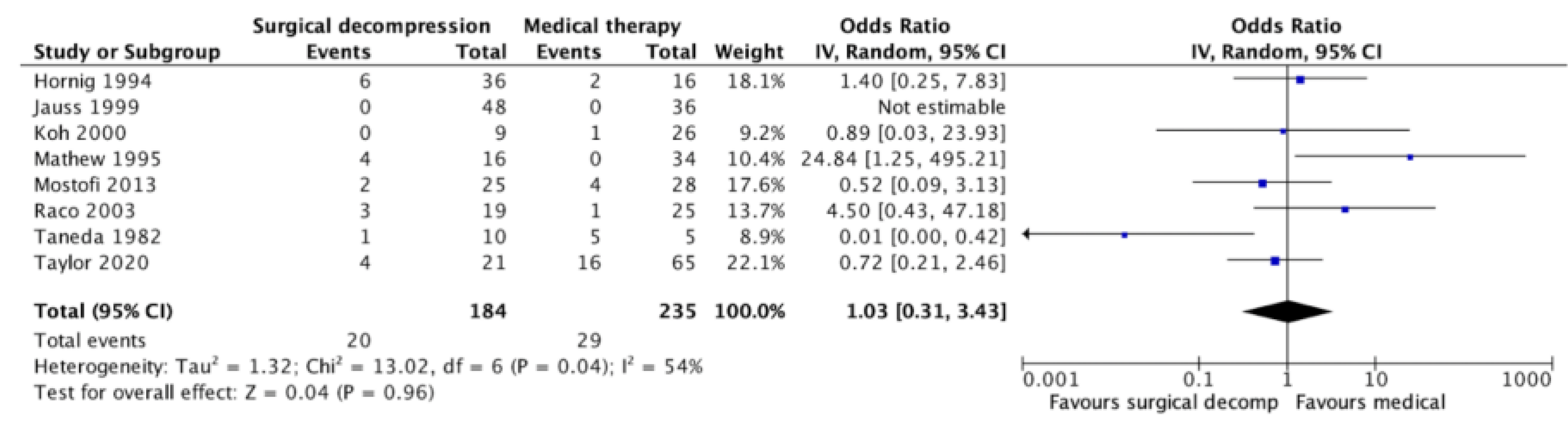
3.1.2. Comparing Functional Outcomes between Medical and Surgical Treatment
3.1.3. Comparing Mortality Rates between Medical and Surgical Treatment
3.2. Surgical Treatment
3.2.1. Timing of Surgical Treatment
3.2.2. Choice of Surgical Intervention
3.3. Assessment of Publication Bias
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ETV | Endoscopic third ventriculostomy |
| EVD | Extraventricular drainage |
| GCS | Glasgow Coma Scale |
| GOS | Glasgow Outcome Scale |
| JBI | Joanna Briggs Institute |
| MPCI | Malignant posterior circulation infarcts |
| mRS | Modified Rankin Scale |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| SDC | Suboccipital decompressive craniectomy |
References
- Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; GBD 2016 Lifetime Risk of Stroke Collaborators; et al. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [PubMed]
- Mehndiratta, M.; Pandey, S.; Nayak, R.; Alam, A. Posterior Circulation Ischemic Stroke—Clinical Characteristics, Risk Factors, and Subtypes in a North Indian Population. Neurohospitalist 2012, 2, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Schulz, U.G.; Fischer, U. Posterior Circulation Cerebrovascular Syndromes: Diagnosis and Management. J. Neurol. Neurosurg. Psychiatry 2017, 88, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Sommer, P.; Posekany, A.; Serles, W.; Marko, M.; Scharer, S.; Fertl, E.; Ferrari, J.; Lang, W.; Vosko, M.; Szabo, S.; et al. Is Functional Outcome Different in Posterior and Anterior Circulation Stroke? Stroke 2018, 49, 2728–2732. [Google Scholar] [CrossRef] [PubMed]
- Wijdicks, E.F.M.; Sheth, K.N.; Carter, B.S.; Greer, D.M.; Kasner, S.E.; Kimberly, W.T.; Schwab, S.; Smith, E.E.; Tamargo, R.J.; Wintermark, M.; et al. Recommendations for the Management of Cerebral and Cerebellar Infarction with Swelling: A Statement for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2014, 45, 1222–1238. [Google Scholar] [CrossRef]
- Vahedi, K.; Hofmeijer, J.; Juettler, E.; Vicaut, E.; George, B.; Algra, A.; Amelink, G.J.; Schmiedeck, P.; Schwab, S.; Rothwell, P.M.; et al. Early Decompressive Surgery in Malignant Infarction of the Middle Cerebral Artery: A Pooled Analysis of Three Randomised Controlled Trials. Lancet Neurol. 2007, 6, 215–222. [Google Scholar] [CrossRef]
- Hofmeijer, J.; Kappelle, L.J.; Algra, A.; Amelink, G.J.; van Gijn, J.; van der Worp, H.B. Others Surgical Decompression for Space-Occupying Cerebral Infarction (the Hemicraniectomy After Middle Cerebral Artery Infarction with Life-Threatening Edema Trial [HAMLET]): A Multicentre, Open, Randomised Trial. Lancet Neurol. 2009, 8, 326–333. [Google Scholar] [CrossRef]
- Honeybul, S.; Gillett, G.R.; Ho, K.M.; Janzen, C.; Kruger, K. Is Life Worth Living? Decompressive Craniectomy and the Disability Paradox. J. Neurosurg. 2016, 125, 775–778. [Google Scholar] [CrossRef]
- Kürten, S.; Munoz, C.; Beseoglu, K.; Fischer, I.; Perrin, J.; Steiger, H.-J. Decompressive Hemicraniectomy for Malignant Middle Cerebral Artery Infarction Including Patients with Additional Involvement of the Anterior And/or Posterior Cerebral Artery Territory-Outcome Analysis and Definition of Prognostic Factors. Acta Neurochir. 2018, 160, 83–89. [Google Scholar] [CrossRef]
- Lee, L.; Loh, D.; Kam King, N.K. Posterior Fossa Surgery for Stroke: Differences in Outcomes Between Cerebellar Hemorrhage and Infarcts. World Neurosurg. 2020, 135, e375–e381. [Google Scholar] [CrossRef]
- Ayling, O.G.S.; Alotaibi, N.M.; Wang, J.Z.; Fatehi, M.; Ibrahim, G.M.; Benavente, O.; Field, T.S.; Gooderham, P.A.; Macdonald, R.L. Suboccipital Decompressive Craniectomy for Cerebellar Infarction: A Systematic Review and Meta-Analysis. World Neurosurg. 2018, 110, 450–459.e5. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Tsitsopoulos, P.P.; Tobieson, L.; Enblad, P.; Marklund, N. Clinical Outcome Following Surgical Treatment for Bilateral Cerebellar Infarction. Acta Neurol. Scand. 2011, 123, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Robertson, J.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta- Analysis. Available online: http://www3.med.unipmn.it/dispense_ebm/2009-2010/Corso%20Perfezionamento%20EBM_Faggiano/NOS_oxford.pdf (accessed on 11 November 2021).
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetic, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. JBI Reviewer’s Manual; JBI: Abelaide, Australia, 2019. [Google Scholar]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological Quality of Case Series Studies: An Introduction to the JBI Critical Appraisal Tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Taneda, M.; Ozaki, K.; Wakayama, A.; Yagi, K.; Kaneda, H.; Irino, T. Cerebellar Infarction with Obstructive Hydrocephalus. J. Neurosurg. 1982, 57, 83–91. [Google Scholar] [CrossRef]
- Jauss, M.; Krieger, D.; Hornig, C.; Schramm, J.; Busse, O. Surgical and Medical Management of Patients with Massive Cerebellar Infarctions: Results of the German-Austrian Cerebellar Infarction Study. J. Neurol. 1999, 246, 257–264. [Google Scholar] [CrossRef]
- Hornig, C.R.; Rust, D.S.; Busse, O.; Jauss, M.; Laun, A. Space-Occupying Cerebellar Infarction. Clinical Course and Prognosis. Stroke 1994, 25, 372–374. [Google Scholar] [CrossRef]
- Mathew, P.; Teasdale, G.; Bannan, A.; Oluoch-Olunya, D. Neurosurgical Management of Cerebellar Haematoma and Infarct. J. Neurol. Neurosurg. Psychiatry 1995, 59, 287–292. [Google Scholar] [CrossRef]
- Koh, M.G.; Phan, T.G.; Atkinson, J.L.; Wijdicks, E.F. Neuroimaging in Deteriorating Patients with Cerebellar Infarcts and Mass Effect. Stroke 2000, 31, 2062–2067. [Google Scholar] [CrossRef]
- Raco, A.; Caroli, E.; Isidori, A.; Salvati, M. Management of Acute Cerebellar Infarction: One Institution’s Experience. Neurosurgery 2003, 53, 1061–1065, discussion 1065–1066. [Google Scholar] [CrossRef]
- Mostofi, K. Neurosurgical Management of Massive Cerebellar Infarct Outcome in 53 Patients. Surg. Neurol. Int. 2013, 4, 28. [Google Scholar] [CrossRef]
- Taylor, D.R.; Basma, J.; Jones, G.M.; Lillard, J.; Wallace, D.; Ajmera, S.; Gienapp, A.J.; Michael, L.M., 2nd. Predicting Surgical Intervention in Cerebellar Stroke: A Quantitative Retrospective Analysis. World Neurosurg. 2020, 142, e160–e172. [Google Scholar] [CrossRef]
- Chen, H.J.; Lee, T.C.; Wei, C.P. Treatment of Cerebellar Infarction by Decompressive Suboccipital Craniectomy. Stroke 1992, 23, 957–961. [Google Scholar] [CrossRef]
- Bertalanffy, H.; de Vries, J. Management of Cerebellar Infarction with Associated Occlusive Hydrocephalus. Clin. Neurol. Neurosurg. 1992, 94, 19–23. [Google Scholar] [CrossRef]
- Krieger, D.; Adams, H.P.; Rieke, K.; Hacke, W. Monitoring Therapeutic Efficacy of Decompressive Craniotomy in Space Occupying Cerebellar Infarcts Using Brain-Stem Auditory Evoked Potentials. Electroencephalogr. Clin. Neurophysiol. 1993, 88, 261–270. [Google Scholar] [CrossRef]
- Koh, M.S.; Goh, K.Y.; Tung, M.Y.; Chan, C. Is Decompressive Craniectomy for Acute Cerebral Infarction of Any Benefit? Surg. Neurol. 2000, 53, 225–230. [Google Scholar] [CrossRef]
- Baldauf, J.; Oertel, J.; Gaab, M.R.; Schroeder, H.W.S. Endoscopic Third Ventriculostomy for Occlusive Hydrocephalus Caused by Cerebellar Infarction. Neurosurgery 2006, 59, 539–544, discussion 539–544. [Google Scholar] [CrossRef]
- Kudo, H.; Kawaguchi, T.; Minami, H.; Kuwamura, K.; Miyata, M.; Kohmura, E. Controversy of Surgical Treatment for Severe Cerebellar Infarction. J. Stroke Cerebrovasc. Dis. 2007, 16, 259–262. [Google Scholar] [CrossRef]
- Yoshimura, K.; Kubo, S.; Nagashima, M.; Hasegawa, H.; Thminaga, S.; Yoshimine, T. Occlusive Hydrocephalus Associated with Cerebellar Infarction Treated with Endoscopic Third Ventriculostomy: Report of 5 Cases. Minim. Invasive Neurosurg. 2007, 50, 270–272. [Google Scholar] [CrossRef]
- Pfefferkorn, T.; Eppinger, U.; Linn, J.; Birnbaum, T.; Herzog, J.; Straube, A.; Dichgans, M.; Grau, S. Long-Term Outcome after Suboccipital Decompressive Craniectomy for Malignant Cerebellar Infarction. Stroke 2009, 40, 3045–3050. [Google Scholar] [CrossRef]
- Jüttler, E.; Schweickert, S.; Ringleb, P.A.; Huttner, H.B.; Köhrmann, M.; Aschoff, A. Long-Term Outcome after Surgical Treatment for Space-Occupying Cerebellar Infarction: Experience in 56 Patients. Stroke 2009, 40, 3060–3066. [Google Scholar] [CrossRef] [PubMed]
- Mangubat, E.Z.; Chan, M.; Ruland, S.; Roitberg, B.Z. Hydrocephalus in Posterior Fossa Lesions: Ventriculostomy and Permanent Shunt Rates by Diagnosis. Neurol. Res. 2009, 31, 668–673. [Google Scholar] [CrossRef] [PubMed]
- Vindigni, M.; Tuniz, F.; Ius, T.; Cramaro, A.; Skrap, M. Endoscopic Third Ventriculostomy in Patients with Secondary Triventricular Hydrocephalus from a Haemorrhage or Ischaemia in the Posterior Cranial Fossa. Minim. Invasive Neurosurg. 2010, 53, 106–111. [Google Scholar] [CrossRef]
- Tsitsopoulos, P.P.; Tobieson, L.; Enblad, P.; Marklund, N. Surgical Treatment of Patients with Unilateral Cerebellar Infarcts: Clinical Outcome and Prognostic Factors. Acta Neurochir. 2011, 153, 2075–2083. [Google Scholar] [CrossRef] [PubMed]
- Moussa, W.M.; Farhoud, A. Ventriculosubgaleal Shunt in the Management of Obstructive Hydrocephalus Caused by Cerebellar Infarction. Alex. J. Med. 2013, 49, 105–110. [Google Scholar] [CrossRef]
- Lee, H.M.; Kim, M.; Suh, S.-I.; Kim, J.H.; Oh, K.; Koh, S.-B.; Seo, W.-K. Lesions on DWI and the Outcome in Hyperacute Posterior Circulation Stroke. Can. J. Neurol. Sci. 2014, 41, 187–192. [Google Scholar] [CrossRef]
- Kim, M.J.; Park, S.K.; Song, J.; Oh, S.-Y.; Lim, Y.C.; Sim, S.Y.; Shin, Y.S.; Chung, J. Preventive Suboccipital Decompressive Craniectomy for Cerebellar Infarction: A Retrospective-Matched Case-Control Study. Stroke 2016, 47, 2565–2573. [Google Scholar] [CrossRef]
- Goedemans, T.; Verbaan, D.; Coert, B.A.; Kerklaan, B.J.; van den Berg, R.; Coutinho, J.M.; van Middelaar, T.; Nederkoorn, P.J.; Vandertop, W.P.; van den Munckhof, P. Neurologic Outcome After Decompressive Craniectomy: Predictors of Outcome in Different Pathologic Conditions. World Neurosurg. 2017, 105, 765–774. [Google Scholar] [CrossRef]
- Tartara, F.; Bongetta, D.; Colombo, E.V.; Bortolotti, C.; Cenzato, M.; Giombelli, E.; Gaetani, P.; Zenga, F.; Pilloni, G.; Ciccone, A.; et al. Strokectomy and Extensive Cerebrospinal Fluid Drainage for the Treatment of Space-Occupying Cerebellar Ischemic Stroke. World Neurosurg. 2018, 115, e80–e84. [Google Scholar] [CrossRef]
- Lindeskog, D.; Lilja-Cyron, A.; Kelsen, J.; Juhler, M. Long-Term Functional Outcome after Decompressive Suboccipital Craniectomy for Space-Occupying Cerebellar Infarction. Clin. Neurol. Neurosurg. 2019, 176, 47–52. [Google Scholar] [CrossRef]
- Suyama, Y.; Wakabayashi, S.; Aihara, H.; Ebiko, Y.; Kajikawa, H.; Nakahara, I. Evaluation of Clinical Significance of Decompressive Suboccipital Craniectomy on the Prognosis of Cerebellar Infarction. Fujita Med. J. 2019, 5, 21–24. [Google Scholar]
- Hernández-Durán, S.; Wolfert, C.; Rohde, V.; Mielke, D. Cerebellar Necrosectomy Instead of Suboccipital Decompression: A Suitable Alternative for Patients with Space-Occupying Cerebellar Infarction. World Neurosurg. 2020, 144, e723–e733. [Google Scholar] [CrossRef]
- Abdelbari Mattar, M.; Maher, H.; Zakaria, K.W. The Impact of Emergent Suboccipital Craniectomy upon Outcome & Prognosis of Massive Cerebellar Infarction: A Single Institutional Study. Interdiscip. Neurosurg. 2021, 25, 101223. [Google Scholar]
- Nagao, T.; Sadoshima, S.; Ibayashi, S.; Takeya, Y.; Fujishima, M. Increase in Extracranial Atherosclerotic Carotid Lesions in Patients with Brain Ischemia in Japan. An Angiographic Study. Stroke 1994, 25, 766–770. [Google Scholar] [CrossRef]
- Subramanian, G.; Silva, J.; Silver, F.L.; Fang, J.; Kapral, M.K.; Oczkowski, W.; Gould, L.; O’Donnell, M.J. Investigators of the Registry of the Canadian Stroke Network Risk Factors for Posterior Compared to Anterior Ischemic Stroke: An Observational Study of the Registry of the Canadian Stroke Network. Neuroepidemiology 2009, 33, 12–16. [Google Scholar] [CrossRef]
- Kim, J.S.; Nah, H.-W.; Park, S.M.; Kim, S.-K.; Cho, K.H.; Lee, J.; Lee, Y.-S.; Kim, J.; Ha, S.-W.; Kim, E.-G.; et al. Risk Factors and Stroke Mechanisms in Atherosclerotic Stroke: Intracranial Compared with Extracranial and Anterior Compared with Posterior Circulation Disease. Stroke 2012, 43, 3313–3318. [Google Scholar] [CrossRef]
- van der Worp, H.B.; Hofmeijer, J.; Jüttler, E.; Lal, A.; Michel, P.; Santalucia, P.; Schönenberger, S.; Steiner, T.; Thomalla, G. European Stroke Organisation (ESO) Guidelines on the Management of Space-Occupying Brain Infarction. Eur. Stroke J. 2021, 6, XC–CX. [Google Scholar] [CrossRef]


| Author and Year | Raco et al., 2003 [22] | Mathew et al., 1995 [20] | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only |
| Number, n (%) | 8 (18%) | 4 (9.1%) | 0 | 5 (11%) | Treatment-limiting decision: 2 (4.5%) | 25 (57%) | 7 (14%) | 2 (4%) | 0 | 0 | Treatment-limiting decision: 3 (6%) Management change: 4 (8%) | 34 (68%) |
| Comorbidities | Recent cardiac infarction: 6 Atrial flutter: 2 Endocarditis with vegetations: 2 Patent foramen ovale: 1 | Unreported | ||||||||||
| Radiological findings | Presence of hydrocephalus | Presence of hydrocephalus | ||||||||||
| 8 | 0 | 0 | 5 | 0 | 0 | Total: 19 | ||||||
| Presence of brainstem compression | Presence of brainstem compression | |||||||||||
| Unreported | Total: 26 | |||||||||||
| Male, n (%) | 24 (55%) | Unreported | ||||||||||
| Age in years ± SD (range) | Median: 56 (9–83) | Mean: 57 (26–85) | ||||||||||
| GCS on admission | GCS 3: 2 GCS 6: 2 GCS 9–12: 15 GCS 13: 15 GCS 14: 7 GCS 15: 3 | Median: 14 (4–15) | ||||||||||
| Good functional outcome, n (%) | 8 (18%) | 1 (2.3%) | - | 4 (9.1%) | 0 | 24 (55%) | 6 (12%) | 1 (2%) | - | - | Management change: 2 (4%) | 34 (68%) |
| Death, n (%) | 0 | 2 (4.5%) | - | 1 (2.3%) | Treatment-limiting decision: 2 (4.5%) | 1 (2.3%) | 1 (2%) | 1 (2%) | - | - | Treatment-limiting decision: 3 (6%) Management change: 2 (4%) | 0 |
| Author and Year | Hornig et al., 1994 [19] | Jauss et al., 1992 [18] | ||||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only |
| Number, n (%) | 2 (3.8%) | 0 | 8 (15%) | 4 (7.7%) | SDC + EVD + necrosectomy: 22 (42%) | 16 (31%) | 14 (17%) | 30 (36%) | 0 | 4 (4.8%) | 0 | 36 (43%) |
| Comorbidities | Arterial hypertension: 33 Diabetes: 21 Hypercholesterolemia: 5 Unilateral/bilateral vertebral artery stenosis: 10 Unilateral/bilateral vertebral artery occlusion: 2 Nonrheumatic atrial fibrillation: 14 Myocardial infarction: 3 | Unreported | ||||||||||
| Radiological findings | Presence of hydrocephalus | Presence of hydrocephalus | ||||||||||
| Total: 42 | Unreported | |||||||||||
| Presence of brainstem compression | Presence of brainstem compression | |||||||||||
| Total: 39 | Unreported | |||||||||||
| Age in years ± SD (range) | Mean: 61.2 ± 10.1 | Mean: 54.5 ± 17.3 | Mean: 57.4 ± 12 | - | - | - | Mean: 61.2 ± 10.3 | |||||
| GCS on admission | Unreported | Unreported | ||||||||||
| Good functional outcome, n (%) | 18 (35%) | 11 (21%) | 10 (12%) | 22 (26%) | - | - | - | 30 (36%) | ||||
| Death, n (%) | 6 (12%) | 2 (3.8%) | unreported | |||||||||
| Author and Year | Mostofi, 2013 [23] | Koh et al., 2000 [28] | ||||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only |
| Number, n (%) | 6 (11%) | 16 (30%) | 0 | 3 (5.7%) | 0 | 28 (53%) | 6 (17%) | 2 (5.7%) | 0 | 1 (2.9%) | 0 | 26 (74%) (2 patients with treatment limiting decision) |
| Comorbidities | Unreported | Large artery disease: 13 Cardioembolism: 12 | ||||||||||
| Radiological findings | Presence of hydrocephalus | Presence of hydrocephalus | ||||||||||
| Unreported | Total among surgical group: 9 | 6 | ||||||||||
| Presence of brainstem compression | Presence of brainstem compression | |||||||||||
| Unreported | Total among surgical group: 7 | 2 | ||||||||||
| Male, n (%) | 32 (60%) | Unreported | ||||||||||
| Age in years ± SD (range) | Mean: 58.7 (SD unreported) | Unreported | ||||||||||
| GCS on admission | Mean: 9.5 | Mean: 9.43 | - | Mean: 6 | - | Mean: 11.6 | Unreported | |||||
| Good functional outcome, n (%) | unreported | 2 (5.7%) | 0 | - | 0 | - | 14 (40%) | |||||
| Death, n (%) | 2 (3.8%) | 4 (7.5%) | 0 | 1 (2.9%) | ||||||||
| Author and Year | Taneda et al., 1982 [17] | Taylor et al., 2020 [24] | ||||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | Medical Only |
| Number, n (%) | 0 | 10 (67%) | 0 | 0 | 0 | 5 (20%) | 2 (2.3%) | 0 | 12 (14%) | 9 (10%) | 0 | 65 (76%) |
| Comorbidities | Unreported | Obese, BMI ≥ 30: 37 Hypertension: 63 Diabetes: 37 Coronary artery disease: 21 Congestive heart failure: 16 Prior cerebrovascular accident: 16 Chronic kidney disease: 8 Alcohol abuse: 22 Tobacco abuse: 23 Hyperlipidemia: 35 | ||||||||||
| Radiological findings | Presence of hydrocephalus | Presence of hydrocephalus | ||||||||||
| Total: 15 | Total among surgical group: 11 | 5 | ||||||||||
| Presence of brainstem compression | Presence of brainstem compression | |||||||||||
| Unreported | Total among surgical group: 10 | 8 | ||||||||||
| Male, n (%) | - | 9 (60%) | - | - | - | 4 (27%) | 12 (14%) | 41 (48%) | ||||
| Age in years ± SD (range) | - | Mean: 55.1 (40–66) | - | - | - | Mean: 67.6 (41–80) | Median: 58.5 IQR: 52–65 | |||||
| GCS on admission | - | unreported | - | - | - | unreported | Median: 14 (IQR: 10–15) | Median: 15 (IQR: 10–15) | ||||
| Good functional outcome, n (%) | - | 7 (47%) | - | - | - | 0 | - | - | - | - | - | - |
| Death, n (%) | - | 1 (6.7%) | - | - | - | 5 (20%) | 4 (4.7%) | 16 (19%) | ||||
| Author and Year | Tsitsopoulos et al., 2010 [36] | Baldauf et al., 2006 [29] | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 0 | 0 | 10 (100%) | 0 | 0 | 0 | 0 | 0 | ETV: 7 (70%) ETV + EVD: 2 (20%) ETV + SDC: 1 (10%) |
| Male, n (%) | - | - | - | 8 (80%) | - | - | - | - | - | 6 (60%) |
| Age in years ± SD (range) | - | - | - | Mean: 54.9 ± 13 | - | - | - | - | - | Mean: 61.8 (SD unreported) |
| GCS on admission | - | - | - | Mean: 12.3 ± 3.1 | - | - | - | - | - | Mean: 11.2 (SD unreported) |
| Good functional outcome, n (%) | - | - | - | 6 (60%) | - | - | - | - | - | unreported |
| Death, n (%) | - | - | - | 1 (10%) | - | - | - | - | - | 0 |
| Author and Year | Koh et al., 2000 [21] | Pfefferkorn et al., 2009 [32] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 3 (100%) | 0 | 0 | 0 | 47 (82%) | 57 (100%) | 0 | 0 | Infarct evacuation: 32/57 (56%) |
| Male, n (%) | - | 1 (33%) | - | - | - | - | 34 | - | - | - |
| Age in years ± SD (range) | - | Mean: 53.6 (SD unreported) | - | - | - | - | Mean: 59.2 ± 12.9 | - | - | - |
| GCS on admission | - | Mean: 12.3 (SD unreported) | - | - | - | - | unreported | - | - | - |
| Good functional outcome, n (%) | - | 2 (66%) | - | - | - | - | 27 (47%) | - | - | - |
| Death, n (%) | - | 1 (33%) | - | - | - | - | 16 (28%) | - | - | - |
| Author and Year | Jüttler et al., 2009 [33] | Lee et al., 2020 [10] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 9 (16%) | - | 8 (14%) | 39 (70%) | 0 | 0 | 0 | 0 | 50 (100%) | 0 |
| Male, n (%) | 37 (66%) | - | - | - | 38 (76%) | - | ||||
| Age in years ± SD (range) | Median: 60 (30–76) | - | - | - | Mean: 57.3 ± 12 | - | ||||
| GCS on admission | Median: 14.5 (3–15) | - | - | - | Unreported | - | ||||
| Good functional outcome, n (%) | 4 (7.1%) | - | 4 (7.1%) | 12 (21%) | - | - | - | - | 30 (60%) | - |
| Death, n (%) | 2 (3.6%) | - | 1 (1.8%) | 9 (16%) | - | - | - | - | 21 (42%) | - |
| Author and Year | Tsitsopoulos et al., 2011 [13] | Chen et al., 1992 [25] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 0 | 0 | 32 (100%) | 0 | 0 | 0 | 0 | 2 (18%) | SDC + EVD + necrosectomy: 9 (82%) |
| Male, n (%) | - | - | - | 24 (75%) | - | - | - | - | 7 (64%) | |
| Age in years ± SD (range) | - | - | - | 64.3 ± 9.9 | - | - | - | - | Mean: 54 (36–73) | |
| GCS on admission | - | - | - | Median: 12.2 (7–15) | - | - | - | - | Mean: 12.9 | |
| Good functional outcome, n (%) | - | - | - | 19 (59%) | - | - | - | - | 2 (18%) | |
| Death, n (%) | - | - | - | 10 (31%) | - | - | - | - | 0 | |
| Author and Year | Moussa et al., 2013 [37] | Tartara et al., 2018 [41] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 5 (50%) | 0 | 5 (50%) | 0 | 0 | 2 (18%) | 0 | 9 (82%) | 0 |
| Male, n (%) | 7 (70%) | 6 (55%) | ||||||||
| Age in years ± SD (range) | 15 ≤ Age < 30 years: 6 30 ≤ Age < 45 years: 3 Age ≥ 45 years: 1 | Mean: 64.7 ± 9.1 | ||||||||
| GCS on admission | GCS 3–9 n = 5 GCS 10–12 n = 3 GCS 13–15 n = 2 | Mean: 13.6 ± 1.1 | ||||||||
| Good functional outcome, n (%) | Unreported | - | 2 (18%) | - | 7 (64%) | - | ||||
| Death, n (%) | - | 2 (20%) | - | 0 | - | - | 0 | - | 1 (9.1%) | - |
| Author and Year | Kudo et al., 2007 [30] | Krieger et al., 1993 [27] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 3 (12%) | 2 (8%) | 0 | 3 (12%) | EVD + necrosectomy: 14 (56%) Necrosectomy only: 3 (12%) | 0 | 0 | 0 | 11 (100%) | 0 |
| Male, n (%) | 21 (84%) | - | - | - | 8 (73%) | - | ||||
| Age in years ± SD (range) | Mean age Group A: 72 ± 6 Group B: 61 ± 15 | - | - | - | Mean: 52 (30–69) | - | ||||
| GCS on admission | Unreported | - | - | - | Unreported | - | ||||
| Good functional outcome, n (%) | 11 (44%) | - | - | - | Unreported | - | ||||
| Death, n (%) | 3 (12%) | - | - | - | 4 (36%) | - | ||||
| Author and Year | Suyama et al., 2019 [43] | Lindeskog et al., 2018 [42] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 5 (36%) | 0 | 9 (64%) | 0 | 0 | 0 | 0 | 22 (100%) | 0 |
| Male, n (%) | 12(86%) | - | - | - | 16 (73%) | - | ||||
| Age in years ± SD (range) | Mean: 65 ± 12 | - | - | - | Median: 53 (IQR: 45–62) | - | ||||
| GCS on admission | Unreported | - | - | - | Median: 8 (IQR: 5–10) | - | ||||
| Good functional outcome, n (%) | 10 (71%) | - | - | - | 12 (55%) | - | ||||
| Death, n (%) | 2 (14%) | - | - | - | 7 (32%) | - | ||||
| Author and Year | Mattar et al., 2021 [45] | Hernández-Durán, 2020 [44] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 42 (100%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | Necrosectomy only: 34 (100%) |
| Male, n (%) | - | 36 (86%) | - | - | - | - | - | - | - | 18 (53%) |
| Age in years ± SD (range) | - | Mean: 66 ± 13 | - | - | - | - | - | - | - | Median: 70 (28–84) |
| GCS on admission | - | Unreported | - | - | - | - | - | - | - | Median: 11 (3–15) |
| Good functional outcome, n (%) | - | 25 (60%) | - | - | - | - | - | - | - | 26 (76%) |
| Death, n (%) | - | 6 (14%) | - | - | - | - | - | - | - | 7 (21%) |
| Author and Year | Goedemans et al., 2017 [40] | Yoshimura et al., 2007 [31] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 10 (100%) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | ETV: 5 (100%) |
| Male, n (%) | Unreported | - | - | - | - | 3 (60%) | ||||
| Age in years ± SD (range) | Unreported | - | - | - | - | Mean: 71.8 (47–92) | ||||
| GCS on admission | Unreported | - | - | - | - | Mean: 12.8 (8–15) | ||||
| Good functional outcome, n (%) | - | - | 5 (50%) | - | - | - | - | - | - | 3 (60%) |
| Death, n (%) | - | - | Unreported | - | - | - | - | - | - | 1 (20%) |
| Author and Year | Lee et al., 2014 [38] | Mangubat et al., 2009 [34] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 0 | 9 (100%) | 0 | 0 | 0 | 4 (100%) | 0 | 0 | 0 | 0 |
| Male, n (%) | - | Unreported | - | - | - | Unreported | - | - | - | - |
| Age in years ± SD (range) | - | Unreported | - | - | - | Unreported | - | - | - | - |
| GCS on admission | - | Unreported | - | - | - | Unreported | - | - | - | - |
| Good functional outcome, n (%) | - | 2 (22%) | - | - | - | Unreported | - | - | - | - |
| Death, n (%) | - | Unreported | - | - | - | 4 (100%) | - | - | - | - |
| Author and Year | Vindigni et al., 2010 [35] | Bertalanffy et al., 1992 [26] | ||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others |
| Number, n (%) | 12 (63%) | 0 | 0 | 0 | ETV: 7 (37%) | 6 (60%) | 0 | 0 | 0 | Ventriculo–arterial shunt: 3 (30%) Ventriculo–peritoneal shunt: 1 (10%) |
| Male, n (%) | Unretrievable | 2 (20%) | - | - | - | Ventriculo–arterial shunt: 1 (10%) Ventriculo–peritoneal shunt: 1 (10%) | ||||
| Age in years ± SD (range) | Mean: 62.3 (52–73) | - | - | - | Mean: 50.4 (23–67) | Mean: 61.8 (SD unreported) | ||||
| GCS on admission | Unreported | Unreported | ||||||||
| Good functional outcome, n (%) | 6 (32%) | - | - | - | 3 (16%) | Unreported | ||||
| Death, n (%) | 1 (5.3%) | - | - | - | 1 (5.3%) | 1 (10%) | - | - | - | Ventriculo–arterial shunt: 1 (10%) Ventriculo–peritoneal shunt: 1 (10%) |
| Author and Year | Kim et al., 2016 [39] | |||||||||
| Treatment Groups | EVD Only | SDC Only | SDC with Necrosectomy Only | SDC and EVD | Others | |||||
| Number, n (%) | 0 | 84 (100%) | 0 | 0 | 0 | |||||
| Male, n (%) | 0 | 52 (62%) | - | - | - | |||||
| Age in years ± SD (range) | - | Mean age Preventive SDC group: 59.0 ± 11.6 Non-preventive SDC group: 59.4 ± 10.9 | - | - | - | |||||
| GCS on admission | - | Mean GCS Preventive SDC group: 12.1 ± 4.1 Non-preventive SDC group: 12.0 ± 3.8 | - | - | - | |||||
| Good functional outcome, n (%) | - | 45 (54%) | - | - | - | |||||
| Death, n (%) | - | 6 (7.1%) | - | - | - | |||||
| Study | Number of Patients | Number of Deaths | Mean Age (Years) | Mean Pre-Operative GCS | Proportion of Good Functional Outcome (%) | Proportion of Patients with Hypertension (%) | Proportion of Patients with Diabetes Mellitus (%) | Proportion of Patients with Dyslipidemia (%) | Proportion of Patients with Atrial Fibrillation (%) | Proportion of Patients with Heart Disease * (%) | Proportion of Patients with Previous Stroke (%) | Proportion of Patients with Bilateral Stroke (%) | Proportion of Patients with Hydrocephalus (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baldauf et al., 2006 [29] | 10 | 0 | 61.8 | 11.2 | NA | 50 | NA | NA | 70 | NA | NA | NA | 100 |
| Bertalanffy et al., 1992 [26] | 10 | 3 | 61.8 | NA | NA | NA | NA | NA | NA | NA | NA | NA | 100 |
| Chen et al., 1992 [25] | 11 | 0 | 54 | 6.27 | 2 | 27.3 | NA | NA | NA | NA | NA | 27.3 | NA |
| Goedemans et al., 2017 [40] | 10 | NA | NA | NA | 5 | NA | NA | NA | NA | NA | NA | NA | NA |
| Hernández-Durán et al., 2020 [44] | 34 | 7 | 70 | 7.5 | 26 | NA | NA | NA | NA | NA | NA | 26.5 | 55.9 |
| Hornig et al., 1994 [19] | 36 | 6 | NA | NA | 18 | NA | NA | NA | NA | NA | NA | NA | NA |
| Jauss et al., 1992 [18] | 48 | NA | 56.55 | NA | 32 | NA | NA | NA | NA | NA | NA | NA | NA |
| Jüttler et al., 2009 [33] | 56 | 14 | 60 | 13 | 20 | NA | NA | NA | NA | NA | NA | 14.3 | NA |
| Kim et al., 2016 [39] | 84 | 6 | 59.27 | NA | 45 | 40.5 | 34.5 | 25 | 41.7 | 3.57 | 13.1 | 42.9 | NA |
| Koh et al., 2000 [21] | 9 | 0 | NA | NA | 2 | NA | NA | NA | NA | NA | NA | NA | 100 |
| Koh et al., 2000 [28] | 3 | 1 | 53.57 | 4 | 2 | NA | NA | NA | NA | NA | NA | 0 | NA |
| Krieger et al., 1993 [27] | 11 | 4 | 52 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Kudo et al., 2007 [30] | 25 | 3 | 63 | 6.4 | 11 | NA | NA | NA | NA | NA | NA | NA | NA |
| Lee et al., 2014 [38] | 9 | NA | NA | NA | 2 | NA | NA | NA | NA | NA | NA | NA | NA |
| Lee et al., 2020 [10] | 50 | 21 | 57.3 | NA | 30 | NA | NA | NA | NA | NA | NA | 48 | NA |
| Lindeskog et al., 2019 [42] | 22 | 7 | 53 | 8 | 12 | 18.2 | 4.55 | 13.6 | 9.09 | 4.55 | NA | 27.3 | NA |
| Mangubat et al., 2009 [34] | 4 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Mathew et al., 1995 [20] | 16 | 7 | NA | NA | 9 | NA | NA | NA | NA | NA | NA | NA | NA |
| Mattar et al., 2021 [45] | 42 | 6 | 66 | NA | 25 | NA | NA | NA | NA | NA | NA | 21.4 | 73.8 |
| Mostofi et al., 2013 [23] | 25 | 2 | 59.67 | 5.33 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Moussa et al., 2013 [37] | 10 | 2 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Pfefferkorn et al., 2009 [32] | 57 | 16 | 59.2 | NA | 27 | 80 | 32 | 30 | NA | NA | NA | 37 | NA |
| Raco et al., 2003 [22] | 19 | 5 | NA | NA | 13 | NA | NA | NA | NA | NA | NA | NA | NA |
| Suyama et al., 2019 [43] | 14 | 2 | 65 | NA | 10 | 35.7 | 7.14 | NA | 14.3 | 14.3 | 21.4 | 57.1 | 85.7 |
| Taneda et al., 1982 [17] | 10 | 1 | 55.1 | NA | 7 | NA | NA | NA | NA | NA | NA | 0 | NA |
| Tartara et al., 2018 [41] | 11 | 1 | 64.7 | 9.27 | 9 | NA | NA | NA | NA | NA | NA | 18.2 | NA |
| Taylor et al., 2020 [24] | 21 | 4 | 55 | 10 | NA | 71.4 | 52.4 | 47.6 | NA | 28.6 | 28.6 | 33.3 | 52.4 |
| Tsitsopoulos et al., 2011 [13] | 10 | 1 | 54.9 | 8.9 | 6 | 20 | 10 | 10 | 20 | 10 | NA | 50 | 70 |
| Tsitsopoulos et al., 2011 [36] | 32 | 10 | 64.3 | 9 | 19 | 46.9 | 18.8 | NA | 18.8 | 15.6 | NA | 25 | 90.6 |
| Vindigni et al., 2010 [35] | 19 | 2 | 50.4 | NA | 9 | 31.6 | NA | NA | 36.8 | NA | NA | 0 | NA |
| Yoshimura et al., 2007 [31] | 5 | 1 | 71.8 | 9.8 | 3 | NA | NA | NA | 20 | NA | NA | 20 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, N.-A.; Lin, H.-Y.; Tan, C.H.; Ho, A.F.W.; Yeo, T.T.; Nga, V.D.W.; Tan, B.Y.Q.; Lim, M.J.R.; Yeo, L.L.L. Functional and Mortality Outcomes with Medical and Surgical Therapy in Malignant Posterior Circulation Infarcts: A Systematic Review. J. Clin. Med. 2023, 12, 3185. https://doi.org/10.3390/jcm12093185
Lim N-A, Lin H-Y, Tan CH, Ho AFW, Yeo TT, Nga VDW, Tan BYQ, Lim MJR, Yeo LLL. Functional and Mortality Outcomes with Medical and Surgical Therapy in Malignant Posterior Circulation Infarcts: A Systematic Review. Journal of Clinical Medicine. 2023; 12(9):3185. https://doi.org/10.3390/jcm12093185
Chicago/Turabian StyleLim, Nicole-Ann, Hong-Yi Lin, Choon Han Tan, Andrew F. W. Ho, Tseng Tsai Yeo, Vincent Diong Weng Nga, Benjamin Y. Q. Tan, Mervyn J. R. Lim, and Leonard L. L. Yeo. 2023. "Functional and Mortality Outcomes with Medical and Surgical Therapy in Malignant Posterior Circulation Infarcts: A Systematic Review" Journal of Clinical Medicine 12, no. 9: 3185. https://doi.org/10.3390/jcm12093185
APA StyleLim, N.-A., Lin, H.-Y., Tan, C. H., Ho, A. F. W., Yeo, T. T., Nga, V. D. W., Tan, B. Y. Q., Lim, M. J. R., & Yeo, L. L. L. (2023). Functional and Mortality Outcomes with Medical and Surgical Therapy in Malignant Posterior Circulation Infarcts: A Systematic Review. Journal of Clinical Medicine, 12(9), 3185. https://doi.org/10.3390/jcm12093185