
Gender Differences in Psychological Symptoms and Quality of Life in Patients with Inflammatory Bowel Disease in China: A Multicenter Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Study Assessments and Data Collection
2.2.1. General Information Collection
2.2.2. Generalized Anxiety Disorder 7-Item Scale (GAD-7) and Patient Health Questionnaire-9 (PHQ-9)
2.2.3. Pittsburgh Sleep Quality Index (PSQI)
2.2.4. Inflammatory Bowel Disease Quality-of-Life Questionnaire (IBD-Q)
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of IBD Patients of Different Genders
3.2. Psychological Symptoms, Sleep Quality, and Quality of Life in IBD Patients of Different Genders
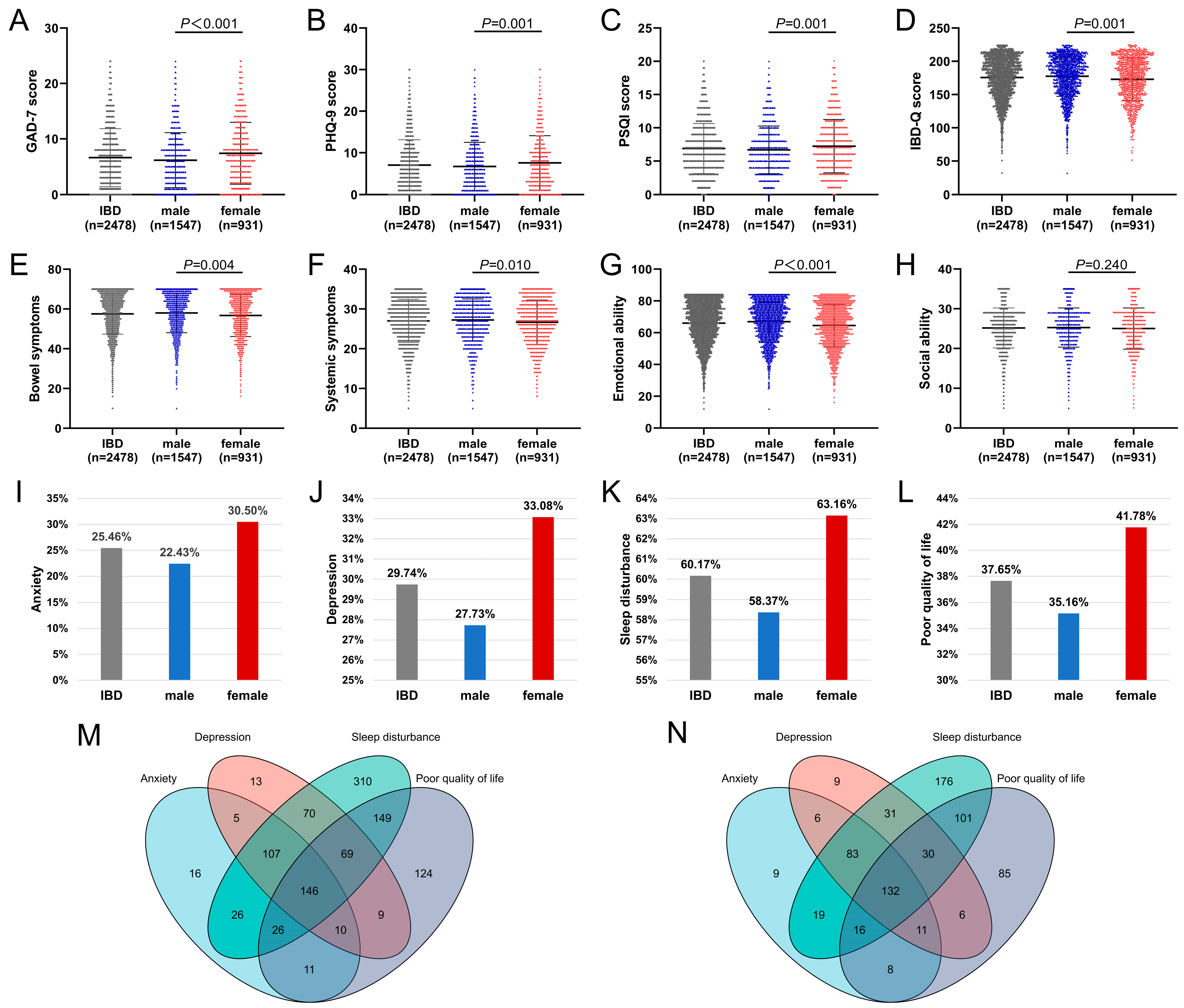
3.2.1. Scores of Psychological Symptoms, Sleep Quality, and Quality of Life in IBD Patients of Different Genders
3.2.2. Psychological Symptoms, Sleep Quality, and Quality of Life in IBD Patients of Different Genders
3.3. Influencing Factors of Psychological Symptoms, Sleep Quality, and Quality of Life in IBD Patients of Different Genders
3.3.1. Univariate Analysis of Influencing Factors of Psychological Symptoms, Sleep Quality and Quality of Life in IBD Patients of Different Genders
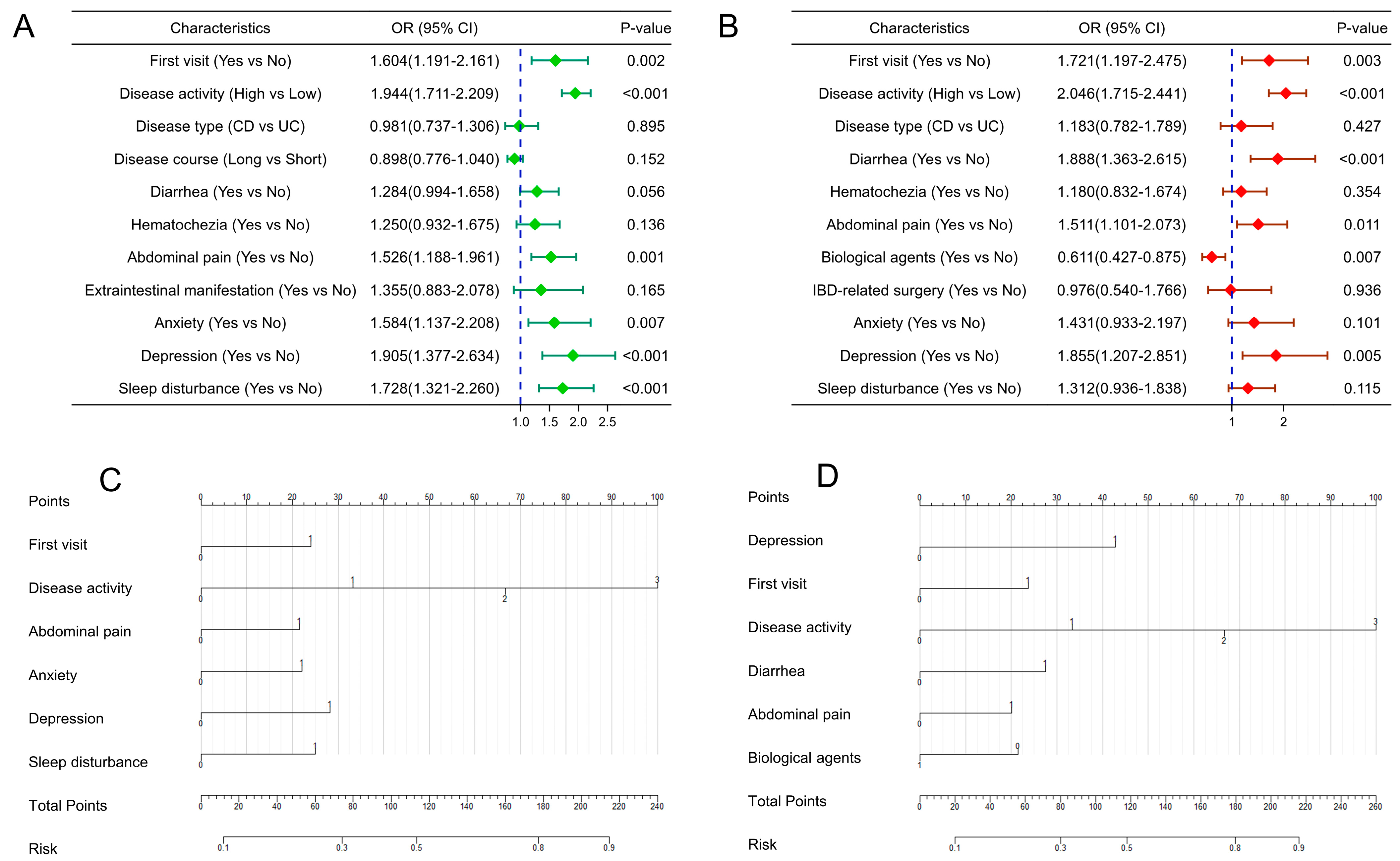
3.3.2. Multivariate Logistic Regression Analysis of Influencing Factors of Psychological Symptoms, Sleep Quality, and Quality of Life in IBD Patients of Different Genders
3.4. Construction and Verification of Nomogram for Predicting Quality of Life in IBD Patients of Different Genders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| IBD | inflammatory bowel disease |
| UC | ulcerative colitis |
| CD | Crohn’s disease |
| GAD-7 | Generalized Anxiety Disorder 7-item Scale |
| PHQ-9 | Patient Health Questionnaire-9 |
| PSQI | Pittsburgh Sleep Quality Index |
| IBD-Q | Inflammatory Bowel Disease Quality-of-Life Questionnaire |
| OR | odds ratio |
| CI | confidence interval |
| ROC | receiver operating characteristic |
| AUC | the area under the ROC curve |
| C-index | consistency index |
| DCA | decision curve analysis |
References
- Zhao, M.; Gonczi, L.; Lakatos, P.L.; Burisch, J. The burden of inflammatory bowel disease in Europe in 2020. J. Crohn’s Colitis 2021, 15, 1573–1587. [Google Scholar] [CrossRef]
- Kappelman, M.D.; Rifas-Shiman, S.L.; Kleinman, K.; Ollendorf, D.; Bousvaros, A.; Grand, R.J.; Finkelstein, J.A. The prevalence and geographic distribution of Crohn’s disease and ulcerative colitis in the United States. Clin. Gastroenterol. Hepatol. 2007, 5, 1424–1429. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Wajda, A.; Svenson, L.W.; Mackenzie, A.; Koehoorn, M.; Jackson, M.; Fedorak, R.; Israel, D.; Blanchard, J.F. The epidemiology of inflammatory bowel disease in Canada: A population-based study. Am. J. Gastroenterol. 2006, 101, 1559–1568. [Google Scholar] [CrossRef] [PubMed]
- Lophaven, S.N.; Lynge, E.; Burisch, J. The incidence of inflammatory bowel disease in Denmark 1980–2013: A nationwide cohort study. Aliment. Pharmacol. Ther. 2017, 45, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, Y.; Kim, S.P.; Lee, S.H.; Oh, S.H.; Yang, S.K.; Yoon, H.J.; Kim, K.M. Shift to a younger age and regional differences in inflammatory bowel disease in Korea: Using healthcare administrative data. Dig. Dis. Sci. 2022, 67, 5079–5089. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Kaur, K.; Mahajan, R.; Midha, V.; Singh, A.; Sharma, S.; Puri, A.S.; Goswami, B.; Desai, D.; Pai, C.G.; et al. Colitis and Crohn’s foundation (India): A first nationwide inflammatory bowel disease registry. Intest. Res. 2021, 19, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Song, P.; Li, J.; Tao, Y.; Li, G.; Li, X.; Yu, Z. The disease burden and clinical characteristics of inflammatory bowel disease in the Chinese population: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2017, 14, 238. [Google Scholar] [CrossRef] [PubMed]
- Greywoode, R.; Ullman, T.; Keefer, L. National prevalence of psychological distress and use of mental health care in inflammatory bowel disease. Inflamm. Bowel Dis. 2023, 29, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Barberio, B.; Zamani, M.; Black, C.J.; Savarino, E.V.; Ford, A.C. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 359–370. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Hitchon, C.A.; Walld, R.; Bolton, J.M.; Sareen, J.; Walker, J.R.; Graff, L.A.; Patten, S.B.; Singer, A.; Lix, L.M.; et al. Increased burden of psychiatric disorders in inflammatory bowel disease. Inflamm. Bowel Dis. 2019, 25, 360–368. [Google Scholar] [CrossRef]
- Lores, T.; Goess, C.; Mikocka-Walus, A.; Collins, K.L.; Burke, A.; Chur-Hansen, A.; Delfabbro, P.; Andrews, J.M. Integrated psychological care is needed, welcomed and effective in ambulatory inflammatory bowel disease management: Evaluation of a new initiative. J. Crohn’s Colitis 2019, 13, 819–827. [Google Scholar] [CrossRef]
- Szigethy, E.M.; Allen, J.I.; Reiss, M.; Cohen, W.; Perera, L.P.; Brillstein, L.; Cross, R.K.; Schwartz, D.A.; Kosinski, L.R.; Colton, J.B.; et al. White paper aga: The impact of mental and psychosocial factors on the care of patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2017, 15, 986–997. [Google Scholar] [CrossRef]
- Liu, C.; Yu, R.; Zhang, J.; Wei, S.; Xue, F.; Guo, Y.; He, P.; Shang, L.; Dong, W. Research hotspot and trend analysis in the diagnosis of inflammatory bowel disease: A machine learning bibliometric analysis from 2012 to 2021. Front. Immunol. 2022, 13, 972079. [Google Scholar] [CrossRef] [PubMed]
- Inflammatory Bowel Disease Group; Chinese Society of Gastroenterology; Chinese Medical Association. Chinese consensus on diagnosis and treatment in inflammatory bowel disease (2018, Beijing). J. Dig. Dis. 2021, 22, 298–317. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, A.; Fan, D.; Borichevsky, G.M.; Mules, T.C.; Hirschfeld, E.; Frampton, C.M.; Day, A.S.; Siegel, C.A.; Gearry, R.B. The disease severity index for inflammatory bowel disease is associated with psychological symptoms and quality of life, and predicts a more complicated disease course. Aliment. Pharmacol. Ther. 2022, 56, 664–674. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The phq-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The gad-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Hashash, J.G.; Knisely, M.R.; Germain, A.; Mcauliff, K.; Strassburger, M.; Vachon, A.; Binion, D.G.; Regueiro, M.; Wallace, M.; Szigethy, E. Brief behavioral therapy and bupropion for sleep and fatigue in young adults with Crohn’s disease: An exploratory open trial study. Clin. Gastroenterol. Hepatol. 2022, 20, 96–104. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.R., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Guyatt, G.; Mitchell, A.; Irvine, E.J.; Singer, J.; Williams, N.; Goodacre, R.; Tompkins, C. A new measure of health status for clinical trials in inflammatory bowel disease. Gastroenterology 1989, 96, 804–810. [Google Scholar] [CrossRef]
- Hlavaty, T.; Persoons, P.; Vermeire, S.; Ferrante, M.; Pierik, M.; Van Assche, G.; Rutgeerts, P. Evaluation of short-term responsiveness and cutoff values of inflammatory bowel disease questionnaire in Crohn’s disease. Inflamm. Bowel Dis. 2006, 12, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, G.G.; Windsor, J.W. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Irving, P.; Barrett, K.; Nijher, M.; de Lusignan, S. Prevalence of depression and anxiety in people with inflammatory bowel disease and associated healthcare use: Population-based cohort study. BMJ Ment. Health 2021, 24, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Tang, A.; Wang, X.; Shen, S. Assessment of quality of life in Chinese patients with inflammatory bowel disease and their caregivers. Inflamm. Bowel Dis. 2018, 24, 2039–2047. [Google Scholar] [CrossRef]
- Fairbrass, K.M.; Gracie, D.J.; Ford, A.C. Relative contribution of disease activity and psychological health to prognosis of inflammatory bowel disease during 6.5 years of longitudinal follow-up. Gastroenterology 2022, 163, 190–203. [Google Scholar] [CrossRef]
- Marrie, R.A.; Graff, L.A.; Fisk, J.D.; Patten, S.B.; Bernstein, C.N. The relationship between symptoms of depression and anxiety and disease activity in IBD over time. Inflamm. Bowel Dis. 2021, 27, 1285–1293. [Google Scholar] [CrossRef]
- Rozich, J.J.; Holmer, A.; Singh, S. Effect of lifestyle factors on outcomes in patients with inflammatory bowel diseases. Am. J. Gastroenterol. 2020, 115, 832–840. [Google Scholar] [CrossRef]
- Goodman, W.A.; Erkkila, I.P.; Pizarro, T.T. Sex matters: Impact on pathogenesis, presentation and treatment of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 740–754. [Google Scholar] [CrossRef]
- Weismuller, T.J.; Trivedi, P.J.; Bergquist, A.; Imam, M.; Lenzen, H.; Ponsioen, C.Y.; Holm, K.; Gotthardt, D.; Farkkila, M.A.; Marschall, H.U.; et al. Patient age, sex, and inflammatory bowel disease phenotype associate with course of primary sclerosing cholangitis. Gastroenterology 2017, 152, 1975–1984. [Google Scholar] [CrossRef]
- Blumenstein, I.; Herrmann, E.; Filmann, N.; Zosel, C.; Tacke, W.; Bock, H.; Dignass, A.; Hartmann, F.; Zeuzem, S.; Stein, J.; et al. Female patients suffering from inflammatory bowel diseases are treated less frequently with immunosuppressive medication and have a higher disease activity: A subgroup analysis of a large multi-centre, prospective, internet-based study. J. Crohn’s Colitis 2011, 5, 203–210. [Google Scholar] [CrossRef]
- Severs, M.; Spekhorst, L.M.; Mangen, M.J.; Dijkstra, G.; Lowenberg, M.; Hoentjen, F.; van der Meulen-De, J.A.; Pierik, M.; Ponsioen, C.Y.; Bouma, G.; et al. Sex-related differences in patients with inflammatory bowel disease: Results of 2 prospective cohort studies. Inflamm. Bowel Dis. 2018, 24, 1298–1306. [Google Scholar] [CrossRef] [PubMed]
- Auzolle, C.; Nancey, S.; Tran-Minh, M.L.; Buisson, A.; Pariente, B.; Stefanescu, C.; Fumery, M.; Marteau, P.; Treton, X.; Hammoudi, N.; et al. Male gender, active smoking and previous intestinal resection are risk factors for post-operative endoscopic recurrence in Crohn’s disease: Results from a prospective cohort study. Aliment. Pharmacol. Ther. 2018, 48, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Gracie, D.J.; Hamlin, P.J.; Ford, A.C. The influence of the brain-gut axis in inflammatory bowel disease and possible implications for treatment. Lancet Gastroenterol. Hepatol. 2019, 4, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Holdam, A.S.; Bager, P.; Dahlerup, J.F. Biological therapy increases the health-related quality of life in patients with inflammatory bowel disease in a clinical setting. Scand. J. Gastroenterol. 2016, 51, 706–711. [Google Scholar] [CrossRef] [PubMed]
- Biedermann, L.; Fournier, N.; Misselwitz, B.; Frei, P.; Zeitz, J.; Manser, C.N.; Pittet, V.; Juillerat, P.; von Kanel, R.; Fried, M.; et al. High rates of smoking especially in female Crohn’s disease patients and low use of supportive measures to achieve smoking cessation—Data from the Swiss IBD cohort study. J. Crohn’s Colitis 2015, 9, 819–829. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.; Parkes, G.C.; Selinger, C.; et al. British society of gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef]
- Hood, M.M.; Wilson, R.; Gorenz, A.; Jedel, S.; Raeisi, S.; Hobfoll, S.; Keshavarzian, A. Sleep quality in ulcerative colitis: Associations with inflammation, psychological distress, and quality of life. Int. J. Behav. Med. 2018, 25, 517–525. [Google Scholar] [CrossRef]
- Van den Brink, G.; Stapersma, L.; Vlug, L.E.; Rizopolous, D.; Bodelier, A.G.; van Wering, H.; Hurkmans, P.; Stuyt, R.; Hendriks, D.M.; van der Burg, J.; et al. Clinical disease activity is associated with anxiety and depressive symptoms in adolescents and young adults with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2018, 48, 358–369. [Google Scholar] [CrossRef]
- Panara, A.J.; Yarur, A.J.; Rieders, B.; Proksell, S.; Deshpande, A.R.; Abreu, M.T.; Sussman, D.A. The incidence and risk factors for developing depression after being diagnosed with inflammatory bowel disease: A cohort study. Aliment. Pharmacol. Ther. 2014, 39, 802–810. [Google Scholar] [CrossRef]
- Paulides, E.; Pasma, A.; Erler, N.S.; van Eijk, R.; de Vries, A.C.; van der Woude, C.J. Impact of the coronavirus disease pandemic on health-related quality of life of patients with inflammatory bowel disease. Dig. Dis. Sci. 2022, 67, 2849–2856. [Google Scholar] [CrossRef]
- Truta, B. The impact of inflammatory bowel disease on women’s lives. Curr. Opin. Gastroenterol. 2021, 37, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Cherepanov, D.; Palta, M.; Fryback, D.G.; Robert, S.A.; Hays, R.D.; Kaplan, R.M. Gender differences in multiple underlying dimensions of health-related quality of life are associated with sociodemographic and socioeconomic status. Med. Care 2011, 49, 1021–1030. [Google Scholar] [CrossRef] [PubMed]
- Orfila, F.; Ferrer, M.; Lamarca, R.; Tebe, C.; Domingo-Salvany, A.; Alonso, J. Gender differences in health-related quality of life among the elderly: The role of objective functional capacity and chronic conditions. Soc. Sci. Med. 2006, 63, 2367–2380. [Google Scholar] [CrossRef] [PubMed]
- Case, A.; Paxson, C. Sex differences in morbidity and mortality. Demography 2005, 42, 189–214. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.V.; van Langenberg, D.R.; Holtmann, G.J.; Andrews, J.M. Functional gastrointestinal disorders in inflammatory bowel disease: Impact on quality of life and psychological status. J. Gastroenterol. Hepatol. 2011, 26, 916–923. [Google Scholar] [CrossRef]
- Vemuri, R.; Sylvia, K.E.; Klein, S.L.; Forster, S.C.; Plebanski, M.; Eri, R.; Flanagan, K.L. The microgenderome revealed: Sex differences in bidirectional interactions between the microbiota, hormones, immunity and disease susceptibility. Semin. Immunopathol. 2019, 41, 265–275. [Google Scholar] [CrossRef]
- Vermeire, S.; Satsangi, J.; Peeters, M.; Parkes, M.; Jewell, D.P.; Vlietinck, R.; Rutgeerts, P. Evidence for inflammatory bowel disease of a susceptibility locus on the X chromosome. Gastroenterology 2001, 120, 834–840. [Google Scholar] [CrossRef]
- Lee, H.S.; Oh, H.; Yang, S.K.; Baek, J.; Jung, S.; Hong, M.; Kim, K.M.; Shin, H.D.; Kim, K.J.; Park, S.H.; et al. X chromosome-wide association study identifies a susceptibility locus for inflammatory bowel disease in Koreans. J. Crohn’s Colitis 2017, 11, 820–830. [Google Scholar] [CrossRef]
- Zelinkova, Z.; Stokkers, P.C.; van der Linde, K.; Kuipers, E.J.; Peppelenbosch, M.P.; van der Woude, C.P. Maternal imprinting and female predominance in familial Crohn’s disease. J. Crohn’s Colitis 2012, 6, 771–776. [Google Scholar] [CrossRef]
- Xu, L.; Huang, G.; Cong, Y.; Yu, Y.; Li, Y. Sex-related differences in inflammatory bowel diseases: The potential role of sex hormones. Inflamm. Bowel Dis. 2022, 28, 1766–1775. [Google Scholar] [CrossRef]
- Jacenik, D.; Cygankiewicz, A.I.; Mokrowiecka, A.; Malecka-Panas, E.; Fichna, J.; Krajewska, W.M. Sex-and age-related estrogen signaling alteration in inflammatory bowel diseases: Modulatory role of estrogen receptors. Int. J. Mol. Sci. 2019, 20, 3175. [Google Scholar] [CrossRef] [PubMed]
- Xing, E.; Billi, A.C.; Gudjonsson, J.E. Sex bias and autoimmune diseases. J. Investig. Dermatol. 2022, 142, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Lotter, H.; Altfeld, M. Sex differences in immunity. Semin. Immunopathol. 2019, 41, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Ngo, S.T.; Steyn, F.J.; Mccombe, P.A. Gender differences in autoimmune disease. Front. Neuroendocrinol. 2014, 35, 347–369. [Google Scholar] [CrossRef]
- Son, H.J.; Kim, N.; Song, C.H.; Nam, R.H.; Choi, S.I.; Kim, J.S.; Lee, D.H. Sex-related alterations of gut microbiota in the C57BL/6 mouse model of inflammatory bowel disease. J. Cancer Prev. 2019, 24, 173–182. [Google Scholar] [CrossRef]
- Kozik, A.J.; Nakatsu, C.H.; Chun, H.; Jones-Hall, Y.L. Age, sex, and TNF associated differences in the gut microbiota of mice and their impact on acute TNBS colitis. Exp. Mol. Pathol. 2017, 103, 311–319. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | IBD (n = 2478) | S | p-Value | UC (n = 1371) | S | p-Value | CD (n = 1107) | S | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 1547) | Female (n = 931) | Male (n = 754) | Female (n = 617) | Male (n = 793) | Female (n = 314) | |||||||
| Age (years old, ± s) | 37.30 ± 12.71 | 39.06 ± 12.19 | −3.378 * | 0.001 | 42.22 ± 13.26 | 40.94 ± 11.69 | 1.899 * | 0.058 | 32.63 ± 10.16 | 35.36 ± 12.33 | −3.483 * | 0.001 |
| First visit (n (%)) | 297 (19.2) | 196 (21.1) | 1.254 | 0.263 | 194 (25.7) | 149 (24.1) | 0.452 | 0.502 | 103 (13.0) | 47 (15.0) | 0.752 | 0.386 |
| Disease activity (n (%)) | 8.635 | 0.003 | 0.329 | 0.566 | 1.687 | 0.194 | ||||||
| Remission | 625 (40.4) | 321 (34.5) | 227 (30.1) | 177 (28.7) | 398 (50.2) | 144 (45.9) | ||||||
| Active | 922 (59.6) | 610 (65.5) | 5.832 | 0.054 | 527 (69.9) | 440 (71.3) | 3.583 | 0.167 | 395 (49.8) | 170 (54.1) | 2.828 | 0.243 |
| Mild | 368 (39.9) | 220 (36.1) | 208 (39.5) | 161 (36.6) | 160 (40.5) | 59 (34.7) | ||||||
| Moderate | 419 (45.4) | 315 (51.6) | 238 (45.2) | 224 (50.9) | 181 (45.8) | 91 (53.5) | ||||||
| Severe | 135 (14.6) | 75 (12.3) | 81 (15.4) | 55 (12.5) | 54 (13.7) | 20 (11.8) | ||||||
| Disease course (n (%)) | 10.473 | 0.005 | 5.080 | 0.079 | 2.833 | 0.243 | ||||||
| <2 years | 560 (36.2) | 379 (40.7) | 303 (40.3) | 280 (45.4) | 257 (32.4) | 99 (31.5) | ||||||
| 2~5 years | 512 (33.1) | 252 (27.1) | 217 (28.9) | 148 (24.0) | 295 (37.2) | 104 (33.1) | ||||||
| >5 years | 473 (30.6) | 300 (32.2) | 232 (30.9) | 189 (30.6) | 241 (30.4) | 111 (35.4) | ||||||
| Diarrhea (n (%)) | 2.631 | 0.105 | 0.019 | 0.891 | 0.570 | 0.450 | ||||||
| Yes | 928 (60.0) | 589 (63.3) | 511 (67.8) | 416 (67.4) | 417 (52.6) | 173 (55.1) | ||||||
| No | 619 (40.0) | 342 (36.7) | 243 (32.2) | 201 (32.6) | 376 (47.4) | 141 (44.9) | ||||||
| Hematochezia (n (%)) | 18.653 | <0.001 | 0.243 | 0.622 | 2.875 | 0.090 | ||||||
| Yes | 609 (39.4) | 449 (48.2) | 479 (63.5) | 384 (62.2) | 130 (16.4) | 65 (20.7) | ||||||
| No | 938 (60.6) | 482 (51.8) | 275 (36.5) | 233 (37.8) | 663 (83.6) | 249 (79.3) | ||||||
| Abdominal pain (n (%)) | 0.991 | 0.319 | 2.769 | 0.096 | 2.461 | 0.117 | ||||||
| Yes | 874 (56.5) | 545 (58.5) | 368 (48.8) | 329 (53.3) | 506 (63.8) | 216 (68.8) | ||||||
| No | 673 (43.5) | 386 (41.5) | 386 (51.2) | 288 (46.7) | 287 (36.2) | 98 (31.2) | ||||||
| Extraintestinal manifestation (n (%)) | 0.159 | 0.690 | 0.354 | 0.552 | 0.227 | 0.634 | ||||||
| Yes | 121 (7.8) | 77 (8.3) | 50 (6.6) | 46 (7.5) | 71 (9.0) | 31 (9.9) | ||||||
| No | 1426 (92.2) | 854 (91.7) | 704 (93.4) | 571 (92.5) | 722 (91.0) | 283 (90.1) | ||||||
| Comorbidities (n (%)) | 7.362 | 0.007 | 0.330 | 0.565 | 1.243 | 0.265 | ||||||
| Yes | 146 (9.4) | 59 (6.3) | 16 (2.1) | 16 (2.6) | 130 (16.4) | 43 (13.7) | ||||||
| No | 1401 (90.6) | 872 (93.7) | 738 (97.9) | 601 (97.4) | 663 (83.6) | 271 (86.3) | ||||||
| 5-Aminosalicylic acid | 26.931 | <0.001 | 0.390 | 0.532 | 0.497 | 0.481 | ||||||
| No | 652 (42.1) | 295 (31.7) | 87 (11.5) | 78 (12.6) | 565 (71.2) | 217 (69.1) | ||||||
| Yes | 895 (57.9) | 636 (68.3) | 667 (88.5) | 539 (87.4) | 228 (28.8) | 97 (30.9) | ||||||
| Mesalamine | 881 (56.9) | 631 (67.8) | 28.647 | <0.001 | 657 (87.1) | 535 (86.7) | 0.054 | 0.816 | 224 (28.2) | 96 (30.6) | 0.592 | 0.442 |
| Sulfasalazine | 42 (2.7) | 24 (2.6) | 0.042 | 0.837 | 36 (4.8) | 23 (3.7) | 0.903 | 0.342 | 6 (0.8) | 1 (0.3) | 0.167 | 0.683 |
| Glucocorticoids | 0.127 | 0.722 | 3.615 | 0.057 | 3.151 | 0.076 | ||||||
| No | 1311 (84.7) | 784 (84.2) | 595 (78.9) | 512 (83.0) | 716 (90.3) | 272 (86.6) | ||||||
| Yes | 236 (15.3) | 147 (15.8) | 159 (21.1) | 105 (17.0) | 77 (9.7) | 42 (13.4) | ||||||
| Prednisone | 147 (9.5) | 88 (9.5) | 0.002 | 0.967 | 88 (11.7) | 54 (8.8) | 3.114 | 0.078 | 59 (7.4) | 34 (10.8) | 3.355 | 0.067 |
| Methylprednisolone | 31 (2.0) | 15 (1.6) | 0.492 | 0.483 | 24 (3.2) | 12 (1.9) | 2.034 | 0.154 | 7 (0.9) | 3 (1.0) | 0.000 | 1.000 |
| Dexamethasone | 16 (1.0) | 15 (1.6) | 1.566 | 0.211 | 14 (1.9) | 15 (2.4) | 0.541 | 0.462 | 2 (0.3) | 0 (0.0) | - | 1.000 |
| Immunosuppressants | 7.493 | 0.006 | 1.429 | 0.232 | 2.473 | 0.116 | ||||||
| No | 1299 (84.0) | 819 (88.0) | 711 (94.3) | 572 (92.7) | 588 (74.1) | 247 (78.7) | ||||||
| Yes | 248 (16.0) | 112 (12.0) | 43 (5.7) | 45 (7.3) | 205 (25.9) | 67 (21.3) | ||||||
| Thiopurines | 225 (14.5) | 95 (10.2) | 9.736 | 0.002 | 31 (4.1) | 30 (4.9) | 0.450 | 0.502 | 194 (24.5) | 65 (20.7) | 1.778 | 0.182 |
| Methotrexate | 14 (0.9) | 11 (1.2) | 0.445 | 0.505 | 6 (0.8) | 9 (1.5) | 1.378 | 0.240 | 8 (1.0) | 2 (0.6) | 0.056 | 0.556 |
| Biological agents | 40.068 | <0.001 | 3.125 | 0.077 | 1.645 | 0.200 | ||||||
| No | 676 (43.7) | 529 (56.8) | 531 (70.4) | 461 (74.7) | 145 (18.3) | 68 (21.7) | ||||||
| Yes | 871 (56.3) | 402 (43.2) | 223 (29.6) | 156 (25.3) | 648 (81.7) | 246 (78.3) | ||||||
| Infliximab | 599 (38.7) | 255 (27.4) | 33.035 | <0.001 | 109 (14.5) | 91 (14.7) | 0.023 | 0.879 | 490 (61.8) | 164 (52.2) | 8.506 | 0.004 |
| Vedolizumab | 158 (10.2) | 96 (10.3) | 0.006 | 0.938 | 98 (13.0) | 55 (8.9) | 5.706 | 0.017 | 60 (7.6) | 41 (13.1) | 8.180 | 0.004 |
| Adalimumab | 71 (4.6) | 32 (3.4) | 1.937 | 0.164 | 17 (2.3) | 10 (1.6) | 0.706 | 0.401 | 54 (6.8) | 22 (7.0) | 0.014 | 0.907 |
| Ustekinumab | 48 (3.1) | 21 (2.3) | 1.541 | 0.214 | 2 (0.3) | 1 (0.2) | 1.000 | 46 (5.8) | 20 (6.4) | 0.130 | 0.719 | |
| Chinese herbs | 1.422 | 0.233 | 0.109 | 0.742 | 0.487 | |||||||
| No | 1495 (96.6) | 891 (95.7) | 703 (93.2) | 578 (93.7) | 792 (99.9) | 313 (99.7) | ||||||
| Yes | 52 (3.4) | 40 (4.3) | 51 (6.8) | 39 (6.3) | 1 (0.1) | 1 (0.3) | ||||||
| IBD-related surgery | 15.576 | <0.001 | 1.571 | 0.210 | 0.373 | 0.542 | ||||||
| No | 1326 (85.7) | 848 (91.1) | 739 (98.0) | 610 (98.9) | 587 (74.0) | 238 (75.8) | ||||||
| Yes | 221 (14.3) | 83 (8.9) | 15 (2.0) | 7 (1.1) | 206 (26.0) | 76 (24.2) | ||||||
| IBD (n = 2478) | χ2 | p-Value | UC (n = 1371) | χ2 | p-Value | CD (n = 1107) | χ2 | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male (n = 1547) | Female (n = 931) | Male (n = 754) | Female (n = 617) | Male (n = 793) | Female (n = 314) | |||||||
| Anxiety | 19.964 | <0.001 | 9.017 | 0.003 | 6.138 | 0.013 | ||||||
| No (GAD-7 < 10) | 1200 (77.6) | 647 (69.5) | 565 (74.9) | 417 (67.6) | 635 (80.1) | 230 (73.2) | ||||||
| Yes (GAD-7 ≥ 10) | 347 (22.4) | 284 (30.5) | 189 (25.1) | 200 (32.4) | 158 (19.9) | 84 (26.8) | ||||||
| Symptom Severity | 31.594 | <0.001 | 22.860 | <0.001 | 7.821 | 0.050 | ||||||
| Minimal | 660 (42.7) | 316 (33.9) | 332 (44.0) | 207 (33.5) | 328 (41.4) | 109 (34.7) | ||||||
| Mild | 540 (34.9) | 331 (35.6) | 233 (30.9) | 210 (34.0) | 307 (38.7) | 121 (38.5) | ||||||
| Moderate | 232 (15.0) | 165 (17.7) | 131 (17.4) | 115 (18.6) | 101 (12.7) | 50 (15.9) | ||||||
| Severe | 115 (7.4) | 119 (12.8) | 58 (7.7) | 85 (13.8) | 57 (7.2) | 34 (10.8) | ||||||
| Depression | 7.966 | 0.005 | 4.677 | 0.031 | 1.765 | 0.184 | ||||||
| No (PHQ-9 < 10) | 1118 (72.3) | 623 (66.9) | 536 (71.1) | 405 (65.6) | 582 (73.4) | 218 (69.4) | ||||||
| Yes (PHQ-9 ≥ 10) | 429 (27.7) | 308 (33.1) | 218 (28.9) | 212 (34.4) | 211 (26.6) | 96 (30.6) | ||||||
| Symptom Severity | 13.296 | 0.004 | 9.612 | 0.022 | 3.572 | 0.312 | ||||||
| Minimal | 656 (42.4) | 376 (40.4) | 340 (45.1) | 248 (40.2) | 316 (39.8) | 128 (40.8) | ||||||
| Mild | 462 (29.9) | 247 (26.5) | 196 (26.0) | 157 (25.4) | 266 (33.5) | 90 (28.7) | ||||||
| Moderate | 260 (16.8) | 162 (17.4) | 134 (17.8) | 109 (17.7) | 126 (15.9) | 53 (16.9) | ||||||
| Severe | 169 (10.9) | 146 (15.7) | 84 (11.1) | 103 (16.7) | 85 (10.7) | 43 (13.7) | ||||||
| Sleep disturbance | 5.557 | 0.018 | 3.959 | 0.047 | 1.573 | 0.210 | ||||||
| No (PSQI ≤ 5) | 644 (41.6) | 343 (36.8) | 316 (41.9) | 226 (36.6) | 328 (41.4) | 117 (37.3) | ||||||
| Yes (PSQI > 5) | 903 (58.4) | 588 (63.2) | 438 (58.1) | 391 (63.4) | 465 (58.6) | 197 (62.7) | ||||||
| Sleep quality | 13.441 | 0.004 | 6.595 | 0.086 | 7.215 | 0.065 | ||||||
| Good | 644 (41.6) | 343 (36.8) | 316 (41.9) | 226 (36.6) | 328 (41.4) | 117 (37.3) | ||||||
| Medium | 670 (43.3) | 403 (43.3) | 312 (41.4) | 267 (43.3) | 358 (45.1) | 136 (43.3) | ||||||
| Poor | 202 (13.1) | 151 (16.2) | 112 (14.9) | 103 (16.7) | 90 (11.3) | 48 (15.3) | ||||||
| Very poor | 31 (2.0) | 34 (3.7) | 14 (1.9) | 21 (3.4) | 17 (2.1) | 13 (4.1) | ||||||
| Quality of life | 10.845 | 0.001 | 3.863 | 0.049 | 2.167 | 0.141 | ||||||
| Not poor (IBD-Q ≥ 169) | 1003 (64.8) | 542 (58.2) | 454 (60.2) | 339 (54.9) | 549 (69.2) | 203 (64.6) | ||||||
| Poor (IBD-Q < 169) | 544 (35.2) | 389 (41.8) | 300 (39.8) | 278 (45.1) | 244 (30.8) | 111 (35.4) | ||||||
| IBD-Q score range | 13.175 | 0.004 | 5.201 | 0.158 | 5.001 | 0.172 | ||||||
| 177–224 | 882 (57.0) | 473 (50.8) | 406 (53.8) | 296 (48.0) | 476 (60.0) | 177 (56.4) | ||||||
| 129–176 | 556 (35.9) | 364 (39.1) | 275 (36.5) | 251 (40.7) | 281 (35.4) | 113 (36.0) | ||||||
| 81–128 | 101 (6.5) | 90 (9.7) | 68 (9.0) | 67 (10.9) | 33 (4.2) | 23 (7.3) | ||||||
| 32–80 | 8 (0.5) | 4 (0.4) | 5 (0.7) | 3 (0.5) | 3 (0.4) | 1 (0.3) | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.; Zhang, J.; Chen, M.; An, P.; Xiang, J.; Yu, R.; Zeng, S.; Wei, S.; Deng, B.; Liu, Z.; et al. Gender Differences in Psychological Symptoms and Quality of Life in Patients with Inflammatory Bowel Disease in China: A Multicenter Study. J. Clin. Med. 2023, 12, 1791. https://doi.org/10.3390/jcm12051791
Liu C, Zhang J, Chen M, An P, Xiang J, Yu R, Zeng S, Wei S, Deng B, Liu Z, et al. Gender Differences in Psychological Symptoms and Quality of Life in Patients with Inflammatory Bowel Disease in China: A Multicenter Study. Journal of Clinical Medicine. 2023; 12(5):1791. https://doi.org/10.3390/jcm12051791
Chicago/Turabian StyleLiu, Chuan, Jixiang Zhang, Min Chen, Ping An, Jiankang Xiang, Rong Yu, Suqi Zeng, Shuchun Wei, Beiying Deng, Zhongchun Liu, and et al. 2023. "Gender Differences in Psychological Symptoms and Quality of Life in Patients with Inflammatory Bowel Disease in China: A Multicenter Study" Journal of Clinical Medicine 12, no. 5: 1791. https://doi.org/10.3390/jcm12051791
APA StyleLiu, C., Zhang, J., Chen, M., An, P., Xiang, J., Yu, R., Zeng, S., Wei, S., Deng, B., Liu, Z., Jiang, C., Shi, J., Wu, K., & Dong, W. (2023). Gender Differences in Psychological Symptoms and Quality of Life in Patients with Inflammatory Bowel Disease in China: A Multicenter Study. Journal of Clinical Medicine, 12(5), 1791. https://doi.org/10.3390/jcm12051791