
“What Did I Tell This Sad Person?”: Memory for Emotional Destinations in Korsakoff’s Syndrome



Abstract
1. Introduction
2. Method
Participants
3. Procedures
3.1. Cognitive Evaluation
3.2. Destination Memory
4. Materials
5. Assessment
6. Results
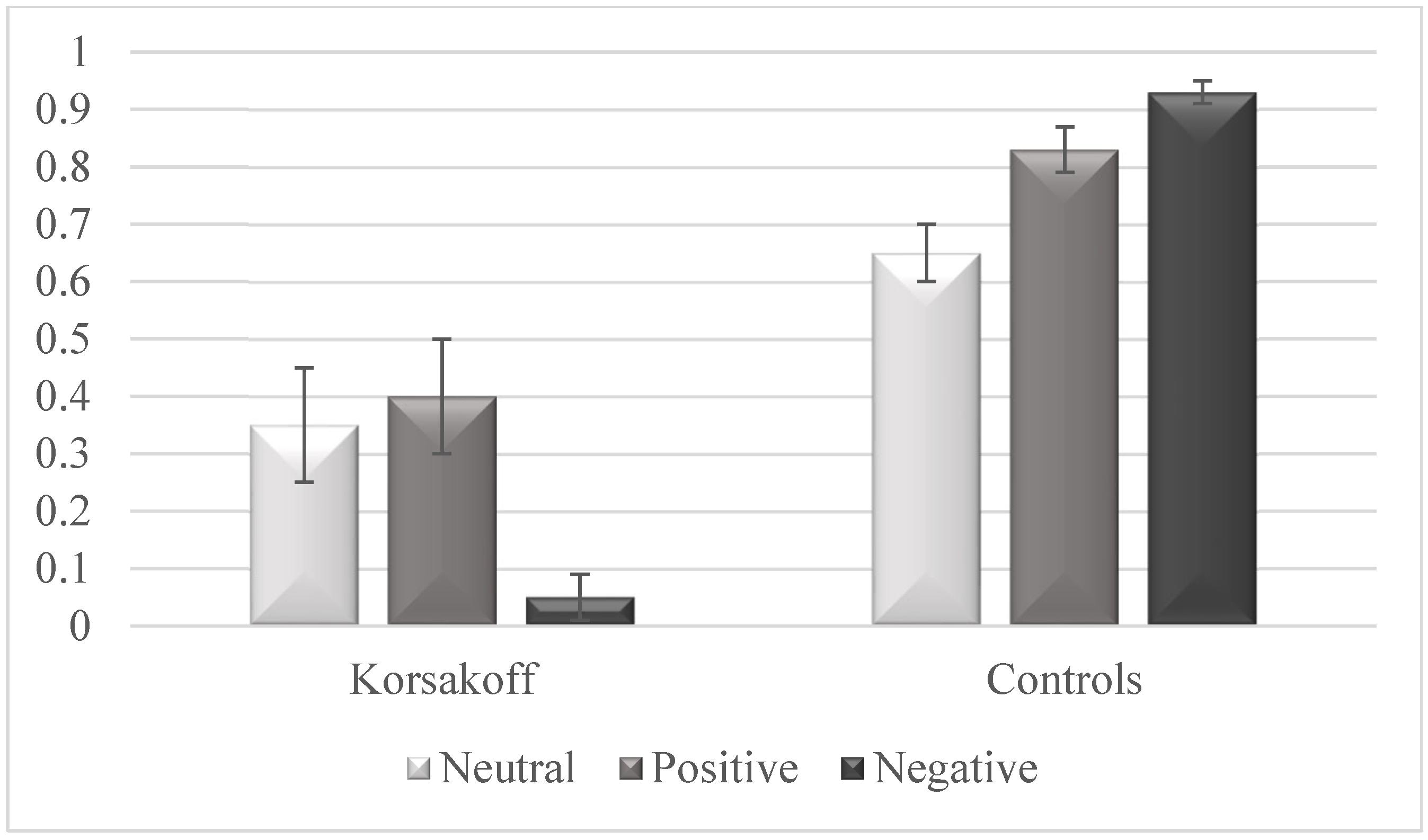
Low Memory for Destination Information in KS
7. Complementary Analysis
8. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kessels, R.P.; Kopelman, M.D. Context memory in Korsakoff’s syndrome. Neuropsychol. Rev. 2012, 22, 117–131. [Google Scholar] [CrossRef]
- Arts, N.J.M.; Walvoort, S.J.W.; Kessels, R.P.C. Korsakoff’s syndrome: A critical review. Neuropsychiatr. Dis. Treat. 2017, 13, 2875–2890. [Google Scholar] [CrossRef]
- El Haj, M.; Miller, R. Destination memory: The relationship between memory and social cognition. Psychol. Res. 2018, 82, 1027–1038. [Google Scholar] [CrossRef]
- El Haj, M.; Miller, R. The communicative function of destination memory. Behav. Brain. Sci. 2018, 41, e12. [Google Scholar] [CrossRef]
- El Haj, M. Destination memory: Memory associated with social interactions. Frontiers 2023, 13, 1061275. [Google Scholar] [CrossRef]
- Wilu Wilu, A.; Allain, P.; El Haj, M. T’ai-je déjà raconté cette histoire?: Troubles de la mémoire de la destination dans les pathologies neurologiques et psychiatriques. Did I tell you about that story?: Decline of destination memory in neurological and psychiatric disorders. Rev. Neuropsychol. 2018, 10, 130–138. [Google Scholar] [CrossRef]
- Koriat, A.; Ben-Zur, H.; Sheffer, D. Telling the same story twice: Output monitoring and age. J. Mem. Lang. 1988, 27, 23–39. [Google Scholar] [CrossRef]
- Koriat, A.; Ben-Zur, H.; Druch, A. The contextualization of input and output events in memory. Psychol. Res. 1991, 53, 260–270. [Google Scholar] [CrossRef]
- El Haj, M.; Kessels, R.P.C. Context Memory in Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. EXTRA 2013, 3, 342–350. [Google Scholar] [CrossRef]
- El Haj, M.; Allain, P.; Kessels, R.P. The cognitive and neuroanatomical underpinnings of destination memory. Transl. Neurosci. 2014, 5, 147–151. [Google Scholar]
- El Haj, M.; Moroni, C.; Luyat, M.; Omigie, D.; Allain, P. To what extent does destination recall induce episodic reliving? Evidence from Alzheimer’s disease. J. Clin. Exp. Neuropsychol. 2014, 36, 127–136. [Google Scholar] [CrossRef]
- El Haj, M.; Caillaud, M.; Verny, C.; Fasotti, L.; Allain, P. Destination and source memory in Huntington’s disease. J. Neuropsychol. 2016, 10, 77–89. [Google Scholar] [CrossRef]
- El Haj, M.; Allain, P. Role of context recall in destination memory decline in normal aging. Geriatr. Psychol. Neuropsych. Vieillissement 2014, 12, 432–439. [Google Scholar] [CrossRef]
- Wili Wilu, A.; Coello, Y.; El Haj, M. Destination memory in traumatic brain injuries. Neurol. Sci. 2018, 39, 1035–1040. [Google Scholar] [CrossRef]
- El Haj, M.; Altman, R.; Bortolon, C.; Capdevielle, D.; Raffard, S. Destination memory in schizophrenia: “Did I told Elvis Presley about the thief?”. Psychiatry. Res. 2017, 248, 71–76. [Google Scholar] [CrossRef]
- El Haj, M.; Fasotti, L.; Allain, P. Destination memory for emotional information in older adults. Exp. Aging. Res. 2015, 41, 204–219. [Google Scholar] [CrossRef]
- El Haj, M.; Raffard, S.; Antoine, P.; Gely-Nargeot, M.C. Emotion and Destination Memory in Alzheimer’s Disease. Curr. Alzheimer. Res. 2015, 12, 796–801. [Google Scholar] [CrossRef]
- Adolphs, R.; Cahill, L.; Schul, R.; Babinsky, R. Impaired declarative memory for emotional material following bilateral amygdala damage in humans. Learn. Mem. 1997, 4, 291–300. [Google Scholar] [CrossRef]
- Kensinger, E.A. How emotion affects older adults’ memories for event details. Memory 2009, 17, 208–219. [Google Scholar] [CrossRef]
- Galton, C.J.; Patterson, K.; Graham, K.; Lambon-Ralph, M.A.; Williams, G.; Antoun, N.; Sahakian, B.J.; Hodges, J.R. Differing patterns of temporal atrophy in Alzheimer’s disease and semantic dementia. Neurology 2001, 57, 216–225. [Google Scholar] [CrossRef]
- El Haj, M.; Kessels, R.P.; Matton, C.; Bacquet, J.E.; Urso, L.; Cool, G.; Guidez, F.; Potier, S.; Nandrino, J.L.; Antoine, P. Destination Memory in Korsakoff’s Syndrome. Alcohol. Clin. Exp. Res. 2016, 40, 1321–1327. [Google Scholar] [CrossRef]
- Kopelman, M.D. Remote and autobiographical memory, temporal context memory and frontal atrophy in Korsakoff and Alzheimer patients. Neuropsychologia 1989, 27, 437–460. [Google Scholar] [CrossRef]
- Fama, R.; Pitel, A.L.; Sullivan, E.V. Anterograde episodic memory in Korsakoff syndrome. Neuropsychol. Rev. 2012, 22, 93–104. [Google Scholar] [CrossRef]
- Pitel, A.L.; Beaunieux, H.; Witkowski, T.; Vabret, F.; de la Sayette, V.; Viader, F.; Desgranges, B.; Eustache, F. Episodic and working memory deficits in alcoholic Korsakoff patients: The continuity theory revisited. Alcohol. Clin. Exp. Res. 2008, 32, 1229–1241. [Google Scholar] [CrossRef]
- Oosterman, J.M.; de Goede, M.; Wester, A.J.; van Zandvoort, M.J.; Kessels, R.P. Perspective taking in Korsakoff’s syndrome: The role of executive functioning and task complexity. Acta. Neuropsychiatr. 2011, 23, 302–308. [Google Scholar] [CrossRef]
- Labudda, K.; Todorovski, S.; Markowitsch, H.J.; Brand, M. Judgment and memory performance for emotional stimuli in patients with alcoholic Korsakoff syndrome. J. Clin. Exp. Neuropsychol. 2008, 30, 224–235. [Google Scholar] [CrossRef]
- Brion, M.; de Timary, P.; de Wilmars, S.M.; Maurage, P. Impaired affective prosody decoding in severe alcohol use disorder and Korsakoff syndrome. Psychiatry Res. 2018, 264, 404–406. [Google Scholar] [CrossRef]
- Oscar-Berman, M.; Hancock, M.; Mildworf, B.; Hutner, N.; Weber, D.A. Emotional perception and memory in alcoholism and aging. Alcohol. Clin. Exp. Res. 1990, 14, 383–393. [Google Scholar] [CrossRef]
- Montagne, B.; Kessels, R.P.; Wester, A.J.; de Haan, E.H. Processing of emotional facial expressions in Korsakoff’s syndrome. Cortex 2006, 42, 705–710. [Google Scholar] [CrossRef]
- Drost, R.; Postma, A.; Oudman, E. Cognitive and affective theory of mind in Korsakoff’s syndrome. Acta Neuropsychiatr. 2019, 31, 128–134. [Google Scholar] [CrossRef]
- APA. Diagnostic and Statistical Manual of Mental Disorder, 5th ed.; DSM-5; APA: Washington, DC, USA, 2013. [Google Scholar]
- Oslin, D.; Atkinson, R.M.; Smith, D.M.; Hendrie, H. Alcohol related dementia: Proposed clinical criteria. Int. J. Geriatr. Psychiatry. 1998, 13, 203–212. [Google Scholar] [CrossRef]
- Grober, E.; Buschke, H. Genuine memory deficits in dementia. Dev. Neuropsychol. 1987, 3, 13–36. [Google Scholar] [CrossRef]
- Baddeley, A. Working memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Gopie, N.; Craik, F.I.; Hasher, L. Destination memory impairment in older people. Psychol. Aging 2010, 25, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Gopie, N.; Macleod, C.M. Destination memory: Stop me if I’ve told you this before. Psychol. Sci. 2009, 20, 1492–1499. [Google Scholar] [CrossRef] [PubMed]
- El Haj, M.; Raffard, S.; Gely-Nargeot, M.C. Destination memory and cognitive theory of mind in normal ageing. Memory 2016, 24, 526–534. [Google Scholar] [CrossRef] [PubMed]
- El Haj, M. Destination memory for self-generated actions. Aging Clin. Exp. Res. 2016, 28, 935–941. [Google Scholar] [CrossRef]
- Ebner, N.C.; Riediger, M.; Lindenberger, U. FACES—A database of facial expressions in young, middle-aged, and older women and men: Development and validation. Behav. Res. Methods 2010, 42, 351–362. [Google Scholar] [CrossRef]
- Herlitz, A.; Reuterskiold, L.; Loven, J.; Thilers, P.P.; Rehnman, J. Cognitive sex differences are not magnified as a function of age, sex hormones, or puberty development during early adolescence. Dev. Neuropsychol. 2013, 38, 167–179. [Google Scholar] [CrossRef]
- He, Y.; Ebner, N.C.; Johnson, M.K. What predicts the own-age bias in face recognition memory? Soc. Cogn. 2011, 29, 97–109. [Google Scholar] [CrossRef]
- Kuefner, D.; Macchi Cassia, V.; Picozzi, M.; Bricolo, E. Do all kids look alike? Evidence for an other-age effect in adults. J. Exp. Psychol. Hum. Percept. Perform. 2008, 34, 811–817. [Google Scholar] [CrossRef]
- Bortolon, C.; Louche, A.; Gely-Nargeot, M.C.; Raffard, S. Do patients suffering from Alzheimer’s disease present an own-age bias in face recognition? Exp. Gerontol. 2015, 70, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, M.G.; Anastasi, J.S. The own-age bias in face recognition: A meta-analytic and theoretical review. Psychol. Bull. 2012, 138, 146–174. [Google Scholar] [CrossRef] [PubMed]
- Anastasi, J.S.; Rhodes, M.G. Evidence for an Own-Age Bias in Face Recognition. N. Am. J. Psychol. 2006, 8, 237–252. [Google Scholar]
- Anastasi, J.S.; Rhodes, M.G. An own-age bias in face recognition for children and older adults. Psychon. Bull. Rev. 2005, 12, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- El Haj, M.; Raffard, S.; Fasotti, L.; Allain, P. Destination memory in social interaction: Better memory for older than for younger destinations in normal aging? Memory 2018, 26, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Snodgrass, J.G.; Corwin, J. Pragmatics of measuring recognition memory: Applications to dementia and amnesia. J. Exp. Psychol. Gen. 1988, 117, 34–50. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Rosenthal, R.; DiMatteo, M.R. Meta-analysis: Recent developments in quantitative methods for literature reviews. Ann. Rev. Psychol. 2001, 52, 59–82. [Google Scholar] [CrossRef]
- Ellis, P.D. The Essential Guide to Effect Sizes: Statistical Power, Meta-Analysis, and the Interpretation of Research Results; Cambridge University Press: New York, NY, USA, 2010. [Google Scholar]
- Kovner, R.; Dopkins, S.; Goldmeier, E. Effects of instructional set on amnesic recognition memory performance. Cortex 1988, 24, 477–483. [Google Scholar] [CrossRef]
- Holdstock, J.S.; Mayes, A.R.; Cezayirli, E.; Aggleton, J.P.; Roberts, N. A comparison of egocentric and allocentric spatial memory in medial temporal lobe and Korsakoff amnesics. Cortex 1999, 35, 479–501. [Google Scholar] [CrossRef] [PubMed]
- Kopelman, M.D.; Stanhope, N.; Kingsley, D. Temporal and spatial context memory in patients with focal frontal, temporal lobe, and diencephalic lesions. Neuropsychologia 1997, 35, 1533–1545. [Google Scholar] [CrossRef]
- Shoqeirat, M.A.; Mayes, A.R. Disproportionate incidental spatial-memory and recall deficits in amnesia. Neuropsychologia 1991, 29, 749–769. [Google Scholar] [CrossRef] [PubMed]
- Mayes, A.R.; Meudell, P.R.; MacDonald, C. Disproportionate intentional spatial-memory impairments in amnesia. Neuropsychologia 1991, 29, 771–784. [Google Scholar] [CrossRef] [PubMed]
- El Haj, M.; Nandrino, J.L.; Coello, Y.; Miller, R.; Antoine, P. Source monitoring in Korsakoff’s syndrome: “Did I touch the toothbrush or did I imagine doing so?”. Cortex 2017, 91, 262–270. [Google Scholar] [CrossRef]
- Conway, M.A. Memory and the self. J. Mem. Lang. 2005, 53, 594–628. [Google Scholar] [CrossRef]
- Rubin, D.C. A basic-systems approach to autobiographical memory. Curr. Dir. Psychol. Sci. 2005, 14, 79–83. [Google Scholar] [CrossRef]
- El Haj, M.; Gandolphe, M.C.; Moustafa, A.A.; Nandrino, J.L. Tell about yourself to improve your autobiographical memory: A study of Korsakoff’s syndrome. Psychiatry Res. 2018, 268, 37–41. [Google Scholar] [CrossRef]
- El Haj, M.; Daoudi, M.; Gallouj, K.; Moustafa, A.A.; Nandrino, J.-L. When your face describes your memories: Facial expressions during retrieval of autobiographical memories. Rev. Neurosci. 2018, 29, 861–872. [Google Scholar] [CrossRef]
- El Haj, M.; Nandrino, J.L. Phenomenological characteristics of autobiographical memory in Korsakoff’s syndrome. Conscious. Cogn. 2017, 55, 188–196. [Google Scholar] [CrossRef]
- Kopelman, M.D.; Stanhope, N.; Kingsley, D. Retrograde amnesia in patients with diencephalic, temporal lobe or frontal lesions. Neuropsychologia 1999, 37, 939–958. [Google Scholar] [CrossRef] [PubMed]
- Oscar-Berman, M. Function and dysfunction of prefrontal brain circuitry in alcoholic Korsakoff’s syndrome. Neuropsychol. Rev. 2012, 22, 154–169. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.K.; Kim, J.K.; Risse, G. Do alcoholic Korsakoff’s syndrome patients acquire affective reactions? J. Exp. Psychol. Learn. Mem. Cogn. 1985, 11, 22–36. [Google Scholar] [CrossRef] [PubMed]
- El Haj, M.; Nandrino, J.-L.; Kessels, R.P.C.; Ndobo, A. High emotional experience during autobiographical retrieval in women with Korsakoff syndrome. Cogn. Neuropsychiatry 2021, 26, 136–148. [Google Scholar] [CrossRef]
- El Haj, M.; Nandrino, J.L. Seeing life through rose-colored spectacles: Autobiographical memory as experienced in Korsakoff’s syndrome. Conscious. Cogn. 2018, 60, 9–16. [Google Scholar] [CrossRef]
- Herrmann, D.; Oudman, E.; Postma, A. The era of our lives: The memory of Korsakoff patients for the first Covid-19 pandemic lockdown in the Netherlands. Conscious. Cogn. 2023, 107, 103454. [Google Scholar] [CrossRef]
- Bechara, A.; Damasio, A.R. The somatic marker hypothesis: A neural theory of economic decision. Games Econ. Behav. 2005, 52, 336–372. [Google Scholar] [CrossRef]
- Mukherjee, K. A dual system model of preferences under risk. Psychol. Rev. 2010, 117, 243–255. [Google Scholar] [CrossRef]
- Carstensen, L.L.; Turan, B.; Scheibe, S.; Ram, N.; Ersner-Hershfield, H.; Samanez-Larkin, G.R.; Brooks, K.P.; Nesselroade, J.R. Emotional experience improves with age: Evidence based on over 10 years of experience sampling. Psychol. Aging 2011, 26, 21–33. [Google Scholar] [CrossRef]
- Reed, A.E.; Carstensen, L.L. The theory behind the age-related positivity effect. Front. Psychol. 2012, 3, 339. [Google Scholar] [CrossRef]
- Mather, M.; Carstensen, L.L. Aging and motivated cognition: The positivity effect in attention and memory. Trends Cogn. Sci. 2005, 9, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.L.; Isaacowitz, D.M.; Charles, S.T. Taking time seriously. A theory of socioemotional selectivity. Am. Psychol. 1999, 54, 165–181. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.; Seymour, T.L.; Gaunt, J.T.; Baker, C.; Nesmith, K.; Mather, M. Aging and goal-directed emotional attention: Distraction reverses emotional biases. Emotion 2007, 7, 705–714. [Google Scholar] [CrossRef] [PubMed]
- Lockenhoff, C.E.; Carstensen, L.L. Aging, emotion, and health-related decision strategies: Motivational manipulations can reduce age differences. Psychol. Aging 2007, 22, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Goeleven, E.; De Raedt, R.; Dierckx, E. The positivity effect in older adults: The role of affective interference and inhibition. Aging Ment. Health 2010, 14, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, D.L.; Gifford, R.K. Illusory correlation in interpersonal perception: A cognitive basis of stereotypic judgments. J. Exp. Soc. Psychol. 1976, 12, 392–407. [Google Scholar] [CrossRef]
- Korsakoff, S.S. Etude médico-psychologique sur une forme des maladies de la mémoire. Révue Philosophique 1889, 28, 501–530. [Google Scholar]
- El Haj, M.; Gely-Nargeot, M.C.; Raffard, S. Destination Memory and Cognitive Theory of Mind in Alzheimer’s Disease. J. Alzheimers Dis. 2015, 48, 529–536. [Google Scholar] [CrossRef]
- El Haj, M.; Saloppé, X.; Nandrino, J.L. Destination memory and deception: When I lie to Barack Obama about the moon. Psychol. Res. 2018, 82, 600–606. [Google Scholar] [CrossRef]


{kind=link}
| Task | Korsakoff n = 25 | Controls n = 28 | Between-Group Comparisons | |
|---|---|---|---|---|
| Episodic memory | Grober and Buschke | 6.92 (2.04) | 10.50 (1.64) | t(51) = 7.07, p < 0.001 |
| Working memory | Forward Span | 5.56 (1.08) | 6.29 (1.30) | t(51) = 2.19, p < 0.05 |
| Backward Span | 4.00 (0.64) | 4.93 (1.01) | t(51) = 3.92, p < 0.001 | |
| Verbal fluency | Verbal Fluency | 10.24 (3.98) | 16.96 (4.34) | t(51) = 5.90, p < 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El Haj, M.; Ndobo, A.; Moustafa, A.A.; Allain, P. “What Did I Tell This Sad Person?”: Memory for Emotional Destinations in Korsakoff’s Syndrome. J. Clin. Med. 2023, 12, 1919. https://doi.org/10.3390/jcm12051919
El Haj M, Ndobo A, Moustafa AA, Allain P. “What Did I Tell This Sad Person?”: Memory for Emotional Destinations in Korsakoff’s Syndrome. Journal of Clinical Medicine. 2023; 12(5):1919. https://doi.org/10.3390/jcm12051919
Chicago/Turabian StyleEl Haj, Mohamad, André Ndobo, Ahmed A. Moustafa, and Philippe Allain. 2023. "“What Did I Tell This Sad Person?”: Memory for Emotional Destinations in Korsakoff’s Syndrome" Journal of Clinical Medicine 12, no. 5: 1919. https://doi.org/10.3390/jcm12051919
APA StyleEl Haj, M., Ndobo, A., Moustafa, A. A., & Allain, P. (2023). “What Did I Tell This Sad Person?”: Memory for Emotional Destinations in Korsakoff’s Syndrome. Journal of Clinical Medicine, 12(5), 1919. https://doi.org/10.3390/jcm12051919