

Procedures in Fecal Microbiota Transplantation for Treating Irritable Bowel Syndrome: Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Selection Criteria
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias Assessment in Individual Studies
2.7. Quantitative Synthesis
2.8. Grading the Evidence
3. Results
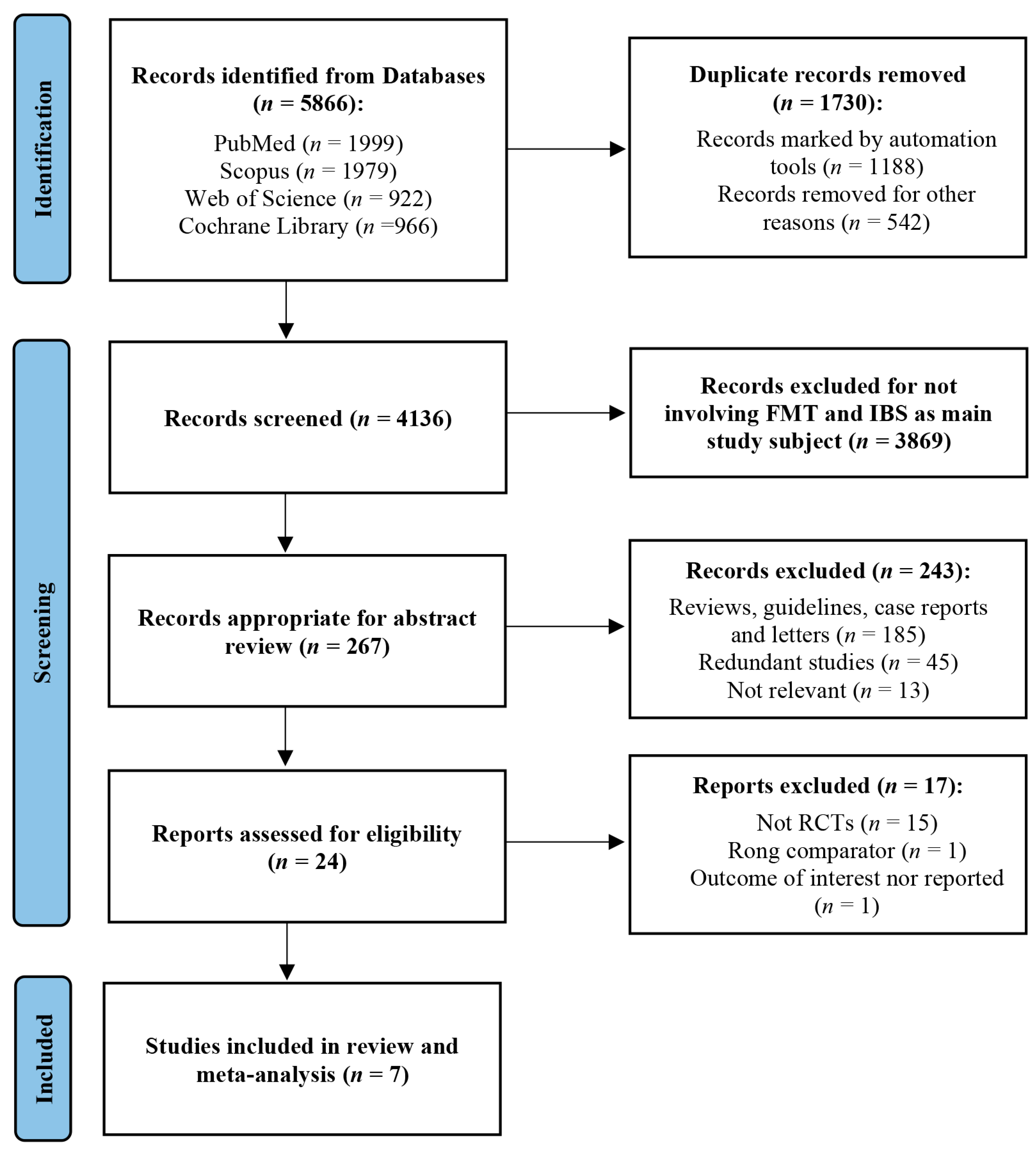
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
3.4. GRADE Assessment
3.5. IBS Symptoms Improvement
3.5.1. Delivery Method
3.5.2. Dose
3.5.3. Fresh vs. Frozen
3.5.4. Bowel Preparation
3.5.5. IBS Subtype
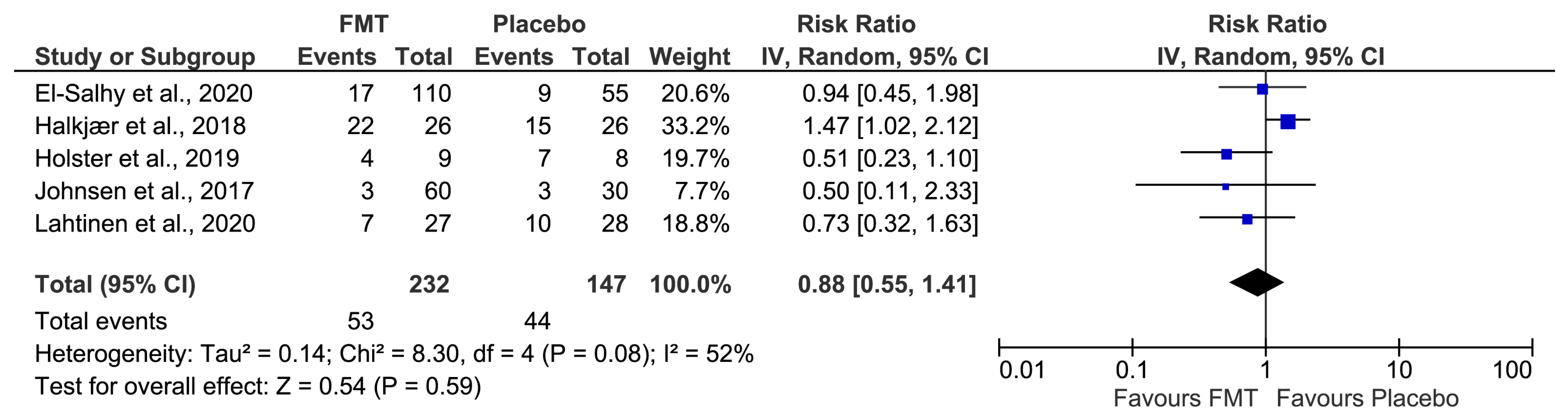
3.6. Safety of FMT in IBS
4. Discussion
4.1. Summary of Evidence
4.2. Global Considerations about Randomized Controlled Trials Evaluating the FMT Efficacy on IBS Treatment
4.3. Strengths and Limitations of This Study
4.4. Future RCTs Assessing FMT Efficacy for IBS Treatment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel Disorders. Gastroenterology 2016, 150, 1393–1407.e5. [Google Scholar] [CrossRef]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef]
- Oka, P.; Parr, H.; Barberio, B.; Black, C.J.; Savarino, E.V.; Ford, A.C. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 908–917. [Google Scholar] [CrossRef]
- Black, C.J.; Ford, A.C. Global burden of irritable bowel syndrome: Trends, predictions and risk factors. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 473–486. [Google Scholar] [CrossRef]
- Sperber, A.D.; Dumitrascu, D.; Fukudo, S.; Gerson, C.; Ghoshal, U.C.; Gwee, K.A.; Hungin, A.P.S.; Kang, J.Y.; Minhu, C.; Schmulson, M.; et al. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome Foundation working team literature review. Gut 2017, 66, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Vasant, D.H.; Paine, P.A.; Black, C.J.; Houghton, L.A.; Everitt, H.A.; Corsetti, M.; Agrawal, A.; Aziz, I.; Farmer, A.D.; Eugenicos, M.P.; et al. British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. Gut 2021, 70, 1214–1240. [Google Scholar] [CrossRef] [PubMed]
- Blake, M.R.; Raker, J.M.; Whelan, K. Validity and reliability of the Bristol Stool Form Scale in healthy adults and patients with diarrhoea-predominant irritable bowel syndrome. Aliment. Pharmacol. Ther. 2016, 44, 693–703. [Google Scholar] [CrossRef]
- Chey, W.D.; Kurlander, J.; Eswaran, S. Irritable bowel syndrome: A clinical review. JAMA 2015, 313, 949–958. [Google Scholar] [CrossRef]
- Kassinen, A.; Krogius-Kurikka, L.; Makivuokko, H.; Rinttila, T.; Paulin, L.; Corander, J.; Malinen, E.; Apajalahti, J.; Palva, A. The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Gastroenterology 2007, 133, 24–33. [Google Scholar] [CrossRef]
- Ringel-Kulka, T.; Benson, A.K.; Carroll, I.M.; Kim, J.; Legge, R.M.; Ringel, Y. Molecular characterization of the intestinal microbiota in patients with and without abdominal bloating. Am. J. Physiol. Gastrointest. Liver Physiol. 2016, 310, G417–G426. [Google Scholar] [CrossRef]
- Jalanka, J.; Salonen, A.; Fuentes, S.; de Vos, W.M. Microbial signatures in post-infectious irritable bowel syndrome—Toward patient stratification for improved diagnostics and treatment. Gut Microbes 2015, 6, 364–369. [Google Scholar] [CrossRef]
- Tap, J.; Derrien, M.; Tornblom, H.; Brazeilles, R.; Cools-Portier, S.; Dore, J.; Storsrud, S.; Le Neve, B.; Ohman, L.; Simren, M. Identification of an Intestinal Microbiota Signature Associated With Severity of Irritable Bowel Syndrome. Gastroenterology 2017, 152, 111–123.e8. [Google Scholar] [CrossRef] [PubMed]
- Clemente, J.C.; Manasson, J.; Scher, J.U. The role of the gut microbiome in systemic inflammatory disease. BMJ 2018, 360, j5145. [Google Scholar] [CrossRef] [PubMed]
- Thaiss, C.A.; Zmora, N.; Levy, M.; Elinav, E. The microbiome and innate immunity. Nature 2016, 535, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Allegretti, J.R.; Kassam, Z.; Osman, M.; Budree, S.; Fischer, M.; Kelly, C.R. The 5D framework: A clinical primer for fecal microbiota transplantation to treat Clostridium difficile infection. Gastrointest. Endosc. 2018, 87, 18–29. [Google Scholar] [CrossRef]
- Zhao, H.J.; Zhang, X.J.; Zhang, N.N.; Yan, B.; Xu, K.K.; Peng, L.H.; Pan, F. Fecal Microbiota Transplantation for Patients With Irritable Bowel Syndrome: A Meta-Analysis of Randomized Controlled Trials. Front. Nutr. 2022, 9, 890357. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.; Chen, V.L.; Steiner, C.A.; Berinstein, J.A.; Eswaran, S.; Waljee, A.K.; Higgins, P.D.R.; Owyang, C. Efficacy of Fecal Microbiota Transplantation in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2019, 114, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Lv, L.; Wang, C. Efficacy of Fecal Microbiota Transplantation in Irritable Bowel Syndrome: A Meta-Analysis of Randomized Controlled Trials. Front. Cell Infect Microbiol. 2022, 12, 827395. [Google Scholar] [CrossRef]
- Green, J.E.; Davis, J.A.; Berk, M.; Hair, C.; Loughman, A.; Castle, D.; Athan, E.; Nierenberg, A.A.; Cryan, J.F.; Jacka, F.; et al. Efficacy and safety of fecal microbiota transplantation for the treatment of diseases other than Clostridium difficile infection: A systematic review and meta-analysis. Gut Microbes 2020, 12, 1–25. [Google Scholar] [CrossRef]
- Ianiro, G.; Eusebi, L.H.; Black, C.J.; Gasbarrini, A.; Cammarota, G.; Ford, A.C. Systematic review with meta-analysis: Efficacy of faecal microbiota transplantation for the treatment of irritable bowel syndrome. Aliment. Pharmacol. Ther. 2019, 50, 240–248. [Google Scholar] [CrossRef]
- Myneedu, K.; Deoker, A.; Schmulson, M.J.; Bashashati, M. Fecal microbiota transplantation in irritable bowel syndrome: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2019, 7, 1033–1041. [Google Scholar] [CrossRef]
- Samuthpongtorn, C.; Kantagowit, P.; Pittayanon, R.; Patcharatrakul, T.; Gonlachanvit, S. Fecal microbiota transplantation in irritable bowel syndrome: A meta-analysis of randomized controlled trials. Front. Med. 2022, 9, 1039284. [Google Scholar] [CrossRef] [PubMed]
- Elhusein, A.M.; Fadlalmola, H.A. Efficacy of Fecal Microbiota Transplantation in Irritable Bowel Syndrome Patients: An Updated Systematic Review and Meta-Analysis. Gastroenterol. Nurs. 2022, 45, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: 2022. Available online: www.training.cochrane.org/handbook (accessed on 8 March 2022).
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Irvine, E.J.; Tack, J.; Crowell, M.D.; Gwee, K.A.; Ke, M.; Schmulson, M.J.; Whitehead, W.E.; Spiegel, B. Design of Treatment Trials for Functional Gastrointestinal Disorders. Gastroenterology 2016, 150, 1469–1480.e1. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Aroniadis, O.C.; Brandt, L.J.; Oneto, C.; Feuerstadt, P.; Sherman, A.; Wolkoff, A.W.; Kassam, Z.; Sadovsky, R.G.; Elliott, R.J.; Budree, S.; et al. Faecal microbiota transplantation for diarrhoea-predominant irritable bowel syndrome: A double-blind, randomised, placebo-controlled trial. Lancet Gastroenterol. Hepatol. 2019, 4, 675–685. [Google Scholar] [CrossRef]
- El-Salhy, M.; Hatlebakk, J.G.; Gilja, O.H.; Brathen Kristoffersen, A.; Hausken, T. Efficacy of faecal microbiota transplantation for patients with irritable bowel syndrome in a randomised, double-blind, placebo-controlled study. Gut 2020, 69, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Halkjaer, S.I.; Christensen, A.H.; Lo, B.Z.S.; Browne, P.D.; Gunther, S.; Hansen, L.H.; Petersen, A.M. Faecal microbiota transplantation alters gut microbiota in patients with irritable bowel syndrome: Results from a randomised, double-blind placebo-controlled study. Gut 2018, 67, 2107–2115. [Google Scholar] [CrossRef]
- Holster, S.; Lindqvist, C.M.; Repsilber, D.; Salonen, A.; de Vos, W.M.; Konig, J.; Brummer, R.J. The Effect of Allogenic Versus Autologous Fecal Microbiota Transfer on Symptoms, Visceral Perception and Fecal and Mucosal Microbiota in Irritable Bowel Syndrome: A Randomized Controlled Study. Clin. Transl. Gastroenterol. 2019, 10, e00034. [Google Scholar] [CrossRef] [PubMed]
- Holvoet, T.; Joossens, M.; Vazquez-Castellanos, J.F.; Christiaens, E.; Heyerick, L.; Boelens, J.; Verhasselt, B.; van Vlierberghe, H.; De Vos, M.; Raes, J.; et al. Fecal Microbiota Transplantation Reduces Symptoms in Some Patients With Irritable Bowel Syndrome With Predominant Abdominal Bloating: Short- and Long-term Results From a Placebo-Controlled Randomized Trial. Gastroenterology 2021, 160, 145–157.e8. [Google Scholar] [CrossRef]
- Johnsen, P.H.; Hilpusch, F.; Cavanagh, J.P.; Leikanger, I.S.; Kolstad, C.; Valle, P.C.; Goll, R. Faecal microbiota transplantation versus placebo for moderate-to-severe irritable bowel syndrome: A double-blind, randomised, placebo-controlled, parallel-group, single-centre trial. Lancet Gastroenterol. Hepatol. 2018, 3, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, P.; Jalanka, J.; Hartikainen, A.; Mattila, E.; Hillila, M.; Punkkinen, J.; Koskenpato, J.; Anttila, V.J.; Tillonen, J.; Satokari, R.; et al. Randomised clinical trial: Faecal microbiota transplantation versus autologous placebo administered via colonoscopy in irritable bowel syndrome. Aliment. Pharmacol. Ther. 2020, 51, 1321–1331. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines & HealthCare. Guide to the Quality and Safety of Tissues and Cells for Human Application, 4th ed. 2019. Available online: https://www.edqm.eu/en/guide-to-the-quality-and-safety-of-tissues-and-cells-for-human-application1 (accessed on 8 March 2022).
- Cammarota, G.; Ianiro, G.; Tilg, H.; Rajilic-Stojanovic, M.; Kump, P.; Satokari, R.; Sokol, H.; Arkkila, P.; Pintus, C.; Hart, A.; et al. European consensus conference on faecal microbiota transplantation in clinical practice. Gut 2017, 66, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Bahl, M.I.; Bergstrom, A.; Licht, T.R. Freezing fecal samples prior to DNA extraction affects the Firmicutes to Bacteroidetes ratio determined by downstream quantitative PCR analysis. FEMS Microbiol. Lett. 2012, 329, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Toscano, M.; De Grandi, R.; Casini, V.; Pace, F. Persisting changes of intestinal microbiota after bowel lavage and colonoscopy. Eur. J. Gastroenterol. Hepatol. 2016, 28, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Nagata, N.; Tohya, M.; Fukuda, S.; Suda, W.; Nishijima, S.; Takeuchi, F.; Ohsugi, M.; Tsujimoto, T.; Nakamura, T.; Shimomura, A.; et al. Effects of bowel preparation on the human gut microbiome and metabolome. Sci. Rep. 2019, 9, 4042. [Google Scholar] [CrossRef]
- Pimentel, M.; Saad, R.J.; Long, M.D.; Rao, S.S.C. ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth. Am. J. Gastroenterol. 2020, 115, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.; Biglari, M.; Nasseri Moghaddam, S. Post-infectious Irritable Bowel Syndrome: A Narrative Review. Middle East J. Dig. Dis. 2019, 11, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Sundin, J.; Rangel, I.; Fuentes, S.; Heikamp-de Jong, I.; Hultgren-Hornquist, E.; de Vos, W.M.; Brummer, R.J. Altered faecal and mucosal microbial composition in post-infectious irritable bowel syndrome patients correlates with mucosal lymphocyte phenotypes and psychological distress. Aliment. Pharmacol. Ther. 2015, 41, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D. Food: The Main Course to Wellness and Illness in Patients with Irritable Bowel Syndrome. Am. J. Gastroenterol. 2016, 111, 366–371. [Google Scholar] [CrossRef]
- Weersma, R.K.; Zhernakova, A.; Fu, J. Interaction between drugs and the gut microbiome. Gut 2020, 69, 1510–1519. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country/Setting | Sample Size (n Analyzed) | Median or Mean Age 1/Years 2 | % Females 2 | Diagnostic Criteria Used for IBS and Subtypes 2 of IBS Recruited | FMT Route | Intervention/Dose | Control |
|---|---|---|---|---|---|---|---|---|
| Aroniadis et al., 2019 [31] | USA/Primary, secondary, and tertiary care (three centers) | 48 (45) | I: 33 (27–48) C: 48 (28–48) | I: 36 C: 39 | ROME III; 100% IBS-D | Oral capsules | 75 FMT capsules containing 50 g feces from 1 of 4 donors | Placebo capsules not containing fecal microbiota |
| Halkjaer et al., 2018 [33] | Denmark/Tertiary care (two centers) | 52 (46) | I: 37.3 (12.5) C: 35.5 (10.6) | I: 68 C: 69 | ROME III; 33.3% IBS-C, 29.4% IBS-D, 37.3% IBS-M | Oral capsules | 300 FMT capsules containing 144 g fecal matter derived from 600 g pooled donor feces (4 donors) | Placebo capsules not containing fecal microbiota |
| Holster et al., 2019 [34] | Sweden/Tertiary care (single center) | 17 (16) | I: 34 (27–49) C: 39 (33–43) | I: 52 C: 65 | ROME III; 25.0% IBS-C, 56.2% IBS-D, 18.8% IBS-M | Colonoscopy | 30 g donor feces from 1 of 2 donors mixed with isotonic saline and 10% glycerol to a final volume of 150 mL | Autologous |
| Johnsen et al., 2017 [36] | Norway/Primary care (single center) | 90 (83) | I: 44 (33–54) C: 45 (34–57) | I: 65 C: 68 | ROME III; 53.0% IBS-D, 47.0% IBS-M | Colonoscopy | 50–80 g pooled donor feces (2 donors) mixed with 200 mL isotonic saline and 50 mL 85% glycerol | Autologous |
| Lahtinen et al., 2020 [37] | Finland/Tertiary care (three centers) | 55 (49) | I: 47.3 (16.8) C: 46.3 (14.3) | I: 52 C: 65 | ROME IV; 51% IBS-D, 4.3% IBS-M, 34.7% IBS-O or IBS-U | Colonoscopy | 30 g donor feces (1 donor) homogenized in 100–200 mL of water | Autologous |
| El-Salhy et al., 2020 [32] | Norway/Tertiary care (single center) | 165 (164) | I60: 39.3 (13.2) I30: 39.2 (12.4) C: 41.2 (13.7) | I: 79 C: 85 | ROME IV; 37.8% IBS-C, 38.4% IBS-D, 23.8% IBS-M | Gastroscopy | 30 g and 60 g donor feces (1 single “super donor”) mixed with 40 mL isotonic saline | Autologous |
| Holvoet et al., 2021 [35] | Belgium/Tertiary care (single center) | 64 (62) | I: 40 (25–59) C: 36 (18–63) | I: 69 C: 41 | ROME III; 100% IBS-D or IBS-M | Nasojejunal tube | 50–80 g pooled donor feces (2 donors) mixed with isotonic saline and glycerol | Autologous |
| Study | Frequency/Duration | Follow-Up | Primary Outcome | Secondary Outcomes | Main Findings | Risk of Bias |
|---|---|---|---|---|---|---|
| Aroniadis et al., 2019 [31] | 25 capsules daily × 3 days 1 | 6 mo. | Decrease in IBS-SSS ≥ 50 points at 12 wk. | IBS-QOL, HADS, Bristol stool scale scores and microbiota profiles. | No significant differences in IBS symptoms improvement, QOL, depression, anxiety, stool consistency and microbiome profiles between intervention and control groups. Significant similarity 2 between the patient and donor microbiota 1 wk after FMT. | Unclear |
| Halkjaer et al., 2018 [33] | 25 capsules daily × 12 days | 6 mo. | Decrease in IBS-SSS ≥ 50 points at 12 wk. | IBS-QOL and microbiota diversity. | Significant improvement in IBS symptoms and QOL in the placebo group compared to the intervention group. Significant similarity4 between the patient and donor microbiota after FMT. | Unclear |
| Holster et al., 2019 [34] | Once | 6 mo. | Decrease in gastrointestinal symptom rating scale-IBS of ≥30% | IBS-SSS, IBS-QOL, HADS, visceral sensitivity and microbiota composition. | No significant differences in IBS symptoms improvement, QOL, anxiety and visceral sensitivity between intervention and control groups. No significant similarity 2 between the patient and donor microbiota after FMT. | Low |
| Johnsen et al., 2017 [36] | Once | 12 mo. | Decrease in IBS-SSS > 75 points at 12 wk. | Decrease in IBS-SSS > 75 points at 12 mo. | Significant improvement in IBS symptoms in the intervention group compared to the control group. | Low |
| Lahtinen et al., 2020 [37] | Once | 12 mo. | Decrease in IBS-SSS ≥ 50 points at 12 wk. | IBS-QOL, BDI, BAI, microbiota composition and fecal water content. | No significant differences in IBS symptoms improvement, QOL, depression, anxiety and stool consistency between intervention and control groups. Significant similarity 4 between patient and donor microbiota after FMT at all points after intervention, significantly higher in the intervention group compared to the control group. | Unclear |
| El-Salhy et al., 2019 [32] | Once | 4 mo. | Decrease in IBS-SSS ≥ 50 points at 12 wk. | IBS-QOL, FAS, SF-NDI, dysbiosis index and microbiota profiles. | Significant improvement in IBS symptoms, QOL, fatigue and dyspepsia in the intervention group compared to the control group. Significant changes in microbiota abundance 3 in the intervention group but not in the placebo group. | Low |
| Holvoet et al., 2021 [35] | Once 1 | 12 mo. | Improvement in overall symptoms and abdominal bloating at 12 wk. | IBS symptom scores by using daily diary, IBS-QOL and microbiota composition. | Significant improvement in IBS symptoms and QOL in the intervention group compared to the control group. No significant similarity between the patient and donor microbiota after FMT. | High |
| Components | Nº of Participants | FMT | Placebo | Relative Effect (95% CI) | Absolute Effect (95% CI) | Certainty of the Evidence | Importance |
|---|---|---|---|---|---|---|---|
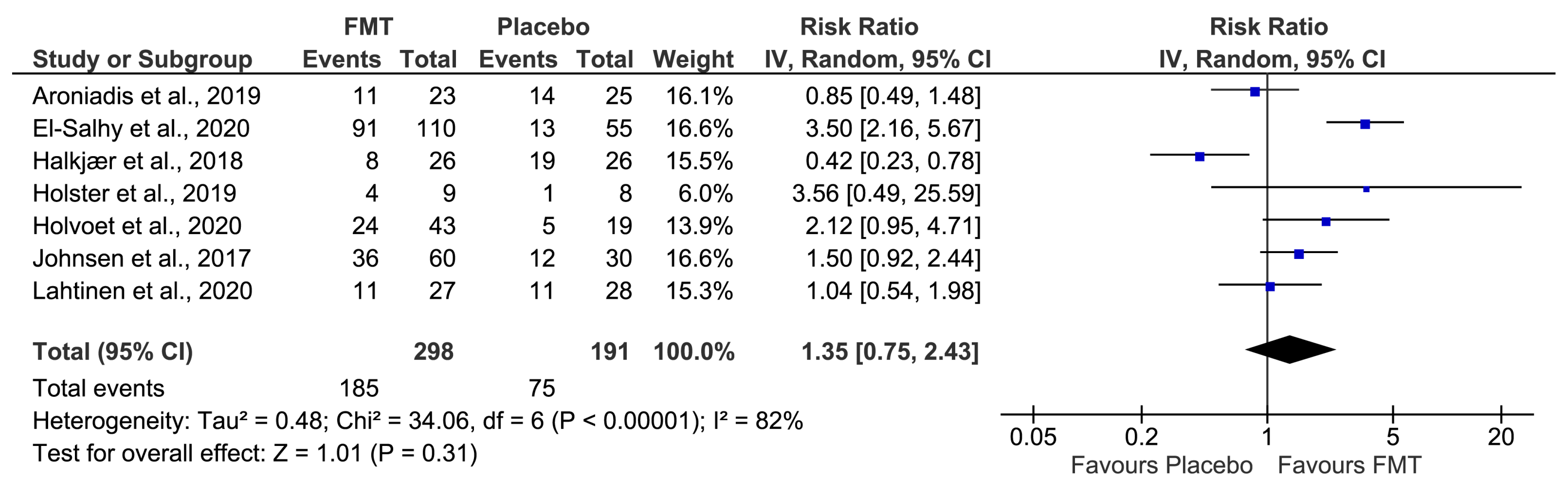
| Overall symptoms improvement | 489 (7 RCTs) | 185/298 (62.1%) | 75/191 (39.3%) | RR 1.35 (0.75 to 2.43) | 137 more per 1000 (from 98 fewer to 562 more) | ⊕◯◯◯ Very low a,b,c | CRITICAL |
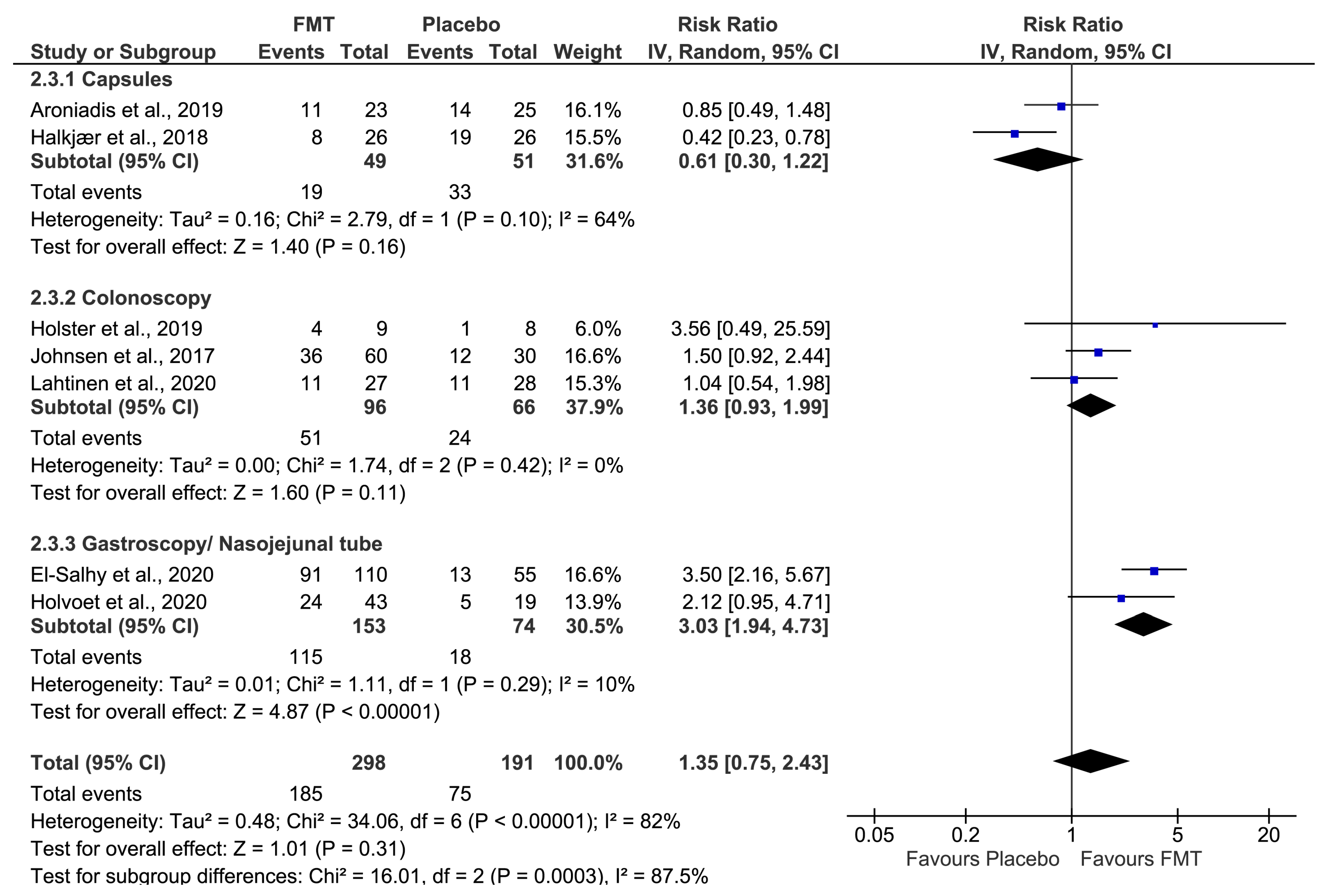
| Symptoms improvement via oral capsules | 100 (2 RCTs) | 19/49 (38.8%) | 33/51 (64.7%) | RR 0.61 (0.30 to 1.22) | 252 fewer per 1000 (from 453 fewer to 142 more) | ⊕◯◯◯ Very low a,b,c | CRITICAL |
| Symptoms improvement via colonoscopy | 162 (3 RCTs) | 51/96 (53.1%) | 24/66 (36.4%) | RR 1.36 (0.93 to 1.99) | 131 more per 1000 (from 25 fewer to 360 more) | ⊕⊕⊕◯ Moderate a | CRITICAL |
| Symptoms improvement via gastroscopy or nasojejunal tube | 227 (2 RCTs) | 115/153 (75.2%) | 18/74 (24.3%) | RR 3.03 (1.94 to 4.73) | 494 more per 1000 (from 229 more to 907 more) | ⊕⊕◯◯ Low a,b | CRITICAL |
| No. of RCTs | No. of Patients | RR (95% CI) | I2 | p1 | |
|---|---|---|---|---|---|
| All studies | 7 | 489 | 1.35 (0.75–2.43) | 82% | |
| Method of administration | 0.0003 | ||||
| Capsules [31,33] | 2 | 100 | 0.61 (0.30–1.22) | 64% | |
| Colonoscopy [34,36,37] | 3 | 162 | 1.36 (0.93–1.99) | 0% | |
| Gastroscopy/Nasojejunal tube [32,35] | 2 | 227 | 3.03 (1.94–4.73) ** | 10% | |
| Total dose | 0.76 | ||||
| ≥50 g [32,33,36] | 3 | 252 | 1.35 (0.42–4.37) | 93% | |
| <50 g [31,32,34,35,37] | 5 | 292 | 1.67 (0.89–3.15) | 74% | |
| FMT sample preparation | 0.44 | ||||
| Fresh [34,35] | 2 | 79 | 2.28 (1.09–4.78) * | 0% | |
| Frozen [31,32,33,37] | 4 | 320 | 1.08 (0.43–2.72) | 90% | |
| Both [36] | 1 | 90 | 1.50 (0.92–2.44) | - | |
| Bowel preparation | 0.80 | ||||
| With bowel preparation [33,34,35,36] | 4 | 221 | 1.26 (0.53–2.97) | 80% | |
| Without bowel preparation [31,32,36] | 3 | 268 | 1.48 (0.58–3.75) | 88% | |
| IBS subtypes | 0.77 | ||||
| With constipation type [32,33,34] | 3 | 234 | 1.61 (0.30–8.69) | 93% | |
| Without constipation type [31,35,36,37] | 4 | 255 | 1.25 (0.87–1.79) | 32% |
| No. of RCTs | No. of Patients | RR (95% CI) | I2 | p1 | |
|---|---|---|---|---|---|
| All studies | 5 | 389 | 1.94 (1.17–3.22) | 63% | |
| Total dose | 0.8 | ||||
| ≥50 g [32,36] | 2 | 200 | 2.38 (0.96–5.87) | 86% | |
| <50 g [32,34,35,37] | 4 | 244 | 2.06 (1.10–3.88) * | 61% | |
| FMT sample preparation | 0.64 | ||||
| Fresh [34,35] | 2 | 79 | 2.28 (1.09–4.78) * | 0% | |
| Frozen [31,32,33,37] | 2 | 220 | 1.94 (0.59–6.40) | 89% | |
| Both [36] | 1 | 90 | 1.50 (0.92–2.44) | - | |
| Bowel preparation | 0.84 | ||||
| With bowel preparation [34,35,36] | 3 | 169 | 1.70 (1.13–2.55) * | 0% | |
| Without bowel preparation [32,37] | 2 | 220 | 1.94 (0.59–6.40) | 89% | |
| IBS subtypes | 0.003 | ||||
| With constipation type [32,34] | 2 | 182 | 3.50 (2.19—5.60) ** | 0% | |
| Without constipation type [35,36,37] | 3 | 207 | 1.44 (1.02–2.04) * | 0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, T.; Rodrigues Fialho, S.; Araújo, J.R.; Rocha, R.; Moreira-Rosário, A. Procedures in Fecal Microbiota Transplantation for Treating Irritable Bowel Syndrome: Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1725. https://doi.org/10.3390/jcm12051725
Rodrigues T, Rodrigues Fialho S, Araújo JR, Rocha R, Moreira-Rosário A. Procedures in Fecal Microbiota Transplantation for Treating Irritable Bowel Syndrome: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(5):1725. https://doi.org/10.3390/jcm12051725
Chicago/Turabian StyleRodrigues, Tânia, Sofia Rodrigues Fialho, João Ricardo Araújo, Rita Rocha, and André Moreira-Rosário. 2023. "Procedures in Fecal Microbiota Transplantation for Treating Irritable Bowel Syndrome: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 5: 1725. https://doi.org/10.3390/jcm12051725
APA StyleRodrigues, T., Rodrigues Fialho, S., Araújo, J. R., Rocha, R., & Moreira-Rosário, A. (2023). Procedures in Fecal Microbiota Transplantation for Treating Irritable Bowel Syndrome: Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(5), 1725. https://doi.org/10.3390/jcm12051725