
Long-Term Results of Femorodistal Sequential Composite-Bypass Combining Heparin-Bonded PTFE-Prosthesis and Autologous Vein Using the Deutsch Bridge Technique in Critical Limb-Threatening Ischemia
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Epidemiological Data and Indication for Operation
3.2. Bypass Configuration
3.3. Patient-Related Outcome
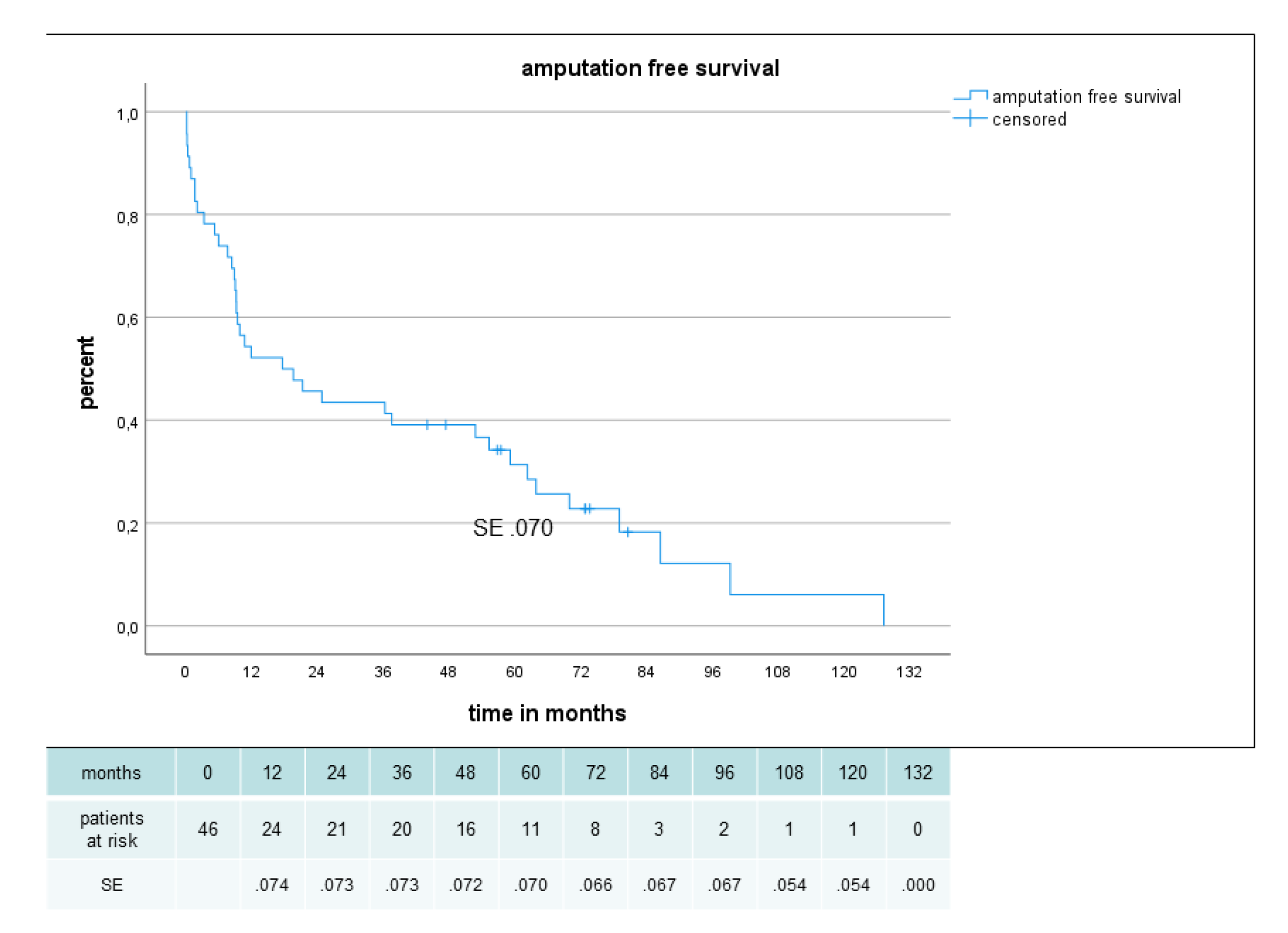
3.4. Graft Function and Limb Salvage
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farber, A.; Menard, M.T.; Conte, M.S.; Kaufman, J.A.; Powell, R.J.; Choudhry, N.K.; Hamza, T.H.; Assmann, S.F.; Creager, M.A.; Cziraky, M.J.; et al. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N. Engl. J. Med. 2022, 387, 2305–2316. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, G.D.; Nagy, J.; Black, D.; Stonebridge, P.A. Randomized clinical trial of distal anastomotic interposition vein cuff in in-frainguinal polytetrafluoroethylene bypass grafting. Br. J. Surg. 2004, 91, 560–562. [Google Scholar] [CrossRef] [PubMed]
- Neville, R.; Lidsky, M.; Capone, A.; Babrowicz, J.; Rahbar, R.; Sidawy, A. An Expanded Series of Distal Bypass Using the Distal Vein Patch Technique to Improve Prosthetic Graft Performance in Critical Limb Ischemia. Eur. J. Vasc. Endovasc. Surg. 2012, 44, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Neville, R.F.; Tempesta, B.; Sidawy, A.N. Tibial bypass for limb salvage using polytetrafluoroethylene and a distal vein patch. J. Vasc. Surg. 2001, 33, 266–271; discussion 271–272. [Google Scholar] [CrossRef] [PubMed]
- Burdick, J.F.; O’Mara, C.; Ricotta, J.; Zinner, M.; Williams, G.M. The multiple sequential distal bypass graft: Improving nature’s al-ternatives. Surgery 1981, 89, 536–542. [Google Scholar]
- Edwards, W.S.; Gerety, E.; Larkin, J.; Hoyt, T.W. Multiple sequential femoral tibial grafting for severe ischemia. Surgery 1976, 80, 722–728. [Google Scholar]
- Flinn, W.R.; Flanigan, D.P.; Verta, M.J.; Bergan, J.J.; Yao, J.S. Sequential femoral-tibial bypass for severe limb ischemia. Surgery 1980, 88, 357–365. [Google Scholar]
- Flinn, W.R.; Ricco, J.B.; Yao, J.S.; McDaniel, M.D.; King, T.A.; Bergan, J.J. Composite sequential grafts in severe ischemia: A compara-tive study. J. Vasc. Surg. 1984, 1, 449–454. [Google Scholar] [CrossRef]
- Jarrett, F.; Berkoff, H.A.; Crummy, A.B. Sequential Femoral-tibial Bypass Grafting for Limb Salvage. Ann. Surg. 1978, 188, 685–688. [Google Scholar] [CrossRef]
- Jarrett, F.; Berkoff, H.A.; Crummy, A.B. Sequential femorotibial bypass: Clinical results. Can. J. Surg. 1980, 23, 78–80. [Google Scholar]
- Verta, M.J. Construction of a composite sequential bypass graft. Surg. Gynecol. Obstet. 1982, 155, 893–894. [Google Scholar]
- Parsons, R.E.; Suggs, W.D.; Veith, F.J.; Sanchez, L.A.; Lyon, R.T.; Marin, M.L.; Goldsmith, J.; Faries, P.L.; Wengerter, K.R.; Schwartz, M.L. Polytetrafluoroethylene bypasses to infrapopliteal arteries without cuffs or patches: A better option than amputation in patients without autologous vein. J. Vasc. Surg. 1996, 23, 347–354; discussion 355–356. [Google Scholar] [CrossRef]
- Dorigo, W.; Pulli, R.; Piffaretti, G.; Castelli, P.; Griselli, F.; Dorrucci, V.; Ferilli, F.; Ottavi, P.; De Blasis, G.; Scalisi, L.; et al. Results from an Italian multicentric registry comparing heparin-bonded ePTFE graft and autologous saphenous vein in below-knee femoro-popliteal bypasses. J. Cardiovasc. Surg. 2012, 53, 187. [Google Scholar]
- Lindholt, J.S.; Houlind, K.; Gottschalksen, B.; Pedersen, C.N.; Ravn, H.; Viddal, B.; Pedersen, G.; Rasmussen, M.; Wedel, C.; Bramsen, M.B. Five-year outcomes following a randomized trial of femorofemoral and femoropopliteal bypass grafting with heparin-bonded or standard polytetrafluoroethylene grafts. Br. J. Surg. 2016, 103, 1300–1305. [Google Scholar] [CrossRef]
- Neville, R.F.; Capone, A.; Amdur, R.; Lidsky, M.; Babrowicz, J.; Sidawy, A.N. A comparison of tibial artery bypass performed with heparin-bonded expanded polytetrafluoroethylene and great saphenous vein to treat critical limb ischemia. J. Vasc. Surg. 2012, 56, 1008–1014. [Google Scholar] [CrossRef]
- Deutsch, M.; Meinhart, J.; Howanietz, N.; Fröschl, A.; Heine, B.; Moidl, R.; Mendel, H.; Sisel, A.; Stümpflen, A.; Zilla, P. The Bridge Graft: A New Concept for Infrapopliteal Surgery. Eur. J. Vasc. Endovasc. Surg. 2001, 21, 508–512. [Google Scholar] [CrossRef]
- Rutherford, R.B.; Baker, J.; Ernst, C.; Johnston, K.; Porter, J.M.; Ahn, S.; Jones, D.N. Recommended standards for reports dealing with lower extremity ischemia: Revised version. J. Vasc. Surg. 1997, 26, 517–538. [Google Scholar] [CrossRef]
- Donaldson, M.C.; Whittemore, A.D.; Mannick, J.A. Further experience with an all-autogenous tissue policy for infrainguinal re-construction. J. Vasc. Surg. 1993, 18, 41–48. [Google Scholar] [CrossRef]
- Kent, K.C.; Whittemore, A.D.; Mannick, J.A. Short-term and midterm results of an all-autogenous tissue policy for infrainguinal reconstruction. J. Vasc. Surg. 1989, 9, 107–114. [Google Scholar] [CrossRef]
- Alexander, J.J.; Wells, K.E.; Yuhas, J.P.; Piotrowski, J.J. The role of composite sequential bypass in the treatment of multilevel in-frainguinal arterial occlusive disease. Am. J. Surg. 1996, 172, 118–122. [Google Scholar] [CrossRef]
- McCarthy, W.J.; Pearce, W.H.; Flinn, W.R.; McGee, G.S.; Wang, R.; Yao, J.S. Long-term evaluation of composite sequential bypass for limb-threatening ischemia. J. Vasc. Surg. 1992, 15, 761–769; discussion 9–70. [Google Scholar] [CrossRef] [PubMed]
- Oppat, W.F.; Pearce, W.H.; McMillan, W.D.; Matsumura, J.S.; McCarthy, W.J.; Yao, J.S. Natural history of composite sequential by-pass: Ten years’ experience. Arch. Surg. 1999, 134, 754–757; discussion 7–8. [Google Scholar] [CrossRef] [PubMed]
- Roddy, S.P.; Darling, I.I.I.R.C.; Ozsvath, K.J.; Kreienberg, P.B.; Chang, B.B.; Mathew, T.S.; Paty, P.S.; Mehta, M.; Shah, D.M. Composite sequential arterial recon-struction for limb salvage. J. Vasc. Surg. 2002, 36, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Bastounis, E.; Georgopoulos, S.; Maltezos, C.; Alexiou, D.; Chiotopoulos, D.; Bramis, J. PTFE-vein composite grafts for critical limb ischaemia: A valuable alternative to all-autogenous infrageniculate reconstructions. Eur. J. Vasc. Endovasc. Surg. 1999, 18, 127–132. [Google Scholar] [CrossRef]
- Chang, J.B.; Stein, T.A. The long-term value of composite grafts for limb salvage. J. Vasc. Surg. 1995, 22, 25–31. [Google Scholar] [CrossRef]
- Gargiulo, N.J.; Veith, F.J., 3rd; O’Connor, D.J.; Lipsitz, E.C.; Suggs, W.D.; Scher, L.A. Experience with a modified composite sequential bypass technique for limb-threatening ischemia. Ann. Vasc. Surg. 2010, 24, 1000–1004. [Google Scholar] [CrossRef]
- Mahmood, A.; Garnham, A.; Sintler, M.; Smith, S.R.; Vohra, R.K.; Simms, M.H. Composite sequential grafts for femorocrural bypass reconstruction: Experience with a modified technique. J. Vasc. Surg. 2002, 36, 772–778. [Google Scholar] [CrossRef]
- Neufang, A.; Dorweiler, B.; Espinola-Klein, C.; Savvidis, S.; Doemland, M.; Schotten, S.; Vahl, C.F. Outcomes of complex femorodistal sequential autologous vein and biologic prosthesis composite bypass grafts. J. Vasc. Surg. 2014, 60, 1543–1553. [Google Scholar] [CrossRef]
- Rogers, A.C.; Reddy, P.W.; Cross, K.S.; McMonagle, M.P. Using the diamond intermediate anastomosis in composite sequential bypass grafting for critical limb ischemia. J. Vasc. Surg. 2016, 63, 1116–1120. [Google Scholar] [CrossRef]
- Dorigo, W.; Pulli, R.; Castelli, P.; Dorrucci, V.; Ferilli, F.; De Blasis, G.; Monaca, V.; Vecchiati, E.; Pratesi, C.; Propaten Italian Registry Group. A multicenter comparison between autologous saphe-nous vein and heparin-bonded expanded polytetrafluoroethylene (ePTFE) graft in the treatment of critical limb ischemia in diabetics. J. Vasc. Surg. 2011, 54, 1332–1338. [Google Scholar] [CrossRef]
- Pulli, R.; Dorigo, W.; Castelli, P.; Dorrucci, V.; Ferilli, F.; De Blasis, G.; Monaca, V.; Vecchiati, E.; Pratesi, C. Midterm results from a multicenter registry on the treatment of infrainguinal critical limb ischemia using a heparin-bonded ePTFE graft. J. Vasc. Surg. 2010, 51, 1167–1177.e1. [Google Scholar] [CrossRef]
- Uhl, C.; Hock, C.; Betz, T.; Greindl, M.; Töpel, I.; Steinbauer, M. Comparison of venous and HePTFE tibial and peroneal bypasses in critical limb ischemia patients unsuitable for endovascular revascularization. Vascular 2015, 23, 607–613. [Google Scholar] [CrossRef]
- Franchin, M.; Palermo, V.; Iannuzzi, C.; Rivolta, N.; Mozzetta, G.; Tozzi, M.; Bush, R.L.; Piffaretti, G. A predictive score for 30-day survival for pa-tients undergoing major lower limb amputation for peripheral arterial obstructive disease. Updates Surg. 2021, 73, 1989–2000. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients n = 46 | % | |
|---|---|---|
| Mean age ± SD range (y) | 79.2 ± 10.1 54.1–93.7 | |
| Age over 80 y | 22 | 48 |
| female | 23 | 50 |
| male | 23 | 50 |
| Risk factors and comorbidities | n | % |
| Hypertension | 46 | 100 |
| Hyperlipidemia | 36 | 78.2 |
| Diabetes mellitus | 20 | 43.5 |
| Nicotine abuse | 13 | 28.2 |
| Cardiac status * | ||
| Category 0 | 3 | 6.5 |
| Category 1 | 28 | 60.8 |
| Category 2 | 8 | 17.5 |
| Category 3 | 7 | 15.2 |
| Coronary artery disease | 34 | 73.9 |
| Previous cerebrovascular accident | 16 | 34.7 |
| Renal status | ||
| Creatinine < 1.5 mg/dL | 29 | 63.1 |
| Creatinine > 1.5 and <2.4 mg/dL | 10 | 21.7 |
| Creatinine > 2.4 and <6.0 mg/dL | 2 | 4.3 |
| dialysis | 5 | 10.9 |
| Previous ipsilateral vascular procedures in 47 limbs | n | % |
| No previous ipsilateral vascular intervention or operation | 11 | 23.4 |
| Infrainguinal bypass ** | 28 | 63.8 |
| Local reconstruction of femoral artery *** | 10 | 21.3 |
| Endovascular procedure | 18 | 38.2 |
| Infrainguinal ipsilateral stent | 5 | 10.6 |
| Surgical and endovascular procedure | 8 | 17.0 |
| Surgical inflow procedure | 5 | 10.6 |
| Endovascular inflow procedure | 4 | 8.5 |
| Indication | n | % |
|---|---|---|
| critical limb threatening ischemia | 47 | 100 |
| rest pain | 8 | 20.5 |
| necrosis/ulceration | 38 | 75.5 |
| acute ischemia on severe chronic ischemia * | 1 | 2.4 |
| total | 47 | 100 |
| Blood Test Preop | Value (Range) | |
|---|---|---|
| Hemoglobin mg/dL | 11.8 ± 1.8 | |
| Thrombocytes per microliter | 261.000 ± 105.000 | |
| Leukocytes per microliter | 9.5 ± 3.4 | |
| CRP | 3.5 ± 5.0 | |
| Creatinine mg/dL | 1.6 ± 1.4 (0.5–6.8) | |
| GFR mL/min | 56.5 ± 34.0 | |
| Medication preop | N | (%) |
| Aspirin | 35 | 76.1 |
| Clopidogrel | 4 | 8.6 |
| Vit K antagonist | 15 | 32.6 |
| DAOC | 1 | 2.2 |
| Statin | 32 | 69.5 |
| Medication postop | ||
| Aspirin | 42 | 91.3 |
| Clopidogrel | 12 | 26.1 |
| Vit K antagonist | 23 | 50.0 |
| DAOC | 2 | 4.4 |
| Statin | 39 | 84.7 |
| Prosthetic Part | n | % |
|---|---|---|
| Heparin-bonded PTFE-prosthesis | 47 | 100 |
| diameter 6 mm | 46 | 98 |
| diameter 8 mm | 1 | 2 |
| venous (bridge) part * | ||
| greater saphenous vein | 12 | 25 |
| arm vein | 29 | 62 |
| Combination of greater saphenous vein and arm vein | 5 | 11 |
| posterior tibial vein | 1 | 2 |
| total | 47 | 100 |
| Proximal Anastomosis | n | % |
|---|---|---|
| Common femoral | 40 | 85 |
| Profunda femoris | 4 | 9 |
| Inflow bypass | 2 | 4 |
| External iliac artery | 1 | 2 |
| Composite anastomosis | ||
| Distal thigh | 1 | 2 |
| Proximal calf | 18 | 38 |
| Distal calf | 28 | 60 |
| First sequential anastomosis | ||
| Popliteal artery (below knee in 9 cases) | 10 | 21 |
| Proximal part of tibial artery | 6 | 13 |
| Middle and distal part of tibial artery | 31 | 66 |
| Second sequential anastomosis | ||
| Proximal and middle part of tibial artery | 20 | 42 |
| distal part of tibial artery * | 5 | 11 |
| pedal artery * | 22 | 47 |
| Postoperative (30 d or in Hospital) Complications in 47 Operations | n | % |
|---|---|---|
| death (ischemic heart failure, pneumonia, visceral ischemia, renal failure * | 5 | 10.6 |
| Myocardial infarction, cardiac failure, arrhythmia | 7 | 14.8 |
| stroke, TIA | 1 | 2.1 |
| respiratory failure, pneumonia | 3 | 6.4 |
| Visceral artery occlusion | 1 | 2.1 |
| Other Arterial occlusion | 1 | 2.1 |
| renal failure (reversible) * | 3 (2) | 6.4 (4.2) |
| sepsis, systemic inflammatory signs | 3 | 6.4 |
| delirium | 3 | 6.4 |
| others | 1 | 2.1 |
| Bypass occlusion complete ** | 2 | 4.2 |
| Occlusion of second distal anastomosis (asymptomatic, left untreated) | 1 | 2.1 |
| hematoma (surgical revision) | 0 | 0 |
| Superficial wound infection/delayed wound healing | 6 | 12.7 |
| Prosthetic graft infection | 0 | 0 |
| combined mortality and morbidity *** | 22 | 46.8 |
| Major amputation | 1 | 2.1 |
| Minor amputation | 10 | 21.3 |
| Late Patient Outcome Mean Follow-Up 34.5 ± 32.8 mo (1–127 mo) | n | % |
|---|---|---|
| Death during follow-up (cardiovascular, tumor) including early mortality | 38 | 82.6 |
| 5 y patient survival (Kaplan–Meier) | 32% | |
| Late bypass and limb outcome | ||
| Bypass or anastomotic stenosis | 5 | 11 |
| PTA proximal anastomosis | 1 | 2 |
| PTA distal anastomosis | 2 | 4 |
| PTA Bypass | 2 | 4 |
| Bypass occlusion | 11 | 23 |
| New bypass | 2 | 4 |
| Successful lysis | 1 | 2 |
| Major amputation | 5 | 11 |
| Bypass explantation (infection) * | 2 | 4 |
| Prosthetic graft infection ** | 2 | 4 |
| Major amputation (below knee) *** | 6 (4) | 13 |
| Author | Year | nr | Prosthesis | Configuration | Popliteal Artery | At Ankle Pedal | Re-Do | Prim. Pat. % | Sec. Pat. % | Limb Salv % |
|---|---|---|---|---|---|---|---|---|---|---|
| Verta [11] | 1982 | 54 | PTFE | Jump graft | yes | yes | unclear | Not given | 72.4 (4y) | 78 (4y) |
| Flinn [8] | 1984 | 30 | PTFE | Jump graft | yes | unclear | unclear | Not given | 80 (2y) | ? |
| McCarthy [21] | 1992 | 67 | PTFE | Jump graft | yes | yes | >50% | 40 (4y) | Not given | 70 (4y) |
| Chang [25] | 1995 | 55 | PTFE | Serial anastomoses | yes | 75% | 35 (8y) | 52 (8y) | 65 (8J) | |
| Alexander [20] | 1996 | 35 | PTFE | unclear | yes | unclear | unclear | 35 (2y) | 60 (2y) | |
| Bastounis [24] | 1999 | 21 | PTFE | Serial anastomoses | no | unclear | no | 59 (5y) | unclear | 80 (5J) |
| Oppat [22] | 1999 | 102 | PTFE | Jump graft | yes | unclear | unclear | 20 (7y) | unclear | Similar to patency |
| Deutsch [16] | 2001 | 45 | PTFE | Vein bridge | no | yes | 62% | 26 (4y) | 39 (4y) | 45 (4y) |
| Roddy [23] | 2002 | 27 | PTFE | Arterial origin of distal vein graft | yes | yes | >90% | 64 (3y) | 64 (3y) | 88 (3y) |
| Mahmood [27] | 2002 | 68 | PTFE | Side by side anastomosis | yes | yes | 49% | 68 (2y) | 73 (2y) | 75 (2y) |
| Gargiulo [26] | 2010 | 25 | PTFE | Vein bridge | 88% | unclear | 64% | 54 (5y) | 85 (4y) | |
| Neufang [28] | 2014 | 122 | HUV ovine collagen | Various configurations | 43% | 67% | 30% | 48% (5y) | 71% (5y) | 87% (5y) |
| Rogers [29] | 2016 | 6 | PTFE | Diamond-shaped anastomosis | 6/6 | unclear | unclear | 6/6 Limited follow-up | 6/6 | 5/6 |
| Neufang | 2023 | 47 | PTFE heparin bonded | Vein bridge | 21% | 58% | 63% | 54% (5y) | 66% (5y) | 85% (5y) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neufang, A.; Zhghenti, V.; Vargas-Gomez, C.; Umscheid, T.; von Flotow, P.; Schmiedel, R.; Savvidis, S. Long-Term Results of Femorodistal Sequential Composite-Bypass Combining Heparin-Bonded PTFE-Prosthesis and Autologous Vein Using the Deutsch Bridge Technique in Critical Limb-Threatening Ischemia. J. Clin. Med. 2023, 12, 2895. https://doi.org/10.3390/jcm12082895
Neufang A, Zhghenti V, Vargas-Gomez C, Umscheid T, von Flotow P, Schmiedel R, Savvidis S. Long-Term Results of Femorodistal Sequential Composite-Bypass Combining Heparin-Bonded PTFE-Prosthesis and Autologous Vein Using the Deutsch Bridge Technique in Critical Limb-Threatening Ischemia. Journal of Clinical Medicine. 2023; 12(8):2895. https://doi.org/10.3390/jcm12082895
Chicago/Turabian StyleNeufang, Achim, Valerian Zhghenti, Carolina Vargas-Gomez, Thomas Umscheid, Peter von Flotow, Rainer Schmiedel, and Savvas Savvidis. 2023. "Long-Term Results of Femorodistal Sequential Composite-Bypass Combining Heparin-Bonded PTFE-Prosthesis and Autologous Vein Using the Deutsch Bridge Technique in Critical Limb-Threatening Ischemia" Journal of Clinical Medicine 12, no. 8: 2895. https://doi.org/10.3390/jcm12082895
APA StyleNeufang, A., Zhghenti, V., Vargas-Gomez, C., Umscheid, T., von Flotow, P., Schmiedel, R., & Savvidis, S. (2023). Long-Term Results of Femorodistal Sequential Composite-Bypass Combining Heparin-Bonded PTFE-Prosthesis and Autologous Vein Using the Deutsch Bridge Technique in Critical Limb-Threatening Ischemia. Journal of Clinical Medicine, 12(8), 2895. https://doi.org/10.3390/jcm12082895