

Pulmonary Recruitment Prior to Intraoperative Multiple Pulmonary Ground-Glass Nodule Localization Increases the Localization Accuracy—A Retrospective Study
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-W.; Chen, J.-S. Image-guided techniques for localizing pulmonary nodules in thoracoscopic surgery. J. Thorac. Dis. 2016, 8, S749. [Google Scholar] [CrossRef] [PubMed]
- Migliore, M.; Palmucci, S.; Nardini, M.; Basile, A. Imaging patterns of early stage lung cancer for the thoracic surgeon. J. Thorac. Dis. 2020, 12, 3349. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Han, K.; Hur, J.; Lee, S.M.; Lee, J.W.; Hwang, S.H.; Seo, J.S.; Lee, K.H.; Kwon, W.; Kim, T.H. Comparative effectiveness and safety of preoperative lung localization for pulmonary nodules: A systematic review and meta-analysis. Chest 2017, 151, 316–328. [Google Scholar] [CrossRef]
- Fang, H.-Y.; Chang, K.-W.; Chao, Y.-K. Hybrid operating room for the intraoperative CT-guided localization of pulmonary nodules. Ann. Transl. Med. 2019, 7, 34. [Google Scholar] [CrossRef]
- Chao, Y.-K.; Pan, K.-T.; Wen, C.-T.; Fang, H.-Y.; Hsieh, M.-J. A comparison of efficacy and safety of preoperative versus intraoperative computed tomography-guided thoracoscopic lung resection. J. Thorac. Cardiovasc. Surg. 2018, 156, 1974–1983.e1971. [Google Scholar]
- Kwok, Y.; Irani, F.; Tay, K.; Yang, C.; Padre, C.; Tan, B. Effective dose estimates for cone beam computed tomography in interventional radiology. Eur. Radiol. 2013, 23, 3197–3204. [Google Scholar] [CrossRef]
- Hu, M.-C.; Yang, Y.-L.; Chen, T.-T.; Lee, C.-I.; Tam, K.-W. Recruitment maneuvers to reduce pulmonary atelectasis after cardiac surgery: A meta-analysis of randomized trials. J. Thorac. Cardiovasc. Surg. 2022, 164, 171–181.e174. [Google Scholar] [CrossRef]
- Oh, E.J.; Lee, E.J.; Heo, B.-y.; Huh, J.; Min, J.-J. Physiological benefits of lung recruitment in the semi-lateral position after laparoscopic surgery: A randomized controlled study. Sci. Rep. 2022, 12, 3909. [Google Scholar] [CrossRef]
- Pei, S.; Wei, W.; Yang, K.; Yang, Y.; Pan, Y.; Wei, J.; Yao, S.; Xia, H. Recruitment Maneuver to reduce postoperative pulmonary complications after laparoscopic abdominal surgery: A systematic review and meta-analysis. J. Clin. Med. 2022, 11, 5841. [Google Scholar] [CrossRef]
- Suzuki, K.; Watanabe, S.-I.; Wakabayashi, M.; Saji, H.; Aokage, K.; Moriya, Y.; Yoshino, I.; Tsuboi, M.; Nakamura, S.; Nakamura, K. A single-arm study of sublobar resection for ground-glass opacity dominant peripheral lung cancer. J. Thorac. Cardiovasc. Surg. 2022, 163, 289–301.e282. [Google Scholar] [CrossRef]
- Cui, Y.; Cao, R.; Li, G.; Gong, T.; Ou, Y.; Huang, J. The effect of lung recruitment maneuvers on post-operative pulmonary complications for patients undergoing general anesthesia: A meta-analysis. PLoS ONE 2019, 14, e0217405. [Google Scholar] [CrossRef]
- Hartland, B.L.; Newell, T.J.; Damico, N.J.R.c. Alveolar recruitment maneuvers under general anesthesia: A systematic review of the literature. Respir. Care 2015, 60, 609–620. [Google Scholar] [CrossRef]
- Reinius, H.; Jonsson, L.; Gustafsson, S.; Sundbom, M.; Duvernoy, O.; Pelosi, P.; Hedenstierna, G.; Freden, F. Prevention of atelectasis in morbidly obese patients during general anesthesia and paralysis: A computerized tomography study. J. Am. Soc. Anesthesiol. 2009, 111, 979–987. [Google Scholar] [CrossRef]
- Hedenstierna, G.; Tokics, L.; Reinius, H.; Rothen, H.U.; Östberg, E.; Öhrvik, J. Higher age and obesity limit atelectasis formation during anaesthesia: An analysis of computed tomography data in 243 subjects. Br. J. Anaesth. 2020, 124, 336–344. [Google Scholar] [CrossRef]
- Pépin, J.L.; Timsit, J.F.; Tamisier, R.; Borel, J.C.; Lévy, P.; Jaber, S. Prevention and care of respiratory failure in obese patients. Lancet Respir. Med. 2016, 4, 407–418. [Google Scholar] [CrossRef]
- Almarakbi, W.; Fawzi, H.; Alhashemi, J. Effects of four intraoperative ventilatory strategies on respiratory compliance and gas exchange during laparoscopic gastric banding in obese patients. Br. J. Anaesth. 2009, 102, 862–868. [Google Scholar] [CrossRef]
- Pang, C.; Yap, J.; Chen, P. The effect of an alveolar recruitment strategy on oxygenation during laparascopic cholecystectomy. Anaesth. Intensive Care 2003, 31, 176–180. [Google Scholar] [CrossRef]
- Severgnini, P.; Selmo, G.; Lanza, C.; Chiesa, A.; Frigerio, A.; Bacuzzi, A.; Dionigi, G.; Novario, R.; Gregoretti, C.; de Abreu, M.G. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology 2013, 118, 1307–1321. [Google Scholar] [CrossRef] [PubMed]
- Borges, J.B.; Okamoto, V.N.; Matos, G.F.; Caramez, M.P.; Arantes, P.R.; Barros, F.; Souza, C.E.; Victorino, J.A.; Kacmarek, R.M.; Barbas, C.S. Reversibility of lung collapse and hypoxemia in early acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2006, 174, 268–278. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.L.; Borges, J.B.; Melo, A.; Suarez-Sipmann, F.; Toufen, C.; Bohm, S.H.; Amato, M.B. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. 2009, 35, 1132–1137. [Google Scholar] [CrossRef]
- Zaman, M.; Bilal, H.; Woo, C.Y.; Tang, A. In patients undergoing video-assisted thoracoscopic surgery excision, what is the best way to locate a subcentimetre solitary pulmonary nodule in order to achieve successful excision? Interact. Cardiovasc. Thorac. Surg. 2012, 15, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.-K.; Wu, Y.-C. Electromagnetic navigation-guided one-stage dual localization of small pulmonary nodules. Chest 2018, 154, 1462–1463. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Kim, T.G.; Song, Y.G. Comparison of hook wire versus coil localization for video-assisted thoracoscopic surgery. Thorac. Cancer 2018, 9, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Kleedehn, M.; Kim, D.H.; Lee, F.T.; Lubner, M.G.; Robbins, J.B.; Ziemlewicz, T.J.; Hinshaw, J.L. Preoperative pulmonary nodule localization: A comparison of methylene blue and hookwire techniques. Am. J. Roentgenol. 2016, 207, 1334–1339. [Google Scholar] [CrossRef]
- Ehrenfeld, J.M.; Funk, L.M.; Van Schalkwyk, J.; Merry, A.F.; Sandberg, W.S.; Gawande, A. The incidence of hypoxemia during surgery: Evidence from two institutions. Can. J. Anaesth. J. Can. D’anesthesie 2010, 57, 888. [Google Scholar] [CrossRef]
- Yuan, X.; Lee, J.W.; Bowser, J.L.; Neudecker, V.; Sridhar, S.; Eltzschig, H.K. Targeting hypoxia signaling for perioperative organ injury. Anesth. Analg. 2018, 126, 308. [Google Scholar] [CrossRef]
- Moller, J.; Johannessen, N.; Berg, H.; Espersen, K.; Larsen, L. Hypoxaemia during anaesthesia—An observer study. Br. J. Anaesth. 1991, 66, 437–444. [Google Scholar] [CrossRef]
- Aakerlund, L.; Rosenberg, J. Postoperative delirium: Treatment with supplementary oxygen. BJA Br. J. Anaesth. 1994, 72, 286–290. [Google Scholar] [CrossRef]
- Gill, N.; Wright, B.; Reilly, C. Relationship between hypoxaemic and cardiac ischaemic events in the perioperative period. Br. J. Anaesth. 1992, 68, 471–473. [Google Scholar] [CrossRef]
- Duggan, M.; McNamara, P.J.; Engelberts, D.; Pace-Asciak, C.; Babyn, P.; Post, M.; Kavanagh, B.P. Oxygen attenuates atelectasis-induced injury in the in vivo rat lung. J. Am. Soc. Anesthesiol. 2005, 103, 522–531. [Google Scholar] [CrossRef]
- Gunnarsson, L.; Tokics, L.; Gustavsson, H.; Hedenstierna, G. Influence of age on atelectasis formation and gas exchange impairment during general anaesthesia. Br. J. Anaesth. 1991, 66, 423–432. [Google Scholar] [CrossRef]
- Ueda, K.; Kaneda, Y.; Sudou, M.; Jinbo, M.; Li, T.-S.; Suga, K.; Tanaka, N.; Hamano, K. Prediction of hypoxemia after lung resection surgery. Interact. CardioVascular Thorac. Surg. 2005, 4, 85–89. [Google Scholar] [CrossRef]
- Mori, S.; Shibazaki, T.; Noda, Y.; Kato, D.; Nakada, T.; Asano, H.; Matsudaira, H.; Ohtsuka, T. Recovery of pulmonary function after lung wedge resection. J. Thorac. Dis. 2019, 11, 3738. [Google Scholar] [CrossRef]
- Danish, M.A. Preoxygenation and anesthesia: A detailed review. Cureus 2021, 13, e13240. [Google Scholar]
- Joyce, C.; Williams, A. Kinetics of absorption atelectasis during anesthesia: A mathematical model. J. Appl. Physiol. 1999, 86, 1116–1125. [Google Scholar] [CrossRef]
- Joyce, C.; Baker, A.; Kennedy, R. Gas uptake from an unventilated area of lung: Computer model of absorption atelectasis. J. Appl. Physiol. 1993, 74, 1107–1116. [Google Scholar] [CrossRef]
- Magnusson, L.; Spahn, D. New concepts of atelectasis during general anaesthesia. Br. J. Anaesth. 2003, 91, 61–72. [Google Scholar] [CrossRef]
- Eger, E.; Severinghaus, J. The rate of rise of PaCO2 in the apneic anesthetized patient. J. Am. Soc. Anesthesiol. 1961, 22, 419–425. [Google Scholar] [CrossRef]
- Oczenski, W.; Hörmann, C.; Keller, C.; Lorenzl, N.; Kepka, A.; Schwarz, S.; Fitzgerald, R.D. Recruitment maneuvers during prone positioning in patients with acute respiratory distress syndrome. Crit. Care Med. 2005, 33, 54–61. [Google Scholar] [CrossRef]
- Wesselink, E.; Kappen, T.; Torn, H.; Slooter, A.; Van Klei, W. Intraoperative hypotension and the risk of postoperative adverse outcomes: A systematic review. Br. J. Anaesth. 2018, 121, 706–721. [Google Scholar] [CrossRef] [PubMed]



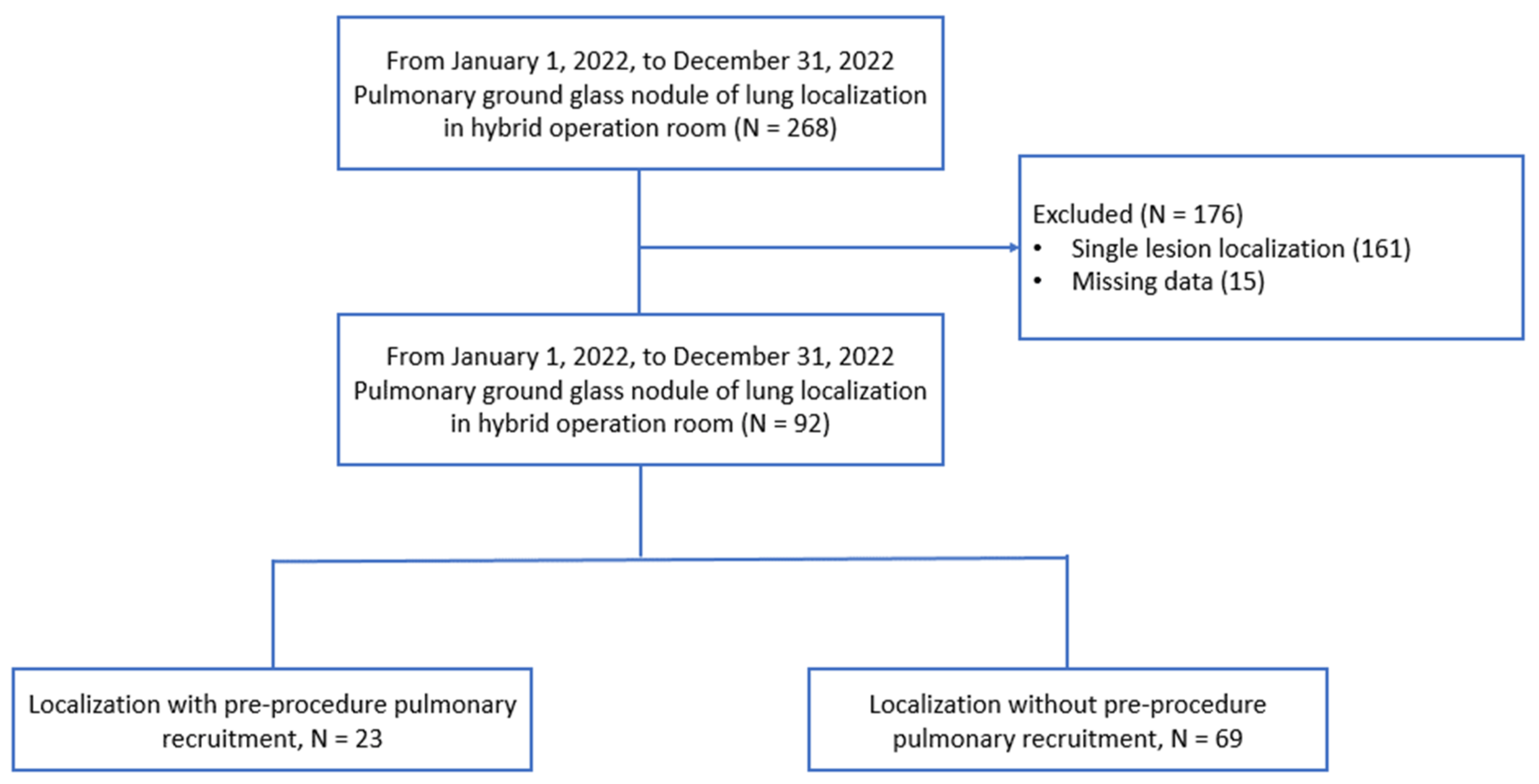{kind=link}
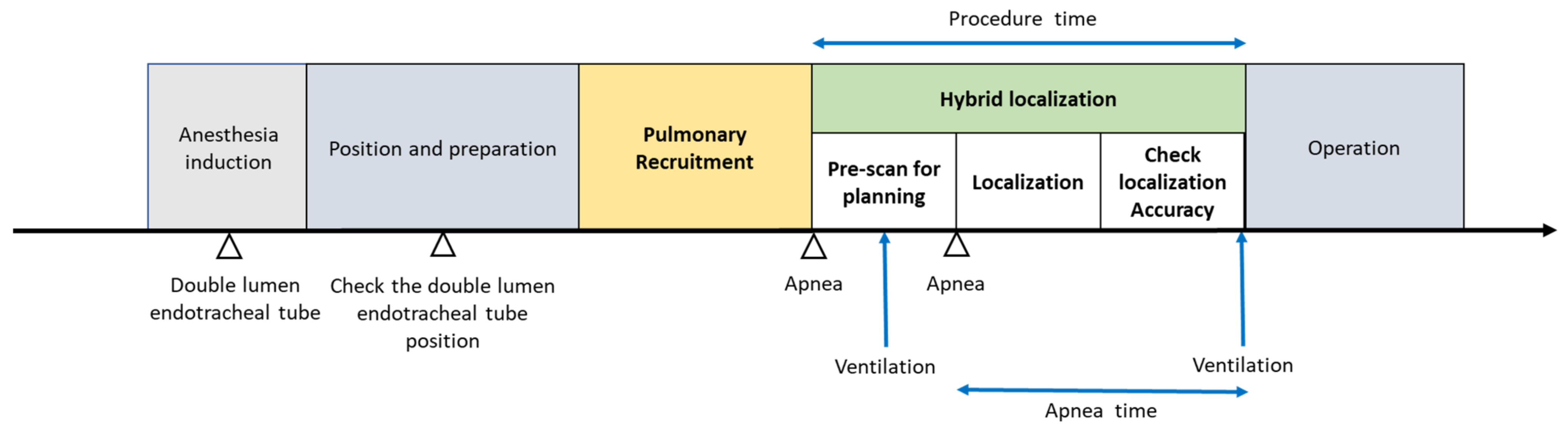{kind=link}
| Non-Recruitment Group (N = 69) | Recruitment Group (N = 23) | p Value | |
|---|---|---|---|
| Age, median (IQR) | 53 (47–63) | 57 (49–66) | 0.281 |
| Gender | † 0.778 | ||
| Female | 52 (75.4%) | 18 (78.3%) | |
| Male | 17 (25.6%) | 5 (21.7%) | |
| Height, median (IQR) | 160.0 (156.0–166.0) | 160.0 (155.0–163.0) | 0.857 |
| Weight, median (IQR) | 63.0 (55.0–70.0) | 57.0 (52.0–69.0) | 0.328 |
| BMI | 24.20 (22.20–26.20) | 22.80 (20.30–26.00) | 0.229 |
| Preoperative lung function | |||
| FVC | 102 (94–110) | 103 (96–108) | 0.921 |
| FEV1 | 97 (88–107) | 103 (91–108) | 0.195 |
| DLCO | 94 (85–102) | 99 (90–104) | 0.116 |
| History of lung contralateral wedge resection | 17 (24.6%) | 4 (17.4%) | † 0.473 |
| Ventilation mode | † 0.441 | ||
| VCV | 8 (11.6%) | 1 (4.3%) | |
| PCVVG | 61 (88.4%) | 22 (95.7%) | |
| Tidal volume during procedure Median (IQR) | 550 (525–600) | 550 (500–600) | 0.281 |
| Lesions | † 0.394 | ||
| 2 lesions | 47 (68.1%) | 16 (69.6%) | |
| 3 lesions | 12 (17.4%) | 6 (26.1%) | |
| 4 lesions | 10 (14.5%) | 1 (4.3%) | |
| Size (mm) | 6.90 (5.70–8.30) | 6.50 (5.50–8.20) | 0.850 |
| Dye/hook localization | † 0.146 | ||
| Dye localization | 26 (37.7%) | 13 (56.5%) | |
| Hook localization | 43 (62.3%) | 10 (43.5%) | |
| Depth, median (IQR) | 70.0 (55.0–80.0) | 65.0 (51.7–75.0) | 0.691 |
| Puncture times | † 0.326 | ||
| 1 time | 64 (92.8%) | 23 (100%) | |
| >1 time | 5 (7.2%) | 0 | |
| Extent of resection | † >0.999 | ||
| Wedge resection | 64 (92.8%) | 21 (91.3%) | |
| Segmentectomy † Wedge resection | 2 (2.9%) | 1 (4.3%) | |
| Lobectomy † Wedge resection | 3 (4.3%) | 1 (4.3%) | |
| Diagnosis | † 0.591 | ||
| Invasive adenocarcinoma | 6 (3.5%) | 3 (5.6%) | |
| Adenocarcinoma in situ (AIS) | 81 (47.6%) | 21 (38.9%) | |
| Minimally invasive adenocarcinoma (MIA) | 51 (30.0%) | 15 (18.5%) | |
| Secondary pulmonary malignancy | 3 (1.8%) | 2 (3.7%) | |
| Benign lesion | 29 (17.1%) | 13 (24.1%) |
| Outcome Setting | Non-Recruitment Group | Recruitment Group | p Value |
|---|---|---|---|
| (N = 69) | (N = 23) | ||
| Apnea time | 5.60 (4.60–6.80) | 5.90 (4.80–6.30) | 0.658 |
| (Min, Median, IQR) | |||
| SpO2 (%, Median, IQR) | 88.0 (84.0–93.0) | 94.0 (87.0–97.0) | 0.016 |
| Re-inflation | † 0.033 | ||
| No need for inflation | 36 (52.2%) | 17 (73.9%) | |
| Need for inflation | 33 (35.9%) | 6 (26.1%) | |
| Procedure time | 19.0 (15.0–24.0) | 17.0 (14.0–19.0) | 0.043 |
| (Min, Median, IQR) | |||
| Pneumothorax | † 0.610 | ||
| Pneumothorax | 46 (66.7%) | 17 (73.9%) | |
| No pneumothorax | 23 (33.3%) | 6 (26.1%) | |
| Accuracy (5 mm) | 38 (55.1%) | 19 (82.6%) | † 0.025 |
| Accuracy | Univariant Logistic Regression Analysis | Multivariant Logistic Regression Analysis | ||
|---|---|---|---|---|
| Odds Ratio | p Value | Odds Ratio | p Value | |
| (95% CI) | (95% CI) | |||
| Pre-localization recruitment | 0.26 | 0.024 | 0.23 | 0.024 |
| (0.08–0.84) | (0.06–0.82) | |||
| Lesions | 0.61 | 0.106 | ||
| (0.33–1.11) | ||||
| History of lung contralateral wedge resection | 0.29 | 0.039 | 0.25 | 0.033 |
| (0.09–0.94) | (0.07–0.90) | |||
| BMI | 0.76 | 0.001 | 0.76 | 0.002 |
| (0.64–0.89) | (0.64–0.90) | |||
| Ventilation mode | 2.43 | 0.286 | ||
| (0.48–12.41) | ||||
| Re-Inflation | Univariant Regression Analysis | Multivariant Regression Analysis | ||
|---|---|---|---|---|
| Odds Ratio | p Value | Odds Ratio | p Value | |
| (95% CI) | (95% CI) | |||
| Pre-localization recruitment | 3.09 | 0.034 | 2.99 | 0.043 |
| (1.08–8.78) | (1.04–8.64) | |||
| Lesions | 1.87 | 0.048 | 1.84 | 0.084 |
| (1.01–3.47) | (0.97–3.48) | |||
| Previous lung operation | 0.43 | 0.093 | ||
| (0.16–1.16) | ||||
| BMI | 1.15 | 0.055 | ||
| (0.99–1.32) | ||||
| Ventilation mode | 0.31 | 0.156 | ||
| (0.06–1.57) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.H.; Su, P.C.; Huang, H.C.; Au, K.; Lin, F.C.F.; Chen, C.Y.; Chou, M.C.; Hsia, J.Y. Pulmonary Recruitment Prior to Intraoperative Multiple Pulmonary Ground-Glass Nodule Localization Increases the Localization Accuracy—A Retrospective Study. J. Clin. Med. 2023, 12, 2998. https://doi.org/10.3390/jcm12082998
Wang YH, Su PC, Huang HC, Au K, Lin FCF, Chen CY, Chou MC, Hsia JY. Pulmonary Recruitment Prior to Intraoperative Multiple Pulmonary Ground-Glass Nodule Localization Increases the Localization Accuracy—A Retrospective Study. Journal of Clinical Medicine. 2023; 12(8):2998. https://doi.org/10.3390/jcm12082998
Chicago/Turabian StyleWang, Yu Hsiang, Pei Chin Su, Hsu Chih Huang, Kenneth Au, Frank Cheau Feng Lin, Chih Yi Chen, Ming Chih Chou, and Jiun Yi Hsia. 2023. "Pulmonary Recruitment Prior to Intraoperative Multiple Pulmonary Ground-Glass Nodule Localization Increases the Localization Accuracy—A Retrospective Study" Journal of Clinical Medicine 12, no. 8: 2998. https://doi.org/10.3390/jcm12082998
APA StyleWang, Y. H., Su, P. C., Huang, H. C., Au, K., Lin, F. C. F., Chen, C. Y., Chou, M. C., & Hsia, J. Y. (2023). Pulmonary Recruitment Prior to Intraoperative Multiple Pulmonary Ground-Glass Nodule Localization Increases the Localization Accuracy—A Retrospective Study. Journal of Clinical Medicine, 12(8), 2998. https://doi.org/10.3390/jcm12082998