
Alterations in Cervical Nerve Root Function during Different Sitting Positions in Adults with and without Forward Head Posture: A Cross-Sectional Study

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Methods
2.1. Procedures
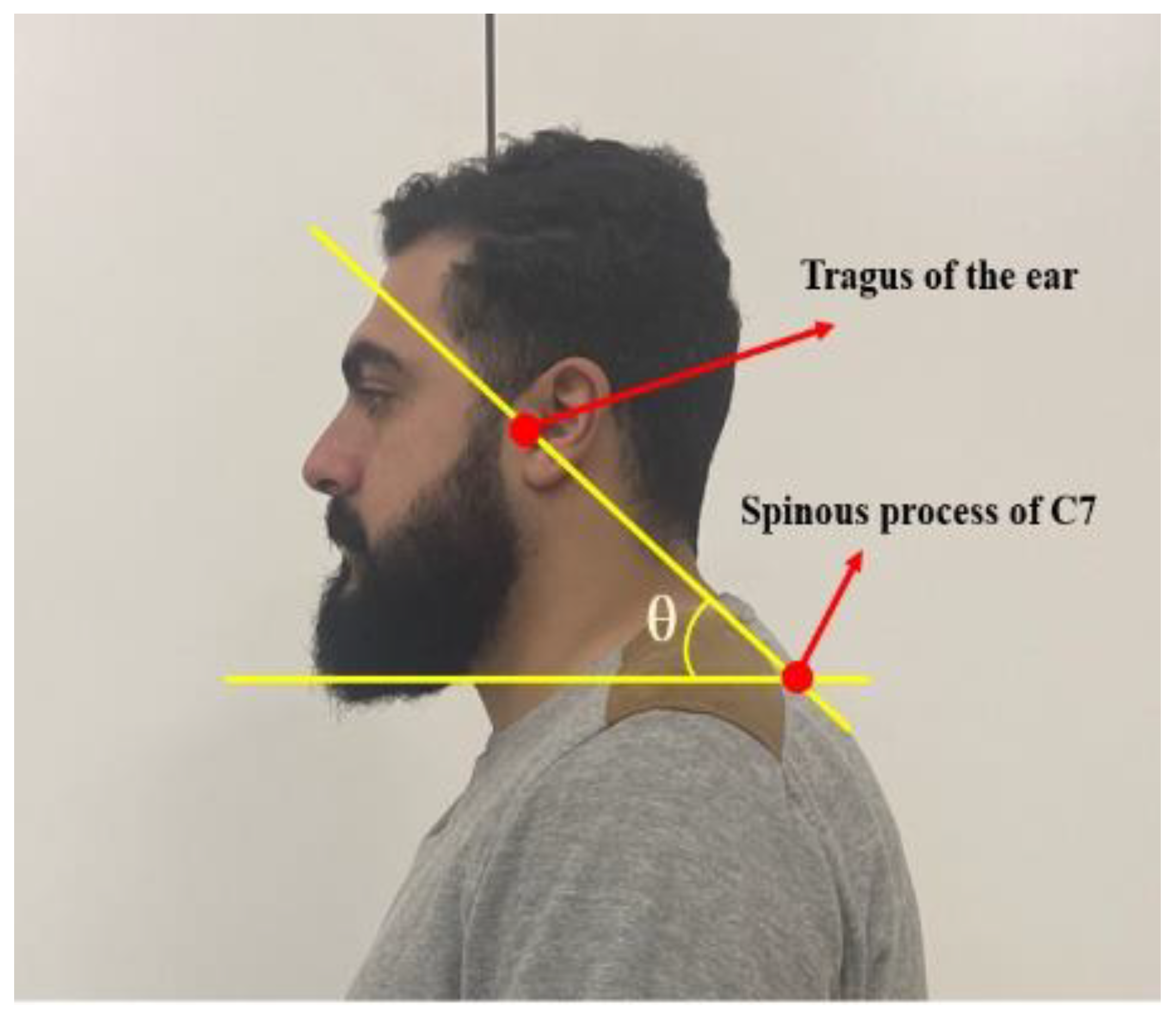
2.1.1. Evaluation of CVA
2.1.2. Positions
- Supine position (which acted as a reference for DSSEPs measurement);
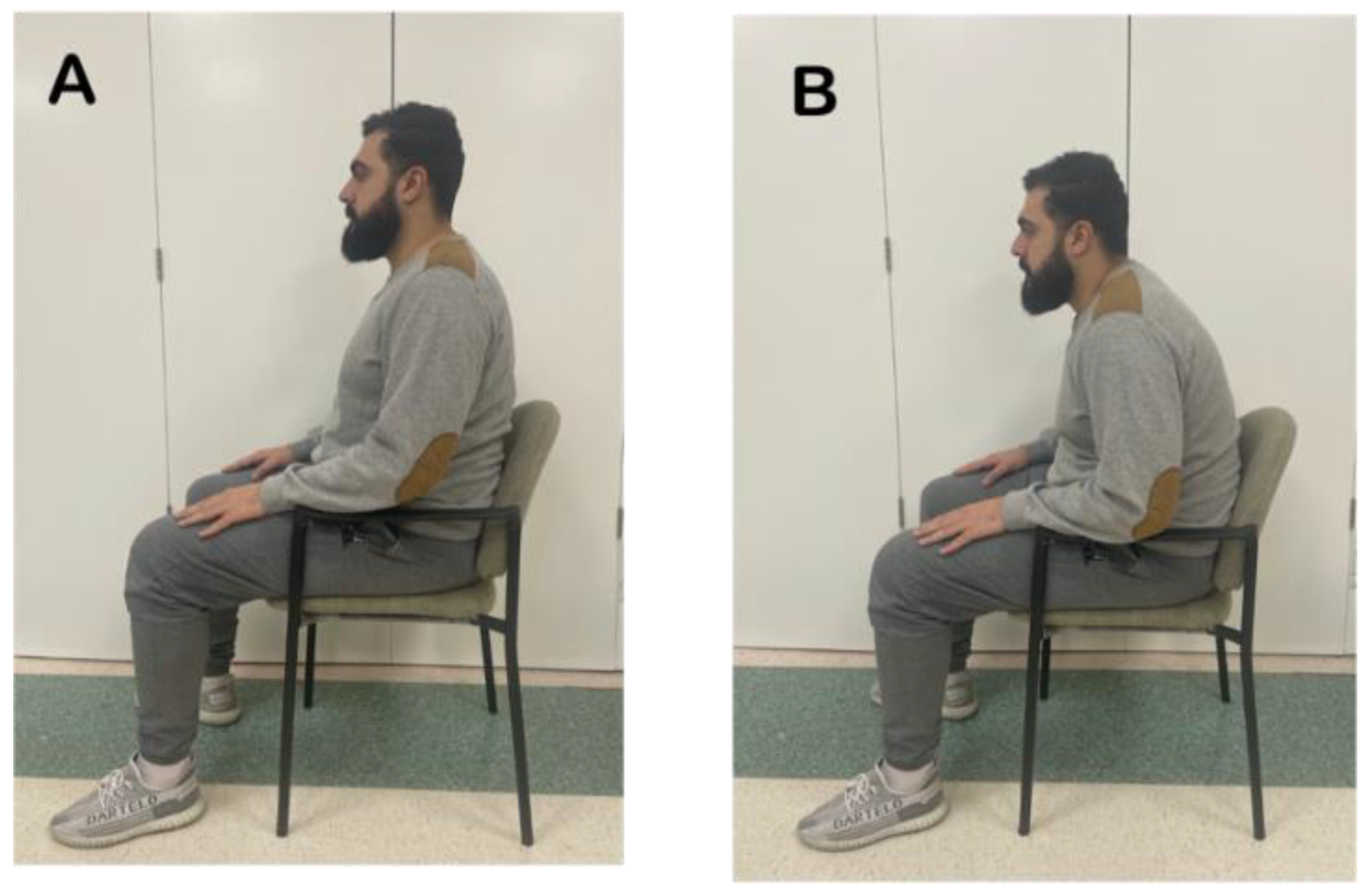
- After assuming the erect sitting posture for 30 min;
- After assuming the slouched sitting posture for 30 min.
Erect Sitting Position
Slouched Sitting Position
Supine Position
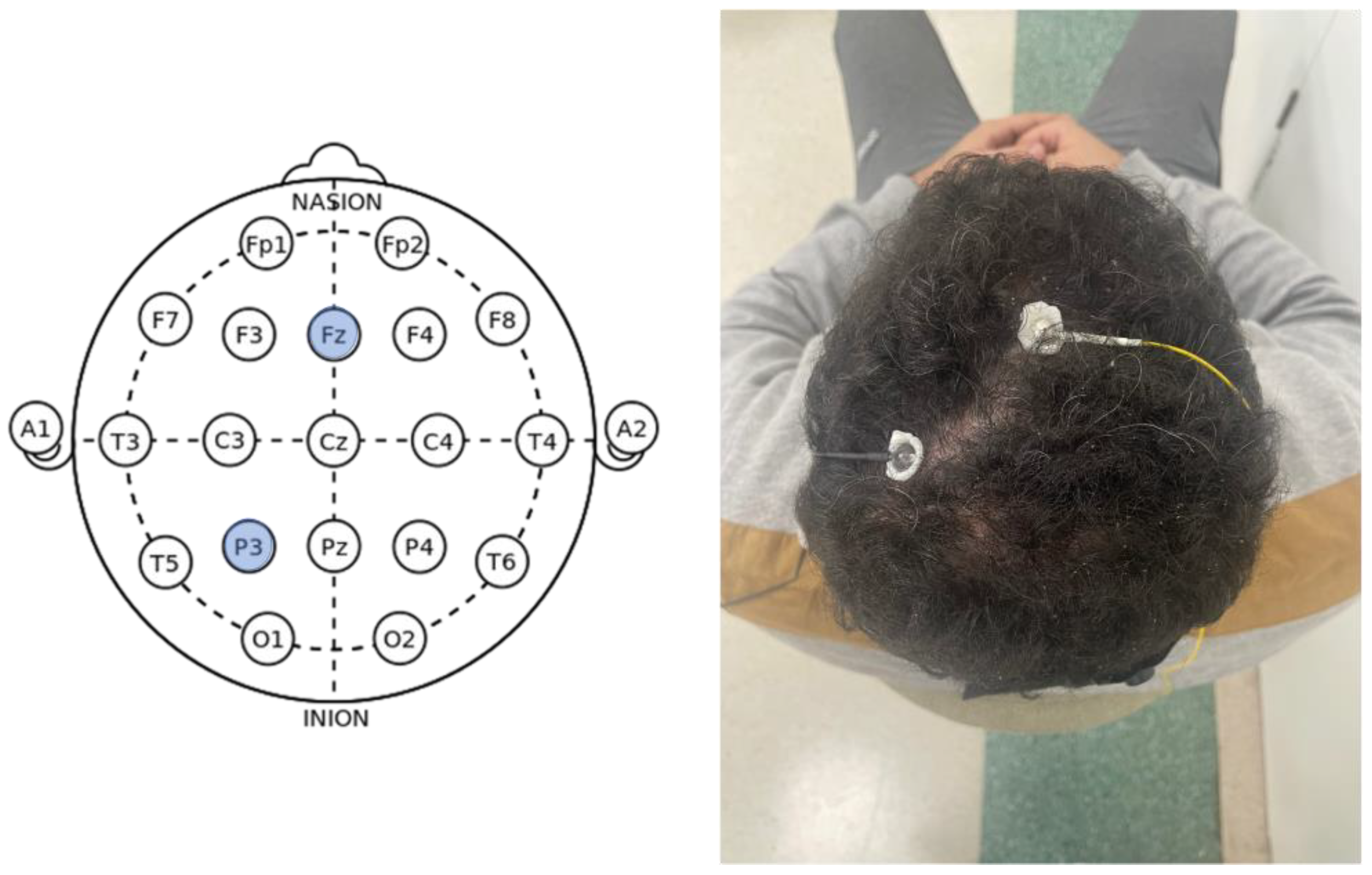
2.2. Neurophysiological Outcome Measures
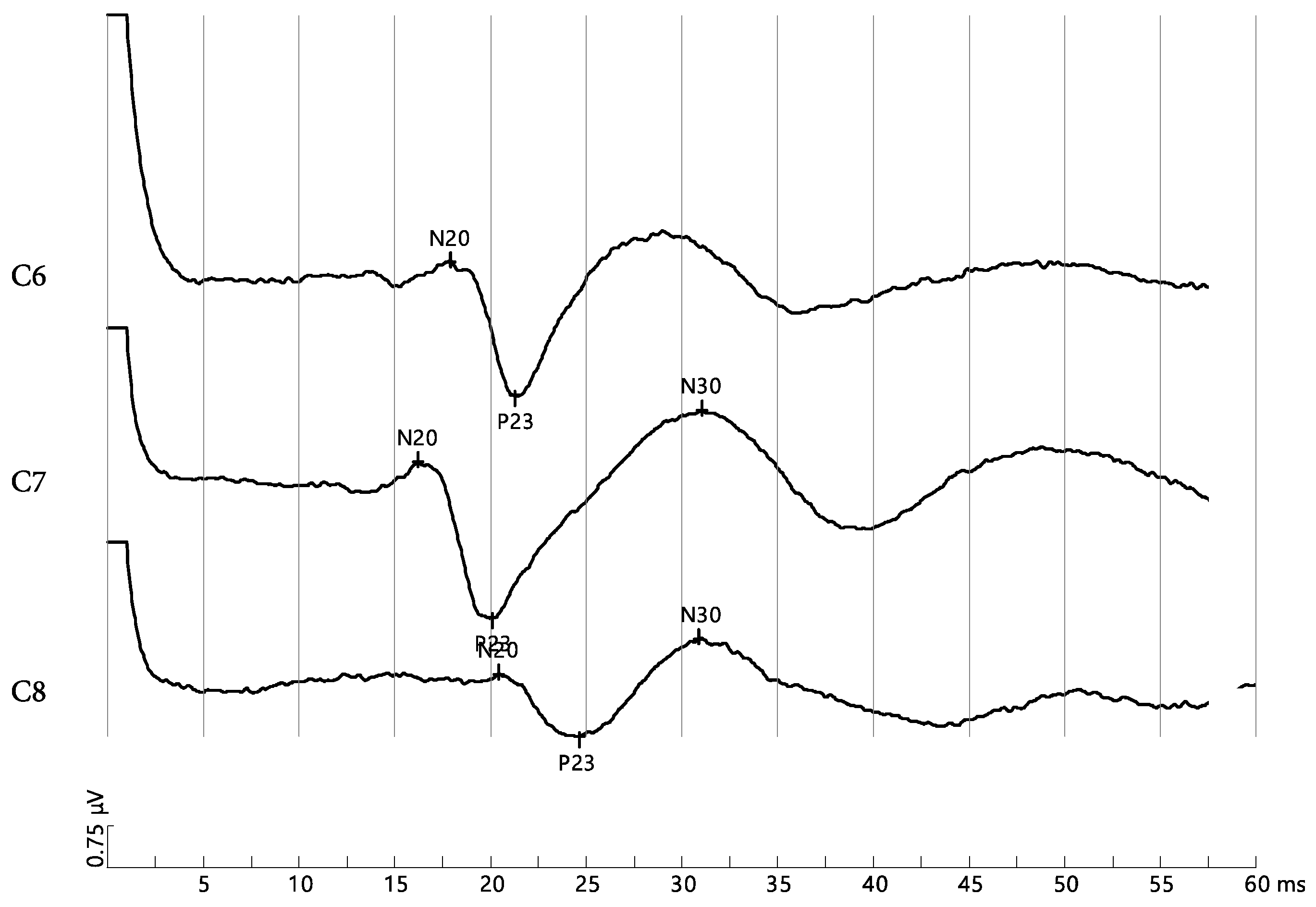
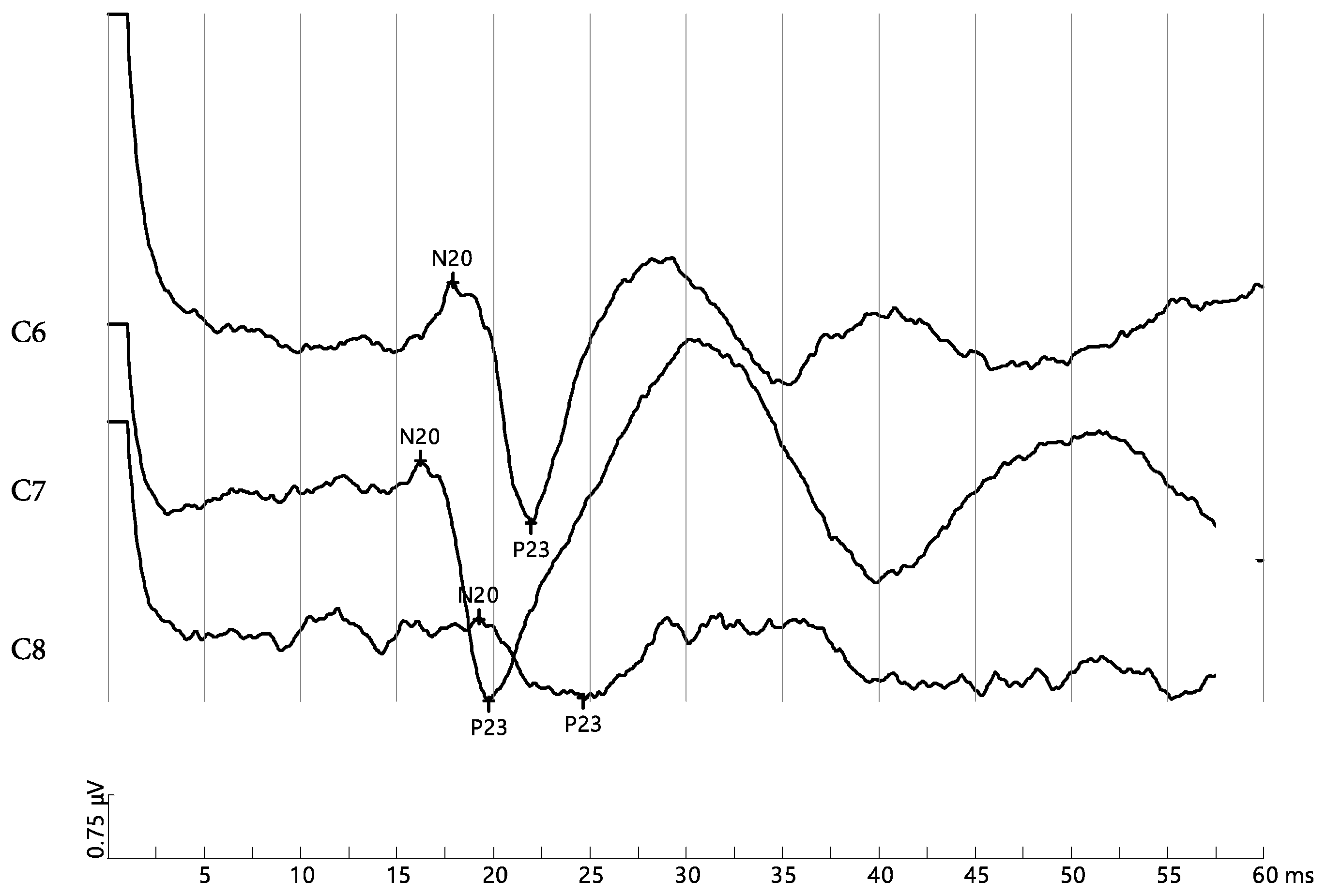
DSSEPs
2.3. Statistical Analysis
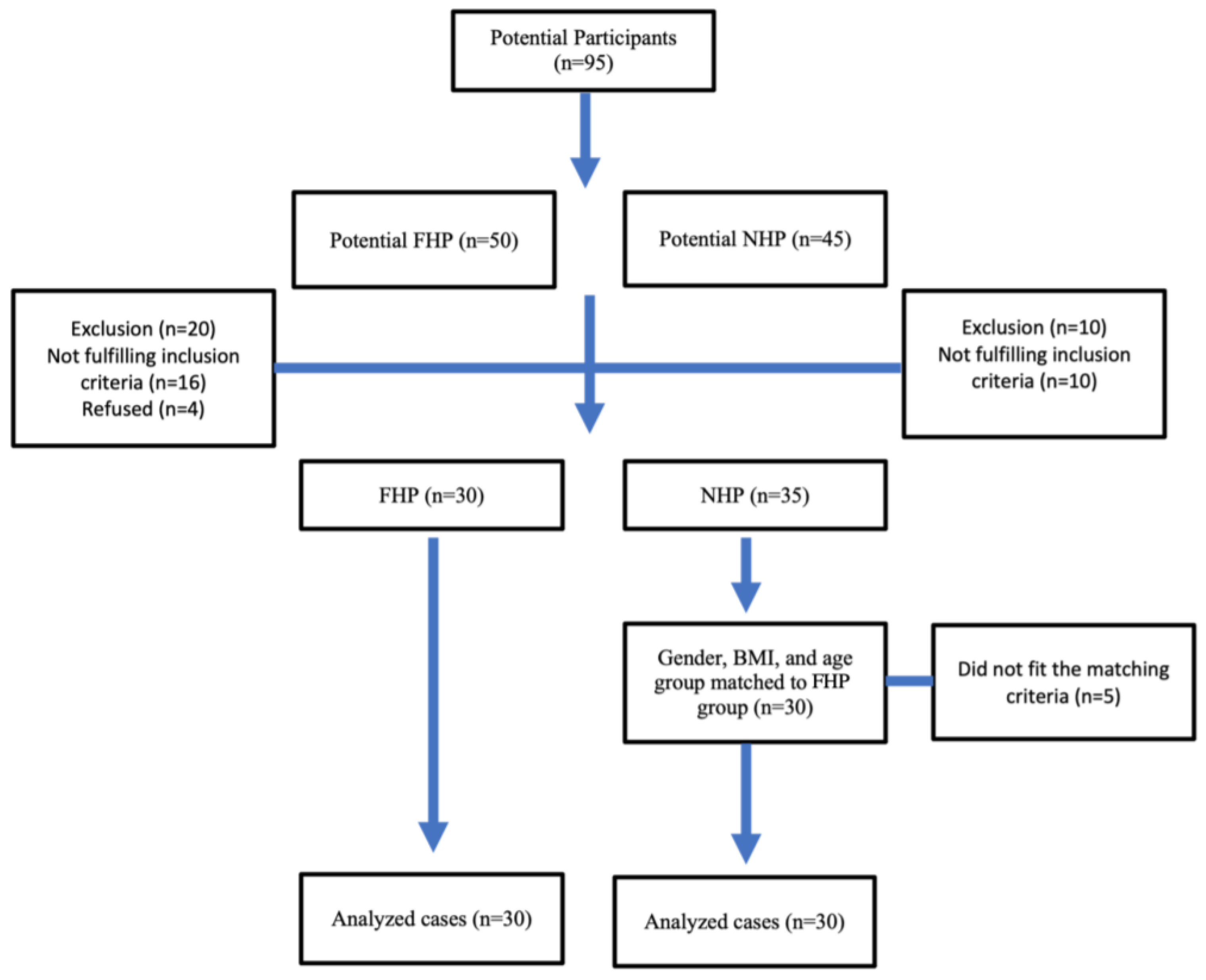
2.3.1. Sample Size
2.3.2. Data Analysis
3. Results
4. Discussion
Study Limitations and Suggestions for Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kallings, L.V.; Blom, V.; Ekblom, B.; Holmlund, T.; Eriksson, J.S.; Andersson, G.; Wallin, P.; Ekblom-Bak, E. Workplace Sitting Is Associated with Self-Reported General Health and Back/Neck Pain: A Cross-Sectional Analysis in 44,978 Employees. BMC Public Health 2021, 21, 875. [Google Scholar] [CrossRef]
- Waongenngarm, P.; van der Beek, A.J.; Akkarakittichoke, N.; Janwantanakul, P. Perceived Musculoskeletal Discomfort and Its Association with Postural Shifts during 4-h Prolonged Sitting in Office Workers. Appl. Ergon. 2020, 89, 103225. [Google Scholar] [CrossRef]
- Pattath, P.; Webb, L. Computer-usage and associated musculoskeletal discomfort in college students. Work 2022, 73, 327–334. [Google Scholar] [CrossRef]
- Yang, F.; Di, N.; Guo, W.W.; Ding, W.B.; Jia, N.; Zhang, H.; Li, D.; Wang, D.; Wang, R.; Zhang, D.; et al. The prevalence and risk factors of work related musculoskeletal disorders among electronics manufacturing workers: A cross-sectional analytical study in China. BMC Public Health 2023, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- De Carvalho, D.E. Spine Biomechanics of Prolonged Sitting: Exploring the Effect Chair Features, Walking Breaks and Spine Manipulation Have on Posture and Perceived Pain in Men and Women; UWSpace, University of Waterloo: Waterloo, ON, Canada, 2015. [Google Scholar]
- Harrison, D.D.; Harrison, S.O.; Croft, A.C.; Harrison, D.E.; Troyanovich, S.J. Sitting biomechanics part I: Review of the literature. J. Manip. Physiol. Ther. 1999, 2, 594–609. [Google Scholar] [CrossRef] [PubMed]
- Hey, H.W.D.; Wong, C.G.; Lau, E.T.C.; Tan, K.A.; Lau, L.L.; Liu, K.P.G.; Wong, H.K. Differences in Erect Sitting and Natural Sitting Spinal Alignment—Insights into a New Paradigm and Implications in Deformity Correction. Spine J. 2017, 17, 183–189. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, K.; O’Sullivan, P.; O’Sullivan, L.; Dankaerts, W. What Do Physiotherapists Consider to Be the Best Sitting Spinal Posture? Man. Ther. 2012, 17, 432–437. [Google Scholar] [CrossRef]
- Ye, J.; Jiang, Z.; Chen, S.; Cheng, R.; Xu, L.; Tsai, T.-Y. Rehabilitation Practitioners’ Perceptions of Optimal Sitting and Standing Posture in Men with Normal Weight and Obesity. Bioengineering 2023, 10, 210. [Google Scholar] [CrossRef]
- Czaprowski, D.; Leszczewska, J.; Sitarski, D.; Rehabilitacji, K.; Rehabilitacji, W.; Fizycznego, W.; Piłsudskiego, J.; Warszawie, A.; Wychowania Fizycznego, W.; Fizjoterapii, W.; et al. Czy Istnieje “Idealna” Pozycja Siedząca? Does “Ideal” Sitting Position Exist? Postep. Rehabil. 2014, 28, 47–54. [Google Scholar] [CrossRef]
- Harrison, D.D.; Harrison, S.O.; Croft, A.C.; Harrison, D.E.; Troyanovich, S.J. Sitting biomechanics, part II: Optimal car driver’s seat and optimal driver′s spinal model. J. Manip. Physiol. Ther. 2000, 23, 37–47. [Google Scholar] [CrossRef]
- Claus, A.P.; Hides, J.A.; Moseley, G.L.; Hodges, P.W. Is “ideal” Sitting Posture Real: Measurement of Spinal Curves in Four Sitting Postures. Man. Ther. 2009, 14, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Douglas, E.C.; Gallagher, K.M. The Influence of a Semi-Reclined Seated Posture on Head and Neck Kinematics and Muscle Activity While Reading a Tablet Computer. Appl. Ergon. 2017, 60, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.W.; Son, S.M.; Lee, K. Changes in Upper-Extremity Muscle Activities Due to Head Position in Subjects with a Forward Head Posture and Rounded Shoulders. J. Phys. Ther. Sci. 2015, 27, 1739–1742. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; O’Leary, S.; Fagan, A.; Jull, G. Recruitment of the Deep Cervical Flexor Muscles during a Postural-Correction Exercise Performed in Sitting. Man. Ther. 2007, 12, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Choi, H. Quantitative Assessment of Co-Contraction in Cervical Musculature. Med. Eng. Phys. 2003, 25, 133–140. [Google Scholar] [CrossRef]
- Eitivipart, A.C.; Viriyarojanakul, S.; Redhead, L. Musculoskeletal disorder and pain associated with smartphone use: A systematic review of biomechanical evidence. Hong Kong Physiother. J. 2018, 38, 77–90. [Google Scholar] [CrossRef]
- Nishikawa, Y.; Watanabe, K.; Chihara, T.; Sakamoto, J.; Komatsuzaki, T.; Kawano, K.; Kobayashi, A.; Inoue, K.; Maeda, N.; Tanaka, S.; et al. Influence of Forward Head Posture on Muscle Activation Pattern of the Trapezius Pars Descendens Muscle in Young Adults. Sci. Rep. 2022, 12, 19484. [Google Scholar] [CrossRef]
- Oliveira, A.C.; Silva, A.G. Neck Muscle Endurance and Head Posture: A Comparison between Adolescents with and without Neck Pain. Man. Ther. 2016, 22, 62–67. [Google Scholar] [CrossRef]
- Harrison, D.E.; Cailliet, R.; Harrison, D.D.; Troyanovich, S.J.; Harrison, S.O. A Review of Biomechanics of the Central Nervous System—Part II: Spinal Cord Strains from Postural Loads. J. Manip. Physiol. Ther. 1999, 22, 322–332. [Google Scholar] [CrossRef]
- Diab, A.A.; Moustafa, I.M. The Efficacy of Forward Head Correction on Nerve Root Function and Pain in Cervical Spondylotic Radiculopathy: A Randomized Trial. Clin. Rehabil. 2012, 26, 351–361. [Google Scholar] [CrossRef]
- Thosar, S.S.; Bielko, S.L.; Wiggins, C.C.; Wallace, J.P. Differences in Brachial and Femoral Artery Responses to Prolonged Sitting. Cardiovasc. Ultrasound 2014, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Youssef, A.; Ahbouch, A.; Tamim, M.; Harrison, D.E. Is Forward Head Posture Relevant to Autonomic Nervous System Function and Cervical Sensorimotor Control? Cross Sectional Study. Gait Posture 2020, 77, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.; Youssef, A.S.A.; Ahbouch, A.; Harrison, D. Demonstration of Autonomic Nervous Function and Cervical Sensorimotor Control after Cervical Lordosis Rehabilitation: A Randomized Controlled Trial. J. Athl. Train. 2021, 56, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Muzyka, I.M.; Estephan, B. Somatosensory Evoked Potentials. Handb. Clin. Neurol. 2019, 160, 523–540. [Google Scholar] [CrossRef]
- Yip, C.H.T.; Chiu, T.T.W.; Poon, A.T.K. The relationship between head posture and severity and disability of patients with neck pain. Man. Ther. 2008, 13, 148–154. [Google Scholar] [CrossRef]
- Singla, D.; Veqar, Z.; Hussain, M.E. Photogrammetric Assessment of Upper Body Posture Using Postural Angles: A Literature Review. J. Chiropr. Med. 2017, 16, 131–138. [Google Scholar] [CrossRef]
- Falla, D.; Jull, G.; Russell, T.; Vicenzino, B.; Hodges, P. Effect of neck exercise on sitting posture in patients with chronic neck pain. Phys. Ther. 2007, 87, 408–417. [Google Scholar] [CrossRef]
- Acharya, J.N.; Hani, A.J.; Cheek, J.; Thirumala, P.; Tsuchida, T.N. American Clinical Neurophysiology Society Guideline 2: Guidelines for Standard Electrode Position Nomenclature. Neurodiagn. J. 2016, 56, 245–252. [Google Scholar] [CrossRef]
- Morley, A.; Hill, L.; Kaditis, A.G. 10-20 System EEG Placement; European Respiratory Society: Lausanne, Switzerland, 2016. [Google Scholar]
- Dunk, N.M.; Callaghan, J.P. Gender-Based Differences in Postural Responses to Seated Exposures. Clin. Biomech. (Bristol. Avon) 2005, 20, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Adams, M.A. Biomechanics of Back Pain. Acupunct. Med. 2004, 22, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Kim, C.; Lee, Y. Correlations between Cervical Lordosis, Forward Head Posture, Cervical ROM and the Strength and Endurance of the Deep Neck Flexor Muscles in College Students. J. Phys. Ther. Sci. 2012, 24, 275–277. [Google Scholar] [CrossRef]
- Ha, S.Y.; Sung, Y.H. Vojta Approach Affects Neck Stability and Static Balance in Sitting Position of Children With Hypotonia. Int. Neurourol. J. 2021, 25, S90–S95, Erratum in Int. Neurourol. J. 2022, 26, 258. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, Z.A.; Alghadir, A.H.; Anwer, S. Efficacy of Deep Cervical Flexor Muscle Training on Neck Pain, Functional Disability, and Muscle Endurance in School Teachers: A Clinical Trial. BioMed Res. Int. 2021, 2021, 7190808. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.; Wang, W.; Wilkinson, T. Changes in deep neck muscle length from the neutral to forward head posture. A cadaveric study using Thiel cadavers. Clin. Anat. 2022, 35, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Larson, B.A.; Nicolaides, E.; Al Zu’bi, B.; Sukkar, N.; Laraki, K.; Matoussi, M.S.; Zaim, K.; Chouchani, C. Examination of the Flexion Relaxation Phenomenon in Erector Spinae Muscles during Short Duration Slumped Sitting. Clin. Biomech. 2002, 17, 353–360. [Google Scholar] [CrossRef]
- Claus, A.P.; Hides, J.A.; Moseley, G.L.; Hodges, P.W. Different Ways to Balance the Spine: Subtle Changes in Sagittal Spinal Curves Affect Regional Muscle Activity. Spine (Phila. Pa. 1976) 2009, 34, E208–E214. [Google Scholar] [CrossRef] [PubMed]
- van Dieën, J.H.; Westebring-van der Putten, E.P.; Kingma, I.; de Looze, M.P. Low-Level Activity of the Trunk Extensor Muscles Causes Electromyographic Manifestations of Fatigue in Absence of Decreased Oxygenation. J. Electromyogr. Kinesiol. 2009, 19, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Granata, K.P.; Slota, G.P.; Wilson, S.E. Influence of Fatigue in Neuromuscular Control of Spinal Stability. Hum. Factors 2004, 46, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Marras, W.S.; Granata, K.P. Changes in Trunk Dynamics and Spine Loading during Repeated Trunk Exertions. Spine (Phila. Pa. 1976) 1997, 22, 2564–2570. [Google Scholar] [CrossRef]
- Kirsch, R.F.; Rymer, W.Z. Neural compensation for fatigue-induced changes in muscle stiffness during perturbations of elbow angle in human. J. Neurophysiol. 1992, 68, 449–470. [Google Scholar] [CrossRef]
- Harrison, D.E.; Jones, E.W.; Janik, T.J.; Harrison, D.D. Evaluation of axial and flexural stresses in the vertebral body cortex and trabecular bone in lordosis and two sagittal cervical translation configurations with an elliptical shell model. J. Manip. Physiol Ther. 2002, 25, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Patwardhan, A.G.; Khayatzadeh, S.; Havey, R.M.; Voronov, L.I.; Smith, Z.A.; Kalmanson, O.; Sears, W. Cervical sagittal balance: A biomechanical perspective can help clinical practice. Eur. Spine J. 2018, 27, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, I.M.; Diab, A.A.; Harrison, D.E. The Efficacy of Cervical Lordosis Rehabilitation for Nerve Root Function and Pain in Cervical Spondylotic Radiculopathy: A Randomized Trial with 2-Year Follow-Up. J. Clin. Med. 2022, 11, 6515. [Google Scholar] [CrossRef] [PubMed]
- Kiebzak, W.P.; Żurawski, A.Ł.; Kosztołowicz, M. Alignment of the Sternum and Sacrum as a Marker of Sitting Body Posture in Children. Int. J. Environ. Res. Public Health 2022, 19, 16287. [Google Scholar] [CrossRef] [PubMed]
- Kiebzak, W.P. Application of Euclidean geometry in the assessment of body posture in a sitting position. Pol. Ann. Med. 2022, 29, 167–171. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Forward Head Group (n = 30) | Normal Head Group (n = 30) | Significance |
|---|---|---|---|
| Age (years) | 20.5 ± 2 | 20 ± 3 | 0.4 |
| Weight (kg) | 61.2 ± 4 | 62.2 ± 5 | 0.3 |
| BMI | 18.4 ± 1.2 | 18.3 ± 1.4 | 0.7 |
| Smoking | |||
| Nonsmoker | 15 | 14 | 0.6 |
| Light Smoker | 10 | 12 | |
| Heavy smoker | 5 | 4 | |
| Sex | |||
| Male | 11 | 11 | - |
| Female | 19 | 19 | |
| CVA | 41.7 ± 2 | 66.9 ± 4.6 | <0.001 |
| Erect | Slouched | Supine | ||
|---|---|---|---|---|
| C6 | FHP | 1.84 ± 0.33 | 2.30 ± 0.38 | 2.50 ± 0.37 |
| NHP | 2.51 ± 0.36 | 1.92 ± 0.30 | 2.60 ± 0.42 | |
| p-value | p < 0.001 | p < 0.001 | p = 0.09 | |
| C.I. | [−0.80, −0.44] | [0.27, 0.62] | [−0.38, 0.03] | |
| C7 | FHP | 1.71 ± 0.23 | 2.24 ± 0.15 | 2.22 ± 0.20 |
| NHP | 2.11 ± 0.38 | 1.60 ± 0.25 | 2.22 ± 0.42 | |
| p-value | p = 0.001 | p < 0.001 | p = 0.72 | |
| C.I. | [−0.50, −0.17] | [0.49, 0.70] | [−0.14, 0.20] | |
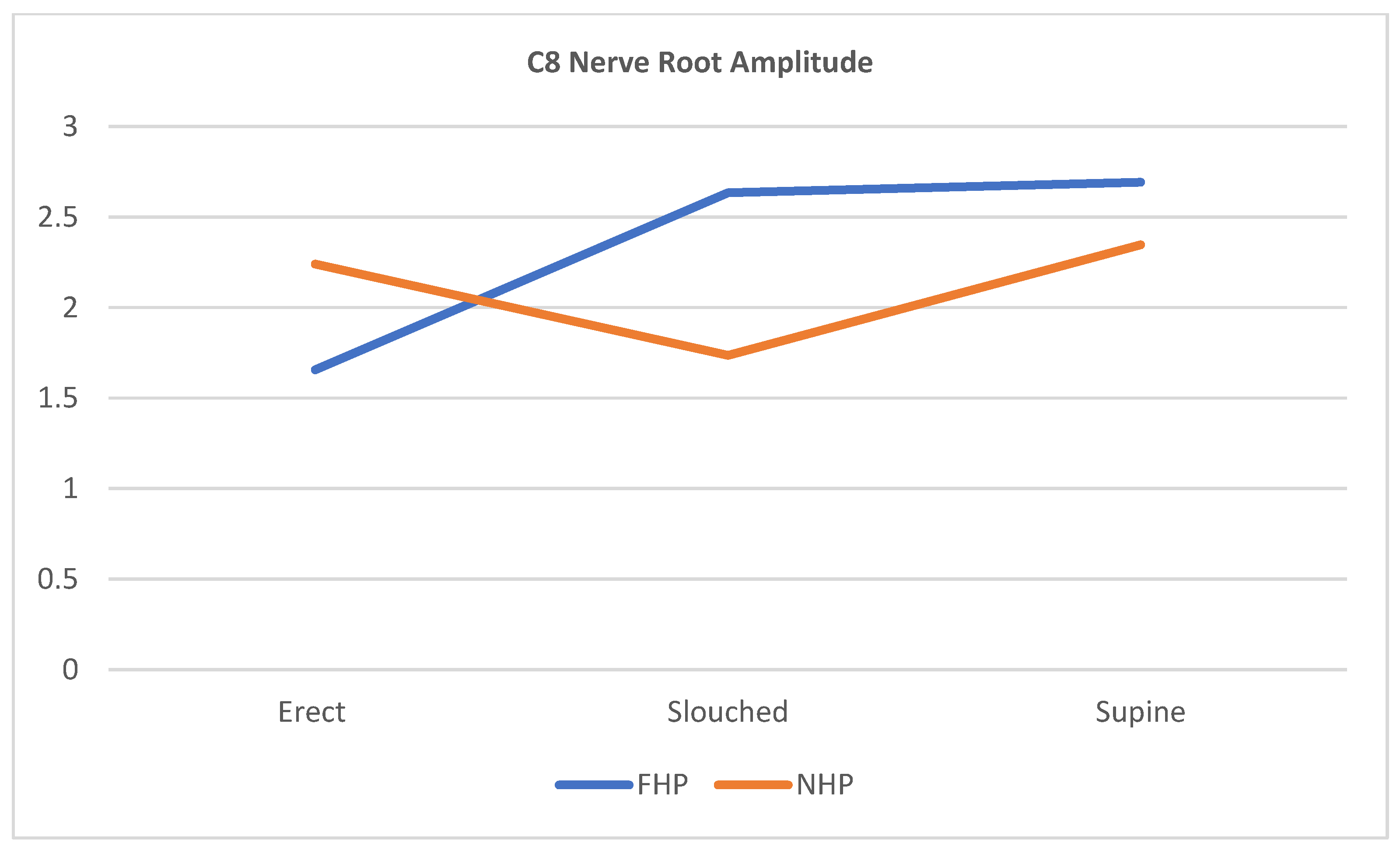
| C8 | FHP | 1.71 ± 0.41 | 2.61 ± 0.56 | 2.73 ± 0.55 |
| NHP | 2.21 ± 0.40 | 1.70 ± 0.31 | 2.34 ± 0.46 | |
| p-value | p < 0.001 | p < 0.001 | p = 0.01 | |
| C.I. | [−0.80, −0.38] | [0.66, 1.13] | [0.08, 0.61] | |
| Tests of Between-Subjects Effects | ||||||
|---|---|---|---|---|---|---|
| Type III Sum of Squares | df | Mean Square | F | Sig. | Partial Eta Squared | |
| C6 amplitude | ||||||
| Corrected Model | 17.272 | 5 | 3.454 | 26.294 | <0.001 | 0.430 |
| Intercept | 917.742 | 1 | 917.742 | 6985.400 | <0.001 | 0.976 |
| Head Posture | 0.629 | 1 | 0.629 | 4.787 | 0.030 | 0.027 |
| Sitting | 8.007 | 2 | 4.004 | 30.474 | <0.001 | 0.259 |
| Head Posture * Sitting | 8.636 | 2 | 4.318 | 32.867 | <0.001 | 0.274 |
| Error | 22.860 | 174 | 0.131 | |||
| C7 amplitude | ||||||
| Corrected Model | 11.095 | 5 | 2.219 | 26.217 | <0.001 | 0.430 |
| Intercept | 726.374 | 1 | 726.374 | 8581.961 | <0.001 | 0.980 |
| Head Posture | 0.431 | 1 | 0.431 | 5.095 | 0.025 | 0.028 |
| Sitting | 4.075 | 2 | 2.037 | 24.070 | <0.001 | 0.217 |
| Head Posture * Sitting | 6.589 | 2 | 3.295 | 38.926 | <0.001 | 0.309 |
| Error | 14.727 | 174 | 0.085 | |||
| C8 amplitude | ||||||
| Corrected Model | 28.892 | 5 | 5.778 | 27.731 | <0.001 | 0.443 |
| Intercept | 885.470 | 1 | 885.470 | 4249.485 | <0.001 | 0.961 |
| Head Posture | 2.185 | 1 | 2.185 | 10.484 | 0.001 | 0.057 |
| Sitting | 9.892 | 2 | 4.946 | 23.737 | <0.001 | 0.214 |
| Head Posture * Sitting | 16.815 | 2 | 8.407 | 40.348 | <0.001 | 0.317 |
| Error | 36.257 | 174 | 0.208 | |||
| (I) Sitting | (J) Sitting | Mean Difference (I–J) | Std. Error | Sig. b | 95% Confidence Interval for | |
|---|---|---|---|---|---|---|
| Difference b | ||||||
| Lower Bound | Upper Bound | |||||
| Dependent Variable: C6 Amplitude | ||||||
| Erect | Slouched | 0.051 | 0.066 | 1 | −0.109 | 0.211 |
| Supine | −0.420 * | 0.066 | <0.001 | −0.580 | −0.260 | |
| Dependent Variable: C7 Amplitude | ||||||
| Erect | Slouched | −0.237 * | 0.083 | 0.015 | −0.439 | −0.036 |
| Supine | −0.572 * | 0.083 | <0.001 | −0.773 | −0.370 | |
| Dependent Variable: C8 Amplitude | ||||||
| Erect | Slouched | −0.012 | 0.053 | 1 | −0.140 | 0.117 |
| Supine | −0.325 * | 0.053 | <0.001 | −0.453 | −0.196 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamel, M.; Moustafa, I.M.; Kim, M.; Oakley, P.A.; Harrison, D.E. Alterations in Cervical Nerve Root Function during Different Sitting Positions in Adults with and without Forward Head Posture: A Cross-Sectional Study. J. Clin. Med. 2023, 12, 1780. https://doi.org/10.3390/jcm12051780
Kamel M, Moustafa IM, Kim M, Oakley PA, Harrison DE. Alterations in Cervical Nerve Root Function during Different Sitting Positions in Adults with and without Forward Head Posture: A Cross-Sectional Study. Journal of Clinical Medicine. 2023; 12(5):1780. https://doi.org/10.3390/jcm12051780
Chicago/Turabian StyleKamel, Maryam, Ibrahim M. Moustafa, Meeyoung Kim, Paul A. Oakley, and Deed E. Harrison. 2023. "Alterations in Cervical Nerve Root Function during Different Sitting Positions in Adults with and without Forward Head Posture: A Cross-Sectional Study" Journal of Clinical Medicine 12, no. 5: 1780. https://doi.org/10.3390/jcm12051780
APA StyleKamel, M., Moustafa, I. M., Kim, M., Oakley, P. A., & Harrison, D. E. (2023). Alterations in Cervical Nerve Root Function during Different Sitting Positions in Adults with and without Forward Head Posture: A Cross-Sectional Study. Journal of Clinical Medicine, 12(5), 1780. https://doi.org/10.3390/jcm12051780