
A Recovery-Oriented Program for People with Bipolar Disorder through Virtual Reality-Based Cognitive Remediation: Results of a Feasibility Randomized Clinical Trial
 , , , ,
, , , ,  , ,
, , 
Abstract
1. Background
2. Aims
2.1. Primary Aim
2.2. Secondary Aim
3. Methods
3.1. Study Design
3.2. Participants
3.3. Randomization
3.4. Blinding
3.5. Intervention
- ➢
- Reception, psychoeducation and orientation to the tool;
- ➢
- Exercise psychoeducation;
- ➢
- Psychoeducation to the function to be learned during the exercise;
- ➢
- Generalization phase, in which the function and its importance were explained in the participants’ life context (a bio-psycho-socio-cultural approach based on cognition);
- ➢
- Execution of the exercise in VR with positive and corrective feedback;
- ➢
- Post-exercise comment;
- ➢
- Second exercise that used the same method mentioned above (the maximum duration of the exposure to Virtual Reality was 15–20 min);
- ➢
- Final comment;
- ➢
- Homework, intended as practical suggestions to be implemented by the patients in their daily life. Sessions included an Attention and Working Memory exercise plus one Memory/Learning exercise or one Cognitive Estimation exercise. In some sessions, depending on the participant, the session, and the operator’s assessment, an extra exercise of any type could also be done.
3.6. Control
3.7. Outcomes
3.8. Data Collection
- -
- Rey Figure Test [72] for the visuospatial function,
- -
- -
- -
- -
- -
- -
- SF-12, Short Form Health Survey, 12 items [86], a self-administered questionnaire that investigates the following dimensions of quality of life and wellbeing: vitality, physical function, physical pain, perception of general health, mental health, physical and emotional health, work functioning and social role;
- -
- TAS-20, Toronto Alexithymia Scale-20 item [87], a self-administered questionnaire that evaluates the level of emotional awareness;
- -
- SAS, Zung Self-Rating Anxiety Scale [88], a self-administered questionnaire that evaluates perceived anxiety levels;
- -
- PHQ-9, Patient Health Questionnaire [89], a self-administered questionnaire that evaluates depressive symptoms;
- -
- HoNOS, Health of The Nation Outcome Scale [90], a clinical scale to evaluate general, personal and social functioning;
- -
- BRIAN, Biological Rhythms Interview of Assessment in Neuropsychiatry [91], a clinical interview consisting of 18 items that investigates four main areas related to the dysregulation of circadian rhythms (sleep, activity, social rhythms and nutrition).
3.9. Data Analyses
3.10. Sample Size Considerations
4. Results
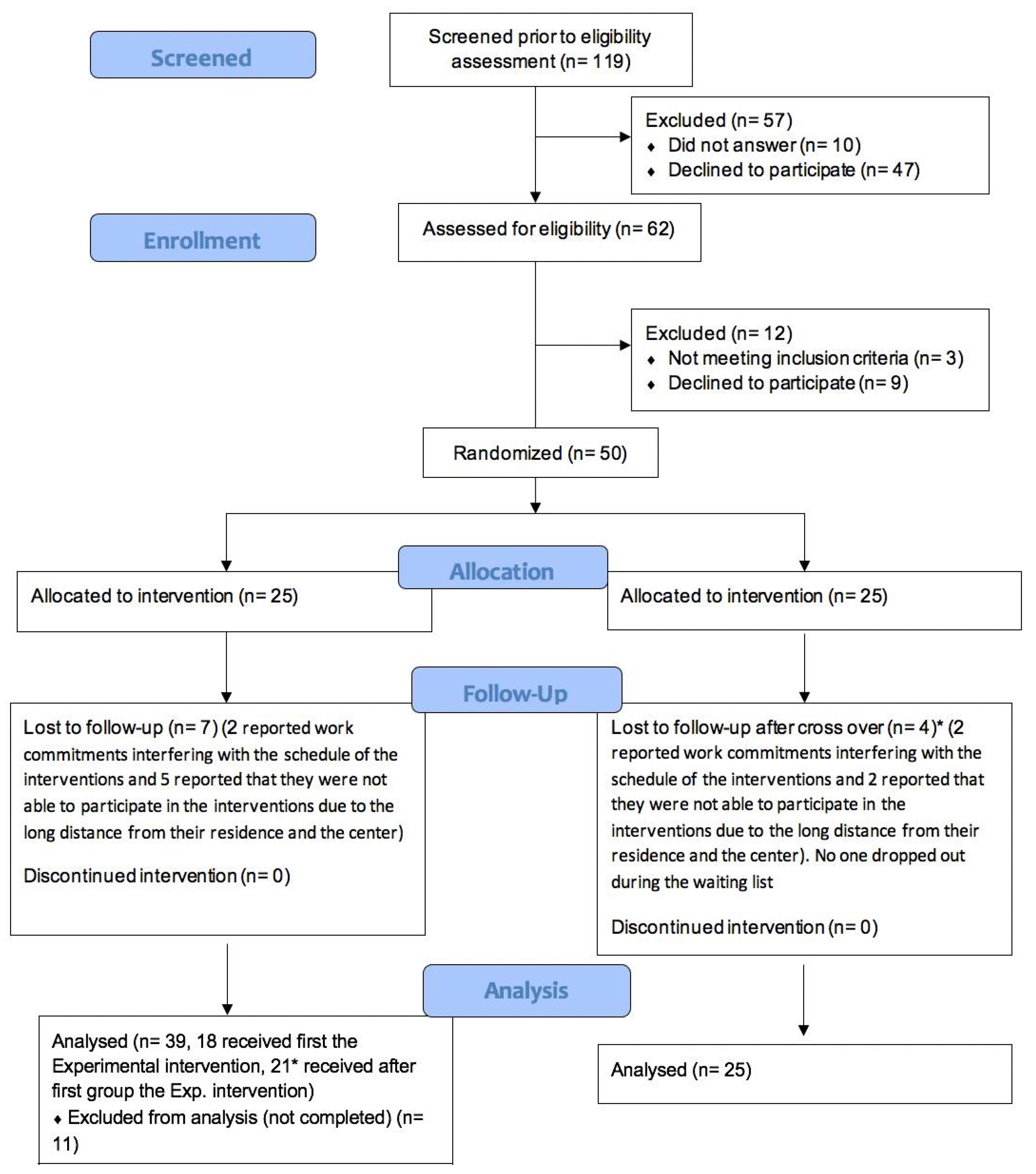
4.1. Primary Outcome: Feasibility of the Trial (Acceptability and Tolerability)
4.2. Secondary Outcome: Efficacy of the Trial (Satisfaction with the Trial; Adverse Effects; Cognitive Functions; Personal and Social Functioning)
5. Discussion
Risk and Benefits
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albanna, A.; Choudhry, Z.; Harvey, P.-O.; Fathalli, F.; Cassidy, C.; Sengupta, S.M.; Iyer, S.N.; Rho, A.; Lepage, M.; Malla, A.; et al. TCF4 gene polymorphism and cognitive performance in patients with first episode psychosis. Schizophr. Res. 2014, 152, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Thorsen, A.L.; Johansson, K.; Lã¸berg, E.-M. Neurobiology of Cognitive Remediation Therapy for Schizophrenia: A Systematic Review. Front. Psychiatry 2014, 5, 103. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhou, F.-C.; Zhang, L.; Ng, C.H.; Ungvari, G.S.; Li, J.; Xiang, Y.-T. Comparison of cognitive dysfunction between schizophrenia and bipolar disorder patients: A meta-analysis of comparative studies. J. Affect. Disord. 2020, 274, 652–661. [Google Scholar] [CrossRef]
- Goff, D.C.; Hill, M.; Barch, D. The treatment of cognitive impairment in schizophrenia. Pharmacol. Biochem. Behav. 2011, 99, 245–253. [Google Scholar] [CrossRef]
- Solé, B.; Jiménez, E.; Torrent, C.; Reinares, M.; Bonnin, C.; Torres, I.; Varo, C.; Grande, I.; Valls, E.; Salagre, E.; et al. Cognitive Impairment in Bipolar Dis-order: Treatment and Prevention Strategies. Int. J. Neuropsychopharmacol. 2017, 20, 670–680. [Google Scholar] [CrossRef]
- Carta, M.; Angst, J. Screening for bipolar disorders: A public health issue. J. Affect. Disord. 2016, 205, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Ouali, U.; Perra, A.; Ahmed, A.B.C.; Boe, L.; Aissa, A.; Lorrai, S.; Cossu, G.; Aresti, A.; Preti, A.; et al. Living With Bipolar Disorder in the Time of Covid-19: Biorhythms During the Severe Lockdown in Cagliari, Italy, and the Moderate Lockdown in Tunis, Tunisia. Front. Psychiatry 2021, 12, 634765. [Google Scholar] [CrossRef]
- Merikangas, K.R.; Jin, R.; He, J.-P.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and Correlates of Bipolar Spectrum Disorder in the World Mental Health Survey Initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef]
- Whiteford, H.A.; Degenhardt, L.; Rehm, J.; Baxter, A.J.; Ferrari, A.J.; Erskine, H.E.; Charlson, F.J.; Norman, R.E.; Flaxman, A.D.; Johns, N.; et al. Global burden of disease attributable to mental and substance use disorders: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 382, 1575–1586. [Google Scholar] [CrossRef]
- Martinez-Aran, A.; Vieta, E. Cognition as a target in schizophrenia, bipolar disorder and depres-sion. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2015, 25, 151–157. [Google Scholar] [CrossRef]
- Martínez-Arán, A.; Vieta, E.; Colom, F.; Reinares, M.; Benabarre, A.; Gastó, C.; Salamero, M. Cognitive Dysfunctions in Bipolar Disorder: Evidence of Neuropsychological Disturbances. Psychother. Psychosom. 1999, 69, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.; Gonçalves-Pereira, M.; Xavier, M.; Mukaetova-Ladinska, E.B. Affective disorders and risk of developing dementia: Systematic review. Br. J. Psychiatry 2013, 202, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Musat, E.M.; Marlinge, E.; Leroy, M.; Olié, E.; Magnin, E.; Lebert, F.; Gabelle, A.; Bennabi, D.; Blanc, F.; Paquet, C.; et al. Characteristics of Bipolar Patients with Cognitive Impairment of Suspected Neurodegenerative Origin: A Multicenter Cohort. J. Pers. Med. 2021, 11, 1183. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, M.M.; Gerraty, R.T. A meta-analytic investigation of neurocognitive deficits in bipolar illness: Profile and effects of clinical state. Neuropsychology 2009, 23, 551–562. [Google Scholar] [CrossRef]
- Torres, I.J.; DeFreitas, V.G.; DeFreitas, C.M.; Kauer-Sant’Anna, M.; Bond, D.J.; Honer, W.G.; Lam, R.W.; Yatham, L.N. Neurocognitive Functioning in Patients With Bipolar I Disorder Recently Recovered From a First Manic Episode. J. Clin. Psychiatry 2010, 71, 1234–1242. [Google Scholar] [CrossRef]
- Carvalho, A.F.; Bortolato, B.; Miskowiak, K.; Vieta, E.; Köhler, C. Cognitive dysfunction in bipolar disorder and schizophrenia: A systematic review of meta-analyses. Neuropsychiatr. Dis. Treat. 2015, 11, 3111–3125. [Google Scholar] [CrossRef] [PubMed]
- Douglas, K.M.; Gallagher, P.; Robinson, L.J.; Carter, J.D.; McIntosh, V.V.; Frampton, C.M.; Watson, S.; Young, A.H.; Ferrier, I.N.; Porter, R.J. Prevalence of cognitive impairment in major depression and bipolar disor-der. Bipolar Dis. 2018, 20, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Brissos, S.; Dias, V.V.; Kapczinski, F. Cognitive performance and quality of life in bipolar disor-der. Canadian journal of psychiatry. Revue Can. Psychiatr. 2008, 53, 517–524. [Google Scholar] [CrossRef]
- American Psychiatric Association. Practice guideline for the treatment of patients with bipolar disorder (revision). Am. J. Psychiatry 2002, 159, 1–50. [Google Scholar]
- Goodwin, G.; Haddad, P.; Ferrier, I.; Aronson, J.; Barnes, T.; Cipriani, A.; Coghill, D.R.; Fazel, S.; Geddes, J.; Grunze, H.; et al. Evidence-based guidelines for treating bipolar disorder: Revised third edition recommendations from the British Association for Psychopharmacology. J. Psychopharmacol. 2016, 30, 495–553. [Google Scholar] [CrossRef]
- Vieta, E. The influence of medications on neurocognition in bipolar disorder. Acta Psychiatr. Scand. 2009, 120, 414–415. [Google Scholar] [CrossRef] [PubMed]
- Steardo, L.; de Filippis, R.; Carbone, E.A.; Segura-Garcia, C.; Verkhratsky, A.; De Fazio, P. Sleep Disturbance in Bipolar Disorder: Neuroglia and Circadian Rhythms. Front. Psychiatry 2019, 10, 501. [Google Scholar] [CrossRef]
- Cullen, C.; Kappelmann, N.; Umer, M.; Abdolizadeh, A.; Husain, M.O.; Bonato, S.; Sharma, G.; Xue, S.; Ortiz, A.; Kloiber, S.M.; et al. Efficacy and acceptability of pharmacotherapy for comorbid anxiety symptoms in bipolar disorder: A systematic review and meta-analysis. Bipolar Disord. 2021, 23, 754–766. [Google Scholar] [CrossRef]
- Albert, U.; Rosso, G.; Maina, G.; Bogetto, F. Impact of anxiety disorder comorbidity on quality of life in euthymic bipolar disorder patients: Differences between bipolar I and II subtypes. J. Affect. Disord. 2008, 105, 297–303. [Google Scholar] [CrossRef]
- Assembly, U.G. Convention on the Rights of Persons with Disabilities. GA Res. 2006, 61, 106. [Google Scholar]
- Vita, A.; Barlati, S.; Ceraso, A.; Nibbio, G.; Ariu, C.; Deste, G.; Wykes, T. Effectiveness, Core Elements, and Moderators of Response of Cognitive Remediation for Schizophrenia: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Psychiatry 2021, 78, 848–858. [Google Scholar] [CrossRef]
- Thérond, A.; Pezzoli, P.; Abbas, M.; Howard, A.; Bowie, C.R.; Guimond, S. The Efficacy of Cognitive Remediation in Depression: A Systematic Literature Review and Meta-Analysis. J. Affect. Disord. 2021, 284, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Stubbs, B.; Rosenbaum, S.; Vancampfort, D.; Malchow, B.; Schuch, F.; Elliott, R.; Nuechterlein, K.H.; Yung, A.R. Aerobic Exercise Improves Cognitive Functioning in People With Schizophrenia: A Systematic Review and Meta-Analysis. Schizophr. Bull. 2016, 43, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Bottai, T.; Biloa-Tang, M.; Christophe, S.; Dupuy, C.; Jacquesy, L.; Kochman, F.; Meynard, J.-A.; Papeta, D.; Rahioui, H.; Adida, M.; et al. Thérapie interpersonnelle et aménagement des rythmes sociaux (TIPARS): Du concept anglo-saxon à l’expérience française. L’Encephale 2010, 36, S206–S217. [Google Scholar] [CrossRef]
- Sancassiani, F.; Lorrai, S.; Cossu, G.; Cocco, A.; Trincas, G.; Floris, F.; Mellino, G.; Machado, S.; Nardi, A.E.; Fabrici, E.P.; et al. The Effects of “VelaMente?!” Project on Social Functioning of People With Severe Psychosocial Disabilities. Clin. Pract. Epidemiol. Ment. Health 2017, 13, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Cossu, G.; Pintus, E.; Zaccheddu, R.; Callia, O.; Conti, G.; Pintus, M.; Gonzalez, C.I.A.; Massidda, M.V.; Mura, G.; et al. Moderate Exercise Improves Cognitive Function in Healthy Elderly People: Results of a Randomized Controlled Trial. Clin. Pract. Epidemiol. Ment. Health 2021, 17, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Cossu, G.; Pintus, E.; Zoccheddu, R.; Callia, O.; Conti, G.; Pintus, M.; Gonzalez, C.I.A.; Massidda, M.V.; Mura, G.; et al. Active elderly and health—Can moderate exercise improve health and wellbeing in older adults? Protocol for a randomized controlled trial. Trials 2021, 22, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Young, J.; Angevaren, M.; Rusted, J.; Tabet, N. Aerobic exercise to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst. Rev. 2015, 4, CD005381. [Google Scholar] [CrossRef] [PubMed]
- Cossu, G.; Gonzalez, C.I.A.; Minerba, L.; Demontis, R.; Pau, M.; Velluzzi, F.; Ferreli, C.; Atzori, L.; Machado, S.; Fortin, D.; et al. Exercise Improves Long-Term Social and Behavioral Rhythms in Older Adults: Did it Play a Role during the COVID-19 Lockdown? J. Public Health Res. 2022, 11, 2432. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Fornaro, M.; Minerba, L.; Pau, M.; Velluzzi, F.; Atzori, L.; Gonzalez, C.I.A.; Romano, F.; Littera, R.; Chessa, L.; et al. Previous Functional Social and Behavioral Rhythms Affect Resilience to Covid-19-Related Stress among Old Adults. J. Public Health Res. 2022, 11, 2768. [Google Scholar] [CrossRef] [PubMed]
- Wykes, T.; Spaulding, W.D. Thinking About the Future Cognitive Remediation Therapy--What Works and Could We Do Better? Schizophr. Bull. 2011, 37, S80–S90. [Google Scholar] [CrossRef] [PubMed]
- Elgamal, S.; McKINNON, M.C.; Ramakrishnan, K.; Joffe, R.T.; MacQUEEN, G. Successful computer-assisted cognitive remediation therapy in patients with unipolar depression: A proof of principle study. Psychol. Med. 2007, 37, 1229–1238. [Google Scholar] [CrossRef]
- Bellani, M.; Biagianti, B.; Zovetti, N.; Rossetti, M.G.; Bressi, C.; Perlini, C.; Brambilla, P. The effects of cognitive remediation on cognitive abilities and real-world functioning among people with bipolar disorder: A systematic review: Special Section on “Translational and Neuroscience Studies in Affective Disorders”. Section Editor, Maria Nobile MD, PhD. This Section of JAD focuses on the relevance of translational and neuroscience studies in providing a better understanding of the neural basis of affective disorders. The main aim is to briefly summaries relevant research findings in clinical neuroscience with particular regards to specific innovative topics in mood and anxiety disorders. J. Affect. Dis. 2019, 257, 691–697. [Google Scholar]
- Choi, J.; Medalia, A. Factors Associated With a Positive Response to Cognitive Remediation in a Community Psychiatric Sample. Psychiatr. Serv. 2005, 56, 602–604. [Google Scholar] [CrossRef]
- Tchanturia, K.; Davies, H.; Campbell, I.C. Cognitive remediation therapy for patients with anorexia nervosa: Preliminary findings. Ann. Gen. Psychiatry 2007, 6, 14. [Google Scholar] [CrossRef]
- Gold, A.K.; Montana, R.E.; Sylvia, L.G.; Nierenberg, A.A.; Deckersbach, T. Cognitive Remediation and Bias Modification Strategies in Mood and Anxiety Disorders. Curr. Behav. Neurosci. Rep. 2016, 3, 340–349. [Google Scholar] [CrossRef]
- Vita, A.; Deste, G.; Barlati, S.; Poli, R.; Cacciani, P.; De Peri, L.; Sacchetti, E. Feasibility and effectiveness of cognitive remediation in the treatment of borderline personality disorder. Neuropsychol. Rehabilitation 2016, 28, 416–428. [Google Scholar] [CrossRef] [PubMed]
- Cella, M.; Preti, A.; Edwards, C.; Dow, T.; Wykes, T. Cognitive remediation for negative symptoms of schizophrenia: A network meta-analysis. Clin. Psychol. Rev. 2017, 52, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Thapa, N.; Park, H.J.; Yang, J.-G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The Effect of a Virtual Reality-Based Intervention Program on Cognition in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef] [PubMed]
- Velligan, D.I.; Kern, R.S.; Gold, J.M. Cognitive Rehabilitation for Schizophrenia and the Putative Role of Motivation and Expectancies. Schizophr. Bull. 2005, 32, 474–485. [Google Scholar] [CrossRef]
- Ventura, J.; Subotnik, K.L.; Gretchen-Doorly, D.; Casaus, L.; Boucher, M.; Medalia, A.; Bell, M.D.; Hellemann, G.S.; Nuechterlein, K.H. Cognitive remediation can improve negative symptoms and social functioning in first-episode schizophrenia: A randomized controlled trial. Schizophr. Res. 2017, 203, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Tsapekos, D.; Seccomandi, B.; Mantingh, T.; Cella, M.; Wykes, T.; Young, A. Cognitive enhancement interventions for people with bipolar disorder: A systematic review of methodological quality, treatment approaches, and outcomes. Bipolar Disord. 2019, 22, 216–230. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. In Proceedings of the European Advisory Committee on Health Research: Fourth MeetingL World Health Organization, Copenhagen, Denmark, 10–11 December 2013; Regional Office for Europe: Geneva, Switzerland, 2014. [Google Scholar]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393–2400. [Google Scholar] [CrossRef] [PubMed]
- Park, M.J.; Kim, D.J.; Lee, U.; Na, E.J.; Jeon, H.J. A Literature Overview of Virtual Reality (VR) in Treatment of Psychiatric Disorders: Recent Advances and Limitations. Front. Psychiatry 2019, 10, 505. [Google Scholar] [CrossRef]
- Costa, M.; Vieira, L.P.; Barbosa, E.O.; Mendes Oliveira, L.; Maillot, P.; Otero Vaghetti, C.A.; Giovani Carta, M.; Machado, S.; Gatica-Rojas, V.; Monteiro-Junior, R.S. Virtual Reality-Based Exercise with Exergames as Medicine in Different Contexts: A Short Review. Clin. Pract. Epidemiol. Ment. Health CP EMH 2019, 15, 74. [Google Scholar] [CrossRef]
- Lima, J.L.; Axt, G.; Teixeira, D.S.; Monteiro, D.; Cid, L.; Yamamoto, T.; Murillo-Rodriguez, E.; Machado, S. Exergames for Children and Adolescents with Autism Spectrum Disorder: An Overview. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Robert, P.H.; König, A.; Amieva, H.; Andrieu, S.; Bremond, F.; Bullock, R.; Manera, V. Recommendations for the use of serious games in people with Alzheimer’s disease, related disorders and frailty Front. Aging Neurosci. 2014, 6, 54. [Google Scholar] [CrossRef]
- Manera, V.; Chapoulie, E.; Bourgeois, J.; Guerchouche, R.; David, R.; Ondrej, J.; Drettakis, G.; Robert, P. A Feasibility Study with Image-Based Rendered Virtual Reality in Patients with Mild Cognitive Impairment and Dementia. PLoS ONE 2016, 11, e0151487. [Google Scholar] [CrossRef]
- Liu, Y.; Tan, W.; Chen, C.; Liu, C.; Yang, J.; Zhang, Y. A Review of the Application of Virtual Reality Technology in the Diagnosis and Treatment of Cognitive Impairment. Front. Aging Neurosci. 2019, 11, 280. [Google Scholar] [CrossRef] [PubMed]
- Powers, M.B.; Emmelkamp, P.M. Virtual reality exposure therapy for anxiety disorders: A meta-analysis. J. Anxiety Disord. 2008, 22, 561–569. [Google Scholar] [CrossRef]
- Maples-Keller, J.L.; Bunnell, B.E.; Kim, S.-J.B.; Rothbaum, B.O. The Use of Virtual Reality Technology in the Treatment of Anxiety and Other Psychiatric Disorders. Harv. Rev. Psychiatry 2017, 25, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Norr, A.M.; Smolenski, D.J.; Reger, G.M. Effects of prolonged exposure and virtual reality exposure on suicidal ideation in active duty soldiers: An examination of potential mechanisms. J. Psychiatr. Res. 2018, 103, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Lasaponara, S.; Marson, F.; Doricchi, F.; Cavallo, M. A Scoping Review of Cognitive Training in Neurodegenerative Diseases via Computerized and Virtual Reality Tools: What We Know So Far. Brain Sci. 2021, 11, 528. [Google Scholar] [CrossRef]
- García-Betances, R.I.; Arredondo Waldmeyer, M.T.; Fico, G.; Cabrera-Umpierrez, M.F. A Succinct Overview of Virtual Reality Technology Use in Alzheimer’s Disease. Front. Aging Neurosci. 2015, 7, 80. [Google Scholar] [CrossRef]
- Zakzanis, K.K.; Quintin, G.; Graham, S.J.; Mraz, R. Age and dementia related differences in spatial navigation within an immersive virtual environment. Med. Sci. Monit. 2009, 15, CR140–CR150. [Google Scholar]
- Cotelli, M.; Manenti, R.; Brambilla, M.; Gobbi, E.; Ferrari, C.; Binetti, G.; Cappa, S.F. Cognitive telereha-bilitation in mild cognitive impairment, Alzheimer’s disease and frontotemporal dementia: A systematic re-view. J. Telemed. Telecare 2019, 25, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Perra, A.; De Lorenzo, V.; Zaccheddu, R.; Locci, A.; Piludu, F.; Preti, A.; Di Natale, L.; Galetti, A.; Nardi, A.E.; Cossu, G.; et al. Cognitive Remediation Virtual Reality Tool a Recovery-Oriented Project for People with Bipolar Disorder: Protocol of a Feasibility Randomized Clinical Trial. Clin. Pract. Epidemiol. Ment. Health 2022, 18, e174501792208220. [Google Scholar] [CrossRef]
- Jahn, F.S.; Skovbye, M.; Obenhausen, K.; Jespersen, A.E.; Miskowiak, K.W. Cognitive training with fully immersive virtual reality in patients with neurological and psychiatric disorders: A systematic review of randomized controlled trials. Psychiatry Res. 2021, 300, 113928. [Google Scholar] [CrossRef]
- Riva, G.; Mancuso, V.; Cavedoni, S.; Stramba-Badiale, C. Virtual reality in neurorehabilitation: A review of its effects on multiple cognitive domains. Expert Rev. Med. Devices 2020, 17, 1035–1061. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; McDonough, D.J.; Gao, Z. The Effectiveness of Virtual Reality Exercise on Individual’s Physiological, Psychological and Rehabilitative Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4133. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster GA PAFS Consensus Group. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Shaigetz, V.G.; Proulx, C.; Cabral, A.; Choudhury, N.; Hewko, M.; Kohlenberg, E.; Segado, M.; Smith, M.S.D.; Debergue, P. An Immersive and Interactive Platform for Cognitive Assessment and Rehabilitation (bWell): Design and Iterative Development Process. JMIR Rehabilitation Assist. Technol. 2021, 8, e26629. [Google Scholar] [CrossRef]
- Saxena, S.; Funk, M.; Chisholm, D. World Health Assembly adopts Comprehensive Mental Health Action Plan 2013–2020. Lancet 2013, 381, 1970–1971. [Google Scholar] [CrossRef]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. Rey-Osterrieth complex figure: Normative values in an Italian population sample. Neurol. Sci. 2002, 22, 443–447. [Google Scholar] [CrossRef]
- Spinnler, H.; Tognoni, G. Standardizzazione e taratura italiana di test neuropsicologici. Ital. J. Neurol. Sci. 1987, 8, 21–120. [Google Scholar]
- Caltagirone, C.; Gainotti, G.; Carlesimo, G.A.; Parnetti, L. Batteria per la valutazione del deterioramento mentale: I/II. Descrizione di uno strumento di diagnosi neuropsicologica. Arch. Psicol. Neurol. Psichiatria 1995, 14, 109–138. [Google Scholar]
- Carlesimo, G.A.; Buccione, I.; Fadda, L.; Graceffa, A.; Mauri, M.; Lorusso, S.; Caltagirone, C. Standardizzazione di due test di memoria per uso clinico: Breve Racconto e Figura di Rey. Nuova Riv. Neurol. 2002, 12, 1–13. [Google Scholar]
- Orsini, A.; Grossi, D.; Capitani, E.; Laiacona, M.; Papagno, C.; Vallar, G. Verbal and spatial immediate memory span: Normative data from 1355 adults and 1112 children. Neurol. Sci. 1987, 8, 537–548. [Google Scholar] [CrossRef]
- Bisiacchi, P.S.; Mapelli, D.; Mondini, S.; Vestri, A. Esame Neuropsicologico Breve, una Batteria di Test per lo Screening Neuropsicologico; Raffaello Cortina Editore: Milano, Italy, 2003. [Google Scholar]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail making test: Normative values from 287 normal adult controls. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef]
- Novelli, G.; Papagno, C.; Capitani, E.; Laiacona, M. Tre test clinici di ricerca e produzione lessicale. Taratura su sogetti normali. Arch. Psicol. Neurol. Psichiatria 1986, 47, 477–506. [Google Scholar]
- Amodio, P.; Wenin, H.; Del Piccolo, F.; Mapelli, D.; Montagnese, S.; Pellegrini, A.; Umiltà, C. Variability of trail making test, symbol digit test and line trait test in normal people. A normative study taking into account age-dependent decline and sociobiological variables. Aging Clin. Exp. Res. 2002, 14, 117–131. [Google Scholar] [CrossRef]
- Amodio, P.; Campagna, F.; Olianas, S.; Iannizzi, P.; Mapelli, D.; Penzo, M.; Angeli, P.; Gatta, A. Detection of minimal hepatic encephalopathy: Normalization and optimization of the Psychometric Hepatic Encephalopathy Score. A neuropsychological and quantified EEG study. J. Hepatol. 2008, 49, 346–353. [Google Scholar] [CrossRef]
- Caffarra, P.; Vezzadini, G.; Dieci, F.; Zonato, F.; Venneri, A. Una versione abbreviata del test di Stroop: Dati normativi nella popolazione italiana. Nuova Riv. Neurol. 2002, 12, 111–115. [Google Scholar]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B.F.A.B. The FAB: A frontal assessment battery at bed-side. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef]
- Scarpina, F.; D’Aniello, G.E.; Mauro, A.; Castelnuovo, G.; MacPherson, S.E. How many segments are there in an orange: Normative data for the new Cognitive Estimation Task in an Italian population. Neurol. Sci. 2015, 36, 1889–1895. [Google Scholar] [CrossRef] [PubMed]
- Della Sala, S.; MacPherson, S.E.; Phillips, L.; Sacco, L.; Spinnler, H. How many camels are there in Italy? Cognitive estimates standardised on the Italian population. Neurol. Sci. 2003, 24, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Bagby, R.M.; Parker, J.D.A.; Taylor, G.J. The twenty-item Toronto Alexithymia scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Zung, W.W. A rating instrument for anxiety disorders. Psychosom. J. Consult. Liaison Psychiatry 1971, 12, 371–379. [Google Scholar] [CrossRef]
- Rizzo, R.; Piccinelli, M.; Mazzi, M.A.; Bellantuono, C.; Tansella, M. The Personal Health Questionnaire: A new screening instrument for detection of ICD-10 depressive disorders in primary care. Psychol. Med. 2000, 30, 831–840. [Google Scholar] [CrossRef]
- Wing, J.K.; Curtis, R.; Beevor, A. Health of the Nation Outcome Scales; Royal College of Psychiatrists: London, UK, 1996. [Google Scholar]
- Moro, M.F.; Carta, M.G.; Pintus, M.; Pintus, E.; Melis, R.; Kapczinski, F.; Colom, F. Validation of the Italian Version of the Biological Rhythms Interview of Assessment in Neuropsychiatry (BRIAN): Some Considerations on its Screening Usefulness. Clin. Pract. Epidemiol. Ment. Health 2014, 10, 48–52. [Google Scholar] [CrossRef]
- Ott, C.V.; Macoveanu, J.; Bowie, C.R.; Fisher, P.M.; Knudsen, G.M.; Kessing, L.V.; Miskowiak, K.W. Change in prefrontal activity and executive functions after action-based cognitive remediation in bipolar disorder: A randomized controlled trial. Neuropsychopharmacology 2020, 46, 1113–1121. [Google Scholar] [CrossRef]
- Abdulatif, M.; Mukhtar, A.; Obayah, G. Pitfalls in reporting sample size calculation in randomized controlled trials published in leading anaesthesia journals: A systematic review. Br. J. Anaesth. 2015, 115, 699–707. [Google Scholar] [CrossRef]
- Wright, I.; Mughal, F.; Bowers, G.; Meiser-Stedman, R. Dropout from randomised controlled trials of psychological treatments for depression in children and youth: A systematic review and meta-analyses. J. Affect. Disord. 2020, 281, 880–890. [Google Scholar] [CrossRef]
- Amico, K.R. Percent Total Attrition: A Poor Metric for Study Rigor in Hosted Intervention Designs. Am. J. Public Health 2009, 99, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, V.; Fallowfield, L. Reasons for accepting or declining to participate in randomized clinical trials for cancer therapy. Br. J. Cancer 2000, 82, 1783–1788. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Perra, A.; Atzeni, M.; D’Oca, S.; Moro, M.F.; Kurotschka, P.K.; Moro, D.; Sancassiani, F.; Minerba, L.; Brasesco, M.V.; et al. An evolutionary approach to mania studying Sardinian immigrants to Argentina. Rev. Bras. Psiquiatr. 2017, 39, 147–153. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Comprehensive Mental Health Action Plan 2013–2030; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Garcia-Palacios, A.; Hoffman, H.; Carlin, A.; Furness, T.; Botella, C. Virtual reality in the treatment of spider phobia: A controlled study. Behav. Res. Ther. 2002, 40, 983–993. [Google Scholar] [CrossRef]
- Klinger, E.; Bouchard, S.; Légeron, P.; Roy, S.; Lauer, F.; Chemin, I.; Nugues, P. Virtual Reality Therapy Versus Cognitive Behavior Therapy for Social Phobia: A Preliminary Controlled Study. CyberPsychol. Behav. 2005, 8, 76–88. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Gazzetta Ufficiale della Repubblica Italiana. Decreto Legislativo 30 Giugno; Gazzetta Ufficiale della Repubblica Italiana: Roma, Italy, 2003; p. 196. [Google Scholar]
- European Union. Regolamento (UE) 2016/679 del Parlamento Europeo e del Consiglio; del 27 Aprile 2016, Relativo Alla Protezione Delle Persone Fisiche Con Riguardo al Trattamento Dei Dati Personali, Nonché Alla Libera Circolazione di Tali Dati e Che Abroga la Direttiva 95/46/CE (regolamento generale sulla protezione dei dati); European Union Regulation: Bruxelles, Belgium, 2016. [Google Scholar]


{kind=link}
| GROUP EXP CONTR | ||||
|---|---|---|---|---|
| EXP | CONTR | TOT | ||
| SEX | F N (%) | 32 (64) | 18 (72) | 50 (66.7) |
| M N (%) | 18 (36) | 7 (28) | 25 (33.3) | |
| Chi-Square | 0.480 | |||
| Sig. | 0.606 | |||
| AGE | N | 50 | 25 | 75 |
| Mean ± SD | 47.76 ± 13.34 | 46.16 ± 13.63 | 47.23 ± 13.37 | |
| F | 0.236 | |||
| Sig. | 0.628 | |||
| Levels | Counts | % of Total | Cumulative % |
|---|---|---|---|
| 3 Good | 9 | 23.1% | 23.1% |
| 4 Great | 11 | 28.2% | 51.3% |
| 5 Excellent | 19 | 48.7% | 100.0% |
| Levels | Counts | % of Total | Cumulative % |
|---|---|---|---|
| NO | 30 | 76.9% | 76.9% |
| Feeling of Emptiness-Disorientation | 1 | 2.6% | 79.5% |
| Nausea, Feeling of Emptiness | 1 | 2.6% | 82.1% |
| Headache | 1 | 2.6% | 84.6% |
| Disorientation | 1 | 2.6% | 87.2% |
| Dizziness | 1 | 2.6% | 89.7% |
| Tremors, Nausea, Blurred Vision, Dizziness | 1 | 2.6% | 92.3% |
| Dizziness | 1 | 2.6% | 94.9% |
| Vertigo | 1 | 2.6% | 97.4% |
| Sense of Unreality | 1 | 2.6% | 100.0% |
| Levels | Counts | % of Total | Cumulative % | |
|---|---|---|---|---|
| NO | 34 | 87.2% | 87.2% | |
| Nausea | 2 | 5.1% | 92.3% | |
| Daze | 2 | 5.1% | 97.4% | |
| Feeling of Emptiness | Unreality | 1 | 2.6% | 100.0% |
| OUTCOMES ° | VR/CR GROUP (N = 39) | CONTROL GROUP (N = 25) | p | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Time | Group | Time × Group | |
| Figure Rey Immediate (Vis.Sp.) | 28.74 ± 8.43 | 30.92 ± 6.68 | 28.16 ± 10.20 | 28.12 ± 8.65 | 0.002 | 0.168 | 0.588 |
| Matrix (Attent.) | 1.95 ± 1.38 | 2.38 ± 1.46 | 2.52 ± 1.53 | 2.16± 1.34 | 0.755 | 0.617 | 0.002 |
| Digit Span Forward (Attent.) | 2.77 ± 1.53 | 2.74 ± 1.48 | 2.84 ± 1.62 | 2.88 ± 1.48 | 0.968 | 0.765 | 0.853 |
| Rey’s Words Immediate (Attent.) | 2.33 ± 1.57 | 2.95 ± 1.52 | 2.52 ± 1.55 | 1.40 ± 1.56 | 0.109 | 0.627 | 0.019 |
| TMT-A (Attent.) | 2.87 ± 1.28 | 3.03 ± 1.42 | 2.64 ± 1.44 | 2.96 ± 1.17 | 0.075 | 0.527 | 0.527 |
| Ray’s Words Delayed (Memory) | 2.15 ± 1.31 | 2.77 ± 1.54 | 2.68 ± 1.31 | 2.20 ± 1.58 | 0.707 | 0.950 | 0.003 |
| Digit Span Backward (Memory) | 1.92 ± 1.62 | 2.23 ± 1.64 | 1.84 ± 1.70 | 2.36 ± 1.68 | 0.033 | 0.952 | 0.579 |
| Test Of Tale (Memory) | 2.13 ± 1.39 | 2.72 ± 1.14 | 1.84 ± 1.34 | 2.28 ± 1.34 | 0.005 | 0.204 | 0.675 |
| Verbal Phonological Test (Leng.) | 2.64 ± 1.47 | 3.08 ± 1.26 | 2.64 ± 1.57 | 2.84 ± 1.31 | 0.006 | 0.729 | 0.297 |
| Verbal Semantic Test (Leng.) | 2.62 ± 1.35 | 3.23 ± 1.13 | 2.72 ± 1.51 | 2.72 ± 1.37 | 0.010 | 0.527 | 0.010 |
| Substit. Digit Symbol (Ex. Fun.) | 36.36 ± 14.67 | 39.04 ± 12.11 | 37.75 ± 12.19 | 39.04 ± 12.92 | 0.302 | 0.743 | 0.815 |
| TMT-B (Ex. Fun.) | 2.90 ± 1.35 | 3.05 ± 1.19 | 2.56 ± 1.32 | 2.80 ± 1.38 | 0.103 | 0.350 | 0.719 |
| Stroop Test Time (Ex. Fun.) | 2.62 ± 1.54 | 3.03 ± 1.42 | 2.40 ± 1.68 | 2.44 ± 1.55 | 0.204 | 0.262 | 0.296 |
| FAB (Ex. Fun.) | 15.08 ± 3.12 | 15.72 ± 2.60 | 14.64 ± 2.92 | 15.08 ± 3.61 | 0.033 | 0.47 | 0.686 |
| Cog. Estimation Test (Ex. Fun.) | 1.95 ± 1.46 | 2.77 ± 1.15 | 2.60 ± 1.19 | 2.16 ± 1.46 | 0.346 | 0.939 | 0.003 |
| OUTCOMES ° | VR/CR GROUP (N = 39) | CONTROL GROUP (N = 25) | p | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Time | Group | Time × Group | |
| TAS-20 | 55.00 ± 14.747 | 49.85 ± 14.982 | 52.08 ± 14.821 | 55.76 ± 16.465 | 0.641 | 0.675 | 0.007 |
| BRIAN | 49.82 ± 12.380 | 47.23 ± 11.773 | 48.12 ± 12.551 | 50.24 ± 12.387 | 0.824 | 0.825 | 0.029 |
| PHQ-9 | 13.72 ± 6.121 | 10.82 ± 6.456 | 12.20 ± 6.265 | 11.92 ± 7.455 | 0.009 | 0.894 | 0.030 |
| SF-12 | 25.95 ± 8.448 | 28.62 ± 9.193 | 28.08 ± 7.129 | 28.48 ± 8.842 | 0.255 | 0.566 | 0.399 |
| SAS | 61.05 ± 17.220 | 53.64 ± 17.609 | 56.92 ± 15.689 | 57.96 ± 16.900 | 0.236 | 0.978 | 0.117 |
| HONOS | 9.67 ± 6.417 | 7.38 ± 6.364 | 10.48 ± 6.771 | 8.12 ± 6.579 | 0.006 | 0.595 | 0.962 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perra, A.; Galetti, A.; Zaccheddu, R.; Locci, A.; Piludu, F.; Preti, A.; Primavera, D.; Di Natale, L.; Nardi, A.E.; Kurotshka, P.K.; et al. A Recovery-Oriented Program for People with Bipolar Disorder through Virtual Reality-Based Cognitive Remediation: Results of a Feasibility Randomized Clinical Trial. J. Clin. Med. 2023, 12, 2142. https://doi.org/10.3390/jcm12062142
Perra A, Galetti A, Zaccheddu R, Locci A, Piludu F, Preti A, Primavera D, Di Natale L, Nardi AE, Kurotshka PK, et al. A Recovery-Oriented Program for People with Bipolar Disorder through Virtual Reality-Based Cognitive Remediation: Results of a Feasibility Randomized Clinical Trial. Journal of Clinical Medicine. 2023; 12(6):2142. https://doi.org/10.3390/jcm12062142
Chicago/Turabian StylePerra, Alessandra, Alessia Galetti, Rosanna Zaccheddu, Aurora Locci, Federica Piludu, Antonio Preti, Diego Primavera, Lorenzo Di Natale, Antonio Egidio Nardi, Peter Konstantin Kurotshka, and et al. 2023. "A Recovery-Oriented Program for People with Bipolar Disorder through Virtual Reality-Based Cognitive Remediation: Results of a Feasibility Randomized Clinical Trial" Journal of Clinical Medicine 12, no. 6: 2142. https://doi.org/10.3390/jcm12062142
APA StylePerra, A., Galetti, A., Zaccheddu, R., Locci, A., Piludu, F., Preti, A., Primavera, D., Di Natale, L., Nardi, A. E., Kurotshka, P. K., Cossu, G., Sancassiani, F., Stella, G., De Lorenzo, V., Zreik, T., & Carta, M. G. (2023). A Recovery-Oriented Program for People with Bipolar Disorder through Virtual Reality-Based Cognitive Remediation: Results of a Feasibility Randomized Clinical Trial. Journal of Clinical Medicine, 12(6), 2142. https://doi.org/10.3390/jcm12062142