
Reintervention of Residual Aortic Dissection after Type A Aortic Repair: Results of a Prospective Follow-Up at 5 Years

 ,
,
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Endpoints
2.3. Follow-Up
2.4. CT Protocol
2.5. Surgical Procedures
2.5.1. Initial Surgery for TAAD
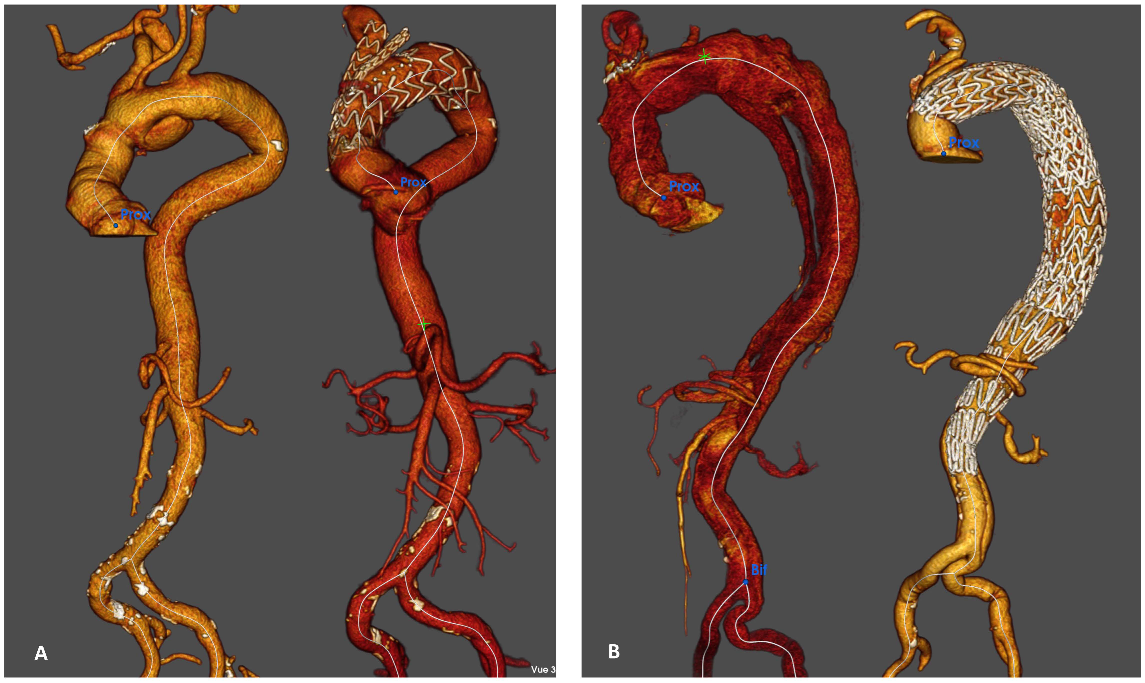
2.5.2. Distal Reintervention on the Descending Thoracic aorta
2.6. Management of the Aortic Arch
2.6.1. Hybrid Repair
2.6.2. Branched Aortic Arch Endoprosthesis
2.6.3. TEVAR
2.7. Statistical Analysis
3. Results
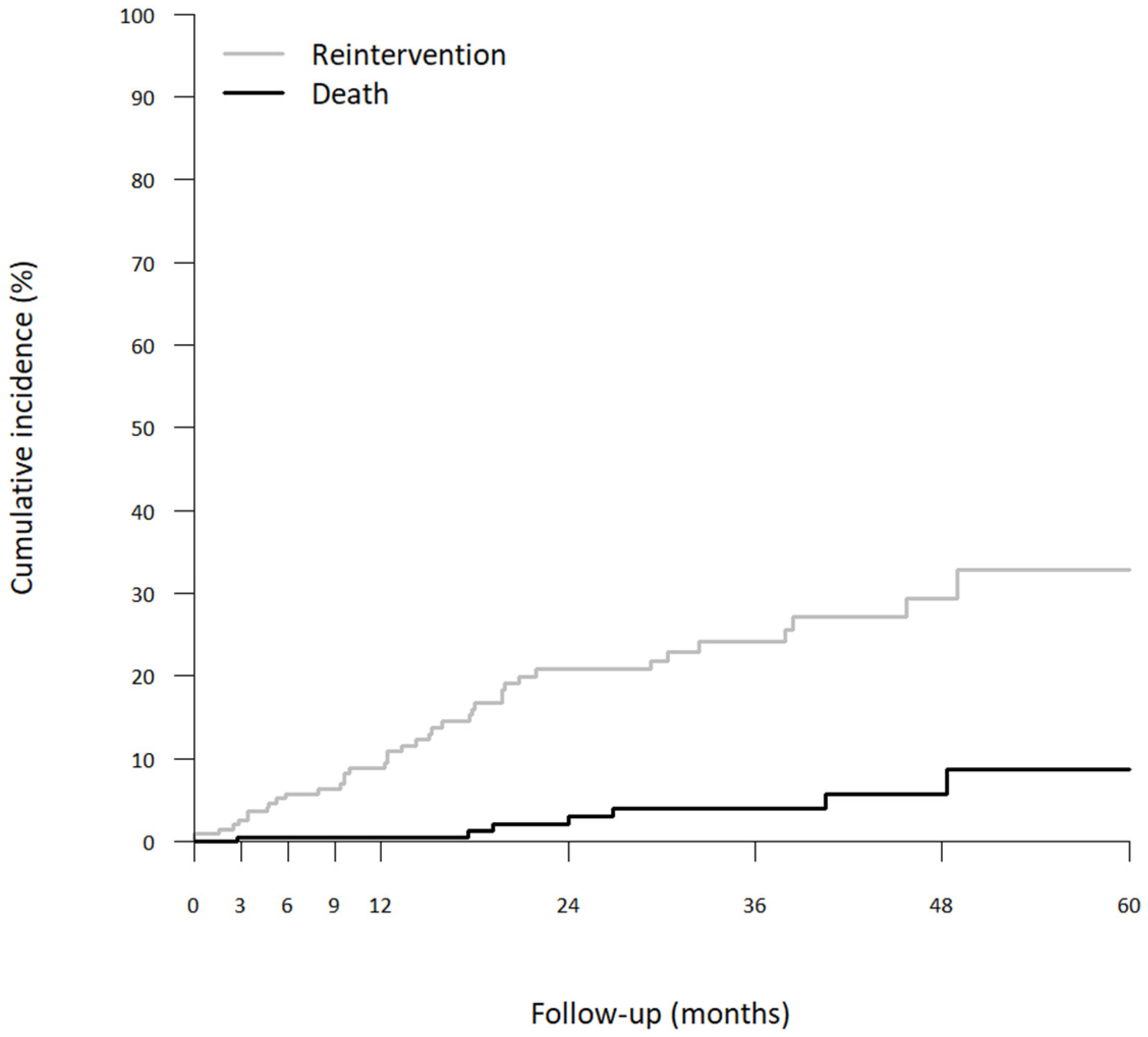
3.1. All-Cause Mortality of RAD
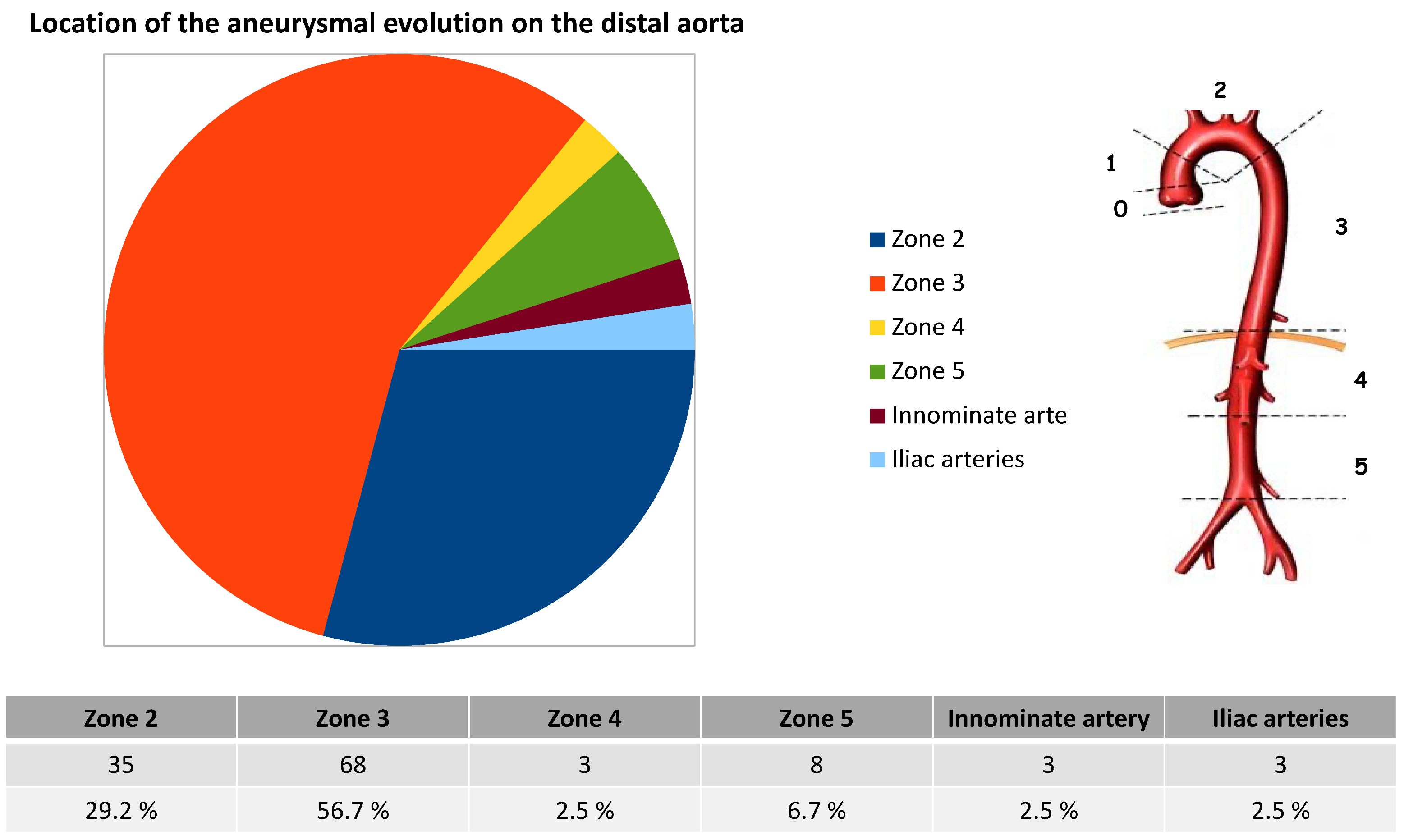
3.2. Distal Aneurysm Evolution
3.3. Distal Reintervention
3.4. Indications
3.5. Perioperative Results of Distal Reintervention
3.5.1. Results after Hybrid Repair
3.5.2. Results after Branched Aortic Arch Endoprosthesis
3.5.3. Results for Other Reinterventions
3.6. Risk Factors for Reinterventions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CA | Circulatory Arrest |
| CAD | Coronary Artery Disease |
| CPB | Cardiopulmonary Bypass |
| COPD | Chronic Obstructive Pulmonary Disease |
| CT | Computed Tomography |
| IA | Innominate Artery |
| FL | False Lumen |
| LCCA | Left Common Carotid Artery |
| LSA | Left Subclavian Artery |
| RAD | Residual Aortic Dissection |
| TEVAR | Total Endo Vascular Aortic Repair |
References
- Gouveia, E.M.R.; Mourao, M.; Caldeira, D.; Alves, M.; Lopes, A.; Duarte, A.; Fernandes, E.F.R.; Mendes Pedro, L. A systematic review and meta-analysis of the incidence of acute aortic dissections in population-based studies. J. Vasc. Surg. 2022, 75, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, A.; Isselbacher, E.M.; Bossone, E.; Gleason, T.G.; Eusanio, M.D.; Sechtem, U.; Ehrlich, M.P.; Trimarchi, S.; Braverman, A.C.; Myrmel, T.; et al. Insights From the International Registry of Acute Aortic Dissection: A 20-Year Experience of Collaborative Clinical Research. Circulation 2018, 137, 1846–1860. [Google Scholar] [CrossRef] [PubMed]
- Berretta, P.; Patel, H.J.; Gleason, T.G.; Sundt, T.M.; Myrmel, T.; Desai, N.; Korach, A.; Panza, A.; Bavaria, J.; Khoynezhad, A.; et al. IRAD experience on surgical type A acute dissection patients: Results and predictors of mortality. Ann. Cardiothorac. Surg. 2016, 5, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Chabry, Y.; Porterie, J.; Gautier, C.H.; Nader, J.; Chaufour, X.; Alsac, J.M.; Reix, T.; Marcheix, B.; Koskas, F.; Ruggieri, V.G.; et al. The frozen elephant trunk technique in an emergency: THORAFLEX French National Registry offers new insights. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2020, 3, ezaa325. [Google Scholar] [CrossRef]
- Isselbacher, E.M.; Preventza, O.; Black, J.H., 3rd; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 80, e223–e393. [Google Scholar] [CrossRef]
- Kimura, N.; Itoh, S.; Yuri, K.; Adachi, K.; Matsumoto, H.; Yamaguchi, A.; Adachi, H. Reoperation for enlargement of the distal aorta after initial surgery for acute type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2015, 149, S91–S98. [Google Scholar] [CrossRef]
- Yeh, C.H.; Chen, M.C.; Wu, Y.C.; Wang, Y.C.; Chu, J.J.; Lin, P.J. Risk factors for descending aortic aneurysm formation in medium-term follow-up of patients with type A aortic dissection. Chest 2003, 124, 989–995. [Google Scholar] [CrossRef]
- Inoue, Y.; Matsuda, H.; Omura, A.; Seike, Y.; Uehara, K.; Sasaki, H.; Kobayashi, J. Long-term outcomes of total arch replacement with the non-frozen elephant trunk technique for Stanford Type A acute aortic dissection. Interact. Cardiovasc. Thorac. Surg. 2018, 27, 455–460. [Google Scholar] [CrossRef]
- Suzuki, T.; Asai, T.; Kinoshita, T. Predictors for Late Reoperation After Surgical Repair of Acute Type A Aortic Dissection. Ann. Thorac. Surg. 2018, 106, 63–69. [Google Scholar] [CrossRef]
- Tamura, K.; Chikazawa, G.; Hiraoka, A.; Totsugawa, T.; Sakaguchi, T.; Yoshitaka, H. The prognostic impact of distal anastomotic new entry after acute type I aortic dissection repair. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2017, 52, 867–873. [Google Scholar] [CrossRef]
- Lederle, F.A.; Johnson, G.R.; Wilson, S.E.; Littooy, F.N.; Krupski, W.C.; Bandyk, D.; Acher, C.W.; Chute, E.P.; Hye, R.J.; Gordon, I.L.; et al. Yield of repeated screening for abdominal aortic aneurysm after a 4-year interval. Aneurysm Detection and Management Veterans Affairs Cooperative Study Investigators. Arch. Intern. Med. 2000, 160, 1117–1121. [Google Scholar] [CrossRef]
- Conzelmann, L.O.; Hoffmann, I.; Blettner, M.; Kallenbach, K.; Karck, M.; Dapunt, O.; Borger, M.A.; Weigang, E.; Investigators, G. Analysis of risk factors for neurological dysfunction in patients with acute aortic dissection type A: Data from the German Registry for Acute Aortic Dissection type A (GERAADA). Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2012, 42, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Tasoudis, P.T.; Magouliotis, D.E.; Varvoglis, D.N.; Ziogas, I.A.; Salmasi, M.Y.; Spanos, K.; Kourliouros, A.; Matsagkas, M.; Giannoukas, A.; Athanasiou, T. Proximal versus extensive repair in acute type A aortic dissection: An updated systematic review and meta-analysis. Gen. Thorac. Cardiovasc. Surg. 2022, 70, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Berger, T.; Kreibich, M.; Mueller, F.; Rylski, B.; Kondov, S.; Schrofel, H.; Pingpoh, C.; Beyersdorf, F.; Siepe, M.; Czerny, M. The frozen elephant trunk technique for aortic dissection is safe after previous aortic repair. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2021, 59, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Demal, T.J.; Bax, L.; Brickwedel, J.; Kolbel, T.; Vettorazzi, E.; Sitzmann, F.; Reichenspurner, H.; Detter, C. Outcome of the frozen elephant trunk procedure as a redo operation. Interact. CardioVascular Thorac. Surg. 2021, 33, 85–92. [Google Scholar] [CrossRef]
- Gaudry, M.; Porto, A.; Blanchard, A.; Chazot, J.V.; Bal, L.; De Masi, M.; Bartoli, A.; Barral, P.A.; Jacquier, A.; Gariboldi, V.; et al. A 10-Year Aortic Center Experience with Hybrid Repair of Chronic “Residual” Aortic Dissection After Type A Repair. Cardiovasc. Drugs Ther. 2022, 36, 285–294. [Google Scholar] [CrossRef]
- Verscheure, D.; Haulon, S.; Tsilimparis, N.; Resch, T.; Wanhainen, A.; Mani, K.; Dias, N.; Sobocinski, J.; Eagleton, M.; Ferreira, M.; et al. Endovascular Treatment of Post Type A Chronic Aortic Arch Dissection With a Branched Endograft: Early Results From a Retrospective International Multicenter Study. Ann. Surg. 2019, 273, 997–1003. [Google Scholar] [CrossRef]
- Nana, P.; Spanos, K.; Dakis, K.; Giannoukas, A.; Kölbel, T.; Haulon, S. Systematic Review on Customized and Non-customized Device Techniques for the Endovascular Repair of the Aortic Arch. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2022, 15266028221133701. [Google Scholar] [CrossRef]
- Kimura, N.; Tanaka, M.; Kawahito, K.; Yamaguchi, A.; Ino, T.; Adachi, H. Influence of patent false lumen on long-term outcome after surgery for acute type A aortic dissection. J. Thorac. Cardiovasc. Surg. 2008, 136, 1160–1166. [Google Scholar] [CrossRef]
- Gaudry, M.; Guivier-Curien, C.; Blanchard, A.; Porto, A.; Bal, L.; Omnes, V.; De Masi, M.; Lu, C.; Jacquier, A.; Piquet, P.; et al. Volume Analysis to Predict the Long-Term Evolution of Residual Aortic Dissection after Type A Repair. J. Cardiovasc. Dev. Dis. 2022, 9, 349. [Google Scholar] [CrossRef]
- Gaudry, M.; Porto, A.; Guivier-Curien, C.; Blanchard, A.; Bal, L.; Resseguier, N.; Omnes, V.; De Masi, M.; Ejargue, M.; Jacquier, A.; et al. Results of a prospective follow-up study after type A aortic dissection repair: A high rate of distal aneurysmal evolution and reinterventions. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2022, 61, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Faure, E.M.; El Batti, S.; Abou Rjeili, M.; Julia, P.; Alsac, J.M. Mid-term Outcomes of Stent Assisted Balloon Induced Intimal Disruption and Relamination in Aortic Dissection Repair (STABILISE) in Acute Type B Aortic Dissection. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Faure, E.M.; El Batti, S.; Sutter, W.; Bel, A.; Julia, P.; Achouh, P.; Alsac, J.M. Stent-assisted balloon-induced intimal disruption and relamination of distal remaining aortic dissection after acute DeBakey type I repair. J. Thorac. Cardiovasc. Surg. 2019, 157, 2159–2165. [Google Scholar] [CrossRef]
- Vecchini, E.; Gulmini, M.; Peluso, A.; Fasoli, G.; Anselmi, A.; Maluta, T.; De Cristan, D.; Magnan, B.; Ricci, M. The treatment of irreparable massive rotator cuff tears with inspace balloon: Rational and medium-term results. Acta Bio Med. Atenei Parm. 2022, 92, e2021584. [Google Scholar] [CrossRef]
- Rohlffs, F.; Tsilimparis, N.; Panuccio, G.; Heidemann, F.; Behrendt, C.A.; Kölbel, T. The Knickerbocker Technique: Technical Aspects and Single-Center Results of a New Endovascular Method for False Lumen Occlusion in Chronic Aortic Dissection. J. Endovasc. Ther. Off. J. Int. Soc. Endovasc. Spec. 2022, 15266028221090439. [Google Scholar] [CrossRef]
- Fann, J.I.; Smith, J.A.; Miller, D.C.; Mitchell, R.S.; Moore, K.A.; Grunkemeier, G.; Stinson, E.B.; Oyer, P.E.; Reitz, B.A.; Shumway, N.E. Surgical management of aortic dissection during a 30-year period. Circulation 1995, 92, II113-121. [Google Scholar] [CrossRef] [PubMed]
- Ohira, S.; Malekan, R.; Kai, M.; Goldberg, J.B.; Laskowski, I.; De La Pena, C.; Mason, I.; Lansman, S.L.; Spielvogel, D. Aortic Reoperation After Prior Acute Type A Aortic Dissection Repair: Don’t Despair the Repair. Ann. Thorac. Surg. 2022. [Google Scholar] [CrossRef]
- Sultan, I.; Wallen, T.J.; Habertheuer, A.; Siki, M.; Arnaoutakis, G.J.; Bavaria, J.; Szeto, W.Y.; Milewski, R.; Vallabhajosyula, P. Concomitant antegrade stent grafting of the descending thoracic aorta during transverse hemiarch reconstruction for acute DeBakey I aortic dissection repair improves aortic remodeling. J. Card. Surg. 2017, 32, 581–592. [Google Scholar] [CrossRef]
- Quintana, E.; Bajona, P.; Schaff, H.V.; Dearani, J.A.; Daly, R.C.; Greason, K.L.; Pochettino, A. Open aortic arch reconstruction after previous cardiac surgery: Outcomes of 168 consecutive operations. J. Thorac. Cardiovasc. Surg. 2014, 148, 2944–2950. [Google Scholar] [CrossRef]
- Malvindi, P.G.; van Putte, B.P.; Sonker, U.; Heijmen, R.H.; Schepens, M.A.; Morshuis, W.J. Reoperation after acute type a aortic dissection repair: A series of 104 patients. Ann. Thorac. Surg. 2013, 95, 922–927. [Google Scholar] [CrossRef]
- Di Bartolomeo, R.; Berretta, P.; Pantaleo, A.; Murana, G.; Cefarelli, M.; Alfonsi, J.; Barberio, G.; Leone, A.; Di Marco, L.; Pacini, D. Long-Term Outcomes of Open Arch Repair After a Prior Aortic Operation: Our Experience in 154 Patients. Ann. Thorac. Surg. 2017, 103, 1406–1412. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, A.M.; Pollari, F.; Fattouch, K.; Santarpino, G.; Hillebrand, J.; Schneider, S.; Landwerht, J.; Nasso, G.; Gregorini, R.; Del Giglio, M.; et al. Early outcomes in re-do operation after acute type A aortic dissection: Results from the multicenter REAAD database. Heart Vessel. 2017, 32, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Haulon, S.; Greenberg, R.K.; Spear, R.; Eagleton, M.; Abraham, C.; Lioupis, C.; Verhoeven, E.; Ivancev, K.; Kolbel, T.; Stanley, B.; et al. Global experience with an inner branched arch endograft. J. Thorac. Cardiovasc. Surg. 2014, 148, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Maurel, B.; Mastracci, T.M.; Spear, R.; Hertault, A.; Azzaoui, R.; Sobocinski, J.; Haulon, S. Branched and fenestrated options to treat aortic arch aneurysms. J. Cardiovasc. Surg. 2016, 57, 686–697. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total n = 200 |
|---|---|
| Age (years), mean (SD) | 62.2 (11.6) |
| Male sex, n (%) | 145 (72.5) |
| Hypertension, n (%) | 121 (60.5) |
| Dyslipidemia, n (%) | 40 (19.8) |
| Smoking, n (%) | 36 (18.0) |
| Diabetes, n (%) | 6 (3.0) |
| COPD, n (%) | 11 (5.4) |
| Atrial fibrillation, n (%) | 16 (7.8) |
| CAD, n (%) | 16 (7.8) |
| Peripheral vascular disease, n (%) | 7 (3.6) |
| Renal failure, n (%) | 4 (1.8) |
| Marfan and related syndrome, n (%) | 12 (6.0) |
| Bicuspid aortic, n (%) | 8 (4.2) |
| Total n = 27 (100.0%) | Hybrid n = 21 (77.8%) | Branched Endograft n = 6 (22.2%) | p Value | |
|---|---|---|---|---|
| Age (years), mean (SD) | 63.0 +/−11.7 | 59.7 +/−10.7 | 74.7 +/−6.9 | 0.12 |
| Male sex, n (%) | 17 (63.0) | 14 (66.7) | 3 (50.0) | 0.79 |
| Hypertension, n (%) | 15 (55.6) | 11 (52.4) | 4 (66.7) | 0.87 |
| Dyslipidemia, n (%) | 2 (7.4) | 1 (4.8) | 1 (16.7) | 0.92 |
| Smoking, n (%) | 4 (14.8) | 2 (9.5) | 2 (33.3) | 0.42 |
| Diabetes, n (%) | 1 (3.7) | 1 (4.8) | 0 (0) | 0.58 |
| COPD, n (%) | 4 (14.8) | 3 (14.3) | 1 (16.7) | 0.77 |
| Atrial fibrillation, n (%) | 2 (7.4) | 2 (9.5) | 0 (0) | 0.43 |
| CAD, n (%) | 1 (3.7) | 1 (4.8) | 0 (0) | 0.58 |
| Peripheral vascular disease, n (%) | 1 (3.7) | 1 (4.8) | 0 (0) | 0.58 |
| Renal failure, n (%) | 2 (7.4) | 1 (4.8) | 1 (16.7) | 0.92 |
| Marfan syndrome, n (%) | 5 (18.5) | 5 (23.8) | 0 (0) | 0.46 |
| Total n = 27 (100%) | Hybrid n = 21 (77.8%) | Branched Endograft n = 6 (22.2%) | p Value | |
|---|---|---|---|---|
| Hospital mortality | 0 (0) | 0 (0) | 0 (0) | NA |
| Postoperative morbidity | 7 (25.9) | 6 (28.6) | 1 (16.7) | 0.95 |
| Stroke | 1 (3.7) | 1 (4.8) | 0 (0) | 0.58 |
| Pulmonary complication | 1 (3.7) | 1 (4.8) | 0 (0) | 0.58 |
| Carotid dissection | 1 (3.7) | 0 (0) | 1 (16.7) | 0.49 |
| Major bleeding | 3 (11.1) | 3 (14.3) | 0 (0) | 0.80 |
| Recurential paralysis | 1 (3.7) | 1 (4.8) | 0 (0) | 0.58 |
| Medullary ischemia | 0 (0) | 0 (0) | 0 (0) | NA |
| Number of hospitalizations | 1.8 +/−0.7 | 1.8 +/−0.7 | 1.8 +/−1.0 | 0.96 |
| Cumulative length of stay in intensive care unit | 3.9 +/−2.0 | 4.4 +/−2.5 | 1.8 +/−0.8 | <0.001 |
| Cumulative length of stay in hospital | 13.9 +/−5.3 | 14.8 +/−8.1 | 11.0 +/−4.2 | 0.14 |
| Anatomical results | ||||
| Total aortic remodeling | 11 (40.7) | 10 (47.6) | 1 (16.7) | 0.37 |
| FL thrombosis | 12 (44.4) | 8 (38.1) | 4 (66.7) | 0.44 |
| FL partial thrombosis | 4 (14.8) | 3 (14.3) | 1 (16.7) | 0.88 |
| Type Ia Endoleak | 0 (0) | 0 (0) | 0 (0) | NA |
| Type Ib Endoleak | 4 (14.8) | 3 (14.3) | 1(16.7) | 0.88 |
| Type II Endoleak | 0 (0) | 0 (0) | 0 (0) | NA |
| Type III Endoleak | 0 (0) | 0 (0) | 0 (0) | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porto, A.; Omnes, V.; Bartoli, M.A.; Azogui, R.; Resseguier, N.; De Masi, M.; Bal, L.; Imbert, L.; Jaussaud, N.; Morera, P.; et al. Reintervention of Residual Aortic Dissection after Type A Aortic Repair: Results of a Prospective Follow-Up at 5 Years. J. Clin. Med. 2023, 12, 2363. https://doi.org/10.3390/jcm12062363
Porto A, Omnes V, Bartoli MA, Azogui R, Resseguier N, De Masi M, Bal L, Imbert L, Jaussaud N, Morera P, et al. Reintervention of Residual Aortic Dissection after Type A Aortic Repair: Results of a Prospective Follow-Up at 5 Years. Journal of Clinical Medicine. 2023; 12(6):2363. https://doi.org/10.3390/jcm12062363
Chicago/Turabian StylePorto, Alizée, Virgile Omnes, Michel A. Bartoli, Ron Azogui, Noémie Resseguier, Mariangela De Masi, Laurence Bal, Laura Imbert, Nicolas Jaussaud, Pierre Morera, and et al. 2023. "Reintervention of Residual Aortic Dissection after Type A Aortic Repair: Results of a Prospective Follow-Up at 5 Years" Journal of Clinical Medicine 12, no. 6: 2363. https://doi.org/10.3390/jcm12062363
APA StylePorto, A., Omnes, V., Bartoli, M. A., Azogui, R., Resseguier, N., De Masi, M., Bal, L., Imbert, L., Jaussaud, N., Morera, P., Jacquier, A., Barral, P.-A., Gariboldi, V., & Gaudry, M. (2023). Reintervention of Residual Aortic Dissection after Type A Aortic Repair: Results of a Prospective Follow-Up at 5 Years. Journal of Clinical Medicine, 12(6), 2363. https://doi.org/10.3390/jcm12062363