
A Rare Case of Hepatocellular Carcinoma Recurrence in Ovarian Site after 12 Years Mimicking a Hepatoid Adenocarcinoma: Case Report

 ,
, 
 ,
,  , , ,
, , , 
Abstract
1. Introduction
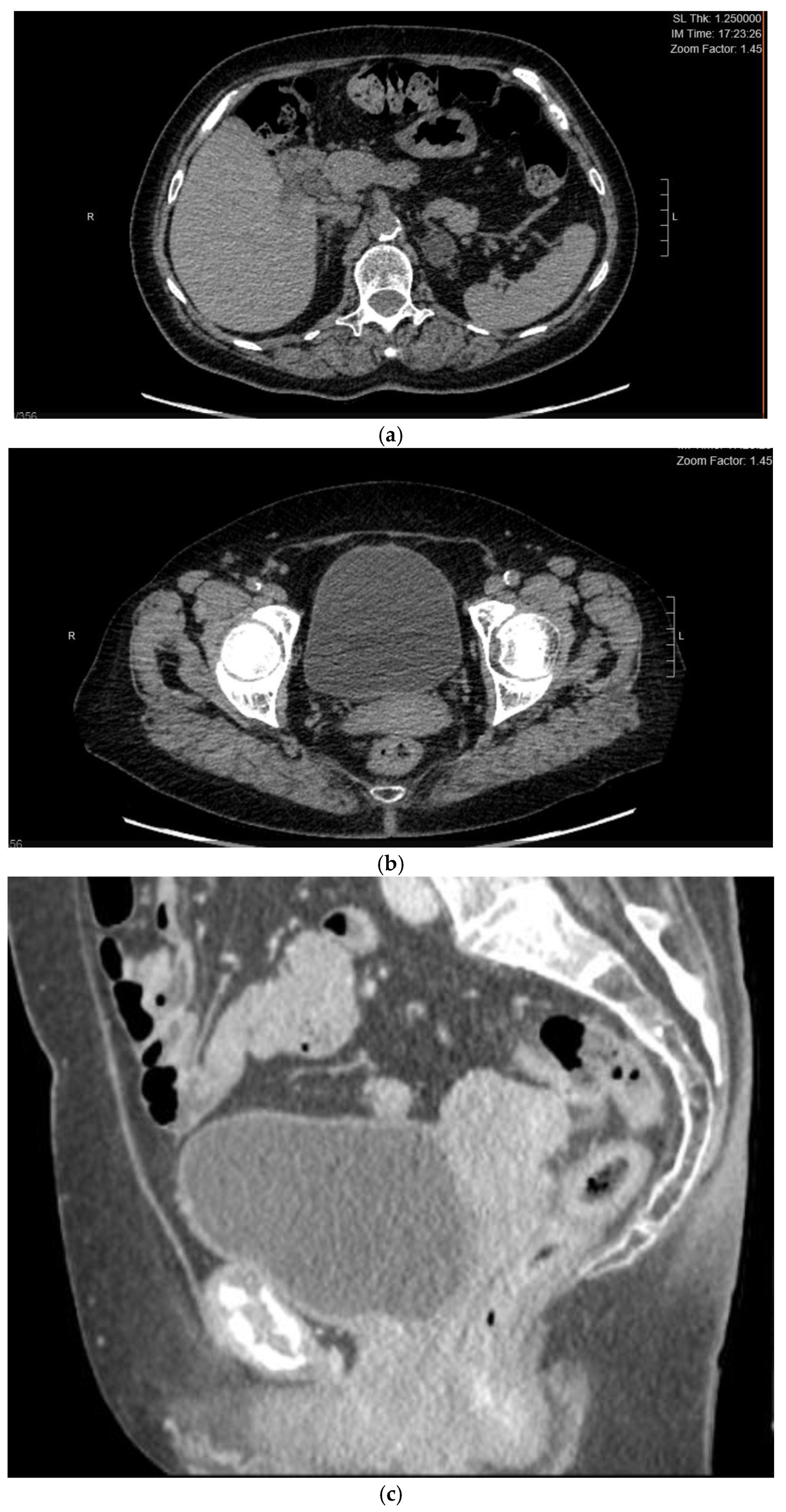
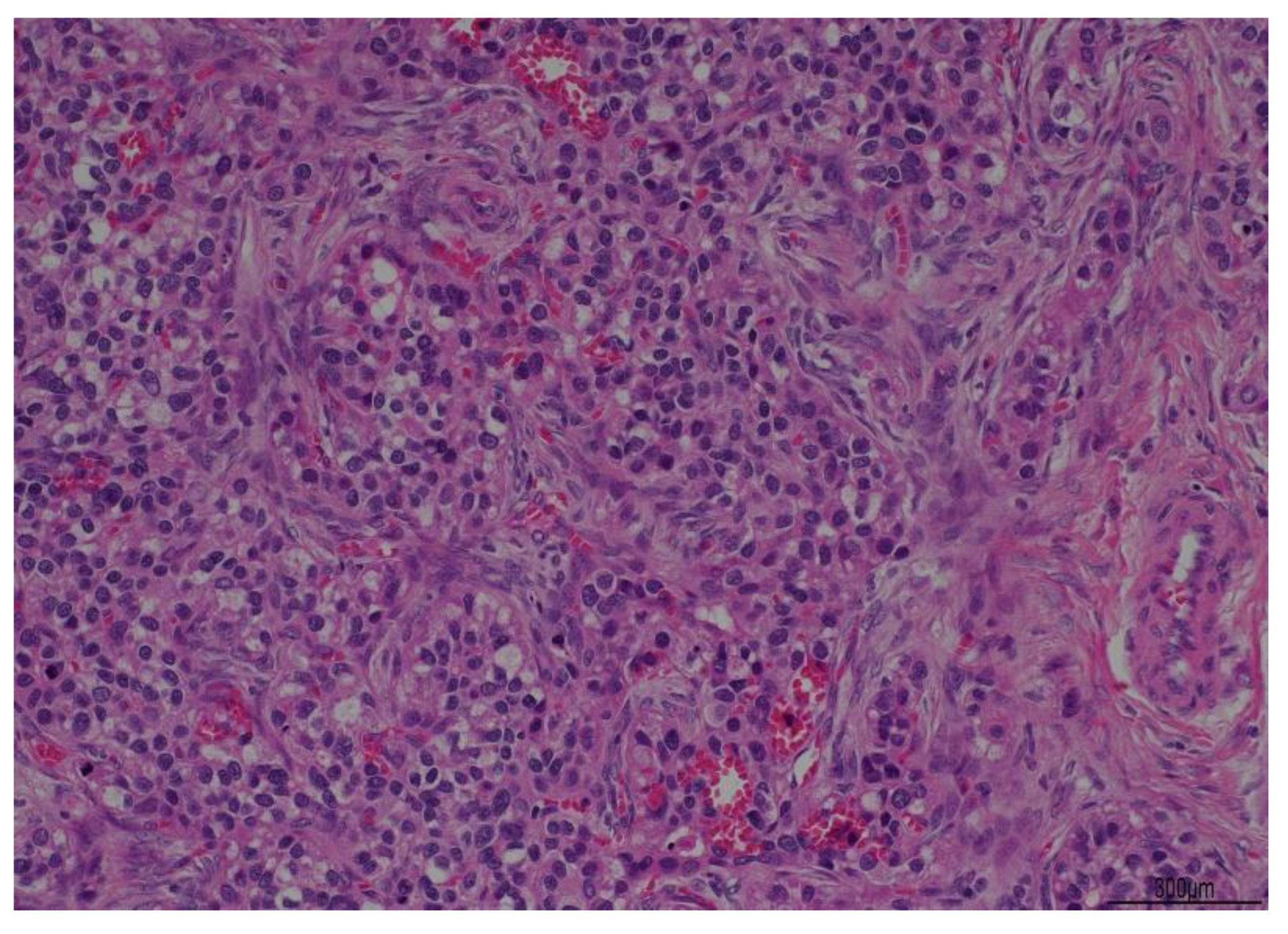
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ishikura, H.; Scully, R.E. Hepatoid carcinoma of the ovary. A newly described tumor. Cancer 1987, 60, 2775–2784. [Google Scholar] [CrossRef] [PubMed]
- Su, J.S.; Chen, Y.T.; Wang, R.C.; Wu, C.Y.; Lee, S.W.; Lee, T.Y. Clinicopathological characteristics in the differential diagnosis of hepatoid adenocarcinoma: A literature review. World J. Gastroenterol. 2013, 19, 321–327. [Google Scholar] [CrossRef]
- Lázaro, J.; Rubio, D.; Repolles, M.; Capote, L. Hepatoid carcinoma of the ovary and management. Acta Obstet. Gynecol. Scand. 2007, 86, 498–499. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.K.; Cho, D.H.; Yim, C.Y.; Lee, N.R. Primary hepatoid carcinoma of the ovary: A case report and review of the literature. Medicine 2020, 99, e20051. [Google Scholar] [CrossRef] [PubMed]
- Lefkowitch, J.H. Liver look-alike: Hepatoid ovarian carcinoma. Hepatology 1988, 8, 1168–1169. [Google Scholar] [CrossRef] [PubMed]
- Matsuta, M.; Ishikura, H.; Murakami, K.; Kagabu, T.; Nishiya, I. Hepatoid carcinoma of the ovary: A case report. Int. J. Gynecol. Pathol. 1991, 10, 302–310. [Google Scholar] [CrossRef]
- Pandey, M.; Truica, C. Hepatoid Carcinoma of the Ovary. J. Clin. Oncol. 2011, 29, e446–e448. [Google Scholar] [CrossRef]
- Acosta, A.M.; Pins, M.R. Hepatoid Carcinoma of the Ovary: Clinical, Histopathologic, and Immunophenotypic Features. Arch. Pathol. Lab. Med. 2019, 143, 883–889. [Google Scholar] [CrossRef]
- Sun, J.; Tang, G.; Dong, G. Hepatoid Carcinoma of the Ovary: A Case Report; 2009; Volume 43, pp. 324–325. [Google Scholar]
- Wong, T.C.; To, K.F.; Hou, S.S.; Yip, S.K.; Ng, C.F. Late retroperitoneal recurrence of hepatocellular carcinoma 12 years after initial diagnosis. World J. Gastroenterol. 2010, 16, 2187–2189. [Google Scholar] [CrossRef]
- Kanda, M.; Tateishi, R.; Yoshida, H.; Sato, T.; Masuzaki, R.; Ohki, T.; Imamura, J.; Goto, T.; Yoshida, H.; Hamamura, K.; et al. Extrahepatic metastasis of hepatocellular carcinoma: Incidence and risk factors. Liver Int. 2008, 28, 1256–1263. [Google Scholar] [CrossRef]
- Liu, X.-L.; Wang, X.; Zhu, F.-F. Hepatoid carcinoma of the ovary: A case report and review of the literature. Oncol. Lett. 2012, 4, 947–950. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Compilato, D.; Genco, C.; Campisi, G. Extrahepatic spread of hepatocellular carcinoma. Panminerva Med. 2012, 54, 313–322. [Google Scholar] [PubMed]
- Motegi, S.; Yokoo, T.; Nozawa, R.; Azumi, R.; Kawata, Y.; Ogawa, K.; Setsu, T.; Mizuno, K.-I.; Nishino, K.; Umezu, H.; et al. Long-term survival of 11 years with multidisciplinary therapy for hepatocellular carcinoma metastasis to the ovary and peritoneum: A case report. Clin. J. Gastroenterol. 2021, 14, 1211–1220. [Google Scholar] [CrossRef]
- Uchino, K.; Tateishi, R.; Shiina, S.; Kanda, M.; Masuzaki, R.; Kondo, Y.; Goto, T.; Omata, M.; Yoshida, H.; Koike, K. Hepatocellular carcinoma with extrahepatic metastasis: Clinical features and prognostic factors. Cancer 2011, 117, 4475–4483. [Google Scholar] [CrossRef]
- Young, R.H.; Gersell, D.J.; Clement, P.B.; Scully, R.E. Hepatocellular carcinoma metastatic to the ovary: A report of three cases discovered during life with discussion of the differential diagnosis of hepatoid tumors of the ovary. Hum. Pathol. 1992, 23, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Braccischi, L.; D’Errico, A.; Pecorelli, A.; Brandi, N.; Golfieri, R.; Albertini, E.; Vasuri, F. State-of-the-art review on the correlations between pathological and magnetic resonance features of cirrhotic nodules. Histol. Histopathol. 2022, 37, 1151–1165. [Google Scholar]
- Nguyen, P.; Hui, S.; Robertson, M. Hepatoid adenocarcinoma: A wolf in hepatocellular carcinoma’s clothing. JGH Open. 2022, 6, 727–729. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M. American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- El Jabbour, T.; Lagana, S.M.; Lee, H. Update on hepatocellular carcinoma: Pathologists’ review. World J. Gastroenterol. 2019, 25, 1653–1665. [Google Scholar] [CrossRef]
- Durnez, A.; Verslype, C.; Nevens, F.; Fevery, J.; Aerts, R.; Pirenne, J.; Lesaffre, E.; Libbrecht, L.; Desmet, V.; Roskams, T. The clinicopathological and prognostic relevance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology 2006, 49, 138–151. [Google Scholar] [CrossRef]
- Karabork, A.; Kaygusuz, G.; Ekinci, C. The best immunohistochemical panel for differentiating hepatocellular carcinoma from metastatic adenocarcinoma. Pathol.-Res. Pr. 2010, 206, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.E.; Kim, S.H.; Cho, N.H. No ancillary finding is valid to distinguish a primary ovarian hepatoid carcinoma from metastatic hepatocellular carcinoma. Int. J. Gynecol. Cancer 2006, 16, 1691–1694. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Site of primary tumor | Ovary (only 1 case of HAC cited in Sheng Su et al. review) |
| Remote pathological history | HCC in 2009 treated surgically |
| Tumor markers | AFP > 200 ng/mL |
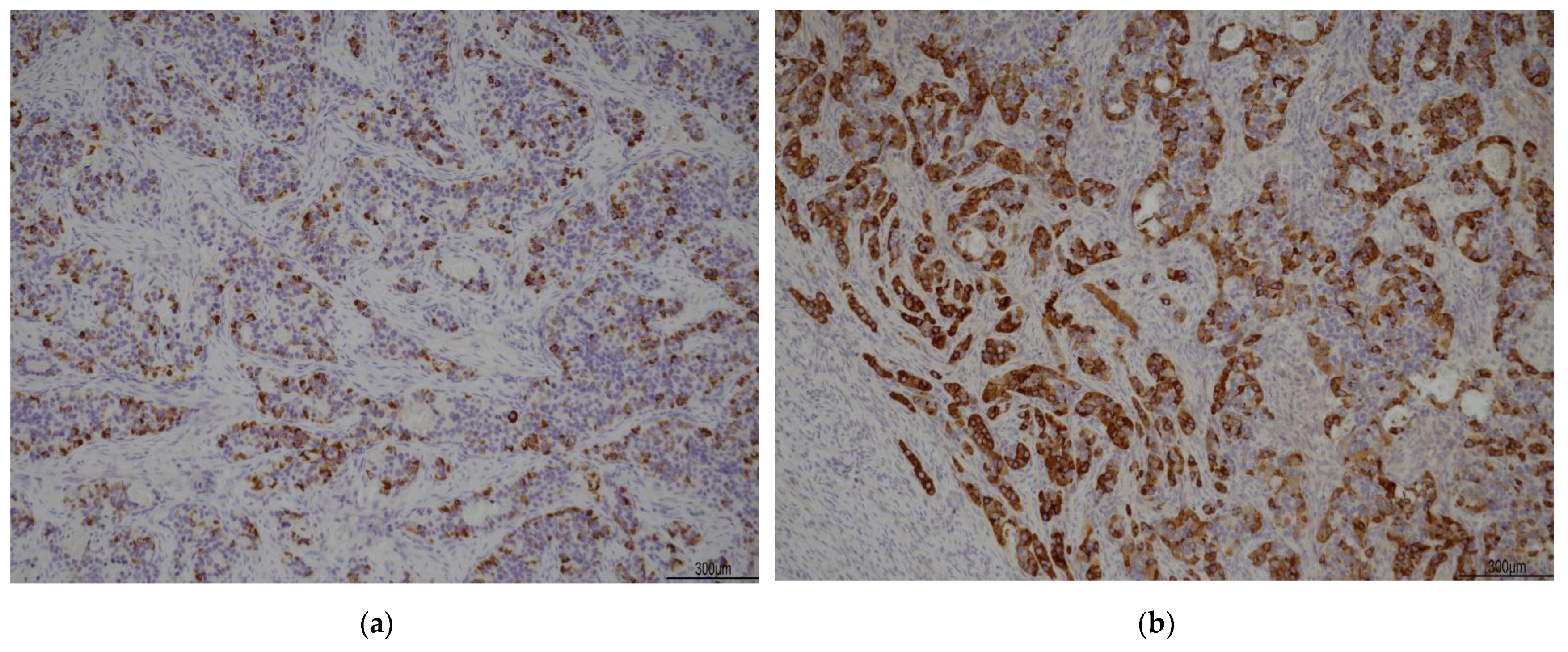
| IHC | - Cytokeratin 7: positive |
| - PAX8: negative | |
| - Hepatocyte: focally positive cells | |
| - Glypican 3: positive | |
| - Arginase: focally positive | |
| - WT1: negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restaino, S.; Pellecchia, G.; Poli, A.; Arcieri, M.; Andreetta, C.; Mariuzzi, L.; Orsaria, M.; Biasioli, A.; Della Martina, M.; Intini, S.G.; et al. A Rare Case of Hepatocellular Carcinoma Recurrence in Ovarian Site after 12 Years Mimicking a Hepatoid Adenocarcinoma: Case Report. J. Clin. Med. 2023, 12, 2468. https://doi.org/10.3390/jcm12072468
Restaino S, Pellecchia G, Poli A, Arcieri M, Andreetta C, Mariuzzi L, Orsaria M, Biasioli A, Della Martina M, Intini SG, et al. A Rare Case of Hepatocellular Carcinoma Recurrence in Ovarian Site after 12 Years Mimicking a Hepatoid Adenocarcinoma: Case Report. Journal of Clinical Medicine. 2023; 12(7):2468. https://doi.org/10.3390/jcm12072468
Chicago/Turabian StyleRestaino, Stefano, Giulia Pellecchia, Alice Poli, Martina Arcieri, Claudia Andreetta, Laura Mariuzzi, Maria Orsaria, Anna Biasioli, Monica Della Martina, Sergio Giuseppe Intini, and et al. 2023. "A Rare Case of Hepatocellular Carcinoma Recurrence in Ovarian Site after 12 Years Mimicking a Hepatoid Adenocarcinoma: Case Report" Journal of Clinical Medicine 12, no. 7: 2468. https://doi.org/10.3390/jcm12072468
APA StyleRestaino, S., Pellecchia, G., Poli, A., Arcieri, M., Andreetta, C., Mariuzzi, L., Orsaria, M., Biasioli, A., Della Martina, M., Intini, S. G., Scambia, G., Driul, L., & Vizzielli, G. (2023). A Rare Case of Hepatocellular Carcinoma Recurrence in Ovarian Site after 12 Years Mimicking a Hepatoid Adenocarcinoma: Case Report. Journal of Clinical Medicine, 12(7), 2468. https://doi.org/10.3390/jcm12072468