
Patients with Acute Limb Ischemia Might Benefit from Endovascular Therapy—A 17-Year Retrospective Single-Center Series of 985 Patients

 , and
, and
Abstract
:1. Introduction
2. Patients and Methods
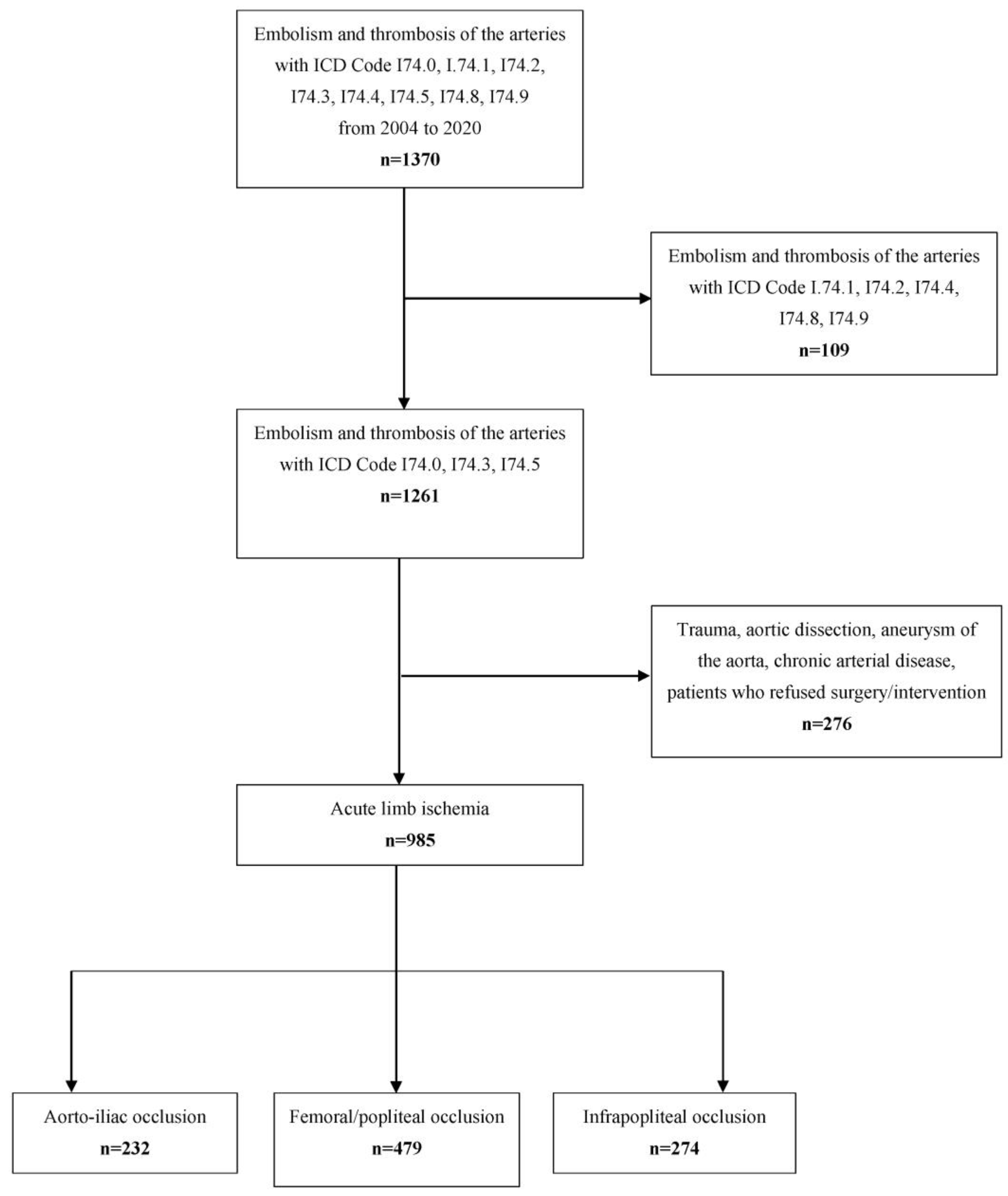
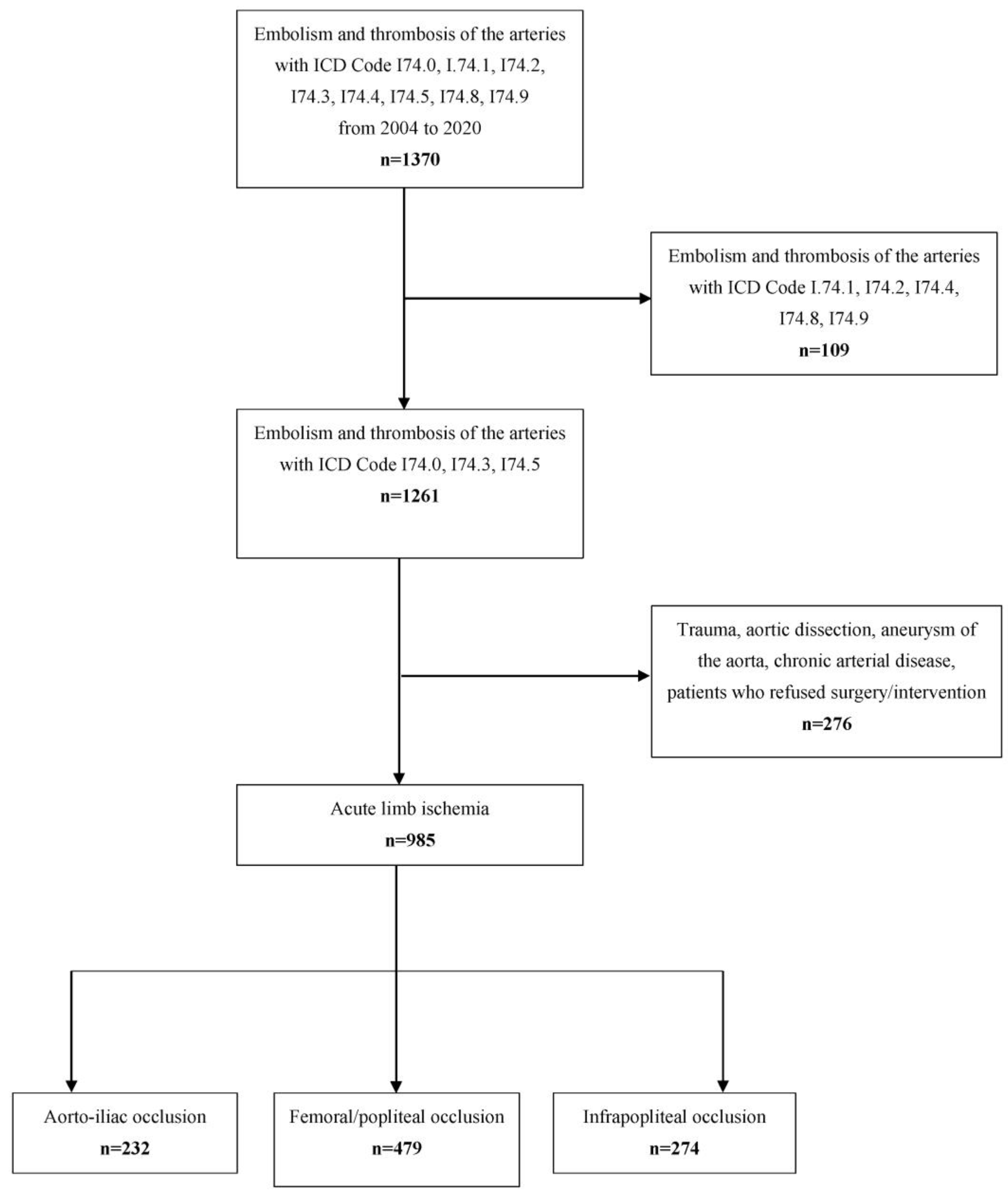
2.1. Inclusion and Exclusion Criteria
2.2. Data Acquisition
2.3. Classification of Acute Limb Ischemia and Treatment Modalities
2.4. Outcome Events
2.5. Statistics
3. Results
3.1. Patient Cohort and Initial Presentation
3.2. Procedural Management
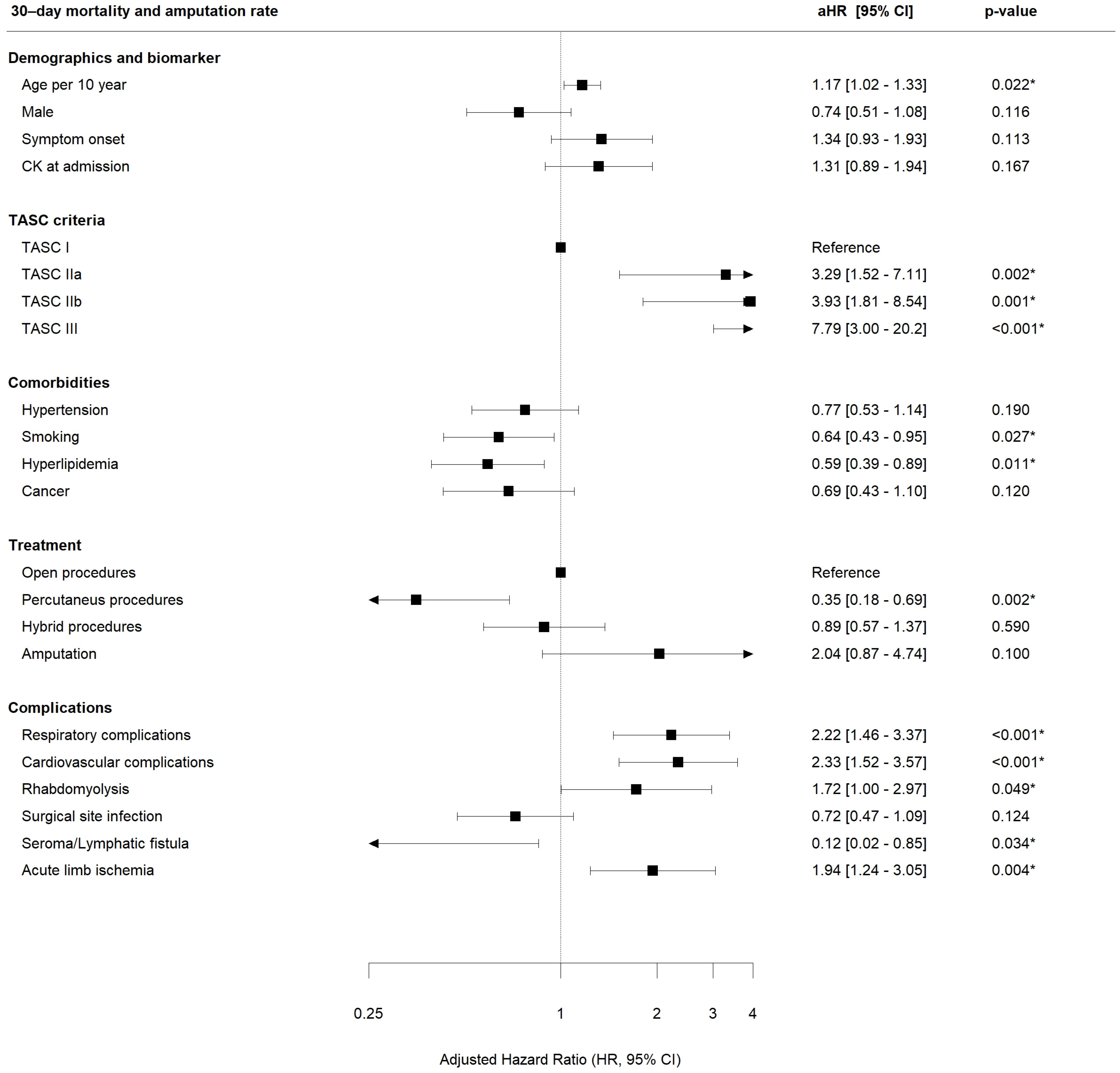
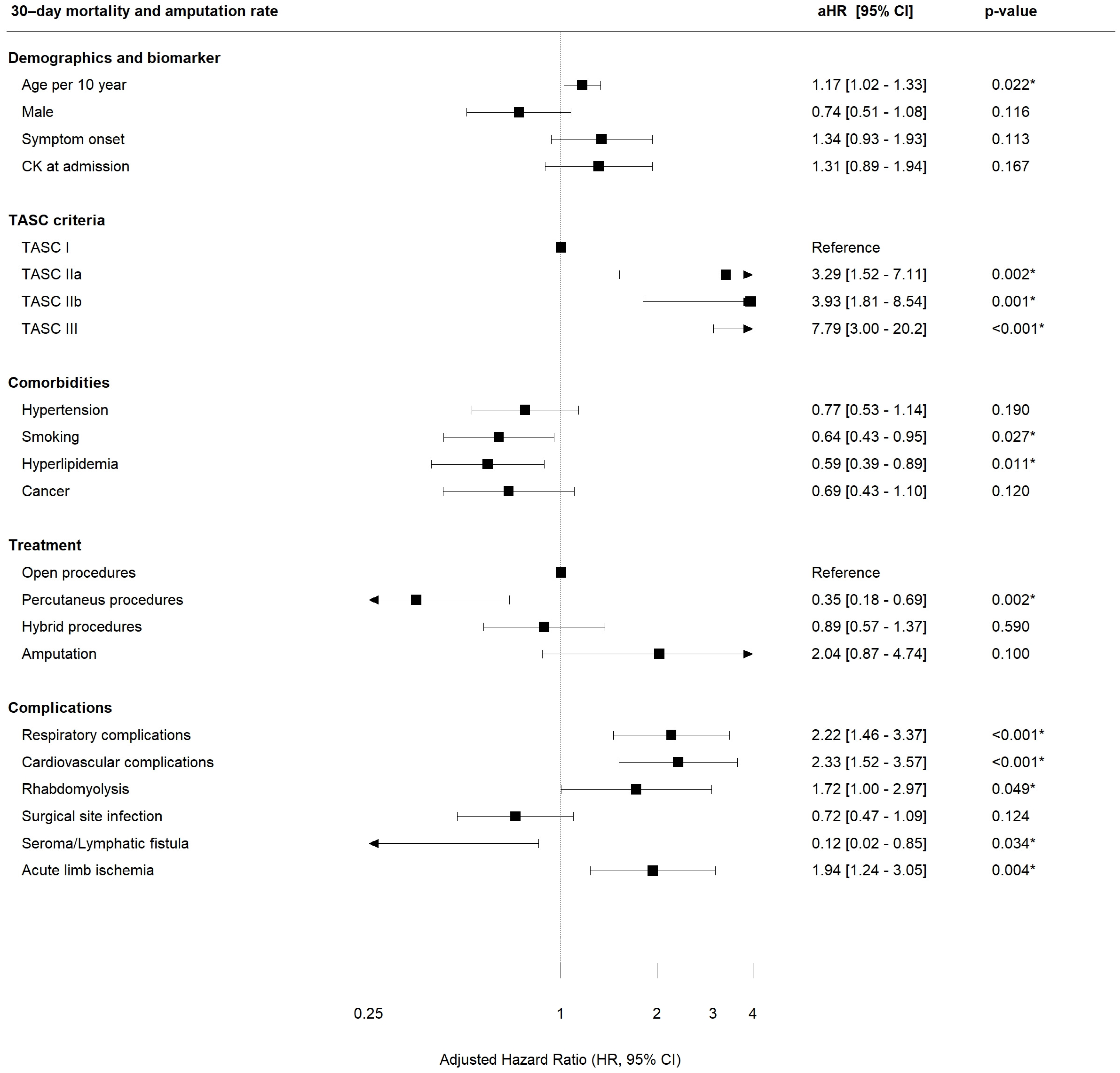
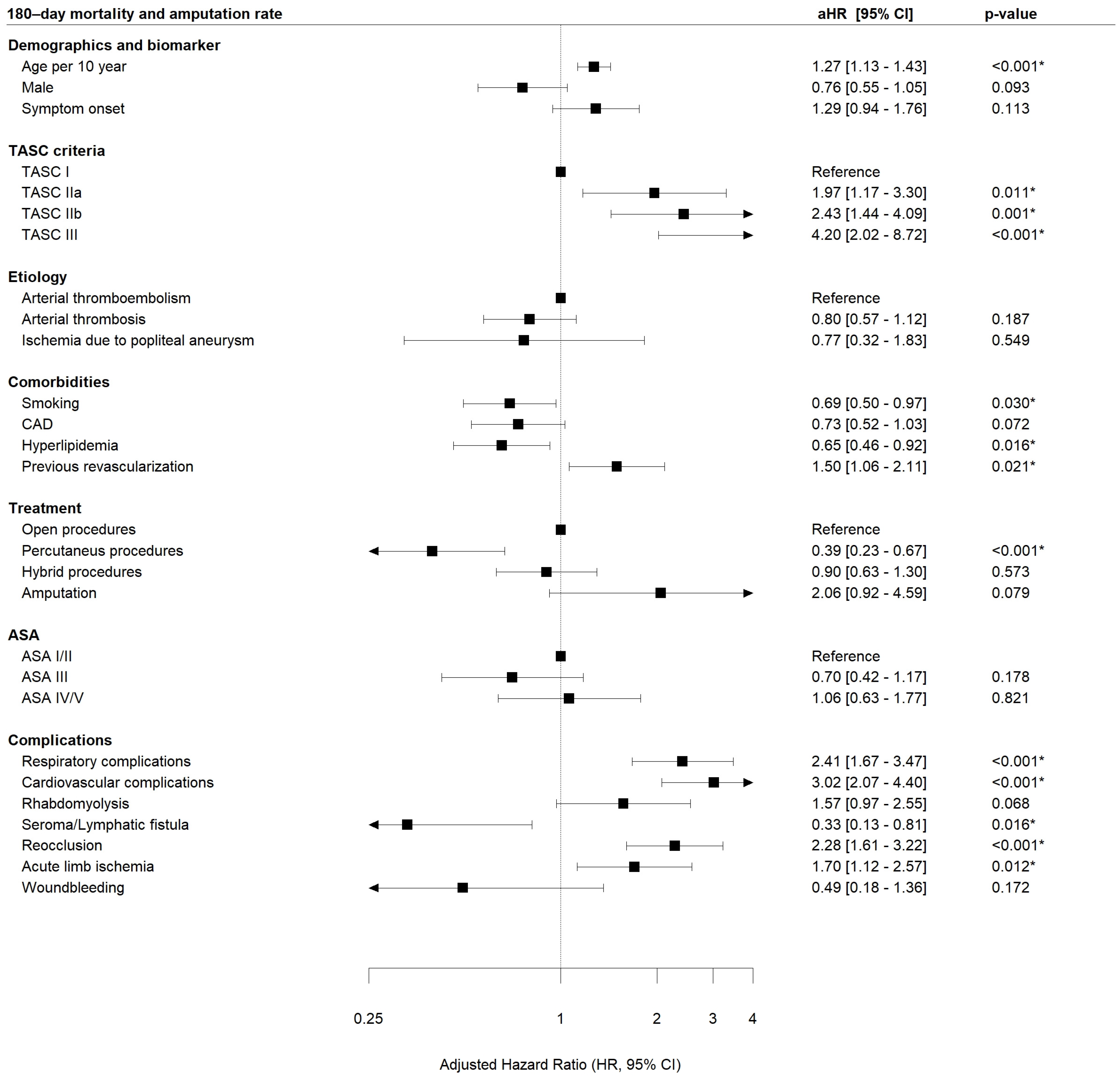
3.3. Outcome Analysis
3.4. Influence of Treatment Modalities on Primary Outcome Events over Time
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Knowles, M.; Timaran, C.H. Epidemiology of acute critical limb ischemia. Crit. Limb Ischemia Acute Chronic 2017, 1–7. [Google Scholar] [CrossRef]
- Creager, M.A.; Kaufman, J.A.; Conte, M.S. Acute limb ischemia. N. Engl. J. Med. 2012, 366, 2198–2206. [Google Scholar] [CrossRef]
- Davies, B.; Braithwaite, B.D.; Birch, P.A.; Poskitt, K.R.; Heather, B.P.; Earnshaw, J.J. Acute leg ischaemia in Gloucestershire. Br. J. Surg. 1997, 84, 504–508. [Google Scholar]
- Genovese, E.A.; Chaer, R.A.; Taha, A.G.; Marone, L.K.; Avgerinos, E.; Makaroun, M.S.; Baril, D.T. Risk Factors for Long-Term Mortality and Amputation after Open and Endovascular Treatment of Acute Limb Ischemia. Ann. Vasc. Surg. 2015, 30, 82–92. [Google Scholar] [CrossRef]
- Norgren, L.; Hiatt, W.R.; Dormandy, J.A.; Nehler, M.R.; Harris, K.A.; Fowkes, F.G.R.; Tasc II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J. Vasc. Surg. 2007, 45, S5–S67. [Google Scholar] [CrossRef]
- Ouriel, K.; Shortell, C.K.; DeWeese, J.A.; Green, R.M.; Francis, C.W.; Azodo, M.V.; Gutierrez, O.H.; Manzione, J.V.; Cox, C.; Marder, V.J. A comparison of thrombolytic therapy with operative revascularization in the initial treatment of acute peripheral arterial ischemia. J. Vasc. Surg. 1994, 19, 1021–1030. [Google Scholar] [CrossRef]
- Baril, D.T.; Patel, V.I.; Judelson, D.R.; Goodney, P.P.; McPhee, J.T.; Hevelone, N.D.; Vascular Study Group of New England. Outcomes of lower extremity bypass performed for acute limb ischemia. J. Vasc. Surg. 2013, 58, 949–956. [Google Scholar] [CrossRef]
- Baril, D.T.; Ghosh, K.; Rosen, A.B. Trends in the incidence, treatment, and outcomes of acute lower extremity ischemia in the United States Medicare population. J. Vasc. Surg. 2014, 60, 669–677.e2. [Google Scholar] [CrossRef]
- Björck, M.; Earnshaw, J.J.; Acosta, S.; Gonçalves, F.B.; Cochennec, F.; Debus, E.; Hinchliffe, R.; Jongkind, V.; Koelemay, M.J.; Menyhei, G.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2020 Clinical Practice Guidelines on the Management of Acute Limb Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 173–218. [Google Scholar] [CrossRef]
- Ouriel, K.; Veith, F.J.; Sasahara, A.A. A comparison of recombinant urokinase with vascular surgery as initial treatment for acute arterial occlusion of the legs. Thrombolysis or Peripheral Arterial Surgery (TOPAS) Investigators. N. Engl. J. Med. 1998, 338, 1105–1111. [Google Scholar] [CrossRef]
- Stile Investigators. Results of a prospective randomized trial evaluating surgery versus thrombolysis for ischemia of the lower extremity. The STILE trial. Ann. Surg. 1994, 220, 251–266; discussion 266–268. [Google Scholar] [CrossRef]
- Weaver, F.A.; Comerota, A.J.; Youngblood, M.; Froehlich, J.; Hosking, J.D.; Papanicolaou, G. Surgical revascularization versus thrombolysis for nonembolic lower extremity native artery occlusions: Results of a prospective randomized trial. The STILE Investigators. Surgery versus Thrombolysis for Ischemia of the Lower Extremity. J. Vasc. Surg. 1996, 24, 513–521; discussion 521–523. [Google Scholar] [CrossRef]
- Han, S.M.; Weaver, F.A.; Comerota, A.J.; Perler, B.A.; Joing, M. Efficacy and safety of alfimeprase in patients with acute peripheral arterial occlusion (PAO). J. Vasc. Surg. 2010, 51, 600–609. [Google Scholar] [CrossRef]
- Nilsson, L.; Albrechtsson, U.; Jonung, T.; Ribbe, E.; Thorvinger, B.; Thörne, J.; Astedt, B.; Norgren, L. Surgical treatment versus thrombolysis in acute arterial occlusion: A randomised controlled study. Eur. J. Vasc. Surg. 1992, 6, 189–193. [Google Scholar] [CrossRef]
- Earnshaw, J.J.; Whitman, B.; Foy, C. National Audit of Thrombolysis for Acute Leg Ischemia (NATALI): Clinical factors associated with early outcome. J. Vasc. Surg. 2004, 39, 1018–1025. [Google Scholar] [CrossRef]
- Kashyap, V.S.; Gilani, R.; Bena, J.F.; Bannazadeh, M.; Sarac, T.P. Endovascular therapy for acute limb ischemia. J. Vasc. Surg. 2011, 53, 340–346. [Google Scholar] [CrossRef]
- Taha, A.G.; Byrne, R.M.; Avgerinos, E.D.; Marone, L.K.; Makaroun, M.S.; Chaer, R.A. Comparative effectiveness of endovascular versus surgical revascularization for acute lower extremity ischemia. J. Vasc. Surg. 2015, 61, 147–154. [Google Scholar] [CrossRef]
- Kempe, K.; Starr, B.; Stafford, J.M.; Islam, A.; Mooney, A.; Lagergren, E.; Corriere, M.A.; Edwards, M.S. Results of surgical management of acute thromboembolic lower extremity ischemia. J. Vasc. Surg. 2014, 60, 702–707. [Google Scholar] [CrossRef]
- Grip, O.; Wanhainen, A.; Michaëlsson, K.; Lindhagen, L.; Björck, M. Open or endovascular revascularization in the treatment of acute lower limb ischaemia. J. Br. Surg. 2018, 105, 1598–1606. [Google Scholar] [CrossRef]
- Yang, P.-K.; Su, C.-C.; Hsu, C.-H. Clinical outcomes of surgical embolectomy versus catheter-directed thrombolysis for acute limb ischemia: A nationwide cohort study. J. Thromb. Thrombolysis 2021, 53, 517–522. [Google Scholar] [CrossRef]
- Enezate, T.H.; Omran, J.; Mahmud, E.; Patel, M.; Abu-Fadel, M.S.; White, C.J.; Al-Dadah, A.S. Endovascular versus surgical treatment for acute limb ischemia: A systematic review and meta-analysis of clinical trials. Cardiovasc. Diagn. Ther. 2017, 7, 264–271. [Google Scholar] [CrossRef]
- Veenstra, E.B.; van der Laan, M.J.; Zeebregts, C.J.; de Heide, E.-J.; Kater, M.; Bokkers, R.P. A systematic review and meta-analysis of endovascular and surgical revascularization techniques in acute limb ischemia. J. Vasc. Surg. 2020, 71, 654–668.e3. [Google Scholar] [CrossRef]
- Wang, J.C.; Kim, A.H.; Kashyap, V.S. Open surgical or endovascular revascularization for acute limb ischemia. J. Vasc. Surg. 2015, 63, 270–278. [Google Scholar] [CrossRef]
- Rutherford, R.B.; Baker, J.; Ernst, C.; Johnston, K.; Porter, J.M.; Ahn, S.; Jones, D.N. Recommended standards for reports dealing with lower extremity ischemia: Revised version. J. Vasc. Surg. 1997, 26, 517–538. [Google Scholar] [CrossRef]
- Fashandi, A.Z.; Mehaffey, J.H.; Hawkins, R.B.; Kron, I.L.; Upchurch, G.R.; Robinson, W.P. Major adverse limb events and major adverse cardiac events after contemporary lower extremity bypass and infrainguinal endovascular intervention in patients with claudication. J. Vasc. Surg. 2018, 68, 1817–1823. [Google Scholar] [CrossRef]
- Sieber, S.; Stoklasa, K.; Reutersberg, B.; Stadlbauer, T.; Salvermoser, M.; Lang, T.; Busch, A.; Eckstein, H.-H. Acute abdominal aortic occlusion: A 16-year single-center experience. J. Vasc. Surg. 2021, 74, 1894–1903.e3. [Google Scholar] [CrossRef]
- Kulezic, A.; Acosta, S. Epidemiology and prognostic factors in acute lower limb ischaemia: A population based study. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 296–303. Available online: https://www.ejves.com/article/S1078-588400829-7/fulltext (accessed on 15 October 2021). [CrossRef]
- Trenner, M.; Knappich, C.; Bohmann, B.; Heuberger, S.; Eckstein, H.-H.; Kuehnl, A. Utilization and Regional Differences of In-Patient Services for Peripheral Arterial Disease and Acute Limb Ischemia in Germany: Secondary Analysis of Nationwide DRG Data. J. Clin. Med. 2022, 11, 2116. [Google Scholar] [CrossRef]
- Moll, M.A.; Zwerger, D.; Grassl, K.J.; Westreicher, W.; Neururer, S.B.; Moll, C.W.; Klocker, J. Prevalence of VOYAGER PAD trial exclusion criteria in unselected patients undergoing lower limb revascularisation. Int. Angiol. J. Int. Union Angiol. 2022, 41, 56–62. [Google Scholar]
- Kaplovitch, E.; Collins, A.; McClure, G.; Tse, R.; Bhagirath, V.; Chan, N.; Szalay, D.; Harlock, J.; Anand, S.S. Medical Therapy Following Urgent/Emergent Revascularization in Peripheral Artery Disease Patients (Canadian Acute Limb Ischemia Registry [CANALISE I]). CJC Open 2021, 3, 1325–1332. [Google Scholar] [CrossRef]
- Twine, C.P.; Kakkos, S.K.; Aboyans, V.; Baumgartner, I.; Behrendt, C.-A.; Bellmunt-Montoya, S.; Jilma, B.; Nordanstig, J.; Saratzis, A.; Reekers, J.A.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on Antithrombotic Therapy for Vascular Diseases. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 627–689. [Google Scholar] [CrossRef]
- Andraska, E.A.; Phillips, A.R.; Reitz, K.M.; Asaadi, S.; Ho, J.; McDonald, M.M.; Madigan, M.; Liang, N.; Eslami, M.; Sridharan, N. Young patients without prior vascular disease are at increased risk of limb loss and reintervention after acute limb ischemia. J. Vasc. Surg. 2022, 76, 1354–1363.e1. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Wiklund, O. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Baigent, C.; Blackwell, L.; Emberson, J.; Holland, L.E.; Reith, C.; Bhala, N.; Peto, R.; Barnes, E.H.; Keech, A.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 2010, 376, 1670–1681. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | n = 985 | % |
|---|---|---|
| Age (years, median, Q1-Q3) | 71 (62–80) | - |
| Male | 555 | 56.3% |
| Symptom onset and biomarker | ||
| Symptom onset (h, median, Q1-Q3) | 24 (6–72) | - |
| CK on admission (U/L, median, Q1-Q3) | 130 (73–412.5) | - |
| Severity of acute limb ischemia at admission (TASC criteria) | ||
| TASC I | 265 | 27% |
| TASC IIa | 347 | 35% |
| TASC IIb | 331 | 34% |
| TASC III | 42 | 4% |
| Etiology | ||
| Arterial thrombosis | 629 | 64% |
| Arterial thromboembolism | 304 | 31% |
| Ischemia due to popliteal aneurysm | 52 | 5% |
| Occlusion Localization | ||
| Aorta-iliac | 232 | 24% |
| Femoral and popliteal arteries | 479 | 49% |
| Infrapopliteal arteries | 274 | 28% |
| Comorbidities | ||
| Hypertension | 687 | 70% |
| Smoking | 454 | 46% |
| PAD | 437 | 44% |
| CAD | 370 | 38% |
| Atrial fibrillation | 287 | 29% |
| Hypercholesterolemia | 456 | 46% |
| Diabetes | 229 | 23% |
| COPD | 98 | 10% |
| Renal insufficiency | 179 | 18% |
| Previous Stroke | 140 | 14% |
| Previous Cancer | 189 | 19% |
| Previous revascularization (same leg) | 506 | 51% |
| ASA Classification | ||
| ASA I/II | 151 | 15% |
| ASA III | 388 | 39% |
| ASA IV/V | 446 | 45% |
| Total | 1st 200 | 2nd 200 | 3rd 200 | 4th 200 | Last 185 | p | Trend | |
|---|---|---|---|---|---|---|---|---|
| 985 | 200 | 200 | 200 | 200 | 185 | |||
| Severity of acute limb ischemia at admission (TASC criteria) | ||||||||
| TASC I n (%) | 265 (26.9) | 49 (24.5) | 44 (22.0) | 45 (22.5) | 59 (29.5) | 68 (36.8) | 0.002 | ↑ |
| TASC IIa n (%) | 347 (35.2) | 87 (43.5) | 70 (35.0) | 84 (42.0) | 49 (24.5) | 57 (30.8) | 0.001 | ↓ |
| TASC IIb n (%) | 331 (33.6) | 56 (28.0) | 80 (40.0) | 62 (31.0) | 77 (38.5) | 56 (30.3) | 0.734 | ↔ |
| TASC III n (%) | 42 (4.26) | 8 (4.00) | 6 (3.00) | 9 (4.50) | 15 (7.50) | 4 (2.16) | 0.798 | ↑ |
| Etiology | ||||||||
| Arterial thrombosis n (%) | 629 (63.9) | 94 (47.0) | 103 (51.5) | 127 (63.5) | 155 (77.5) | 150 (81.1) | <0.001 | ↑ |
| Arterial thromboembolism n (%) | 304 (30.9) | 90 (45.0) | 85 (42.5) | 67 (33.5) | 37 (18.5) | 25 (13.5) | <0.001 | ↓ |
| Ischemia due to popliteal aneurysm n (%) | 52 (5.28) | 16 (8.00) | 12 (6.00) | 6 (3.00) | 8 (4.00) | 10 (5.41) | 0.143 | ↓ |
| Occlusion Localization | ||||||||
| Aorta-iliac n (%) | 232 (23.6) | 40 (20.0) | 58 (29.0) | 54 (27.0) | 41 (20.5) | 39 (21.1) | 0.523 | ↓ |
| Femoral and popliteal arteries n (%) | 479 (48.6) | 119 (59.5) | 97 (48.5) | 98 (49.0) | 70 (35.0) | 95 (51.4) | 0.006 | ↓ |
| Infrapopliteal arteries n (%) | 274 (27.8) | 41 (20.5) | 45 (22.5) | 48 (24.0) | 89 (44.5) | 51 (27.6) | <0.001 | ↑ |
| Previous revascularization (same leg, any level) | 506 (51.4) | 64 (32.0) | 86 (43.0) | 96 (48.0) | 129 (64.5) | 131 (70.8) | <0.001 | ↑ |
| Treatment | ||||||||
| Open procedures n (%) | 535 (54.3) | 133 (66.5) | 105 (52.5) | 118 (59.0) | 111 (55.5) | 67 (36.2) | <0.001 | ↓ |
| Endovascular procedures n (%) | 192 (19.5) | 35 (17.5) | 26 (13.0) | 31 (15.5) | 28 (14.0) | 73 (39.5) | <0.001 | ↑ |
| Hybrid procedures n (%) | 238 (24.2) | 30 (15.0) | 66 (33.0) | 44 (22.0) | 56 (28.0) | 42 (22.7) | 0.260 | ↔ |
| Primary amputation n (%) | 20 (2.03) | 2 (1.00) | 3 (1.50) | 7 (3.50) | 5 (2.50) | 3 (1.62) | 0.458 | ↔ |
| Primary outcome events (POE) * | ||||||||
| 30-day mortality and amputation rate (safety endpoint) n (%) | 141 (15.3) | 32 (17.7) | 31 (16.1) | 31 (16.0) | 26 (13.8) | 21 (12.5) | 0.136 | ↓ |
| 180-day mortality and amputation rate (efficacy endpoint) n (%) | 201 (27.4) | 44 (26.8) | 43 (26.7) | 46 (30.2) | 37 (25.3) | 31 (27.9) | 0.946 | ↔ |
| 30-day mortality rate | 80 (8.66) | 15 (8.29) | 22 (11.5) | 16 (8.25) | 15 (7.94) | 12 (7.14) | 0.376 | ↓ |
| 30-day amputation rate | 79 (8.55) | 19 (10.5) | 15 (7.81) | 18 (9.28) | 14 (7.41) | 13 (7.74) | 0.372 | ↔ |
| Leg-related complications | ||||||||
| Surgical site infection n (%) | 184 (18.7) | 47 (23.5) | 31 (15.5) | 42 (21.0) | 41 (20.5) | 23 (12.4) | 0.059 | ↔ |
| Seroma/Lymphatic fistula n (%) | 57 (5.79) | 25 (12.5) | 4 (2.00) | 12 (6.00) | 11 (5.50) | 5 (2.70) | 0.002 | ↓ |
| Re-occlusion n (%) | 184 (18.7) | 32 (16.0) | 32 (16.0) | 27 (13.5) | 31 (15.5) | 62 (33.5) | <0.001 | ↑ |
| Acute limb ischemia n (%) | 105 (10.7) | 16 (8.00) | 11 (5.50) | 11 (5.50) | 14 (7.00) | 53 (28.6)) | <0.001 | ↑ |
| Wound bleeding n (%) | 36 (3.65) | 4 (2.00) | 9 (4.50) | 8 (4.00) | 9 (4.50) | 6 (3.24) | 0.537 | ↔ |
| Systemic complications | ||||||||
| Respiratory complications n (%) | 106 (10.8) | 18 (9.00) | 21 (10.5) | 21 (10.5) | 25 (12.5) | 21 (11.4) | 0.332 | ↑ |
| Renal complications n (%) | 88 (8.93) | 18 (9.00) | 22 (11.0) | 19 (9.50) | 16 (8.00) | 13 (7.03) | 0.289 | ↓ |
| Cardiovascular complications n (%) | 125 (12.7) | 30 (15.0) | 32 (16.0) | 28 (14.0) | 16 (8.00) | 19 (10.3) | 0.020 | ↓ |
| Rhabdomyolysis n (%) | 47 (4.77) | 15 (7.50) | 13 (6.50) | 4 (2.00) | 6 (3.00) | 9 (4.86) | 0.061 | ↓ |
| n | % | |
|---|---|---|
| Open surgical procedures | 535 | 54% |
| Bypass surgery or interposition graft * | 168 | 17% |
| Embolectomy/thrombectomy * | 353 | 36% |
| Thrombendarterectomy | 14 | 1% |
| Percutaneous endovascular transfemoral recanalization * | 192 | 20% |
| Local catheter-guided thrombolysis | 102 | 11% |
| - 24 h | 84 | 82% |
| - 48 h | 18 | 18% |
| Angioplasty/Thrombectomy (Ballon-/Stentangioplasty, Aspiration, Rotarex, etc.) | 90 | 9% |
| Hybrid procedures * | 238 | 24% |
| Primary amputation | 20 | 2% |
| Additional procedures | ||
| Fasciotomy | 351 | 36% |
| - immediately | 291 | 83% |
| - delayed | 60 | 17% |
| Minor amputation | 6 | 1% |
| Procedure time (hours, median, IQR) | 150.5 | (90–260.75) |
| Length of stay (days, median, IQR) | 10 (6–18) | - |
| Primary outcome events (POE, including single components) | ||
| 30-day-mortality | 80 | 9% |
| 30-day-amputation | 79 | 9% |
| Combined 30-day mortality and amputation | 141 | 15% |
| - after open surgical procedure | 88 | 62.4% |
| - after percutaneous endovascular transfemoral recanalization | 12 | 8.5% |
| - after hybrid procedure | 30 | 21.3% |
| - after primary amputation | 11 | 7.8% |
| Combined 180-day mortality and amputation | 201 | 27% |
| - after open surgical procedure | 122 | 60.7% |
| - after percutaneous endovascular transfemoral recanalization | 20 | 10% |
| - after hybrid procedure | 46 | 22.9% |
| - after primary amputation | 13 | 6.4% |
| Systemic complications (during hospital stay) | ||
| Respiratory complications | 106 | 11% |
| Renal complications | 88 | 9% |
| Cardiovascular complications | 125 | 13% |
| MACE | 33 | 13.5% |
| Rhabdomyolysis | 47 | 5% |
| Local complications (during hospital stay) | ||
| Re-occlusion | 184 | 19% |
| Acute limb ischemia | 105 | 11% |
| MALE | 305 | 30.5% |
| Surgical site infection | 184 | 19% |
| Seroma/lymphatic fistula | 66 | 6% |
| Wound bleeding | 36 | 4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stoklasa, K.; Sieber, S.; Naher, S.; Bohmann, B.; Kuehnl, A.; Stadlbauer, T.; Wendorff, H.; Biro, G.; Kallmayer, M.A.; Knappich, C.; et al. Patients with Acute Limb Ischemia Might Benefit from Endovascular Therapy—A 17-Year Retrospective Single-Center Series of 985 Patients. J. Clin. Med. 2023, 12, 5462. https://doi.org/10.3390/jcm12175462
Stoklasa K, Sieber S, Naher S, Bohmann B, Kuehnl A, Stadlbauer T, Wendorff H, Biro G, Kallmayer MA, Knappich C, et al. Patients with Acute Limb Ischemia Might Benefit from Endovascular Therapy—A 17-Year Retrospective Single-Center Series of 985 Patients. Journal of Clinical Medicine. 2023; 12(17):5462. https://doi.org/10.3390/jcm12175462
Chicago/Turabian StyleStoklasa, Kerstin, Sabine Sieber, Shamsun Naher, Bianca Bohmann, Andreas Kuehnl, Thomas Stadlbauer, Heiko Wendorff, Gabor Biro, Michael A. Kallmayer, Christoph Knappich, and et al. 2023. "Patients with Acute Limb Ischemia Might Benefit from Endovascular Therapy—A 17-Year Retrospective Single-Center Series of 985 Patients" Journal of Clinical Medicine 12, no. 17: 5462. https://doi.org/10.3390/jcm12175462
APA StyleStoklasa, K., Sieber, S., Naher, S., Bohmann, B., Kuehnl, A., Stadlbauer, T., Wendorff, H., Biro, G., Kallmayer, M. A., Knappich, C., Busch, A., & Eckstein, H.-H. (2023). Patients with Acute Limb Ischemia Might Benefit from Endovascular Therapy—A 17-Year Retrospective Single-Center Series of 985 Patients. Journal of Clinical Medicine, 12(17), 5462. https://doi.org/10.3390/jcm12175462