
Dysnatremia in COVID-19 Patients—An Analysis of the COLOS Study
 ,
,  ,
,  , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Follow Up and Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Univariate Analyses
3.3. Kaplan-Meyer Curve
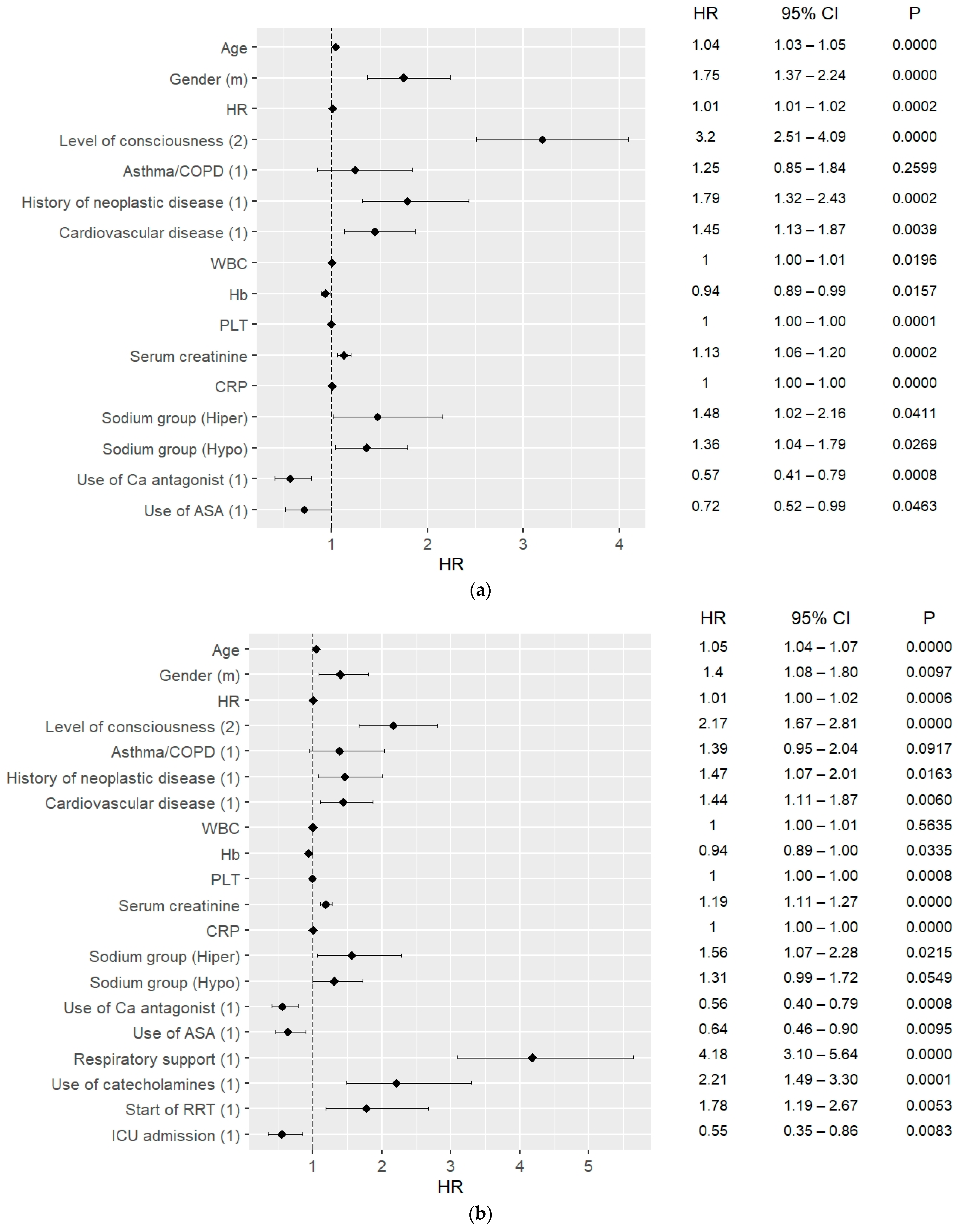
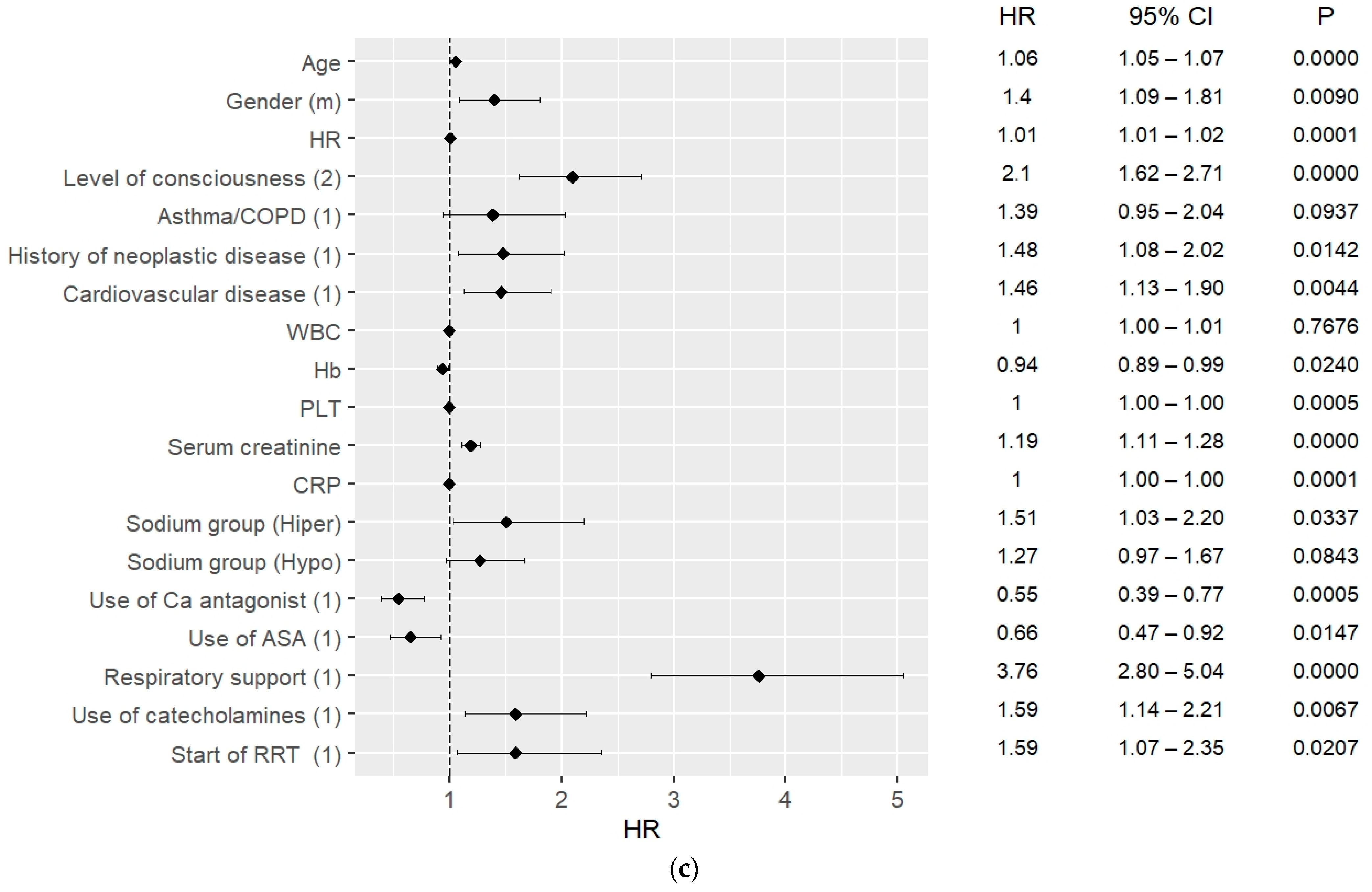
3.4. 30-Day and 90-Day Mortality Predictors
3.5. ICU Admission Predictors
3.6. Possible Dysnatremia Predictors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peri, A. Morbidity and Mortality of Hyponatremia. Front. Horm. Res. 2019, 52, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Muhsin, S.A.; Mount, D.B. Diagnosis and treatment of hypernatremia. Best Pract. Res. Clin. Endocrinol. Metab. 2016, 30, 189–203. [Google Scholar] [CrossRef] [PubMed]
- Lindner, G.; Funk, G.-C. Hypernatremia in critically ill patients. J. Crit. Care 2013, 28, 216.e11–216.e20. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, K.; Pattharanitima, P.; Patel, N.; Duffy, A.; Saha, A.; Chaudhary, K.; Debnath, N.; Van Vleck, T.; Chan, L.; Nadkarni, G.N.; et al. Rate of Correction of Hypernatremia and Health Outcomes in Critically Ill Patients. Clin. J. Am. Soc. Nephrol. 2019, 14, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Tzoulis, P.; Grossman, A.B.; Baldeweg, S.E.; Bouloux, P.; Kaltsas, G. Management of Endocrine Disease: Dysnatraemia in COVID-19: Prevalence, prognostic impact, pathophysiology, and management. Eur. J. Endocrinol. 2021, 185, R103–R111. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Sánchez, J.G.; Núñez-Gil, I.J.; Cuesta, M.; Rubio, M.A.; Maroun-Eid, C.; Arroyo-Espliguero, R.; Romero, R.; Becerra-Muñoz, V.M.; Uribarri, A.; Feltes, G.; et al. Prognostic Impact of Hyponatremia and Hypernatremia in COVID-19 Pneumonia. A HOPE-COVID-19 (Health Outcome Predictive Evaluation for COVID-19) Registry Analysis. Front. Endocrinol. 2020, 11, 599255. [Google Scholar] [CrossRef]
- Hoorn, E.J.; Zietse, R. Diagnosis and Treatment of Hyponatremia: Compilation of the Guidelines. J. Am. Soc. Nephrol. 2017, 28, 1340–1349. [Google Scholar] [CrossRef]
- Corona, G.; Giuliani, C.; Verbalis, J.G.; Forti, G.; Maggi, M.; Peri, A. Hyponatremia Improvement Is Associated with a Reduced Risk of Mortality: Evidence from a Meta-Analysis. PLoS ONE 2015, 10, e0124105. [Google Scholar] [CrossRef] [PubMed]
- Chewcharat, A.; Thongprayoon, C.; Cheungpasitporn, W.; Mao, M.A.; Thirunavukkarasu, S.; Kashani, K.B. Trajectories of Serum Sodium on In-Hospital and 1-Year Survival among Hospitalized Patients. Clin. J. Am. Soc. Nephrol. 2020, 15, 600–607. [Google Scholar] [CrossRef] [PubMed]
- de La Flor, J.C.; Gomez-Berrocal, A.; Marschall, A.; Valga, F.; Linares, T.; Albarracin, C.; Ruiz, E.; Gallegos, G.; Gómez, A.; de Los Santos, A.; et al. Smart RBN. The impact of the correction of hyponatremia during hospital admission on the prognosis of SARS-CoV-2 infection. Ann. Oncol. 2020, 159, 19–21. [Google Scholar]
- Czapla, M.; Uchmanowicz, I.; Juárez-Vela, R.; Durante, A.; Kałużna-Oleksy, M.; Łokieć, K.; Baeza-Trinidad, R.; Smereka, J. Relationship between nutritional status and length of hospital stay among patients with atrial fibrillation—A result of the nutritional status heart study. Front. Nutr. 2022, 9, 1086715. [Google Scholar] [CrossRef] [PubMed]
- Eskandar, E.N.; Altschul, D.J.; Ramos, R.D.L.G.; Cezayirli, P.; Unda, S.R.; Benton, J.; Dardick, J.; Toma, A.; Patel, N.; Malaviya, A.; et al. Neurologic Syndromes Predict Higher In-Hospital Mortality in COVID-19. Neurology 2020, 96, e1527–e1538. [Google Scholar] [CrossRef] [PubMed]
- Marin, B.G.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.B.; South, A.M.; Shaltout, H.A.; Sinclair, M.R.; Sparks, M.A. Renin–angiotensin system blockade in the COVID-19 pandemic. Clin. Kidney J. 2021, 14 (Suppl. S1), i48–i59. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, B.; Fernandes, S. Bacterial coinfection and secondary infection in patient with COVID-19. Diabetes Metab. Syndr. 2020, 14, 8. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All | Normonatremia | Hyponatremia | Hypernatremia | p-Value (ANOVA/Chi Square) | Hypo vs. Normo | Hyper vs. Normo | Hypo vs. Hyper |
|---|---|---|---|---|---|---|---|---|
| Mean ± SD; median (Q1–Q3) or n (%) | 1570 (77.49%) | 354 (17.47%) | 102 (5.03%) | |||||
| Age, yr. | 61.21 ± 18.21 | 59.34 ± 18.55 | 66.70 ± 15.10 | 70.96 ± 15.86 | 0.0000 w | 0.0000 | 0.0000 | 0.2036 |
| 65.0 (48.0–74.0) | 63.00 (45.00–73.00) | 68.00 (61.00–77.00) | 70.50 (63.00–83.00) | |||||
| Gender | ||||||||
| Male | 1021 (50.4%) | 767 (48.9%) | 197 (55.6%) | 57 (55.9%) | 0.0363 | |||
| Female | 1005 (49.6%) | 803 (51.1%) | 157 (44.4%) | 45 (44.1%) | ||||
| Vital signs | ||||||||
| Systolic BP, mm Hg | 132.10 ± 22.93 | 132.33 ± 22.46 | 134.28 ± 23.13 | 121.13 ± 26.72 | 0.0000 | 0.2033 | 0.0000 | 0.0000 |
| 130.0 (120.0–145.0) | 130.0 (120.0–144.0) | 130.0 (120.0–150.0) | 122.5 (110.0–134.0) | |||||
| Diastolic BP | 78.02 ± 13.41 | 78.21 ± 13.10 | 78.11 ± 13.07 | 74.54 ± 18.51 | 0.2389 w | |||
| 80.0 (70.0–85.0) | 80.0 (70.0–85.0) | 80.0 (70.0–85.0) | 72.5 (60.0–85.5) | |||||
| Heart rate, BPM | 85.64 ± 16.38 | 84.97 ± 15.71 | 87.53 ± 17.14 | 90.04 ± 22.39 | 0.0164 w | 0.0198 | 0.0075 | 0.2300 |
| 82.0 (75.0–94.0) | 81.0 (75.0–92.0) | 83.0 (76.0–96.0) | 82.0 (74.0–105.0) | |||||
| Impaired consciousness | 323 (15.6%) | 197 (12.56%) | 60 (16.95%) | 66 (64.71%) | 0.0000 | |||
| Comorbidities | ||||||||
| Hypertension | 988 (48.8%) | 730 (46.5%) | 204 (57.6%) | 54 (52.9%) | 0.0005 | |||
| History of myocardial infarction | 189 (9.3%) | 134 (8.5%) | 47 (13.3%) | 8 (7.8%) | 0.0187 | |||
| Heart failure | 250 (12.3%) | 174 (11.1%) | 59 (16.7%) | 17 (16.7%) | 0.0061 | |||
| History of stroke or TIA | 160 (7.9%) | 116 (7.4%) | 32 (9.0%) | 12 (11.8%) | 0.1929 | |||
| Diabetes mellitus | 467 (23.1%) | 331 (21.1%) | 112 (31.7%) | 24 (23.5%) | 0.0001 | |||
| Chronic kidney disease | 226 (11.2%) | 165 (10.5%) | 47 (13.3%) | 14 (13.7%) | 0.2290 | |||
| Chronic obstructive pulmonary disease or asthma | 148 (7.3%) | 110 (7.0%) | 28 (7.9%) | 10 (9.8%) | 0.5121 | |||
| Peripheral occlusive arterial disease | 99 (4.9%) | 69 (4.4%) | 24 (6.8%) | 6 (5.9%) | 0.1523 | |||
| History of cancer | 196 (9.7%) | 147 (9.4%) | 37 (10.5%) | 12 (11.8%) | 0.6284 | |||
| Charlson Comorbidity Index | 3.25 ± 2.69 | 3.00 ± 2.65 | 3.98 ± 2.65 | 4.45 ± 2.64 | 0.0000 | |||
| 3(1–5) | 3 (1–5) | 4(2–5) | 4(2–6) | |||||
| Drugs | ||||||||
| ACEI/ARB/ARNI | 492 (24.3%) | 355 (22.6%) | 112 (31.6%) | 25 (24.5%) | 0.0017 | |||
| Beta-blockers | 522 (25.8%) | 383 (24.4%) | 111 (31.4%) | 28 (27.5%) | 0.0238 | |||
| Calcium blockers | 289 (14.3%) | 217 (13.8%) | 55 (15.5%) | 17 (16.7%) | 0.5484 | |||
| Mineral receptor antagonists | 100 (4.9%) | 74 (4.7%) | 24 (6.8%) | 2 (2.0%) | 0.0976 | |||
| Diuretics | 317 (15.7%) | 226 (14.4%) | 76 (21.5%) | 15 (14.7%) | 0.0040 | |||
| Statins | 349 (17.2%) | 270 (17.2%) | 59 (16.7%) | 20 (19.6%) | 0.7849 | |||
| Acetylsalicylic acid | 254 (12.5%) | 195 (12.4%) | 47 (13.3%) | 12 (11.8%) | 0.8818 | |||
| Anticoagulants | 282 (13.9%) | 203 (12.9%) | 58 (16.4%) | 21 (20.6%) | 0.0323 | |||
| Steroids or immunosuppressants | 119 (5.9%) | 99 (6.3%) | 18 (5.1%) | 2 (2.0%) | 0.1531 | |||
| Laboratory values | ||||||||
| White blood cell count, 103/mL | 9.14 ± 11.72 | 8.98 ± 12.75 | 8.88 ± 6.57 | 12.45 ± 8.19 | 0.0135 | 0.8798 | 0.0038 | 0.0067 |
| 7.36 (5.37–10.30) | 7.21 (5.30–9.99) | 7.30 (5.17–10.77) | 10.59 (7.82–14.88) | |||||
| Hemoglobin, g/dL | 12.93 ± 2.29 | 12.94 ± 2.25 | 12.84 ± 2.43 | 12.98 ± 2.42 | 0.7570 w | |||
| 13.10 (11.70–14.50) | 13.20 (11.90–14.40) | 13.05 (11.20–14.7) | 13.15 (11.40–14.20) | |||||
| Platelets, 103/L | 232.17 ± 108.40 | 232.19 ± 107.53 | 230.32 ± 114.69 | 238.20 ± 99.85 | 0.8116 | |||
| 211.00 (163.00–282.00) | 211.0 (164.0–282.0) | 204.5 (160.0–275.0) | 229.0 (173.0–300.0) | |||||
| Sodium, mEq/L | 138.08 ± 5.45 | 139.04 ± 2.55 | 130.39 ± 5.27 | 150.14 ± 5.45 | 0.0000 | |||
| 138.00 (136.00–141.00) | 139.0 (137.0–141.0) | 132.0 (129.0–134.0) | 148.0 (147.0–152.0) | |||||
| Serum creatinine, mg/dL | 1.32 ± 1.30 | 1.26 ± 1.22 | 1.47 ± 1.52 | 1.70 ± 1.52 | 0.0017 w | 0.0063 | 0.0008 | 0.1070 |
| 0.94 (0.76–1.28) | 0.92 (0.75–1.22) | 1.00 (0.82–1.46) | 1.11 (0.83–2.06) | |||||
| CRP | 78.67 ± 84.77 | 70.63 ± 78.25 | 97.96 ± 93.02 | 133.39 ± 114.57 | 0.0000 w | 0.0000 | 0.0000 | 0.0002 |
| 49.28 (13.27–116.40) | 43.36 (10.03–105.07) | 68.69 (27.52–141.25) | 99.05 (46.00–203.60) | |||||
| In-hospital procedures | ||||||||
| ICU admission | 212 (10.5%) | 144 (9.2%) | 46 (13.0%) | 22 (21.6%) | 0.0001 | |||
| Respiratory support | 383 (18.9%) | 273 (17.4%) | 75 (21.3%) | 35 (34.3%) | 0.0001 | |||
| No support | 887 (43.85%) | 736 (46.94%) | 131 (37.11%) | 20 (19.61%) | ||||
| Passive oxygen therapy | 753 (37.22%) | 559 (35.65%) | 147 (41.64%) | 47 (46.08%) | ||||
| HFNC | 131 (6.48%) | 99 (6.31%) | 22 (6.23%) | 10 (9.80%) | ||||
| BiPAP/CPAP | 42 (2.08%) | 27 (1,72%) | 13 (3.68%) | 2 (1.96%) | ||||
| Respiratory therapy | 210 (10.38%) | 147 (9.38%) | 40 (11.33%) | 23 (22.55%) | ||||
| Vasopressors | 217 (10.7%) | 147 (9.4%) | 41 (11.6%) | 29 (28.4%) | 0.0000 | |||
| Intravenous loop diuretic | 333 (16.4%) | 229 (14.6%) | 72 (20.3%) | 32 (31.4%) | 0.0000 | |||
| Start of renal replacement therapy | 72 (3.6%) | 45 (2.9%) | 17 (14.8%) | 10 (9.8%) | 0.0005 | |||
| Steroids | 1090 (53.8%) | 834 (53.1%) | 194 (54.8%) | 62 (60.8%) | 0.2958 | |||
| Antibiotics | 1229 (60.7%) | 931 (59.3%) | 213 (60.2%) | 85 (83.3%) | 0.0000 | |||
| 30-Day Mortality Predictors | 90-Day Mortality Predictors | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | Hazard Ratio (HR) | Standard Error (SE) | 95% HR Lower Bound | 95% HR Upper Bound | p Value | Hazard Ratio (HR) | Standard Error (SE) | 95% HR Lower Bound | 95% HR Upper Bound | p Value |
| Hyponatremia | 1.69 | 0.10 | 1.29 | 2.21 | 0.4204 | 1.60 | 0.09 | 1.26 | 2.04 | 0.1657 |
| Hypernatremia | 3.63 | 0.12 | 2.54 | 5.20 | 0.0000 | 3.73 | 0.11 | 2.71 | 5.14 | 0.0000 |
| Demographic data and vital signs | ||||||||||
| Age | 1.05 | 0.00 | 1.04 | 1.06 | 0.0000 | 1.05 | 0.00 | 1.05 | 1.06 | 0.0000 |
| Sex (female) | 1.54 | 0.06 | 1.22 | 1.94 | 0.0002 | 0.73 | 0.05 | 0.59 | 0.89 | 0.0019 |
| HR | 1.01 | 0.00 | 1.01 | 1.02 | 0.0000 | 1.01 | 0.00 | 1.01 | 1.02 | 0.0001 |
| SBP | 0.99 | 0.00 | 0.99 | 1.00 | 0.0153 | 1.00 | 0.00 | 0.99 | 1.00 | 0.0448 |
| DBP | 0.97 | 0.00 | 0.96 | 0.98 | 0.0000 | 0.98 | 0.00 | 0.97 | 0.99 | 0.0000 |
| Consciousness | 5.21 | 0.06 | 4.17 | 6.52 | 0.0000 | 5.13 | 0.05 | 4.20 | 6.27 | 0.0000 |
| Comorbidities | ||||||||||
| Hypertension | 1.89 | 0.06 | 1.49 | 2.40 | 0.0000 | 2.06 | 0.05 | 1.67 | 2.55 | 0.0000 |
| History of myocardial infarction | 2.51 | 0.07 | 1.91 | 3.29 | 0.0000 | 2.52 | 0.06 | 1.97 | 3.22 | 0.0000 |
| History of stroke/TIA | 1.60 | 0.08 | 1.15 | 2.23 | 0.0057 | 1.73 | 0.07 | 1.29 | 2.30 | 0.0002 |
| Diabetes mellitus | 1.68 | 0.06 | 1.33 | 2.13 | 0.0000 | 1.78 | 0.05 | 1.45 | 2.19 | 0.0000 |
| Chronic kidney disease | 2.00 | 0.07 | 1.53 | 2.63 | 0.0000 | 2.24 | 0.06 | 1.77 | 2.83 | 0.0000 |
| Heart failure | 2.55 | 0.06 | 1.99 | 3.27 | 0.0000 | 2.65 | 0.06 | 2.13 | 3.30 | 0.0000 |
| Asthma/COBP | 1.19 | 0.10 | 0.82 | 1.74 | 0.3587 | 1.34 | 0.08 | 0.97 | 1.84 | 0.0748 |
| Peripheral obstructive arterial disease | 2.49 | 0.09 | 1.75 | 3.54 | 0.0000 | 2.23 | 0.08 | 1.60 | 3.10 | 0.0000 |
| History of neoplastic disease | 2.40 | 0.07 | 1.82 | 3.17 | 0.0000 | 2.50 | 0.06 | 1.95 | 3.21 | 0.0000 |
| Cardiovascular disease | 2.62 | 0.06 | 2.10 | 3.28 | 0.0000 | 2.67 | 0.05 | 2.19 | 3.26 | 0.0000 |
| Long-term use of drugs | ||||||||||
| ACEI/ARB/ARNI | 1.12 | 0.06 | 0.88 | 1.42 | 0.3553 | 1.17 | 0.05 | 0.95 | 1.44 | 0.1490 |
| Beta-blockers | 1.33 | 0.06 | 1.06 | 1.67 | 0.0152 | 1.50 | 0.05 | 1.23 | 1.84 | 0.0001 |
| Calcium antagonists | 0.77 | 0.08 | 0.56 | 1.07 | 0.1162 | 0.95 | 0.07 | 0.73 | 1.24 | 0.6906 |
| MRAs | 1.24 | 0.11 | 0.82 | 1.88 | 0.3155 | 1.56 | 0.09 | 1.11 | 2.19 | 0.0098 |
| Diuretics | 1.45 | 0.07 | 1.12 | 1.87 | 0.0052 | 1.55 | 0.06 | 1.24 | 1.95 | 0.0001 |
| Statins | 1.24 | 0.07 | 0.96 | 1.61 | 0.1055 | 1.34 | 0.06 | 1.07 | 1.68 | 0.0115 |
| ASA | 0.99 | 0.08 | 0.73 | 1.36 | 0.9686 | 1.08 | 0.07 | 0.83 | 1.42 | 0.5503 |
| Anticoagulants | 1.50 | 0.07 | 1.15 | 1.95 | 0.0030 | 1.62 | 0.06 | 1.29 | 2.05 | 0.0000 |
| GCS/immunosupressants | 1.09 | 0.11 | 0.71 | 1.68 | 0.7003 | 1.19 | 0.09 | 0.82 | 1.73 | 0.3500 |
| Laboratory findings | ||||||||||
| WBC | 1.02 | 0.00 | 1.02 | 1.03 | 0.0000 | 1.02 | 0.00 | 1.02 | 1.02 | 0.0000 |
| Hemoglobin | 0.87 | 0.02 | 0.84 | 0.91 | 0.0000 | 0.87 | 0.02 | 0.83 | 0.90 | 0.0000 |
| PLT | 1.00 | 0.00 | 1.00 | 1.00 | 0.0063 | 1.00 | 0.00 | 1.00 | 1.00 | 0.0024 |
| Creatinine | 1.18 | 0.02 | 1.12 | 1.23 | 0.0000 | 1.17 | 0.02 | 1.13 | 1.22 | 0.0000 |
| CRP | 1.00 | 0.00 | 1.00 | 1.01 | 0.0000 | 1.00 | 0.00 | 1.00 | 1.01 | 0.0000 |
| Sodium | 1.02 | 0.01 | 1.00 | 1.04 | 0.0635 | 1.03 | 0.01 | 1.01 | 1.05 | 0.0082 |
| In-hospital procedures | ||||||||||
| ICU admission | 3.84 | 0.06 | 3.01 | 4.91 | 0.0000 | 3.84 | 0.06 | 3.01 | 4.91 | 0.0000 |
| Respiratory support | 6.05 | 0.06 | 4.84 | 7.58 | 0.0000 | 6.05 | 0.06 | 4.84 | 7.58 | 0.0000 |
| Use of catecholamines | 5.60 | 0.06 | 4.44 | 7.06 | 0.0000 | 5.60 | 0.06 | 4.44 | 7.06 | 0.0000 |
| IV loop diuretic | 3.93 | 0.06 | 3.14 | 4.91 | 0.0000 | 3.93 | 0.06 | 3.14 | 4.91 | 0.0000 |
| Start of RRT | 3.98 | 0.09 | 2.81 | 5.63 | 0.0000 | 3.98 | 0.09 | 2.81 | 5.63 | 0.0000 |
| Use of steroids | 1.29 | 0.06 | 1.02 | 1.63 | 0.0360 | 1.29 | 0.06 | 1.02 | 1.63 | 0.0360 |
| Use of antibiotics | 3.38 | 0.08 | 2.45 | 4.69 | 0.0000 | 3.38 | 0.08 | 2.45 | 4.69 | 0.0000 |
| Univariate Analysis | Multivariate Analysis—Averaged Best Subset Selection Models (with the Use of AIC) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | OR | CI 95 Lower | CI 95 Upper | p | OR | CI 95 Lower | CI 95 Upper | p | |||
| Basic demographic data and vital signs | |||||||||||
| Age | 0.99 | 0.99 | 1.00 | 0.1877 | |||||||
| Sex (M) | 1.94 | 1.38 | 2.72 | 0.0001 | 1.0550 | 1.0231 | 1.0878 | 0.00063 | |||
| HR | 1.00 | 0.99 | 1.01 | 0.7279 | |||||||
| SBP | 0.99 | 0.98 | 1.00 | 0.0099 | 1.0014 | 1.0005 | 1.0023 | 0.00183 | |||
| DBP | 0.95 | 0.94 | 0.96 | 0.0000 | 0.9949 | 0.9934 | 0.9964 | 0.00000 | |||
| Consciousness | 0.18 | 0.13 | 0.25 | 0.0000 | 1.2050 | 1.1558 | 1.2564 | 0.00000 | |||
| Comorbidities | |||||||||||
| Hypertension | 1.28 | 0.92 | 1.76 | 0.1380 | |||||||
| Diabetes mellitus | 1.39 | 0.98 | 1.97 | 0.0626 | |||||||
| Chronic kidney disease | 0.86 | 0.52 | 1.40 | 0.5366 | |||||||
| Asthma/COPD | 1.04 | 0.59 | 1.82 | 0.9022 | |||||||
| History of neoplastic disorder | 0.94 | 0.55 | 1.60 | 0.8170 | |||||||
| Cardiovascular disease | 1.05 | 0.74 | 1.50 | 0.7823 | |||||||
| Laboratory findings | |||||||||||
| WBC | 1.06 | 1.04 | 1.08 | 0.0000 | 1.0037 | 1.0024 | 1.0050 | 0.00000 | |||
| Hemoglobin | 0.94 | 0.88 | 1.01 | 0.0733 | |||||||
| PLT | 1.00 | 1.00 | 1.00 | 0.1625 | |||||||
| Creatinine | 1.03 | 0.92 | 1.16 | 0.6180 | |||||||
| CRP | 1.01 | 1.01 | 1.01 | 0.0000 | 1.0005 | 1.0003 | 1.0007 | 0.00000 | |||
| Hyponatremia | 1.35 | 0.90 | 2.02 | 0.3598 | 1.0061 | 0.9664 | 1.0474 | 0.76825 | |||
| Hypernatremia | 2.79 | 1.59 | 4.91 | 0.0026 | 1.0020 | 0.9313 | 1.0782 | 0.95654 | |||
| Characteristic | Hyponatremia | Hypernatremia | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | CI 95 Upper | CI 95 Lower | p | OR | CI 95 Upper | CI 95 Lower | p | |
| Age | 1.02 | 1.01 | 1.03 | 0.0000 | 1.04 | 1.02 | 1.05 | 0.0000 |
| Sex (female) | 0.86 | 0.66 | 1.14 | 0.2978 | 0.90 | 0.56 | 1.44 | 0.6510 |
| HR | 1.01 | 1.00 | 1.02 | 0.0182 | 1.01 | 1.00 | 1.03 | 0.0894 |
| SBP | 1.00 | 0.99 | 1.01 | 0.8926 | 0.98 | 0.97 | 0.99 | 0.0018 |
| DBP | 1.00 | 0.99 | 1.01 | 0.5917 | 0.98 | 0.96 | 1.00 | 0.0294 |
| Consciousness | 1.49 | 1.05 | 2.10 | 0.0248 | 11.20 | 6.72 | 18.66 | 0.0000 |
| Comorbidities | ||||||||
| Hypertension | 1.40 | 1.06 | 1.85 | 0.0170 | 1.24 | 0.77 | 1.99 | 0.3854 |
| MI | 1.76 | 1.19 | 2.59 | 0.0043 | 1.13 | 0.53 | 2.43 | 0.7452 |
| Stroke/TIA | 1.08 | 0.67 | 1.74 | 0.7530 | 1.94 | 0.99 | 3.81 | 0.0542 |
| DM | 1.71 | 1.28 | 2.30 | 0.0003 | 1.01 | 0.58 | 1.77 | 0.9712 |
| CKD | 1.30 | 0.89 | 1.90 | 0.1714 | 0.61 | 0.26 | 1.43 | 0.2574 |
| Heart failure | 1.57 | 1.11 | 2.23 | 0.0115 | 1.37 | 0.73 | 2.55 | 0.3237 |
| Asthma/COBP | 0.88 | 0.53 | 1.46 | 0.6150 | 1.74 | 0.86 | 3.49 | 0.1222 |
| POAD | 1.63 | 0.96 | 2.77 | 0.0701 | 1.42 | 0.55 | 3.65 | 0.4721 |
| CVD | 1.58 | 1.18 | 2.12 | 0.0022 | 1.73 | 1.05 | 2.84 | 0.0313 |
| Neoplastic disorder | 1.32 | 0.87 | 2.00 | 0.1982 | 1.30 | 0.63 | 2.68 | 0.4831 |
| Laboratory findings | ||||||||
| WBC | 1.00 | 0.99 | 1.01 | 0.7957 | 1.01 | 1.00 | 1.02 | 0.0613 |
| Hb | 0.99 | 0.94 | 1.05 | 0.7718 | 1.01 | 0.91 | 1.12 | 0.9051 |
| PLT | 1.00 | 1.00 | 1.00 | 0.9114 | 1.00 | 1.00 | 1.00 | 0.2087 |
| Creatinine | 1.12 | 1.02 | 1.23 | 0.0141 | 1.12 | 0.97 | 1.29 | 0.1215 |
| CRP | 1.00 | 1.00 | 1.00 | 0.0003 | 1.01 | 1.00 | 1.01 | 0.0000 |
| Long-term use of drugs | ||||||||
| ACEI/ARB/ARNI | 1.64 | 1.23 | 2.18 | 0.0007 | 1.26 | 0.75 | 2.09 | 0.3821 |
| Beta-blockers | 1.41 | 1.06 | 1.87 | 0.0185 | 1.05 | 0.62 | 1.75 | 0.8629 |
| Ca blockers | 1.16 | 0.82 | 1.65 | 0.4078 | 1.34 | 0.74 | 2.41 | 0.3362 |
| MRAs | 1.27 | 0.76 | 2.13 | 0.3657 | 0.42 | 0.10 | 1.75 | 0.2353 |
| Diuretics | 1.40 | 1.01 | 1.94 | 0.0453 | 0.92 | 0.49 | 1.74 | 0.7943 |
| Statins | 1.06 | 0.76 | 1.47 | 0.7382 | 1.17 | 0.67 | 2.06 | 0.5757 |
| ASA | 1.13 | 0.78 | 1.63 | 0.5209 | 1.02 | 0.53 | 1.98 | 0.9529 |
| Anticoagulants | 1.38 | 0.98 | 1.94 | 0.0677 | 1.77 | 1.01 | 3.08 | 0.0442 |
| Steroids/immunosuppressants | 0.99 | 0.57 | 1.71 | 0.9717 | 0.39 | 0.09 | 1.63 | 0.1977 |
| Characteristics | Coefficient | SE | CI-Min | CI-Max | p | OR | CI95 Lower | CI95 Upper | p |
|---|---|---|---|---|---|---|---|---|---|
| Predictors of hyponatremia | |||||||||
| Age | 0.02 | 0.00 | 0.01 | 0.03 | 0.0017 | 1.02 | 1.01 | 1.03 | 0.0017 |
| HR | 0.01 | 0.00 | 0.00 | 0.02 | 0.0177 | 1.01 | 1.00 | 1.02 | 0.0177 |
| Consciousness | 0.17 | 0.19 | −0.19 | 0.54 | 0.3538 | 1.19 | 0.82 | 1.72 | 0.3538 |
| Hypertension | −0.27 | 0.19 | −0.64 | 0.09 | 0.1458 | 0.76 | 0.53 | 1.10 | 0.1458 |
| DM | 0.34 | 0.16 | 0.02 | 0.66 | 0.0376 | 1.40 | 1.02 | 1.93 | 0.0376 |
| ACEI/ARB/ARNI | 0.42 | 0.18 | 0.08 | 0.76 | 0.0170 | 1.52 | 1.08 | 2.15 | 0.0170 |
| Beta-blockers | 0.01 | 0.17 | −0.33 | 0.36 | 0.9400 | 1.01 | 0.72 | 1.43 | 0.9400 |
| Diuretics | −0.04 | 0.19 | −0.42 | 0.34 | 0.8228 | 0.96 | 0.66 | 1.40 | 0.8228 |
| CRP | 0.00 | 0.00 | 0.00 | 0.00 | 0.0045 | 1.00 | 1.00 | 1.00 | 0.0045 |
| Creatinine | 0.08 | 0.05 | −0.02 | 0.18 | 0.0987 | 1.09 | 0.98 | 1.20 | 0.0987 |
| CVD | 0.12 | 0.17 | −0.22 | 0.46 | 0.4904 | 1.13 | 0.80 | 1.58 | 0.4904 |
| Predictors of hypernatremia | |||||||||
| Age | 0.02 | 0.01 | 0.00 | 0.03 | 0.051 | 1.02 | 1.00 | 1.03 | 0.0510 |
| SBP | −0.02 | 0.01 | −0.04 | 0.00 | 0.026 | 0.98 | 0.96 | 1.00 | 0.0263 |
| DBP | 0.02 | 0.01 | 0.00 | 0.05 | 0.090 | 1.02 | 1.00 | 1.05 | 0.0896 |
| Consciousness | 2.14 | 0.29 | 1.58 | 2.71 | 0.000 | 8.54 | 4.83 | 15.09 | 0.0000 |
| Anticoagulants | 0.44 | 0.32 | −0.18 | 1.06 | 0.163 | 1.55 | 0.84 | 2.89 | 0.1629 |
| CRP | 0.00 | 0.00 | 0.00 | 0.01 | 0.028 | 1.00 | 1.00 | 1.01 | 0.0277 |
| CVD | −0.10 | 0.29 | −0.67 | 0.47 | 0.728 | 0.90 | 0.51 | 1.60 | 0.7279 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Królicka, A.; Letachowicz, K.; Adamik, B.; Doroszko, A.; Kaliszewski, K.; Kiliś-Pstrusińska, K.; Kujawa, K.; Matera-Witkiewicz, A.; Madziarski, M.; Pomorski, M.; et al. Dysnatremia in COVID-19 Patients—An Analysis of the COLOS Study. J. Clin. Med. 2023, 12, 2802. https://doi.org/10.3390/jcm12082802
Królicka A, Letachowicz K, Adamik B, Doroszko A, Kaliszewski K, Kiliś-Pstrusińska K, Kujawa K, Matera-Witkiewicz A, Madziarski M, Pomorski M, et al. Dysnatremia in COVID-19 Patients—An Analysis of the COLOS Study. Journal of Clinical Medicine. 2023; 12(8):2802. https://doi.org/10.3390/jcm12082802
Chicago/Turabian StyleKrólicka, Anna, Krzysztof Letachowicz, Barbara Adamik, Adrian Doroszko, Krzysztof Kaliszewski, Katarzyna Kiliś-Pstrusińska, Krzysztof Kujawa, Agnieszka Matera-Witkiewicz, Marcin Madziarski, Michał Pomorski, and et al. 2023. "Dysnatremia in COVID-19 Patients—An Analysis of the COLOS Study" Journal of Clinical Medicine 12, no. 8: 2802. https://doi.org/10.3390/jcm12082802
APA StyleKrólicka, A., Letachowicz, K., Adamik, B., Doroszko, A., Kaliszewski, K., Kiliś-Pstrusińska, K., Kujawa, K., Matera-Witkiewicz, A., Madziarski, M., Pomorski, M., Protasiewicz, M., Sokołowski, J., Trocha, M., Jankowska, E. A., & Madziarska, K. (2023). Dysnatremia in COVID-19 Patients—An Analysis of the COLOS Study. Journal of Clinical Medicine, 12(8), 2802. https://doi.org/10.3390/jcm12082802