
Dental Implant Surface Decontamination and Surface Change of an Electrolytic Method versus Mechanical Approaches: A Pilot In Vitro Study

 ,
,  ,
,  ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Size Calculation and Allocation of Interventions
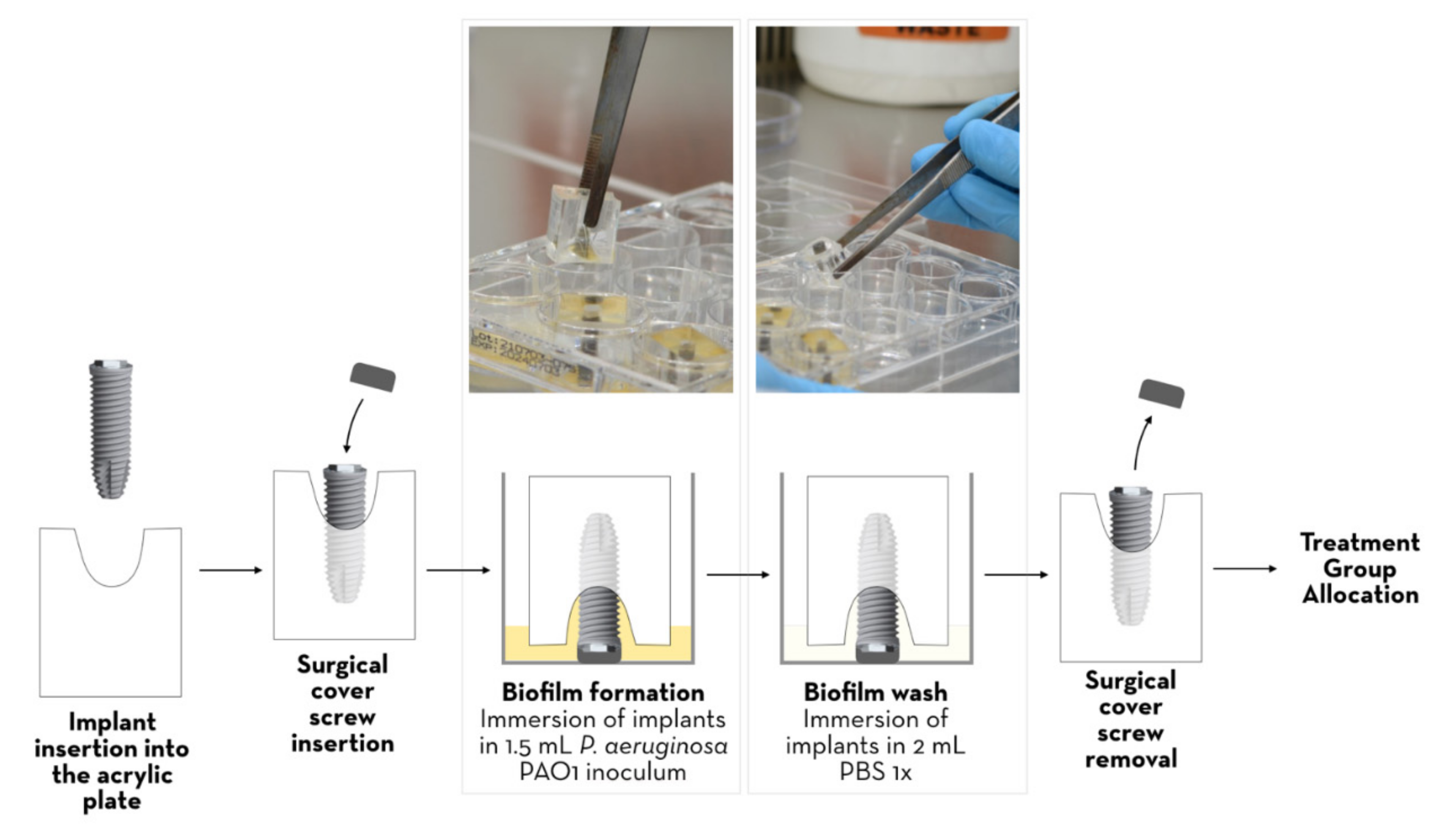
2.3. In Vitro Model of Peri-Implantitis and Surface Contamination with P. aeruginosa
2.4. Plaque Removal Interventions
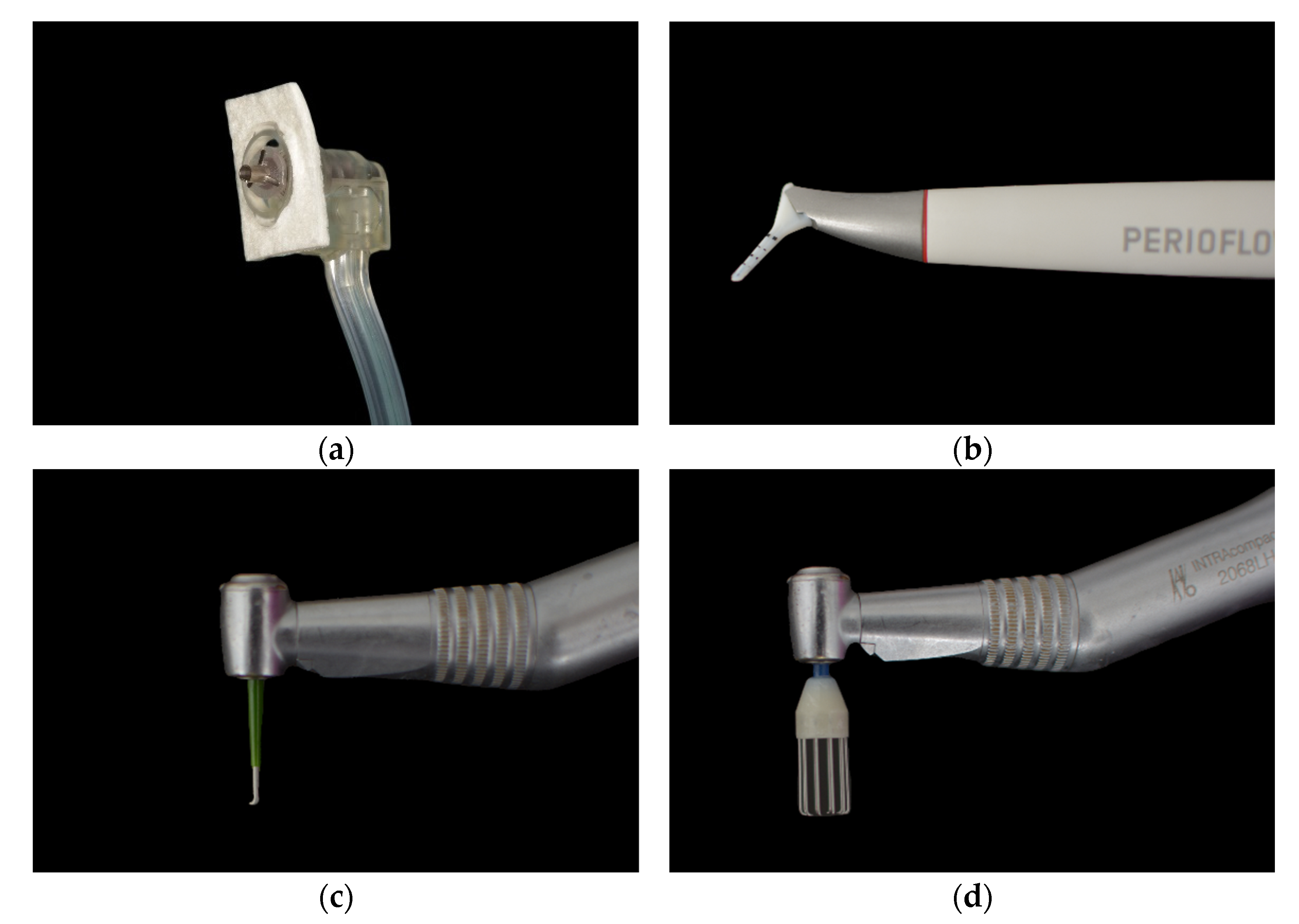
- Electrolytic decontamination [Figure 2a]: Electrolytic decontamination device using galvanic currents (Galvosurge; Galvosurge Dental AG, Widnau, Switzerland), used according to the manufacturer’s instructions. The head of the device is inserted into the implant and held in place throughout the cleaning process. The Galvosurge cleaning solution is pumped in, and a galvanic current forms hydrogen bubbles on the implant surface to release the adherent biofilm. The unit automatically stops working when it reaches 100% (2 min).
- Air abrasion with erythritol powder [Figure 2b]: An erythritol-based air-powder abrasive device with a subgingival plastic nozzle (Perioflow; EMS, Nyon, Switzerland), used according to the manufacturer’s recommendations, with the “liquid” and “power” settings set to the maximum (2 min).
- Mechanical debridement with i-Brush™ [Figure 2c]: Titanium brushes with stainless bristles (i-Brush; NeoBiotech, Seoul, Republic of Korea) used with irrigation at 10,000 rpm (2 min).
- Mechanical debridement using R-Brush™ [Figure 2d]: Rotary titanium brushes (5.6/6.6 in diameter; R-Brush; NeoBiotech, Seoul, Republic of Korea) were used at a rotational speed of 5000 rpm under irrigation with water (2 min).
2.5. Biofilm Quantification
2.6. Scanning Electron Microscopy
2.7. Statistical Analysis
3. Results
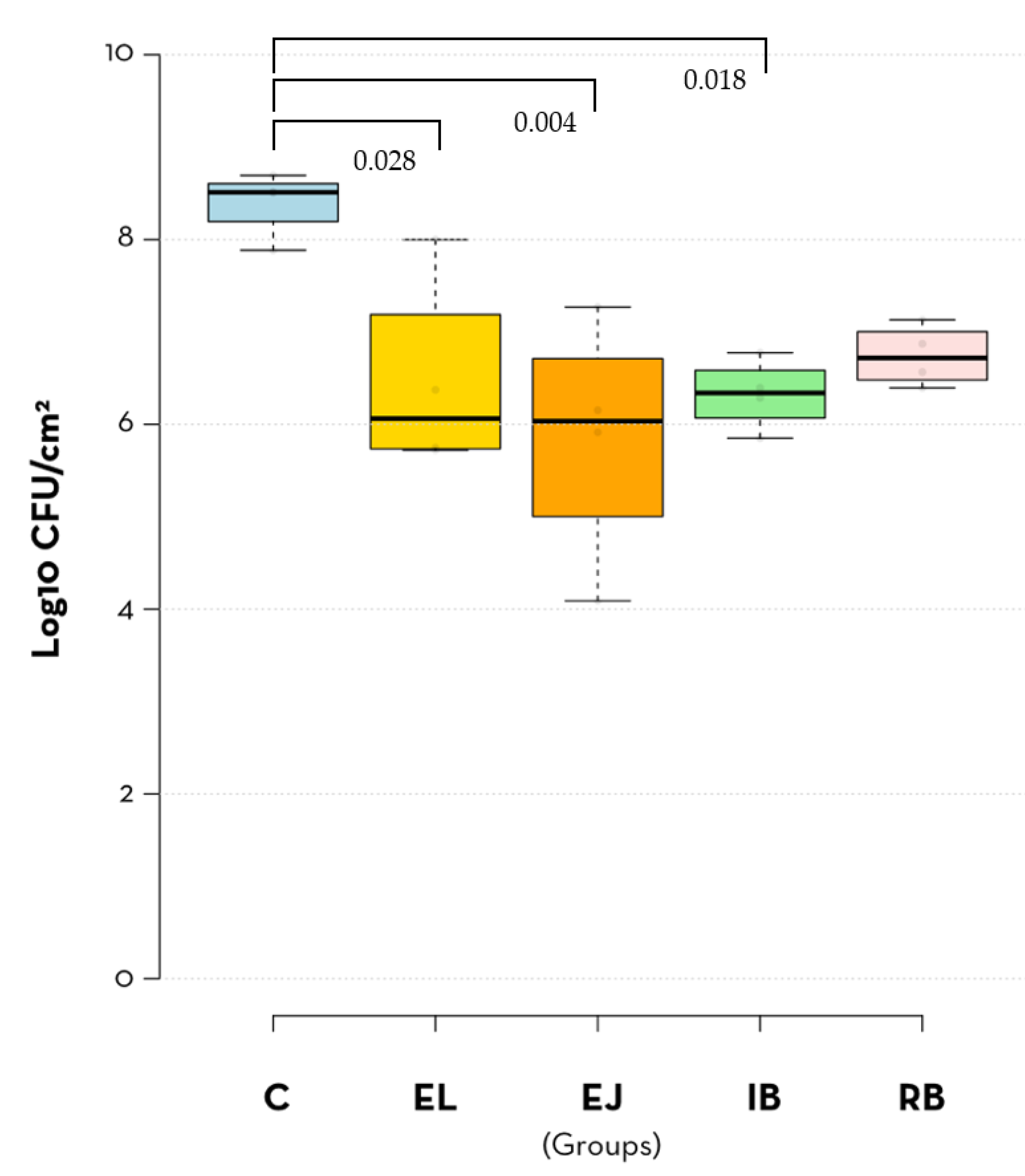
3.1. Quantitative Analysis of Implant-Adhered Bacteria
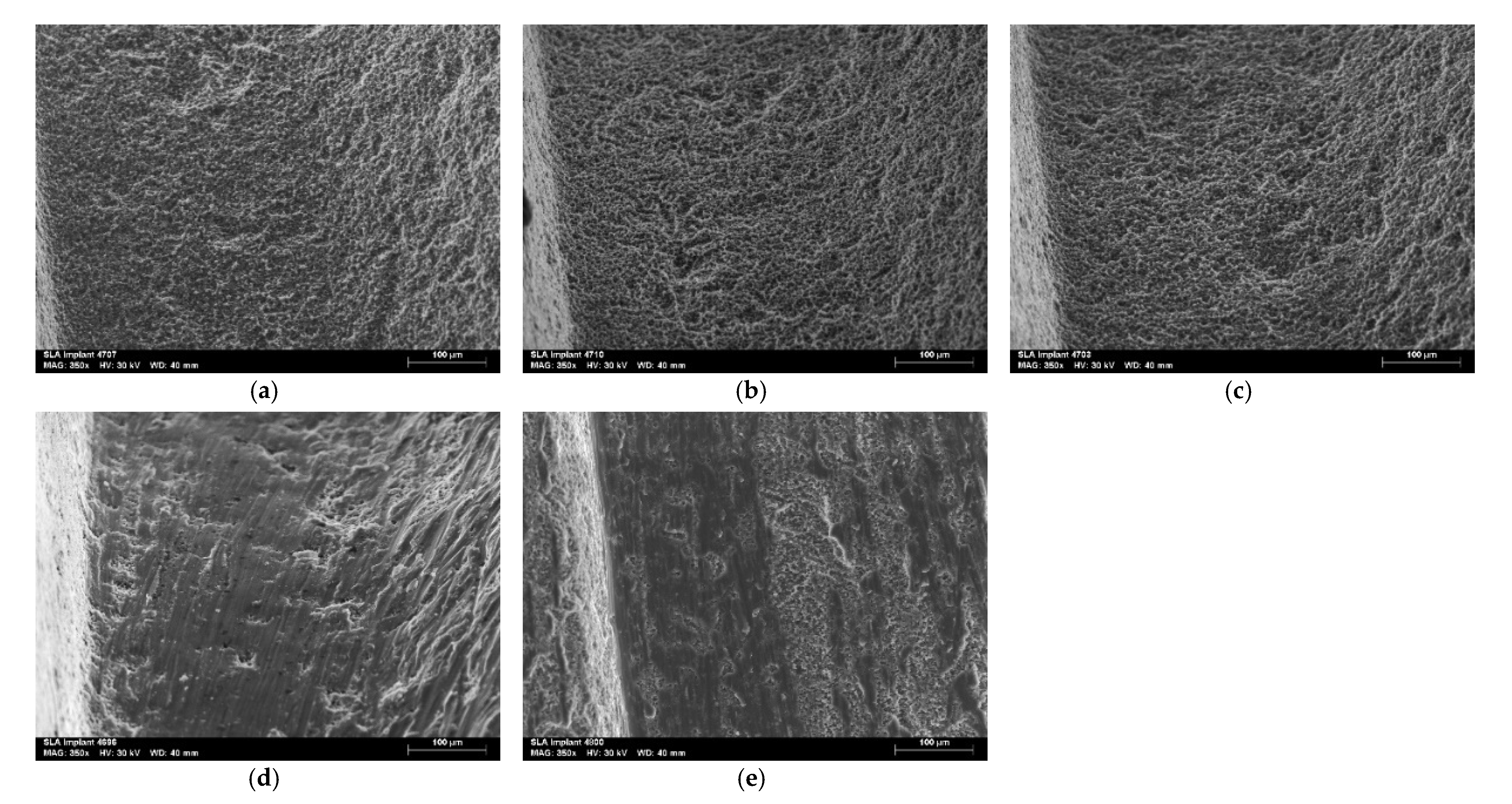
3.2. Qualitative Evaluation of Treated Implants by Scanning Electron Microscopy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diaz, P.; Gonzalo, E.; Villagra, L.J.G.; Miegimolle, B.; Suarez, M.J. What Is the Prevalence of Peri-Implantitis? A Systematic Review and Meta-Analysis. BMC Oral Health 2022, 22, 449. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Jepsen, S.; Stadlinger, B.; Terheyden, H. Peri-Implantitis and Its Prevention. Clin. Oral Implant. Res. 2019, 30, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Albertini, M.; López-Cerero, L.; O’Sullivan, M.G.; Chereguini, C.F.; Ballesta, S.; Ríos, V.; Herrero-Climent, M.; Bullón, P. Assessment of Periodontal and Opportunistic Flora in Patients with Peri-Implantitis. Clin. Oral Implant. Res. 2015, 26, 937–941. [Google Scholar] [CrossRef]
- Rokaya, D.; Srimaneepong, V.; Wisitrasameewon, W.; Humagain, M.; Thunyakitpisal, P. Peri-Implantitis Update: Risk Indicators, Diagnosis, and Treatment. Eur. J. Dent. 2020, 14, 672–682. [Google Scholar] [CrossRef] [PubMed]
- El-Telbany, M.; El-Sharaki, A. Antibacterial and Anti-Biofilm Activity of Silver Nanoparticles on Multi-Drug Resistance Pseudomonas Aeruginosa Isolated from Dental-Implant. J. Oral Biol. Craniofacial Res. 2022, 12, 199–203. [Google Scholar] [CrossRef]
- Derks, J.; Schaller, D.; Håkansson, J.; Wennström, J.L.; Tomasi, C.; Berglundh, T. Peri-Implantitis—Onset and Pattern of Progression. J. Clin. Periodontol. 2016, 43, 383–388. [Google Scholar] [CrossRef]
- Renvert, S.; Hirooka, H.; Polyzois, I.; Kelekis-Cholakis, A.; Wang, H.-L. Diagnosis and Non-Surgical Treatment of Peri-Implant Diseases and Maintenance Care of Patients with Dental Implants—Consensus Report of Working Group 3. Int. Dent. J. 2019, 69, 12–17. [Google Scholar] [CrossRef]
- Wang, C.-W.; Renvert, S.; Wang, H.-L. Nonsurgical Treatment of Periimplantitis. Implant. Dent. 2019, 28, 155–160. [Google Scholar] [CrossRef]
- Kormas, I.; Pedercini, C.; Pedercini, A.; Raptopoulos, M.; Alassy, H.; Wolff, L.F. Peri-Implant Diseases: Diagnosis, Clinical, Histological, Microbiological Characteristics and Treatment Strategies. A Narrative Review. Antibiotics 2020, 9, 835. [Google Scholar] [CrossRef]
- Khoury, F.; Keeve, P.L.; Ramanauskaite, A.; Schwarz, F.; Koo, K.-T.; Sculean, A.; Romanos, G. Surgical Treatment of Peri-Implantitis—Consensus Report of Working Group 4. Int. Dent. J. 2019, 69, 18–22. [Google Scholar] [CrossRef]
- Amate-Fernández, P.; Figueiredo, R.; Blanc, V.; Àlvarez, G.; León, R.; Valmaseda-Castellón, E. Erythritol-Enriched Powder and Oral Biofilm Regrowth on Dental Implants: An in Vitro Study. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e602–e610. [Google Scholar] [CrossRef] [PubMed]
- Toma, S.; Brecx, M.C.; Lasserre, J.F. Clinical Evaluation of Three Surgical Modalities in the Treatment of Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Clin. Med. 2019, 8, 966. [Google Scholar] [CrossRef] [PubMed]
- Ratka, C.; Weigl, P.; Henrich, D.; Koch, F.; Schlee, M.; Zipprich, H. The Effect of In Vitro Electrolytic Cleaning on Biofilm-Contaminated Implant Surfaces. J. Clin. Med. 2019, 8, 1397. [Google Scholar] [CrossRef] [PubMed]
- Alovisi, M.; Carossa, M.; Mandras, N.; Roana, J.; Costalonga, M.; Cavallo, L.; Pira, E.; Putzu, M.G.; Bosio, D.; Roato, I.; et al. Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials 2022, 15, 4850. [Google Scholar] [CrossRef] [PubMed]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface Characteristics of Dental Implants: A Review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef] [PubMed]
- Vernon-Parry, K.D. Scanning Electron Microscopy: An Introduction. III-Vs Rev. 2000, 13, 40–44. [Google Scholar] [CrossRef]
- Al-Hashedi, A.A.; Laurenti, M.; Benhamou, V.; Tamimi, F. Decontamination of Titanium Implants Using Physical Methods. Clin. Oral Implant. Res. 2017, 28, 1013–1021. [Google Scholar] [CrossRef]
- Alotaibi, M.; Moran, G.; Grufferty, B.; Renvert, S.; Polyzois, I. The Effect of a Decontamination Protocol on Contaminated Titanium Dental Implant Surfaces with Different Surface Topography in Edentulous Patients. Acta Odontol. Scand. 2019, 77, 66–75. [Google Scholar] [CrossRef]
- El Chaar, E.; Almogahwi, M.; Abdalkader, K.; Alshehri, A.; Cruz, S.; Ricci, J. Decontamination of the Infected Implant Surface: A Scanning Electron Microscope Study. Int. J. Periodontics Restor. Dent. 2020, 40, 395–401. [Google Scholar] [CrossRef]
- Furtsev, T.V.; Zeer, G.M. Efficiency of Cleaning the Various Types of Dental Implants’ Surfaces (Tiu-Nite, Sla, Rbm) Using the Air-Flow Erythritol Method. J. Int. Dent. Med. Res. 2020, 13, 448–452. [Google Scholar]
- Keim, D.; Nickles, K.; Dannewitz, B.; Ratka, C.; Eickholz, P.; Petsos, H. In Vitro Efficacy of Three Different Implant Surface Decontamination Methods in Three Different Defect Configurations. Clin. Oral Implant. Res. 2019, 30, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, V.H.; Leong, B.W.; Leong, M.J.L.; Lawrence, Z.; Becker, T.; Quaranta, A. Cleaning Potential of Different Air Abrasive Powders and Their Impact on Implant Surface Roughness. Clin. Implant. Dent. Relat. Res. 2020, 22, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Otsuki, M.; Wada, M.; Yamaguchi, M.; Kawabata, S.; Maeda, Y.; Ikebe, K. Evaluation of Decontamination Methods of Oral Biofilms Formed on Screw-Shaped, Rough and Machined Surface Implants: An Ex Vivo Study. Int. J. Implant. Dent. 2020, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Passarelli, P.C.; De Leonardis, M.; Piccirillo, G.B.; Desantis, V.; Papa, R.; Rella, E.; Mastandrea Bonaviri, G.N.; Papi, P.; Pompa, G.; Pasquantonio, G.; et al. The Effectiveness of Chlorhexidine and Air Polishing System in the Treatment of Candida Albicans Infected Dental Implants: An Experimental In Vitro Study. Antibiotics 2020, 9, 179. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Martín, I.; Paeng, K.; Park, H.; Cha, J.-K.; Jung, U.-W.; Sanz, M. Significance of Implant Design on the Efficacy of Different Peri-Implantitis Decontamination Protocols. Clin. Oral Investig. 2021, 25, 3589–3597. [Google Scholar] [CrossRef]
- AlMoharib, H.S.; Steffensen, B.; Zoukhri, D.; Finkelman, M.; Gyurko, R. Efficacy of an Er:YAG Laser in the Decontamination of Dental Implant Surfaces: An in Vitro Study. J. Periodontol. 2021, 92, 1613–1621. [Google Scholar] [CrossRef]
- Biazussi, B.R.; Perrotti, V.; D’Arcangelo, C.; Elias, C.N.; Bianchini, M.A.; Tumedei, M.; de Vasconcellos, D.K. Evaluation of the Effect of Air Polishing With Different Abrasive Powders on the Roughness of Implant Abutment Surface: An In Vitro Study. J. Oral Implantol. 2019, 45, 202–206. [Google Scholar] [CrossRef]
- Pranno, N.; Cristalli, M.P.; Mengoni, F.; Sauzullo, I.; Annibali, S.; Polimeni, A.; La Monaca, G. Comparison of the Effects of Air-Powder Abrasion, Chemical Decontamination, or Their Combination in Open-Flap Surface Decontamination of Implants Failed for Peri-Implantitis: An Ex Vivo Study. Clin. Oral Investig. 2021, 25, 2667–2676. [Google Scholar] [CrossRef]
- Drago, L.; Del Fabbro, M.; Bortolin, M.; Vassena, C.; De Vecchi, E.; Taschieri, S. Biofilm Removal and Antimicrobial Activity of Two Different Air-Polishing Powders: An In Vitro Study. J. Periodontol. 2014, 85, e363–e369. [Google Scholar] [CrossRef]
- Mensi, M.; Cochis, A.; Sordillo, A.; Uberti, F.; Rimondini, L. Biofilm Removal and Bacterial Re-Colonization Inhibition of a Novel Erythritol/Chlorhexidine Air-Polishing Powder on Titanium Disks. Materials 2020, 11, 1510. [Google Scholar] [CrossRef]
- Schneider, S.; Rudolph, M.; Bause, V.; Terfort, A. Electrochemical Removal of Biofilms from Titanium Dental Implant Surfaces. Bioelectrochemistry 2018, 121, 84–94. [Google Scholar] [CrossRef] [PubMed]
- Gianfreda, F.; Punzo, A.; Pistilli, V.; Bollero, P.; Cervino, G.; D’Amico, C.; Cairo, F.; Cicciù, M. Electrolytic Cleaning and Regenerative Therapy of Peri-Implantitis in the Esthetic Area: A Case Report. Eur. J. Dent. 2022, 16, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M.; Rathe, F.; Brodbeck, U.; Ratka, C.; Weigl, P.; Zipprich, H. Treatment of Peri-Implantitis—Electrolytic Cleaning Versus Mechanical and Electrolytic Cleaning—A Randomized Controlled Clinical Trial—Six-Month Results. J. Clin. Med. 2019, 8, 1909. [Google Scholar] [CrossRef] [PubMed]
- Ruan, X.; Luo, J.; Zhang, P.; Howell, K. The Salivary Microbiome Shows a High Prevalence of Core Bacterial Members yet Variability across Human Populations. NPJ Biofilms Microbiomes 2022, 8, 85. [Google Scholar] [CrossRef] [PubMed]
- LaBauve, A.E.; Wargo, M.J. Growth and Laboratory Maintenance of Pseudomonas Aeruginosa. Curr. Protoc. Microbiol. 2012, 25, 6E.1.1–6E.1.8. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PC | EL | EJ | IB | RB | |
|---|---|---|---|---|---|
| Mean (SD) | 8.39 (0.36) | 6.46 (1.07) | 5. 86 (1.32) | 6.32 (0.38) | 6.74 (0.33) |
| SE | 0.18 | 0.54 | 0.66 | 0.19 | 0.16 |
| 95% CI | 7.83–8.96 | 4.76–8.16 | 3.76–7.95 | 5.72–6.93 | 6.22–7.26 |
| Minimum | 7.88 | 5.72 | 4.09 | 5.85 | 6.39 |
| Maximum | 8.69 | 8.00 | 7.27 | 6.77 | 7.13 |
| C | EL | EJ | IB | RB | |
|---|---|---|---|---|---|
| C | - | 0.028 | 0.004 | 0.018 | 0.070 |
| EL | - | - | 0.824 | 0.999 | 0.987 |
| EJ | - | - | - | 0.920 | 0.549 |
| IB | - | - | - | - | 0.947 |
| RB | - | - | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assunção, M.A.; Botelho, J.; Machado, V.; Proença, L.; Matos, A.P.A.; Mendes, J.J.; Bessa, L.J.; Taveira, N.; Santos, A. Dental Implant Surface Decontamination and Surface Change of an Electrolytic Method versus Mechanical Approaches: A Pilot In Vitro Study. J. Clin. Med. 2023, 12, 1703. https://doi.org/10.3390/jcm12041703
Assunção MA, Botelho J, Machado V, Proença L, Matos APA, Mendes JJ, Bessa LJ, Taveira N, Santos A. Dental Implant Surface Decontamination and Surface Change of an Electrolytic Method versus Mechanical Approaches: A Pilot In Vitro Study. Journal of Clinical Medicine. 2023; 12(4):1703. https://doi.org/10.3390/jcm12041703
Chicago/Turabian StyleAssunção, Mariana Anselmo, João Botelho, Vanessa Machado, Luís Proença, António P. A. Matos, José João Mendes, Lucinda J. Bessa, Nuno Taveira, and Alexandre Santos. 2023. "Dental Implant Surface Decontamination and Surface Change of an Electrolytic Method versus Mechanical Approaches: A Pilot In Vitro Study" Journal of Clinical Medicine 12, no. 4: 1703. https://doi.org/10.3390/jcm12041703
APA StyleAssunção, M. A., Botelho, J., Machado, V., Proença, L., Matos, A. P. A., Mendes, J. J., Bessa, L. J., Taveira, N., & Santos, A. (2023). Dental Implant Surface Decontamination and Surface Change of an Electrolytic Method versus Mechanical Approaches: A Pilot In Vitro Study. Journal of Clinical Medicine, 12(4), 1703. https://doi.org/10.3390/jcm12041703