
Advances in Canaloplasty—Modified Techniques Yield Strong Pressure Reduction with Low Risk Profile

Abstract
1. Introduction
2. Development and Rationale of Canaloplasty
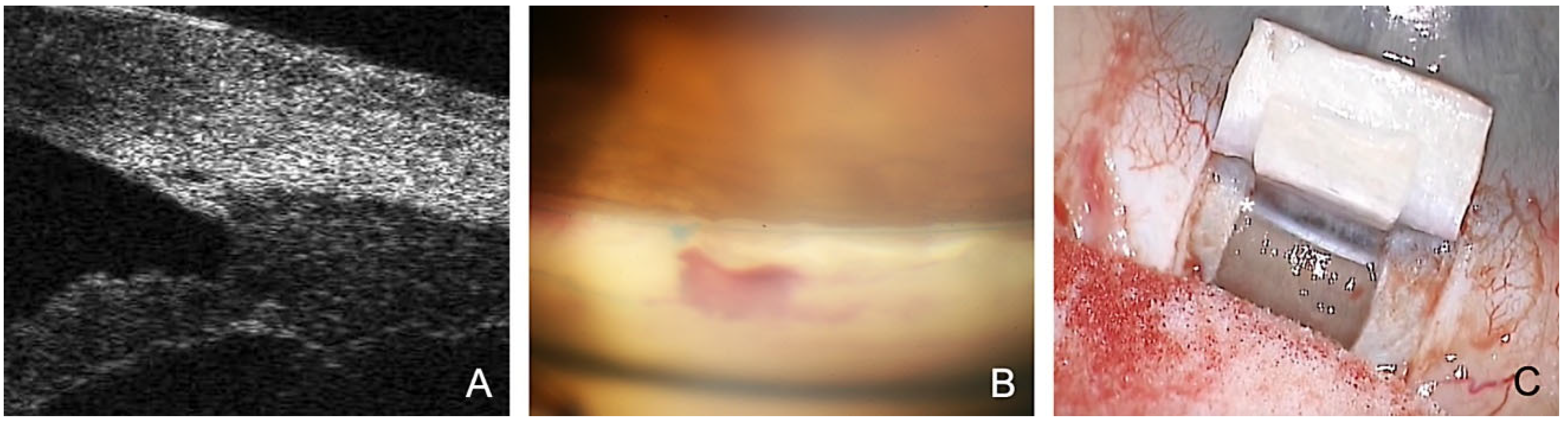
- The SC is probed using a microcatheter (iTrack 250, Ellex Inc., Eden Prairie, MN, USA) for dilatation of the ostia and lumen of SC, and the adjacent collector channels using a viscoelastic. This effect dilates the canal to almost triple its original size, making it easily visible in the ultrasound biomicroscope (UBM) 50 MHz (Figure 1A).
- Applying tension to the TDW results in the controlled percolation of aqueous humor into the intrascleral cleft formed after resection of the deep flap, which can be enhanced by YAG goniopuncture [13].
3. Surgical Technique of Conventional Canaloplasty
4. Spectrum of Severe Glaucomas Treated Using Canaloplasty
5. Results of Conventional Canaloplasty
6. Rationale for Modification of Canaloplasty
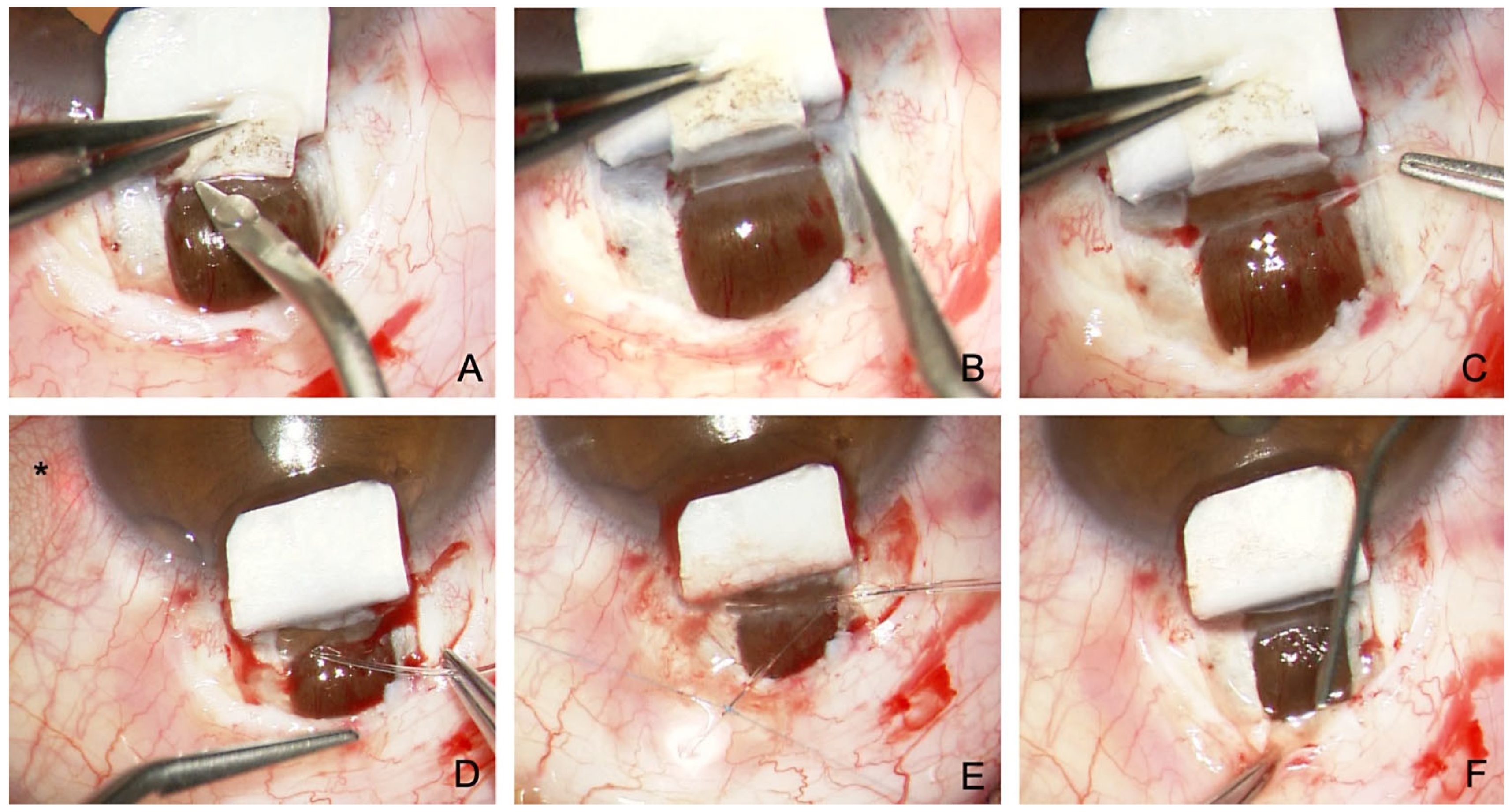
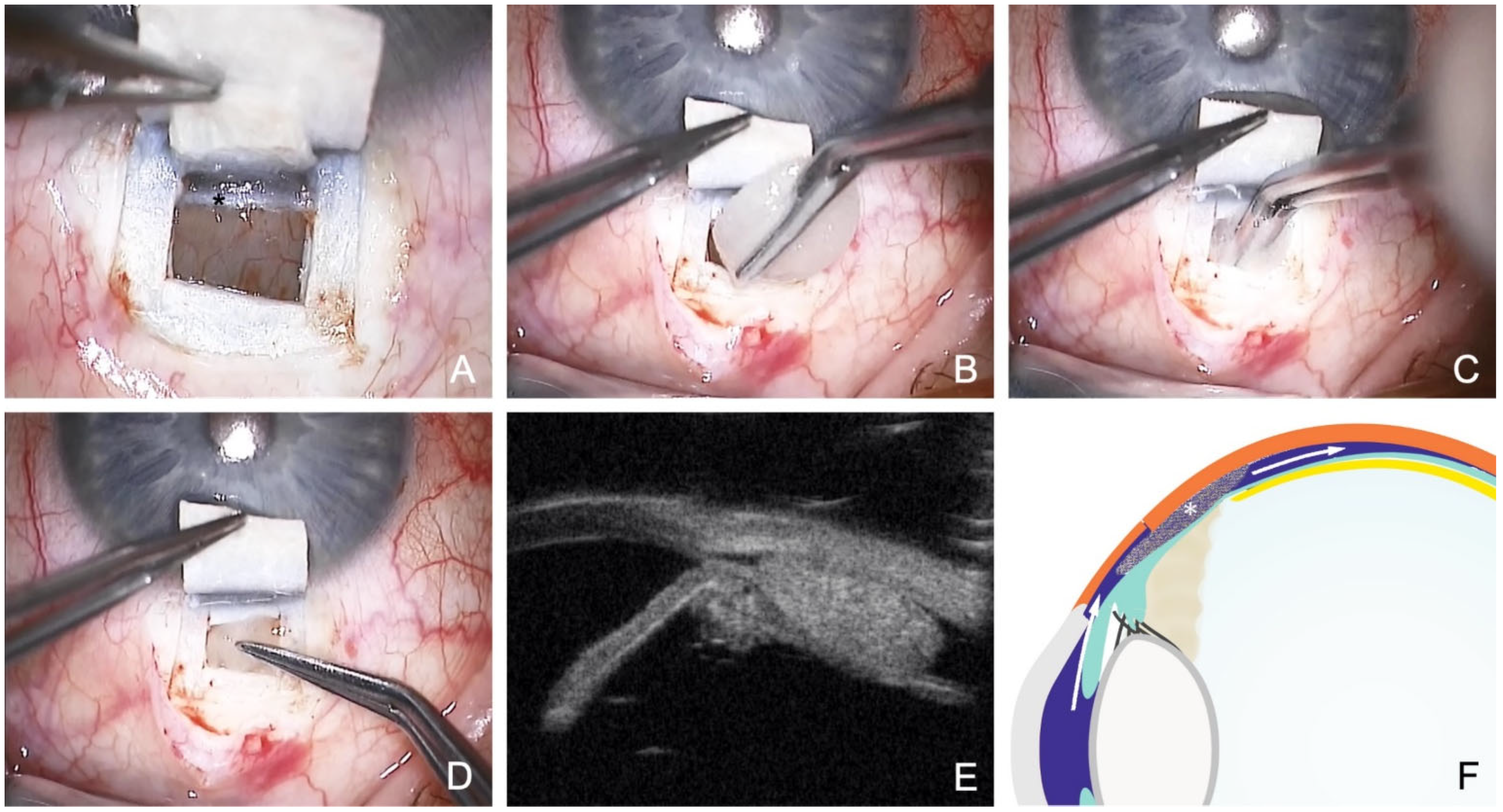
7. Canaloplasty Combined with Suprachoroidal Drainage
8. Canaloplasty with ScD and Suprachoroidal Collagen Implant
9. Phacocanaloplasty with ScD
10. “Filtering” Canaloplasty with Bleb Formation
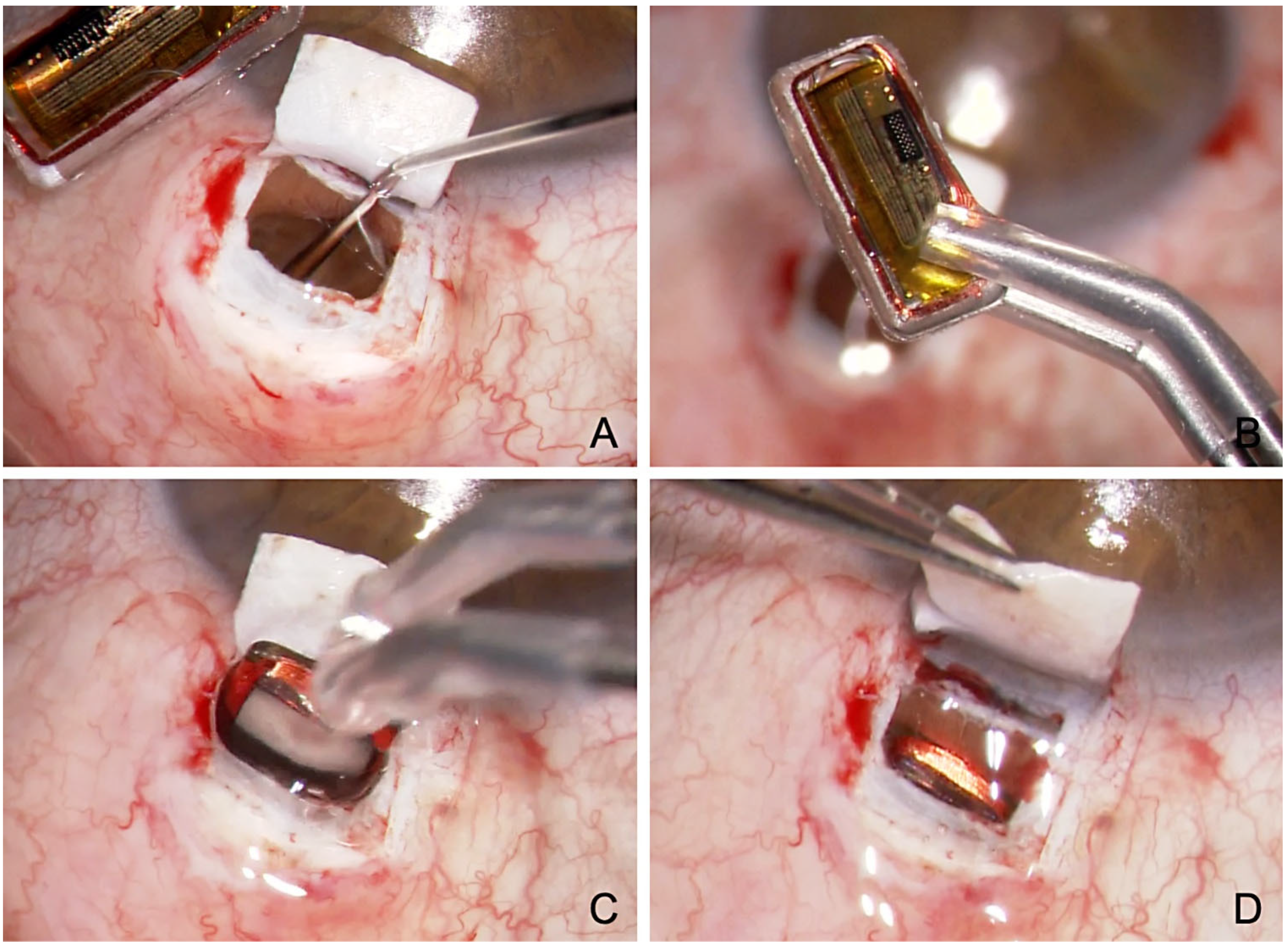
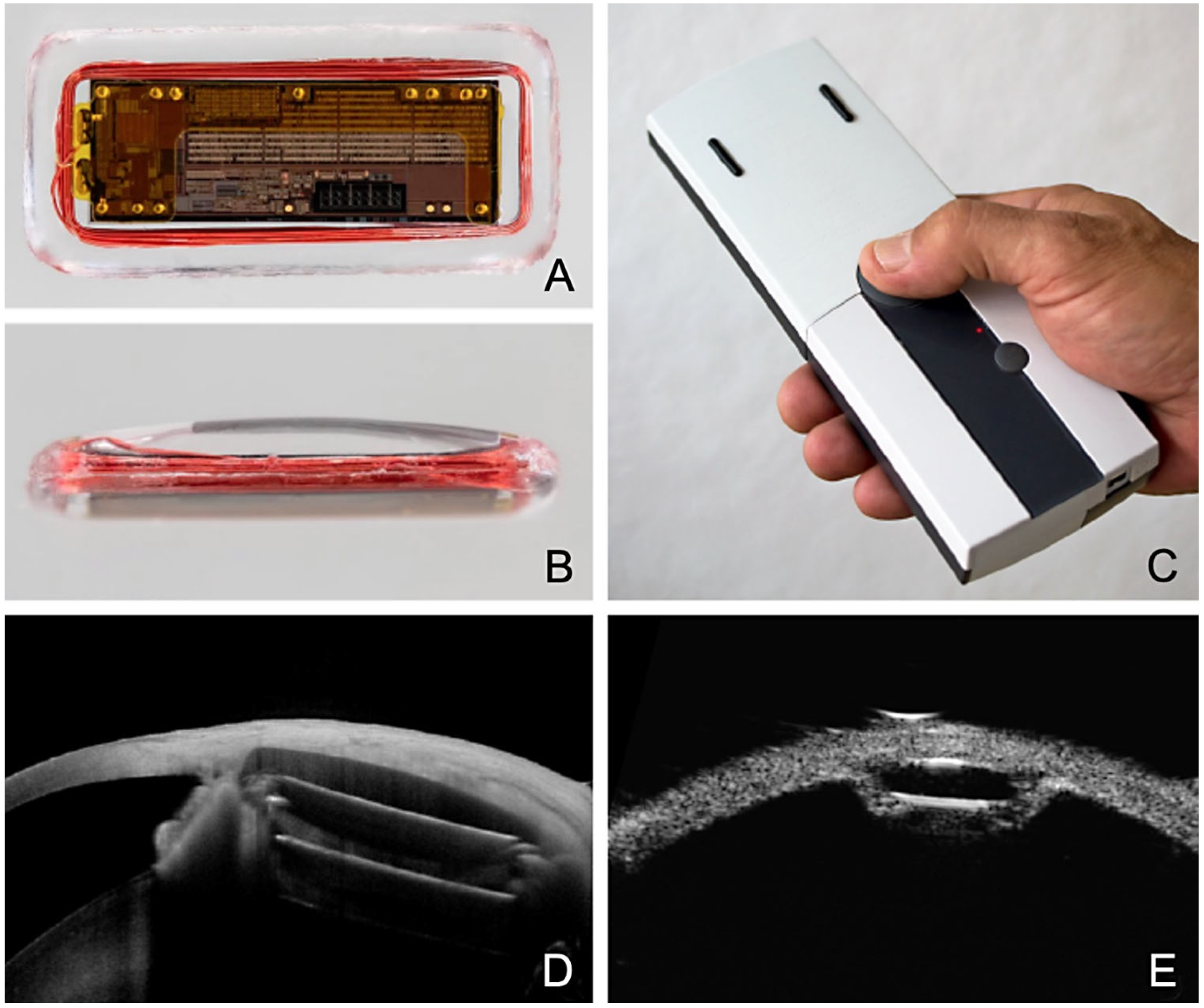
11. Canaloplasty with ScD and Suprachoroidal Eyemate-SC IOP Sensor
12. Disadvantages of Modified Canaloplasty
13. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jampel, H.D.; Musch, D.C.; Gillespie, B.W.; Lichter, P.R.; Wright, M.M.; Guire, K.E.; Collaborative Initial Glaucoma Treatment Study Group. Perioperative complications of trabeculectomy in the collaborative initial glaucoma treatment study (CIGTS). Am. J. Ophthalmol. 2005, 140, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, K.; Schwartz, S.G.; Kishor, K.S.; Fortun, J.A.; Moshfeghi, D.M.; Moshfeghi, A.A.; Flynn, H.W., Jr. Incidence of postoperative suprachoroidal hemorrhage after glaucoma filtration surgeries in the United States. Clin. Ophthalmol. 2015, 9, 579–584. [Google Scholar]
- Patel, H.Y.; Danesh-Meyer, H.V. Incidence and management of cataract after glaucoma surgery. Curr. Opin. Ophthalmol. 2013, 24, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Sawada, A.; Mayama, C.; Araie, M.; Ohkubo, S.; Sugiyama, K.; Kuwayama, Y.; Collaborative Bleb-Related Infection Incidence and Treatment Study Group. The 5-year incidence of bleb-related infection and its risk factors after filtering surgeries with adjunctive mitomycin C: Collaborative bleb-related infection incidence and treatment study 2. Ophthalmology 2014, 121, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Rulli, E.; Biagioli, E.; Riva, I.; Gambirasio, G.; De Simone, I.; Floriani, I.; Quaranta, L. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: A systematic review and meta-analysis. JAMA Ophthalmol. 2013, 131, 1573–1582. [Google Scholar] [CrossRef]
- Kim, E.A.; Law, S.K.; Coleman, A.L.; Nouri-Mahdavi, K.; Giaconi, J.A.; Yu, F.; Lee, J.W.; Caprioli, J. Long-Term Bleb-Related Infections After Trabeculectomy: Incidence, Risk Factors, and Influence of Bleb Revision. Am. J. Ophthalmol. 2015, 159, 1082–1091. [Google Scholar] [CrossRef]
- Thederan, L.; Grehn, F.; Klink, T. Comparison of canaloplasty with trabeculectomy. Klin. Monbl. Augenheilkd. 2014, 231, 256–261. [Google Scholar]
- Ayyala, R.S.; Chaudhry, A.L.; Okogbaa, C.B.; Zurakowski, D. Comparison of surgical outcomes between canaloplasty and trabeculectomy at 12 months’ follow-up. Ophthalmology 2011, 118, 2427–2433. [Google Scholar] [CrossRef]
- Eldaly, M.A.; Bunce, C.; Elsheikha, O.Z.; Wormald, R. Non-penetrating filtration surgery versus trabeculectomy for open-angle glaucoma. Cochrane Database Syst. Rev. 2014, 15, CD007059. [Google Scholar] [CrossRef]
- Fyodorov, S. Non penetrating deep sclerectomy in open-angle glaucoma. Eye Microsurg. 1989, 2, 52–55. [Google Scholar]
- Stegmann, R.; Pienaar, A.; Miller, D. Viscocanalostomy for open-angle glaucoma in black African patients. J. Cataract. Refract. Surg. 1999, 25, 316–322. [Google Scholar] [CrossRef]
- Cameron, B.; Field, M.; Ball, S.; Kearney, J. Circumferential viscodilation of Schlemm’s canal with a flexible microcannula during non-penetrating glaucoma surgery. Digit. J. Ophthalmol. 2006, 12, 1. [Google Scholar]
- Tam, D.Y.; Barnebey, H.S.; Ahmed, I.I. Nd: YAG laser goniopuncture: Indications and procedure. J. Glaucoma 2013, 22, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Brusini, P. Canaloplasty in open-angle glaucoma surgery: A four-year follow-up. Sci. World J. 2014, 2014, 469609. [Google Scholar]
- Brusini, P.; Tosoni, C.; Zeppieri, M. Canaloplasty in corticosteroid-induced glaucoma. Preliminary results. J. Clin. Med. 2018, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Lommatzsch, C.; Heinz, C.; Heiligenhaus, A.; Koch, J.M. Canaloplasty in patients with uveitic glaucoma: A pilot study. Graefes. Arch. Clin. Exp. Ophthalmol. 2016, 254, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Seuthe, A.M.; Szurman, P.; Januschowski, K. Canaloplasty with Suprachoroidal Drainage in Patients with Pseudoexfoliation Glaucoma—Four Years Results. Curr. Eye Res. 2021, 46, 217–223. [Google Scholar] [CrossRef]
- Riva, I.; Brusini, P.; Oddone, F.; Michelessi, M.; Weinreb, R.N.; Quaranta, L. Canaloplasty in the Treatment of Open-Angle Glaucoma: A Review of Patient Selection and Outcomes. Adv. Ther. 2019, 36, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.B.; Parrish, R.K., II; Feuer, W.F. 2002 survey of the American Glaucoma Society: Practice preferences for glaucoma surgery and antifibrotic use. J. Glaucoma 2005, 14, 172–174. [Google Scholar] [CrossRef]
- Lin, Z.J.; Xu, S.; Huang, S.Y.; Zhang, X.B.; Zhong, Y.S. Comparison of canaloplasty and trabeculectomy for open angle glaucoma: A Meta-analysis. Int. J. Ophthalmol. 2016, 9, 1814–1819. [Google Scholar]
- Seuthe, A.M.; Jung, S.; Januschowski, K.; Szurman, P. Predictive factors for the IOP reduction in phacocanaloplasty with suprachoroidal drainage. Int. Ophthalmol. 2020, 40, 1897–1903. [Google Scholar] [PubMed]
- Szurman, P.; Klabe, K. Modifications of canaloplasty: Strong pressure-lowering effect with a low risk profile. Ophthalmologie 2022, 119, 989–999. [Google Scholar] [CrossRef] [PubMed]
- Matlach, J.; Dhillon, C.; Hain, J.; Schlunck, G.; Grehn, F.; Klink, T. Trabeculectomy versus canaloplasty (TVC study) in the treatment of patients with open-angle glaucoma: A prospective randomized clinical trial. Acta Ophthalmol. 2015, 93, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Seuthe, A.M.; Ivanescu, C.; Leers, S.; Boden, K.; Januschowski, K.; Szurman, P. Modified canaloplasty with suprachoroidal drainage versus conventional canaloplasty-1-year results. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 1591–1597. [Google Scholar] [PubMed]
- Erokhina, M.; Seuthe, A.M.; Szurman, P.; Haus, A. One Year Results of PRESERFLOTM MicroShunt Implantation for Refractory Glaucoma. J. Glaucoma 2022, in press. [Google Scholar]
- Gedde, S.J.; Schiffman, J.C.; Feuer, W.J.; Herndon, L.W.; Brandt, J.D.; Budenz, D.L.; Tube versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am. J. Ophthalmol. 2012, 153, 789–803. [Google Scholar]
- Brusini, P.; Tosoni, C. Canaloplasty after failed trabeculectomy: A possible option. J. Glaucoma 2014, 23, 33–34. [Google Scholar] [CrossRef]
- Korber, N. Canaloplasty after trabeculectomy. Ophthalmologe 2015, 112, 332–336. [Google Scholar]
- Xin, C.; Chen, X.; Shi, Y.; Li, M.; Wang, H.; Wang, N. One-year interim comparison of canaloplasty in primary open-angle glaucoma following failed filtering surgery with primary canaloplasty. Br. J. Ophthalmol. 2016, 100, 1692–1696. [Google Scholar] [CrossRef]
- Bull, H.; von Wolff, K.; Korber, N.; Tetz, M. Three-year canaloplasty outcomes for the treatment of open-angle glaucoma: European study results. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 1537–1545. [Google Scholar] [CrossRef]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Koerber, N.; Kearney, J.R.; Shingleton, B.J.; Samuelson, T.W. Canaloplasty: Three-year results of circumferential viscodilation and tensioning of Schlemm canal using a microcatheter to treat open-angle glaucoma. J. Cataract. Refract. Surg. 2011, 37, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Khaimi, M.A.; Dvorak, J.D.; Ding, K. An analysis of 3-year outcomes following canaloplasty for the treatment of open-angle glaucoma. J. Ophthalmol. 2017, 2017, 2904272. [Google Scholar] [CrossRef] [PubMed]
- Lewis, R.A.; von Wolff, K.; Tetz, M.; Koerber, N.; Kearney, J.R.; Shingleton, B.J.; Samuelson, T.W. Canaloplasty: Circumferential viscodilation and tensioning of Schlemm canal using a flexible microcatheter for the treatment of open-angle glaucoma in adults: Two-year interim clinical study results. J. Cataract. Refract. Surg. 2009, 35, 814–824. [Google Scholar] [CrossRef]
- Tetz, M.; Koerber, N.; Shingleton, B.J.; von Wolff, K.; Bull, H.; Samuelson, T.W.; Lewis, R.A. Phacoemulsification and intraocular lens implantation before, during, or after canaloplasty in eyes with open-angle glaucoma: 3-year results. J. Glaucoma 2015, 24, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Januschowski, K.; Leers, S.; Haus, A.; Szurman, P.; Seuthe, A.M.; Boden, K.T. Is trabeculectomy really superior to canaloplasty? Acta Ophthalmol. 2016, 94, e666–e667. [Google Scholar] [CrossRef]
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Bengtsson, B.; Hussein, M.; Early Manifest Glaucoma Trial Group. Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef]
- Malik, R.; O’Leary, N.; Mikelberg, F.S.; Balazsi, A.G.; LeBlanc, R.P.; Lesk, M.R.; Nicolela, M.T.; Trope, G.E.; Chauhan, B.C.; Canadian Glaucoma Study Group. Neuroretinal Rim Area Change in Glaucoma Patients with Visual Field Progression Endpoints and Intraocular Pressure Reduction. The Canadian Glaucoma Study: 4. Am. J. Ophthalmol. 2016, 163, 140–147. [Google Scholar] [CrossRef]
- Klink, T.; Sauer, J.; Körber, N.J.; Grehn, F.; Much, M.M.; Thederan, L.; Matlach, J.; Salgado, J.P. Quality of life following glaucoma surgery: Canaloplasty versus trabeculectomy. Clin. Ophthalmol. 2014, 9, 7–16. [Google Scholar]
- Szurman, P.; Januschowski, K.; Boden, K.T.; Szurman, G.B. A modified scleral dissection technique with suprachoroidal drainage for canaloplasty. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 254, 351–354. [Google Scholar] [CrossRef]
- Overby, D.R.; Stamer, W.D.; Johnson, J. The changing paradigm of outflow resistance generation: Towards synergistic models of the JCT and inner wall endothelium. Exp. Eye Res. 2009, 88, 656–670. [Google Scholar] [CrossRef]
- Lutjen-Drecoll, E.; Kruse, F.E. Primary open angle glaucoma. Morphological bases for the understanding of the pathogenesis and effects of antiglaucomatic substances. Ophthalmologe 2007, 104, 167–178. [Google Scholar]
- Szurman, P.; Januschowski, K.; Boden, K.T.; Seuthe, A.M. Suprachoroidal drainage with collagen sheet implant—A novel technique for non-penetrating glaucoma surgery. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 381–385. [Google Scholar] [PubMed]
- Seuthe, A.M.; Januschowski, K.; Mariacher, S.; Ebner, M.; Opitz, N.; Szurman, P.; Boden, K. The effect of canaloplasty with suprachoroidal drainage combined with cataract surgery—1-year results. Acta Ophthalmol. 2018, 96, e74–e78. [Google Scholar] [PubMed]
- Grieshaber, M.C.; Pienaar, A.; Olivier, J.; Stegmann, R. Canaloplasty for primary open-angle glaucoma: Long-term outcome. Br. J. Ophthalmol. 2010, 94, 1478–1482. [Google Scholar] [CrossRef] [PubMed]
- Klink, T.; Panidou, E.; Kanzow-Terai, B.; Klink, J.; Schlunck, G.; Grehn, F.J. Are there filtering blebs after canaloplasty? J. Glaucoma 2012, 21, 89–94. [Google Scholar] [PubMed]
- Barnebey, H.S. Canaloplasty with intraoperative low dosage mitomycin C: A retrospective case series. J. Glaucoma 2013, 22, 201–204. [Google Scholar] [CrossRef]
- Liang, Y.; Sun, H.; Shuai, J.; Xu, K.; Ji, F.F.; Sucijanti Yuan, Z.L. Modified viscocanalostomy in the Chinese population with open angle glaucoma: A 10-year follow-up results. Int. J. Ophthalmol. 2019, 12, 429–435. [Google Scholar] [PubMed]
- Elksne, E.; Mercieca, K.; Prokosch-Willing, V. Canaloplasty with mitomycin C after previous combined cataract surgery and Schlemm’s canal microstent implantation. Eur. J. Ophthalmol. 2022, 32, 712–716. [Google Scholar] [CrossRef]
- Cheng, J.W.; Cai, J.P.; Li, Y.; Wei, R.L. Intraoperative mitomycin C for nonpenetrating glaucoma surgery: A systematic review and meta-analysis. J. Glaucoma 2011, 20, 322–326. [Google Scholar]
- Szurman, P.; Mansouri, K.; Dick, H.B.; Mermoud, A.; Hoffmann, E.M.; Mackert, M.; Weinreb, R.N.; Rao, H.L.; Seuthe, A.M. Safety and performance of a suprachoroidal sensor for telemetric measurement of intraocular pressure in the EYEMATE-SC trial. Br. J. Ophthalmol. 2023, 107, 518–524. [Google Scholar] [CrossRef]
- Wasielica-Poslednik, J.; Schmeisser, J.; Hoffmann, E.M.; Weyer-Elberich, V.; Bell, K.; Lorenz, K.; Pfeiffer, N. Fluctuation of intraocular pressure in glaucoma patients before and after trabeculectomy with mitomycin C. PLoS ONE 2017, 12, e0185246. [Google Scholar] [CrossRef] [PubMed]
- Szurman, P. Implant for Determining Intraocular Pressure. International Application No. PCT/EP2015/062976, 30 December 2015. [Google Scholar]
- Mariacher, S.; Ebner, M.; Januschowski, K.; Hurst, J.; Schnichels, S.; Szurman, P. Investigation of a novel implantable suprachoroidal pressure transducer for telemetric intraocular pressure monitoring. Exp. Eye Res. 2016, 151, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Sleath, B.; Blalock, S.; Covert, D.; Stone, J.L.; Skinner, A.C.; Muir, K.; Robin, A.L. The relationship between glaucoma medication adherence, eye drop technique, and visual field defect severity. Ophthalmology 2011, 118, 2398–2402. [Google Scholar] [CrossRef] [PubMed]
- Szurman, P.; Gillmann, K.; Seuthe, A.M.; Dick, H.B.; Hoffmann, E.M.; Mermoud, A.; Mackert, M.J.; Weinreb, R.N.; Rao, H.L.; Mansouri, K. EYEMATE-SC Trial: Twelve-Month Safety, Performance, and Accuracy of a Suprachoroidal Sensor for Telemetric Measurement of Intraocular Pressure. Ophthalmology 2023, 130, 304–312. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szurman, P. Advances in Canaloplasty—Modified Techniques Yield Strong Pressure Reduction with Low Risk Profile. J. Clin. Med. 2023, 12, 3031. https://doi.org/10.3390/jcm12083031
Szurman P. Advances in Canaloplasty—Modified Techniques Yield Strong Pressure Reduction with Low Risk Profile. Journal of Clinical Medicine. 2023; 12(8):3031. https://doi.org/10.3390/jcm12083031
Chicago/Turabian StyleSzurman, Peter. 2023. "Advances in Canaloplasty—Modified Techniques Yield Strong Pressure Reduction with Low Risk Profile" Journal of Clinical Medicine 12, no. 8: 3031. https://doi.org/10.3390/jcm12083031
APA StyleSzurman, P. (2023). Advances in Canaloplasty—Modified Techniques Yield Strong Pressure Reduction with Low Risk Profile. Journal of Clinical Medicine, 12(8), 3031. https://doi.org/10.3390/jcm12083031