
Sympathetic Ophthalmia after Vitreoretinal Surgery without Antecedent History of Trauma: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection Data Extraction and Data Synthesis
2.3. Risk of Bias Assessment
2.4. Assessment of Quality of Evidence
2.5. Statistical Analysis
3. Results
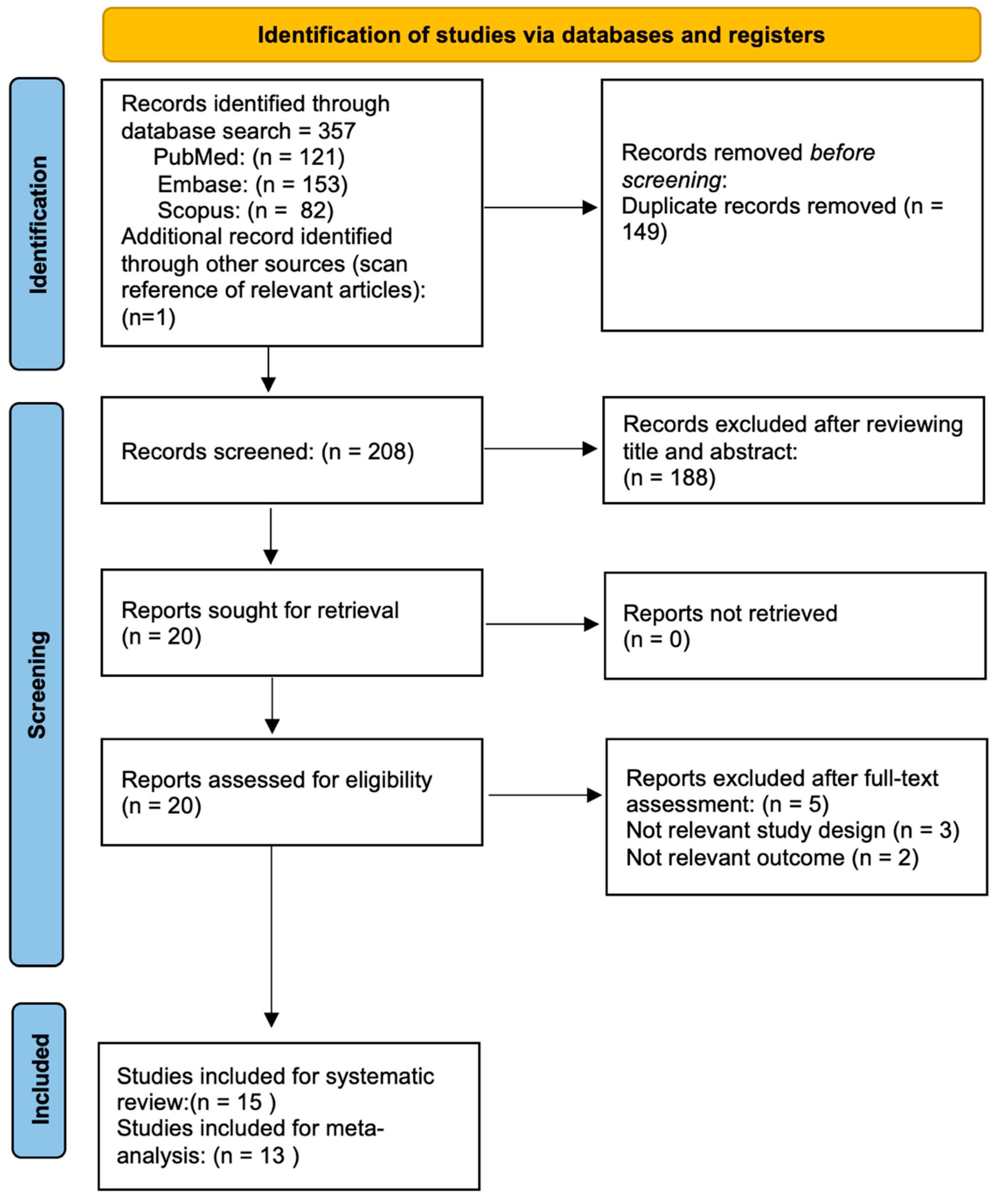
3.1. Study Selection
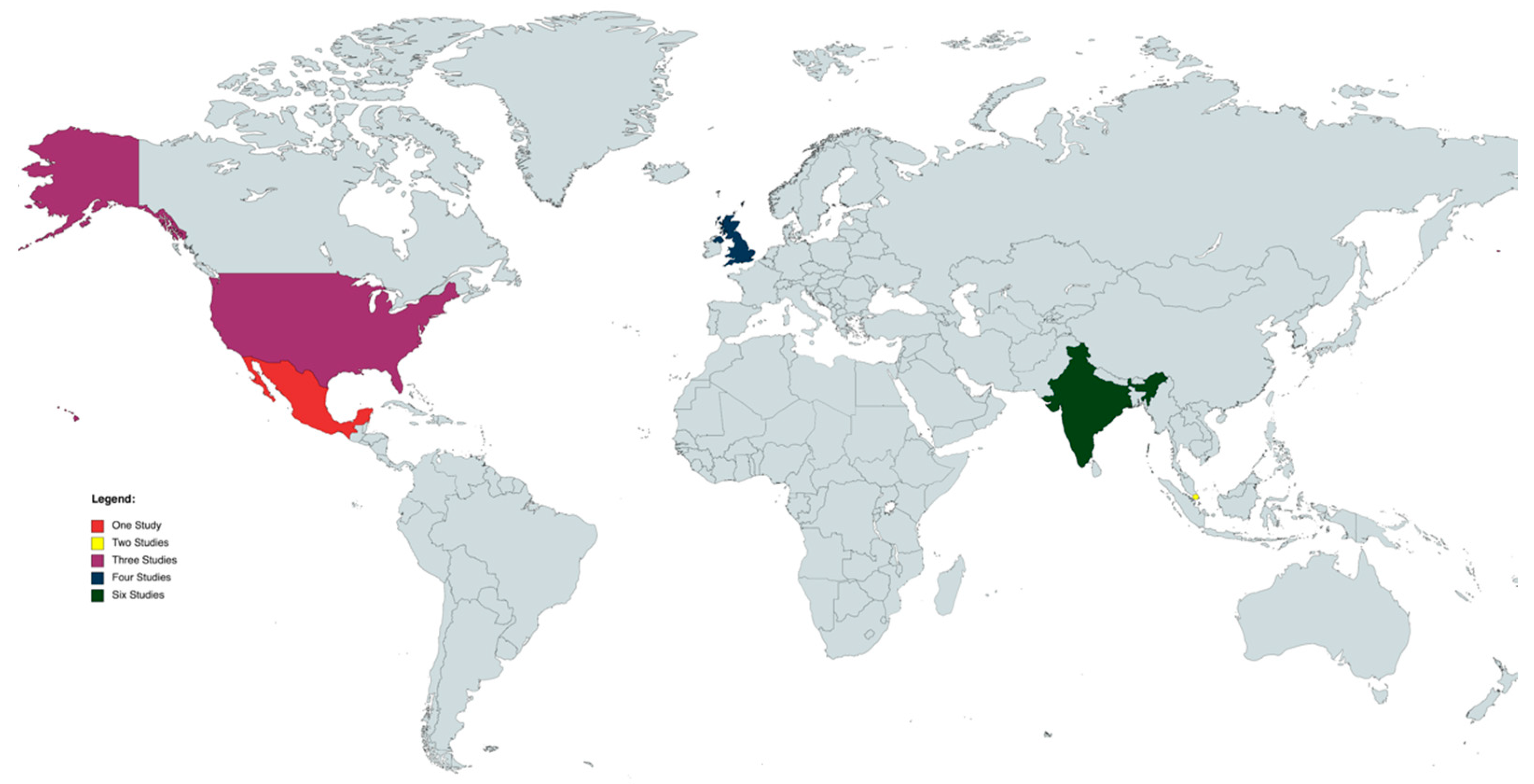
3.2. Study Characteristics
3.3. Meta-Analyses of Cumulative Incidence and Subgroups Meta-Analysis
3.4. Risk of Bias and GRADE Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Name | Year of Publication | Country | Age of SO Patients after VR Surgery (Average ± SD) | Study Design | Duration (y.) | Number of SO Cases in the Study | Number of Cases of SO after Trauma (N and %) in the Study | Number of Cases of SO after Surgery (N and %) in the Study | Number of Cases of SO after VR Surgery (±Lens Extraction) (N and %) in the Study | Number of Cases of SO after Other Surgeries (N and %) in the Study | VR Procedures | Other Surgeries: | Total Number of VR Procedures in the Study | Other Relevant Parameters Evaluated: |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gass et al. [9] | 1982 | USA | 52 ± 13.98 | Cross-Sectional | Five years | 1. Survey of eye pathology laboratories: 53 2. Armed Forces Institute of Pathology: 33 3. Survey of retinal surgeons: 9 | 1. Survey of eye pathology laboratories: 29 (54.7%) 2. Armed Forces Institute of Pathology: not stated 3. Survey of retinal surgeons: 3 (33.3%) | 1. Survey of eye pathology laboratories: 24 (45.3%) 2. Armed Forces Institute of Pathology: 1 (3%) 3. Survey of retinal surgeons: 4 (44.4%) | 1. Survey of eye pathology laboratories: Exclusively Retinal Surgery: 3 (5.7%) Retinal Surgery + Lens extraction: 3 (5.7%) 2. Armed Forces Institute of Pathology: Retinal Surgery + Lens extraction: 1 (3%) 3. Survey of retinal surgeons: Exclusively Retinal Surgery: 1 (11.1%) | 1. Survey of eye pathology laboratories: 14 (26.4%) 2. Armed Forces Institute of Pathology: not stated 3. Survey of retinal surgeons: not stated | 1. Survey of eye pathology laboratories: SB: 3 (5.7%) 2. Armed Forces Institute of Pathology: 0 3. Survey of retinal surgeons: PPV: 1 (11.1%) | 1. Survey of eye pathology laboratories: Cataract extraction. 10 Filtering operation 3, Combined cataract extraction and filtering operation 1 2. Armed Forces Institute of Pathology: not stated 3. Survey of retinal surgeons: not stated | 1. Survey of eye pathology laboratories: 22.840 (surgical specimens) 2. Armed Forces Institute of Pathology: 3.000 eyes 3. Survey of retinal surgeons: 14.915 vitrectomies | / |
| Jennings et al. [7] | 1989 | USA | 62.3 ± 7.76 | Cross-Sectional | 11-year period: 1974 to 1985 | 20 | 16 (80%) | 3 (15%) | Exclusively Retinal Surgery: 1 (5%) | 2 (10%) | PPV: 1 (5%) | 2 (10%) Extracapsular Extraction with vitreous loss, 2 steroid injections, and 2 vitrectomies. Extracapsular Extraction with a dropped nucleus. | Not stated | SO from onset to last Observation in patients after VR surgery: 12.33 ± 14.46 months |
| Kilmartin et al. [6] | 2000 | UK | 66 ± 10.2 | Cross-Sectional | July 1997 to September 1998, 14 months | 18 | Exclusively Trauma: 6 (33%) Trauma + Surgery: 2 (11.1%) | 10 (56%) | Exclusively Retinal Surgery: 6 (33%) 3 of these patients having undergone just one PPV Retinal Surgery + Lens extraction: 2 (11.1%) | 3 (16.7%) | PPV RD: 5 (27.8%) Ext RD: 1 (5.5%) | Trabeculectomy: 1 (5.5%) Ext beam DTX, PPV X2, Enucl: 1 (5.5%) Ext RD, PPV RD, Cyclodiodetx: 1 (5.5%) | Not stated | / |
| Pollack et al. [16] | 2001 | USA | 48.87 ± 21.79 | Case series | Not stated | 8 | 0 | 8 (100%) | Exclusively Retinal Surgery: 1 (12.5%) Retinal Surgery + Lens extraction: 6 | 1 (12.5%) | PPV: 1 PPV + SB + Lens Extraction:6 | Tectonic PKP, PPV: 1 (12.5%) | Not Stated | Time from PPV to onset of symptoms of SO: median of 7 months. Follow-up from onset of symptoms: 10.5 months Initial VA in sympathizing eye: 0.67 ± 0.56 LogMAR Final VA in the sympathizing eye: 0.47 ± 0.59 |
| Grigoropoulos et al. [11] | 2006 | UK | Not stated | Cohort | Not stated | 1 | 0 | 0 | 1 | 0 | PPV + 210° retinectomy. | None | 1142 operations performed on the 304 eyes. | VA was limited to PL and the eye was hypotonus Thirty-one months after the initial procedure and 9 months after the last procedure, the fellow eye developed SO VA in the fellow eye decreased from 6/9 to 6/18 and remained stable |
| Su et al. [18] | 2005 | Singapore | 63 ± 19.98 | Case series | 1993–2003, ten years | 10 (1.08%) | Exclusively Trauma: 1 (10%) Trauma + Surgery: 3 (30%) | 6 (60%) | Exclusively Retinal Surgery: 1 (10%) Retinal Surgery + Lens extraction: 2 (20%) | 3 (30%) | Not stated | TCP: 2 YAG-TCP: 1 | 924 | Retinal surgery patients: Patient 1: initial VA in SE: 0.4 LogMAR Final VA in SE: 0.7 LogMAR Patient 2: initial VA in SE: 0.4 LogMAR Final VA in SE: 0.5 LogMAR Patient 3: initial VA in SE: HM Final VA in SE: NPL Interval between IE and onset of symptoms: (mean ± SD): 29 ± 32.51 months |
| Gupta et al. [10] | 2007 | India | Not stated | Cross-Sectional | June 1989–August 2004, 15 years and 2 months | 40 | 30 (75%) | 10 (25%) | Exclusively Retinal Surgery: 4 (10%) | 6 (15%) | PPV: 2 (5%) SB: 2 (5%) | Lens extraction: 5 (12.5%) Glaucoma Filtration Surgery: 1 (2.5%) | Not stated | / |
| Kumar et al. [13] | 2013 | India | Not stated (pediatric age) | Cross-Sectional | 2001–2011, ten years | 14 | Exclusively Trauma:13 (92.9%) | 1 (7.1%) | Exclusively Retinal Surgery: 1 (7.1%) | 0 | PPV: 1 (7.1%) | / | 2511 pediatric patients with open globe injuries | / |
| Rishi et al. [17] | 2015 | India | 39.4 ± 14.72 | Comparative case series | 1995–2011, 16 years | 17 | Trauma + VR surgery: 7 (41.2%) | 10 (58.8%) | Exclusively Retinal Surgery: 5 (29.4%) Retinal Surgery + Lens extraction: 5 (29.4%) | 0 | SB: 3 SB + PPV: 2 | None | Not stated | Initial VA in SE (mean ± SD): 0.78 ± 0.72 Final VA in SE (mean ± SD): 0.26 ± 0.55 Follow-up (mean ± SD): 45 ± 52.74 months Duration of symptoms 22.5 days Interval between surgery and SO (mean ± SD): 38.1 ± 52.79 months Average Follow-up period 34 months |
| Guzman-Salas et al. [15] | 2016 | Mexico | Not Stated | Cross-Sectional | 2007–2013, 6 years | 20 | 10 (50%) | 10 (50%) | Exclusively Retinal Surgery: 3 (15%) | 7 (45%) | Retinopexy | Lens Extraction: 6 (30%) Ahmed valve implantation 1 (5%) | Not Stated | / |
| Dutta Majumder et al. [12] | 2017 | India | Not Stated | Cross-Sectional | June 1994–November 2015: 21 years and 5 months | 197 | Not Stated | 14 (7.1%) | Exclusively Retinal Surgery: 8 (4.1%) | 6 (3%) | SB: 4 (2%) PPV: 4 (2%) | Lens Extraction: 1 (0.5%) Lens Extraction + Anterior Vitrectomy: 3 (1.5%) Trabeculectomy: 1 (0.5%) PKP: 1 (0.5%) | Not Stated | / |
| Tyagi et al. [20] | 2019 | India | 41.14 ± 16.53 | Retrospective case series | 2005–2015, ten years | 175 | 0 | 16 (9.1%) | Exclusively Retinal Surgery: 13 (7.4%) Retinal Surgery + Lens extraction: 3 (1.7%) | Not Stated | PPV: 8 (4.6%) SB + PPV: 5 (2.9%) | Not Stated | 41.365 PPV | Time interval from surgery to diagnosis: (mean): 154 days 2. VA: Initial VA in SE (mean ± SD): 1.03 ± 0.56 LogMar Final VA in SE (mean ± SD): 0.43 ± 0.57 LogMar Duration of follow-up of (mean) 25.8 months Duration from surgery (days): 194.5 ± 349.28 |
| Tan et al. [19] | 2018 | India UK Singapore | Not Stated | Retrospective Multicenter Case Series | 1995–2014, 9 years | 130 | 94 (72.3%) | 36 (27.9%) | 13 (36.1%) | 23 | Not Stated | Lens Extraction 11 (30.5%) Glaucoma surgery 6 (16.7%) Others: 6 (16.7%) | Not Stated | / |
| Dutta Majumder et al. [8] | 2020 | India | Not Stated (Pediatric Age) | Retrospective Case Series | December 1997–January 2017, 19 years, 1 month | 20 | Exclusively Trauma: 13 (65%) Trauma + Surgery: 4 (20%) | 3 (15%) | 3 (15%) | 0 | Not Stated | None | Not Stated | / |
| Anikina et al. [14] | 2022 | UK | Cross-Sectional | January 2000 and December 2015, 15 year period | 61 | 40 (65.6%) | 21 (34.4%) as main trigger | 13 (21.3%) as main trigger | Not Stated | 10 multiple procedures: SB: 6 PPV: 21 (1 of the cases involved a combination). | Not Stated | 39.391 VR procedures SO after a single VR procedure was estimated to be 0.008%, rising to 6.67% with 7 procedures | / |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lucchini, S.; Govetto, A.; Carini, E.; Casalino, G.; Donati, S.; Radice, P. Presumed sympathetic ophthalmia following scleral buckling surgery: A case report and review of the literature. Eur. J. Ophthalmol. 2022, 14, 11206721221145212. [Google Scholar] [CrossRef]
- Vote, B.J.; Hall, A.; Cairns, J.; Buttery, R. Changing trends in sympathetic ophthalmia. Clin. Exp. Ophthalmol. 2004, 32, 542–545. [Google Scholar] [CrossRef]
- Galor, A.; Davis, J.L.; Flynn, H.W.; Feuer, W.J.; Dubovy, S.R.; Setlur, V.; Kesen, M.R.; Goldstein, D.A.; Tessler, H.H.; Ganelis, I.B.; et al. Sympathetic ophthalmia: Incidence of ocular complications and vision loss in the sympathizing eye. Am. J. Ophthalmol. 2009, 148, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Marak, G.E. Recent advances in sympathetic ophthalmia. Surv. Ophthalmol. 1979, 24, 141–156. [Google Scholar] [CrossRef]
- Lam, S.; Tessler, H.H.; Lam, B.L.; Wilensky, J.T. High incidence of sympathetic ophthalmia after contact and noncontact neodymium: YAG cyclotherapy. Ophthalmology 1992, 99, 1818–1822. [Google Scholar] [CrossRef]
- Kilmartin, D.J.; Dick, A.D.; Forrester, J.V. Prospective surveillance of sympathetic ophthalmia in the UK and Republic of Ireland. Br. J. Ophthalmol. 2000, 84, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Jennings, T.; Tessler, H.H. Twenty cases of sympathetic ophthalmia. Br. J. Ophthalmol. 1989, 73, 140–145. [Google Scholar] [CrossRef]
- Majumder, P.D.; Mistry, S.; Sridharan, S.; George, A.E.; Rao, V.; Ganesh, S.K.; Biswas, J. Pediatric sympathetic ophthalmia: 20 years of data from a tertiary eye center in India. J. Pediatr. Ophthalmol. Strabismus 2020, 57, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Gass, J.D.M. Sympathetic ophthalmia following vitrectomy. Am. J. Ophthalmol. 1982, 93, 552–558. [Google Scholar] [CrossRef]
- Gupta, V.; Gupta, A.; Dogra, M.R. Posterior sympathetic ophthalmia: A single centre long-term study of 40 patients from North India. Eye 2008, 22, 1459–1464. [Google Scholar] [CrossRef] [PubMed]
- Grigoropoulos, V.G.; Benson, S.; Bunce, C.; Charteris, D.G. Functional outcome and prognostic factors in 304 eyes managed by retinectomy. Graefes Arch. Clin. Exp. Ophthalmol. 2007, 245, 641–649. [Google Scholar] [CrossRef]
- Dutta Majumder, P.; Anthony, E.; George, A.E.; Ganesh, S.K.; Biswas, J. Postsurgical sympathetic ophthalmia: Retrospective analysis of a rare entity. Int. Ophthalmol. 2018, 38, 2487–2493. [Google Scholar] [CrossRef]
- Kumar, K.; Mathai, A.; Murthy, S.I.; Jalali, S.; Sangwan, V.; Reddy Pappuru, R.; Pathangay, A. Sympathetic ophthalmia in pediatric age group: Clinical features and challenges in management in a tertiary center in Southern India. Ocul. Immunol. Inflamm. 2014, 22, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Anikina, E.; Wagner, S.K.; Liyanage, S.; Sullivan, P.; Pavesio, C.; Okhravi, N. The risk of sympathetic ophthalmia after vitreoretinal surgery. Ophthalmol. Retina 2022, 6, 347–360. [Google Scholar] [CrossRef]
- Guzman-Salas, P.J.; Serna-Ojeda, J.C.; Guinto-Arcos, E.B.; Pedroza-Seres, M. Characteristics of sympathetic ophthalmia in a single international center. Open Ophthalmol. J. 2016, 10, 154. [Google Scholar] [CrossRef] [PubMed]
- Pollack, A.L.; McDonald, H.R.; Ai, E.; Green, W.R.; Halpern, L.S.; Jampol, L.M.; Leahy, J.M.; Johnson, R.N.; Spencer, W.H.; Stern, W.H.; et al. Sympathetic ophthalmia associated with Pars Plana Vitrectomy without antecedent penetrating trauma. Retina 2001, 21, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Rishi, E.; Rishi, P.; Appukuttan, B.; Walinjkar, J.; Biswas, J.; Sharma, T. Sympathetic ophthalmitis following vitreoretinal surgery: Does antecedent trauma make a difference? Indian J. Ophthalmol. 2015, 63, 692–698. [Google Scholar] [CrossRef]
- Su, D.H.W.; Chee, S.P. Sympathetic ophthalmia in Singapore: New trends in an old disease. Graefes Arch. Clin. Exp. Ophthalmol. 2006, 244, 243–247. [Google Scholar] [CrossRef]
- Tan, X.L.; Seen, S.; Dutta Majumder, P.; Ganesh, S.K.; Agarwal, M.; Soni, A.; Biswas, J.; Aggarwal, K.; Mahendradas, P.; Gupta, V.; et al. Analysis of 130 cases of sympathetic ophthalmia—A retrospective multicenter case series. Ocul. Immunol. Inflamm. 2018, 27, 1259–1266. [Google Scholar] [CrossRef]
- Tyagi, M.; Agarwal, K.; Reddy Pappuru, R.R.; Dedhia, C.; Agarwal, H.; Nayak, S.; Panchal, B.; Kaza, H.; Basu, S.; Pathengay, A.; et al. Sympathetic ophthalmia after vitreoretinal surgeries: Incidence, clinical presentations and outcomes of a rare disease. Semin. Ophthalmol. 2019, 34, 157–162. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Cleo, G.; Scott, A.M.; Islam, F.; Julien, B.; Beller, E. Usability and acceptability of four systematic review automation software packages: A mixed method design. Syst. Rev. 2019, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal Tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Barker, T.H.; Borges Migliavaca, C.; Stein, C.; Colpani, V.; Falavigna, M.; Aromataris, E.; Munn, Z. Conducting proportional meta-analysis in different types of systematic reviews: A guide for synthesisers of evidence. BMC Med. Res. Methodol. 2021, 21, 189. [Google Scholar] [CrossRef]
- Hakin, K.N.; Pearson, R.V.; Lightman, S.L. Sympathetic ophthalmia: Visual results with modern immunosuppressive therapy. Eye 1992, 6 Pt 5, 453–455. [Google Scholar] [CrossRef] [PubMed]
- De Juan, E.; Hickingbotham, D. Refinements in microinstrumentation for vitreous surgery. Am. J. Ophthalmol. 1990, 109, 218–220. [Google Scholar] [CrossRef] [PubMed]
- Haruta, M.; Mukuno, H.; Nishijima, K.; Takagi, H.; Kita, M. Sympathetic ophthalmia after 23-gauge transconjunctival sutureless vitrectomy. Clin. Ophthalmol. 2010, 4, 1347–1349. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ripa, M.; Panos, G.D.; Rejdak, R.; Empeslidis, T.; Toro, M.D.; Costagliola, C.; Ferrara, A.; Gotzaridis, S.; Frisina, R.; Motta, L. Sympathetic Ophthalmia after Vitreoretinal Surgery without Antecedent History of Trauma: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 2316. https://doi.org/10.3390/jcm12062316
Ripa M, Panos GD, Rejdak R, Empeslidis T, Toro MD, Costagliola C, Ferrara A, Gotzaridis S, Frisina R, Motta L. Sympathetic Ophthalmia after Vitreoretinal Surgery without Antecedent History of Trauma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(6):2316. https://doi.org/10.3390/jcm12062316
Chicago/Turabian StyleRipa, Matteo, Georgios D. Panos, Robert Rejdak, Theodoros Empeslidis, Mario Damiano Toro, Ciro Costagliola, Andrea Ferrara, Stratos Gotzaridis, Rino Frisina, and Lorenzo Motta. 2023. "Sympathetic Ophthalmia after Vitreoretinal Surgery without Antecedent History of Trauma: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 6: 2316. https://doi.org/10.3390/jcm12062316
APA StyleRipa, M., Panos, G. D., Rejdak, R., Empeslidis, T., Toro, M. D., Costagliola, C., Ferrara, A., Gotzaridis, S., Frisina, R., & Motta, L. (2023). Sympathetic Ophthalmia after Vitreoretinal Surgery without Antecedent History of Trauma: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(6), 2316. https://doi.org/10.3390/jcm12062316