
Safe and Successful Surgical Outcome in Persons with Hemophilia A with and without Inhibitors Treated with Emicizumab: A Large, Single Center, Real-World Experience

 , , ,
, , ,  ,
,
Abstract
1. Introduction
1.1. Patients and Methods
1.2. Data Analyses
2. Results
2.1. Patient Characteristics and Surgery Overview
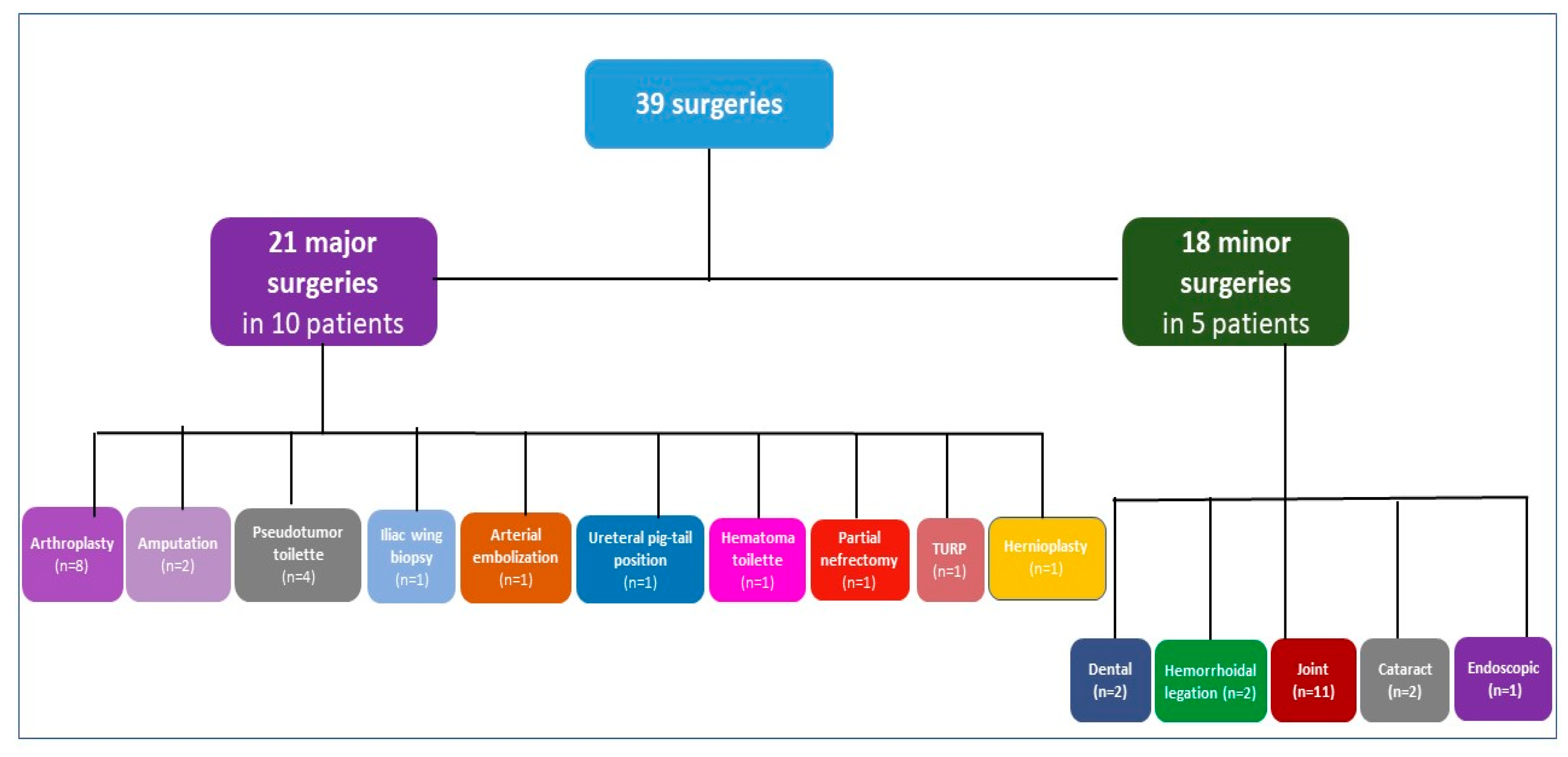
2.2. Surgeries in PWSHA and Inhibitors
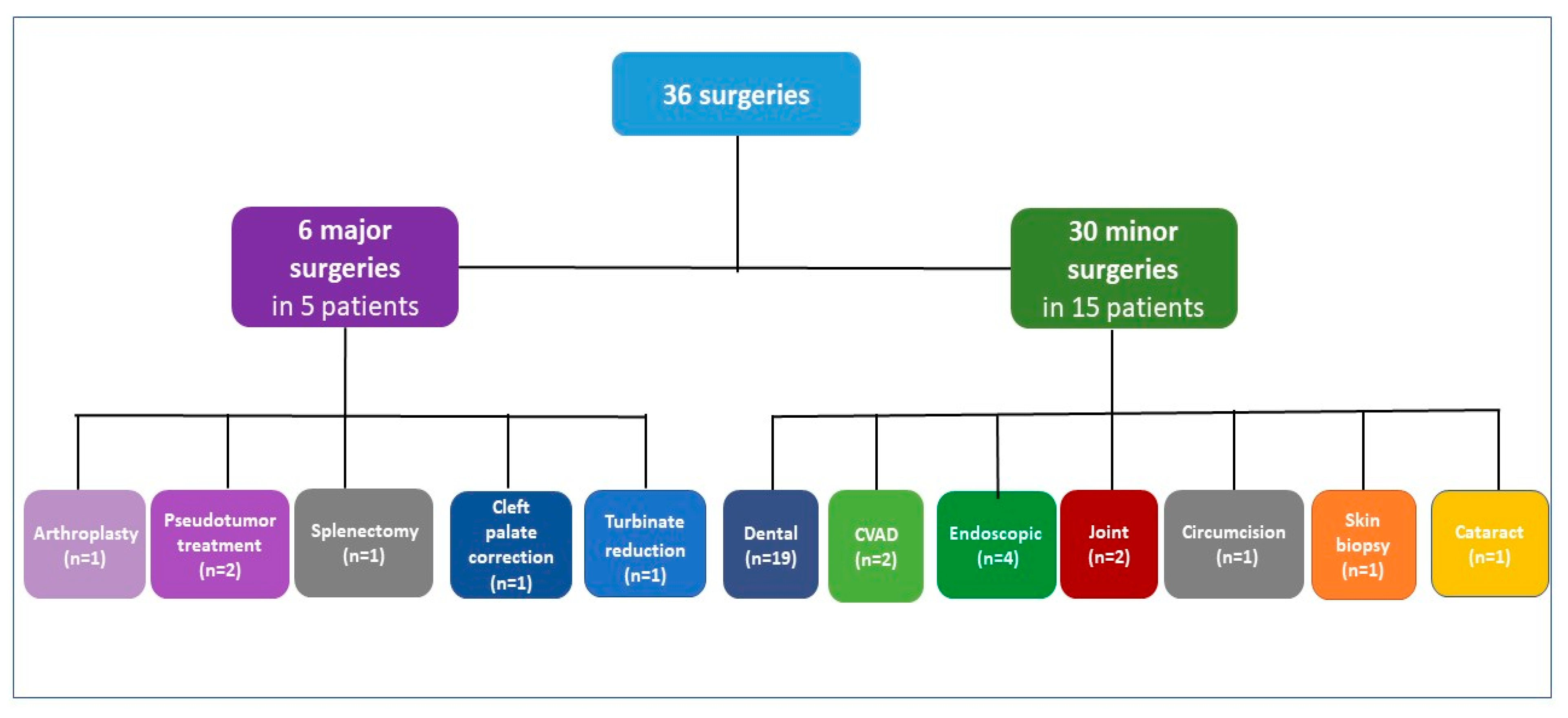
2.3. Surgeries in PWSHA without Inhibitors
3. Discussion
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Srivastava, A.; Santagostino, E.; Dougall, A.; Kitchen, S.; Sutherland, M.; Pipe, S.W.; Carcao, M.; Mahlangu, J.; Ragni, M.V.; Windyga, J.; et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia 2020, 26 (Suppl. S6), 1–158. [Google Scholar] [CrossRef] [PubMed]
- Shima, M.; Hanabusa, H.; Taki, M.; Matsushitaet, T.; Sato, T.; Fukutake, K.; Fukazawa, N.; Yoneyama, K.; Yoshida, H.; Nogami, K. Factor VIII-mimetic function of humanized bispecific antibody in hemophilia A. N. Engl. J. Med. 2016, 374, 2044–2053. [Google Scholar] [CrossRef] [PubMed]
- Lenting, P.J.; Denis, C.V.; Christophe, O.D. Emicizumab, a bispecific antibody recognizing coagulation factors IX and X: How does it actually compare to factor VIII? Blood 2017, 130, 2463–2468. [Google Scholar] [CrossRef]
- Oldenburg, J.; Mahlangu, J.N.; Kim, B.; Schmitt, C.; Callaghan, M.U.; Young, G.; Santagostino, E.; Kruse-Jarres, R.; Negrier, C.; Kessler, C.; et al. Emicizumab prophylaxis in hemophilia A with Inhibitors. N. Engl. J. Med. 2017, 377, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Young, G.; Liesner, R.; Chang, T.; Sidonio, R., Jr.; Oldenburg, J.; Jiménez-Yuste, V.; Mahlangu, J.; Kruse-Jarres, R.; Wang, M.; Uguen, M.; et al. A multicenter, open-label phase 3 study of emicizumab prophylaxis in children with hemophilia A with inhibitors. Blood 2019, 134, 2127–2138. [Google Scholar] [CrossRef]
- Mahlangu, J.; Oldenburg, J.; Paz-Priel, I.; Negrier, C.; Niggli, M.; Mancuso, M.E.; Schmitt, C.; Kempton, C.; Dhalluin, C.; Callaghan, M.U.; et al. Emicizumab prophylaxis in patients who have hemophilia A without inhibitors. N. Engl. J. Med. 2018, 379, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Pipe, S.W.; Shima, M.; Lehle, M.; Shapiro, A.; Chebon, S.; Fukutake, K.; Key, N.S.; Portron, A.; Schmitt, C.; Podolak-Dawidziak, M.; et al. Efficacy, safety, and pharmacokinetics of emicizumab prophylaxis given every 4 weeks in people with haemophilia A (HAVEN 4): A multicentre, open-label, non-randomised phase 3 study. Lancet Haematol. 2019, 6, e295–e305. [Google Scholar] [CrossRef]
- Coppola, A.; Castaman, G.; Santoro, R.C.; Mancuso, M.E.; Franchini, M.; Marino, R.; Rivolta, G.F.; Santoro, C.; Zanon, E.; Sciacovelli, L.; et al. Management of patients with severe haemophilia a without inhibitors on prophylaxis with emicizumab: AICE recommendations with focus on emergency in collaboration with SIBioC, SIMEU, SIMEUP, SIPMeL and SISET. Haemophilia 2020, 26, 937–945. [Google Scholar] [CrossRef]
- Levy, G.G.; Asikanius, E.; Kuebler, P.; Benchikh El Fegoun, S.; Esbjerg, S.; Seremetis, S. Safety analysis of rFVIIa with emicizumab dosing in congenital hemophilia A with inhibitors: Experience from the HAVEN clinical program. J. Thromb. Haemost. 2019, 17, 1470–1477. [Google Scholar] [CrossRef]
- Castaman, G.; Santoro, C.; Coppola, A.; Mancuso, M.E.; Santoro, R.C.; Bernardini, S.; Pugliese, F.R.; Lubrano, R.; Golato, M.; Tripodi, A.; et al. Emergency management in patients with haemophilia A and inhibitors on prophylaxis with emicizumab: AICE practical guidance in collaboration with SIBioC, SIMEU, SIMEUP, SIPMeL and SISET. Blood Transfus. 2020, 18, 143–151. [Google Scholar]
- Callaghan, M.U.; Negrier, C.; Paz-Priel, I.; Chang, T.; Chebon, S.; Lehle, M.; Mahlangu, J.; Young, G.; Kruse-Jarres, R.; Mancuso, M.E.; et al. Long-term outcomes with emicizumab prophylaxis for hemophilia A with or without FVIII inhibitors from the HAVEN 1-4 studies. Blood 2021, 137, 2231–2242. [Google Scholar] [CrossRef] [PubMed]
- Kruse-Jarres, R.; Peyvandi, F.; Oldenburg, J.; Chang, T.; Chebon, S.; Doral, M.Y.; Croteau, S.E.; Lambert, T.; Kempton, C.L.; Pipe, S.W.; et al. Surgical outcomes in people with hemophilia A taking emicizumab prophylaxis: Experience from the HAVEN 1–4 studies. Blood Adv. 2022, 6, 6140–6149. [Google Scholar] [CrossRef] [PubMed]
- McCary, I.; Guelcher, C.; Kuhn, J.; Butler, R.; Massey, G.; Guerrera, M.F.; Ballester, L.; Raffini, L. Real-world use of emicizumab in patients with haemophilia A: Bleeding outcomes and surgical procedures. Haemophilia 2020, 26, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, M.; Randall, N.; Bakeer, N.; Maahs, J.; Sagar, J.; Greist, A.; Shapiro, A.D. Management of people with haemophilia a undergoing surgery while receiving emicizumab prophylaxis: Real-world experience from a large comprehensive treatment centre in the US. Haemophilia 2021, 27, 90–99. [Google Scholar] [CrossRef]
- Jiménez-Yuste, V.; Rodríguez-Merchán, E.C.; Matsushita, T.; Holme, P.A. Concomitant use of bypassing agents with emicizumab for people with haemophilia A and inhibitors undergoing surgery. Haemophilia 2021, 27, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Swan, D.; Paran, S.; Nolan, B. Port removal in patients receiving emicizumab prophylaxis: A single centre experience and review of the literature. Haemophilia 2022, 28, 42–45. [Google Scholar] [CrossRef]
- Santagostino, E.; Lentz, S.R.; Misgav, M.; Brand, B.; Chowdary, P.; Savic, A.; Kilinc, Y.; Amit, Y.; Amendola, A.; Solimeno, L.P.; et al. Safety and efficacy of turoctocog alfa (NovoEight®) during surgery in patients with haemophilia A: Results from the multinational guardian clinical trials. Haemophilia 2015, 21, 34–40. [Google Scholar] [CrossRef]
- Schulman, S.; Angerås, U.; Bergqvist, D.; Eriksson, B.; Lassen, M.R.; Fisher, W.; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J. Thromb. Haemost. 2010, 8, 202–204. [Google Scholar] [CrossRef]
- Müller, J.; Pekrul, I.; Pötzsch, B.; Berning, B.; Oldenburg, J.; Spannagl, M. Laboratory monitoring in emicizumab-treated persons with hemophilia A. Thromb. Haemost. 2019, 119, 1384–1393. [Google Scholar] [CrossRef]
- Frusconi, S.; Passerini, I.; Girolami, F.; Masieri, M.; Linari, S.; Longo, G.; Morfini, M.; Torricelli, F. Identification of seven novel mutations of F8C by DHPLC. Hum. Mutat. 2002, 20, 231–232. [Google Scholar] [CrossRef]
- Barg, A.A.; Budnik, I.; Avishai, E.; Brutman-Barazani, T.; Bashari, D.; Misgav, M.; Lubetsky, A.; Kuperman, A.A.; Livnat, T.; Kenet, G. Emicizumab prophylaxis: Prospective longitudinal real-world follow-up and monitoring. Haemophilia 2021, 27, 383–391. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient N. | Surgery N. | Age (yrs) | Pathogenic Mutation | Historical FVIII INH Peak (BU/mL) | FVIII INH at Surgery (BU/mL) | Surgery Type | rFVIIa Use ° | TA Use * | Bleeding Episode | Transfusion Requirement | Days of Hospitalization |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 59 | EX 23-26 deletion | 70 | 2 | THR | Yes | Yes | Yes | Yes (2 RBC) | 12 |
| 1 | 2 | 62 | - | 70 | 1.8 | TURP | Yes | No | No | No | 5 |
| 1 | 3 | 62 | - | 70 | 1.8 | Inguinal hernioplasty | Yes | No | No | No | 5 |
| 2 | 4 | 56 | EX 15 c.1727 del3bp ins22bp | 7.9 | 2.8 | Amputation of a thigh | Yes | Yes | No | No | 12 |
| 2 | 5 | 57 | 7.9 | 4.4 | TKR | Yes | Yes | No | No | 15 | |
| 3 | 6 | 49 | EX 2-25 deletion | 840 | 760 | TKR revision | Yes | Yes | No | No | 12 |
| 3 | 7 | 49 | - | 840 | 680 | Revision THR | Yes | Yes | Yes | Yes (4 RBC) | 23 |
| 4 | 8 | 61 | IVS-22 | UK | 2.9 | Revision THR | Yes | Yes | No | No | 12 |
| 5 | 9 | 62 | IVS-22 | UK | 6.1 | Pseudotumor of thigh biopsy | Yes | Yes | No | No | 4 |
| 5 | 10, 11, 12 | 62 | - | UK | 6.1 | Pseudotumor of thigh removal | Yes | Yes | No | No | 15 |
| 5 | 13 | 62 | - | UK | 6.1 | Amputation of a thigh | Yes | Yes | Yes | 3 | 32 |
| 6 | 14 | 58 | EX 7-13 deletion | 16,400 | 2.5 | Iliac wing biopsy | Yes | Yes | No | No | 41 |
| 6 | 15 | 58 | - | 16,400 | 2.5 | Lumbar arterial embolization | Yes | Yes | No | No | 41 |
| 6 | 16 | 58 | - | 16,400 | 2.5 | Ureteral pig-tail positioning | Yes | Yes | No | No | 41 |
| 6 | 17 | 58 | - | 16,400 | 2.5 | Retroperitoneal hematoma curettage | Yes | Yes, for 14 days | Yes | Yes (5 RBC, 10 FFP, 2 PC) | 41 |
| 7 | 18 | 64 | p. Arg427X | 154 | 15 | Partial nefrectomy for renal cancer | Yes | Yes | No | No | 7 |
| 8 | 19 | 42 | EX 5-13 deletion | 1200 | 15 | TKR | Yes | Yes | No | No | 12 |
| 9 | 20 | 49 | IVS 22 | 32 | 0.5 | THR | Yes | Yes | No | No | 12 |
| 10 | 21 | 56 | p.Leu264Gln | 41 | 0.5 | THR | Yes | Yes | No | No | 15 |
| Patient N. | Surgery N. | Age (yrs) | Pathogenic Mutation | FVIII INH Historical Peak (BU/mL) | FVIII INH at Surgery (BU/mL) | Surgery Type | Pre-Operative Factor Treatment | Post-Operative Factor Treatment | TA Use | Bleeding Episode | Hemostatic Treatment | Days of Hospitalization |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1, 2 | 59 | EX 23-26 deletion | 70 | 2 | Intra-articular administration of hyaluronic acid (N.2) | No | No | No | No | No | 0 |
| 1 | 3, 4 | 60 | 70 | 2 | Cataract (N.2) | No | No | No | No | No | 0 | |
| 1 | 5 * | 62 | 70 | 1.8 | Endoscopic removal of bladder stones * | Yes * | Yes * | No | No | No | 5 * | |
| 2 | 6, 7, 8, 9, 10, 11, 12, 13, 14 | 42 | EX 5-13 deletion | 1200 | 15 | Intra-articular administration of hyaluronic acid (N.9) | No | No | No | No | No | 0 |
| 3 | 15, 16 | 56 | EX 15 cod 1727 del3bp ins22bp | 7.9 | 4.4 | Hemorrhoidal varices ligation (N.2) | No | No | No | Yes, in surgery N.15 | FVIIa 90 µg/kg + TA 1 g every 8 h for 4 days | 0 |
| 3 | 17 | 56 | EX 15 cod 1727 del3bp ins22bp | 7.9 | 4.4 | Dental extraction | FVIIa 90 µg/kg | No | Mouth wash with TA 0.5 g every 8 h for 7 days | No | No | 0 |
| 4 | 18 | 32 | EX 14-27 deletion | 10,200 | 520 | Dental extraction | FVIIa 90 µg/kg | No | Mouth wash with TA 0.5 g every 8 h for 7 days | No | No | 0 |
| Patient N. | Surgery N. | Age (yrs) | Pathogenic Mutation | Surgery Type | Pre-Operative Factor Treatment | Post-Operative Factor Treatment | Adjunctive Antifibrinolytics | Bleeding Episode | Transfusion Requirement | Days of Hospitalization |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 28 | p.Trp1854Cys | TKR with forced extension on post-operative 9 day | SHL-rFVIII 70 IU/kg | 43 IU/kg every 12 h × 3 days; 43 IU/kg every 24 h × 5 days; 43 IU/kg every 12 h × 1 day; 28 IU/kg every 12 h × 3 days; 14 IU/kg every 12 h × 2 days; 14 IU/kg every 24 h × 7 days | TA 1 g i.v. every 12 h × 7 days | No | No | 15 |
| 2 | 2 | 63 | Arg1689Cys + Asp1241Glu | Pseudotumor of thigh biopsy | SHL-rFVIII 66 IU/kg | 50 U/kg every 24 h × 3 days; 50 U/kg every 48 h × 4 days | TA 1 g i.v. every 12 h × 7 days | No | No | 0 |
| 2 | 3 | 63 | Arg1689Cys + Asp1241Glu | Pseudotumor of thigh excision | SHL-rFVIII 85 IU/kg | 50 IU/kg every 12 h × 1 day; 30 IU/kg every 12 h × 6 days; 50 IU/kg every 24 h × 7 days | TA 1 g i.v. every 12 h × 7 days | No | No | 7 |
| 3 | 4 | 47 | IVS-1 | Splenectomy | SHL-rFVIII 70 IU/kg | 35 IU/kg every 12 h × 2 days; 23 IU/kg every 12 h × 4 days; 35 IU/kg every 24 h × 7 days | TA 1 g i.v. every 8 h × 7 days | No | No | 11 |
| 4 | 5 | 5 | c.[3430del], p.Ser1144ValfsX5 | Cleft palate correction (2nd operation) | SHL-rFVIII 55 IU/kg | 55 IU/kg every 12 h × 1 day; 55 IU/kg every 24 h × 6 days. 55 IU/kg every 48 h × 7 days | TA 0.5 g orally every 8 h × 14 days | No | No | 7 |
| 5 | 6 | 39 | p.Arg2323Cys | Turbinate reduction | EHL-rFVIII 25IU/kg | 25 IU/kg every 24 h × 2 days | TA 1 g orally every 8 h × 7 days | No | No | 2 |
| Patient N. | Surgery N. | Age (yrs) | Pathogenic Mutation | Surgery Type | Pre-Operative Factor Treatment | Post-Operative Factor Treatment | TA Use | Bleeding Episode | Hemostatic Treatment | Days of Hospitalization |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 47 | IVS-1 | Intra-articular administration of rifampicin | SHL-rFVIII 25 IU/kg | No | No | No | No | 0 |
| 1 | 2 | 47 | - | EGDS for hematemesis | SHL-rFVIII 60 IU/kg | No | 1 g orally every 8 h for 7 days | No | No | 5 |
| 1 | 3 | 47 | - | Dental extraction | No | No | 0.5 g every 8 h for 7 days (mouth wash) | No | No | 0 |
| 2 | 4 | 54 | p.Gly469Arg | Intra-articular administration of rifampicin | SHL-rFVIII 25 IU/kg | No | No | No | No | 0 |
| 2 | 5 | 54 | - | Dental extraction | No | No | 0.5 g every 8 h for 7 days (mouth wash) | Yes | SHL-rFVIII 25 IU/kg × 3 days | 0 |
| 3 | 6, 7, 8 | 63 | IVS22 | Dental extraction and implant (N.3) | SHL-rFVIII 50 IU/kg | No | 0.5 g every 8 h for 7 days (mouth wash) | No | No | 0 |
| 4 | 9 | 62 | EX14 ins 1 bp +A 1588-1590 | Dental extraction and implant | SHL-rFVIII 50 IU/kg | No | 0.5 g every 8 h for 7 days (mouth wash) | No | No | 0 |
| 5 | 10, 11 | 63 | p.Arg1689Cys + p.Asp1241Glu | Dental procedure (N.2) | No | No | No | No | No | 0 |
| 6 | 12, 13 | 56 | p.Leu308Arg | Dental procedure (N.2) | No | No | No | No | No | 0 |
| 7 | 14, 15 | 18 | IVS22 | Dental procedure (N.2) | No | No | No | No | No | 0 |
| 8 | 16, 17, 18 | 42 | IVS22 | Dental procedure (N.3) | No | No | No | No | No | 0 |
| 9 | 19, 20 | 60 | C.4379del p.Asn1460Ilefs*5 | Dental procedure (N.2) | No | No | No | No | No | 0 |
| 10 | 21, 22 | 57 | IVS22 | Dental procedure (N.2) | No | No | No | No | No | 0 |
| 11 | 23 | 52 | IVS22 | Colonscopy | SHL-rFVIII 30 IU/kg | No | No | No | No | 0 |
| 11 | 24 | 52 | - | EGDS with biopsy | SHL-rFVIII 45 IU/kg | No | 1 g orally every 12 h for 5 days | No | No | 0 |
| 11 | 25 | 52 | - | Cystoscopy | SHL-rFVIII 45 IU/kg | No | No | No | No | 0 |
| 12 | 26 | 39 | p.Arg2323Cys | Circumcision for phimosis | EHL-rFVIII 25 IU/kg | 25 IU/kg every 24 h × 1 day | 1 g orally every 8 h × 5 days | No | No | 0 |
| 13 | 27 | 65 | p.Asp222_Tyr2351delins13 | Cataract | No | No | No | No | No | 0 |
| 13 | 28 | 65 | - | Skin biopsy | SHL-rFVIII 50 IU/kg | No | No | No | No | 0 |
| 14 | 29 | 2 | p.Arg2182His | Port removal | SHL-rFVIII 50 IU/kg | No | No | No | No | 1 |
| 15 | 30 | 2 | IVS22 | Port removal | SHL-rFVIII 50 IU/kg | No | No | No | No | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castaman, G.; Linari, S.; Pieri, L.; Carulli, C.; Prosperi, P.; Tonelli, P.; Demartis, F.; Fjerza, R.; Attanasio, M.; Coppo, M.; et al. Safe and Successful Surgical Outcome in Persons with Hemophilia A with and without Inhibitors Treated with Emicizumab: A Large, Single Center, Real-World Experience. J. Clin. Med. 2023, 12, 2317. https://doi.org/10.3390/jcm12062317
Castaman G, Linari S, Pieri L, Carulli C, Prosperi P, Tonelli P, Demartis F, Fjerza R, Attanasio M, Coppo M, et al. Safe and Successful Surgical Outcome in Persons with Hemophilia A with and without Inhibitors Treated with Emicizumab: A Large, Single Center, Real-World Experience. Journal of Clinical Medicine. 2023; 12(6):2317. https://doi.org/10.3390/jcm12062317
Chicago/Turabian StyleCastaman, Giancarlo, Silvia Linari, Lisa Pieri, Christian Carulli, Paolo Prosperi, Paolo Tonelli, Francesco Demartis, Rajmonda Fjerza, Monica Attanasio, Mirella Coppo, and et al. 2023. "Safe and Successful Surgical Outcome in Persons with Hemophilia A with and without Inhibitors Treated with Emicizumab: A Large, Single Center, Real-World Experience" Journal of Clinical Medicine 12, no. 6: 2317. https://doi.org/10.3390/jcm12062317
APA StyleCastaman, G., Linari, S., Pieri, L., Carulli, C., Prosperi, P., Tonelli, P., Demartis, F., Fjerza, R., Attanasio, M., Coppo, M., & Salvianti, F. (2023). Safe and Successful Surgical Outcome in Persons with Hemophilia A with and without Inhibitors Treated with Emicizumab: A Large, Single Center, Real-World Experience. Journal of Clinical Medicine, 12(6), 2317. https://doi.org/10.3390/jcm12062317