
Association between Exposure to Selected Heavy Metals and Blood Eosinophil Counts in Asthmatic Adults: Results from NHANES 2011–2018


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population
2.3. Measurement of Metal Exposures
2.4. Blood Eosinophil Count Measurement
2.5. Covariates and Asthma Assessment
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. The Associations between the Blood Metal Concentrations and Blood Eosinophil Counts
3.3. Stratified Associations between Blood Pb Concentrations and Blood Eosinophil Counts
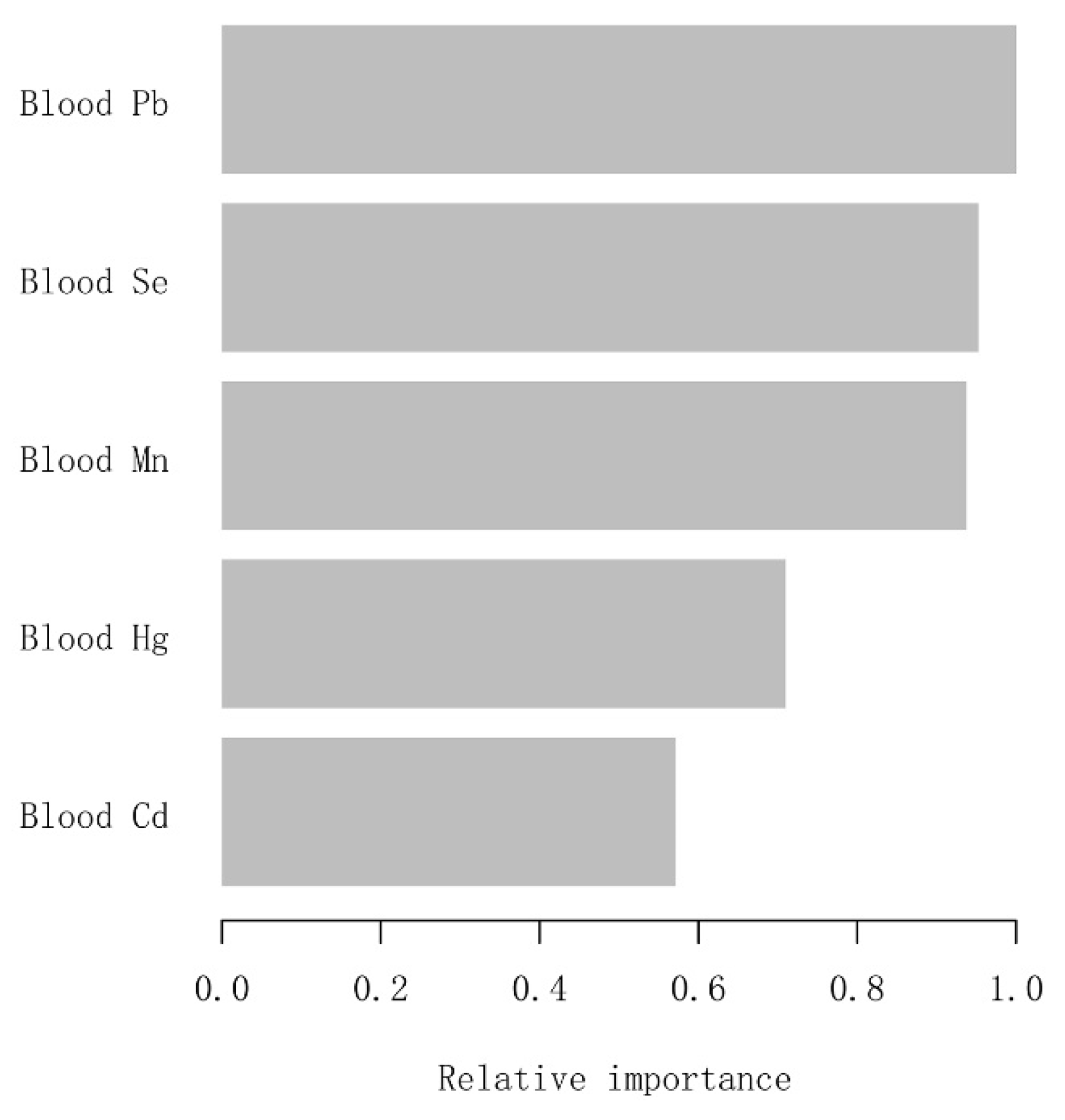
3.4. Using Machine Learning from the XGBoost Algorithm Model to Explore the Blood Metals’ Relative Importance
3.5. Exploring Dose-Response Relationships of Blood Pb Concentrations with Blood Eosinophil Counts by the Generalized Additive Model (GAM)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wenzel, S. Severe asthma: From characteristics to phenotypes to endotypes. Clin. Exp. Allergy 2012, 42, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Wenzel, S.E.; Brozek, J.L.; Bush, A.; Castro, M.; Sterk, P.J.; Adcock, I.M.; Bateman, E.D.; Bel, E.H.; Bleecker, E.R.; et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur. Respir. J. 2014, 43, 343–373. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Res. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Naghabi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Caset, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, A.J.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar]
- Pate, C.A.; Zahran, H.S.; Qin, X.; Johnson, C.; Hummelman, E.; Malilay, J. Asthma Surveillance—United States, 2006–2018. Morbidity and mortality weekly report. Surveill. Summ. 2021, 70, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Nurmagambetov, T.; Kuwahara, R.; Garbe, P. The Economic Burden of Asthma in the United States, 2008–2013. Ann. Am. Thorac. Soc. 2018, 15, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Denlinger, L.C.; Phillips, B.R.; Ramratnam, S.; Ross, K.; Bhakta, N.R.; Cardet, J.C.; Castro, M.; Peters, S.P.; Phipatanakul, W.; Aujla, S.; et al. Inflammatory and Comorbid Features of Patients with Severe Asthma and Frequent Exacerbations. Am. J. Respir. Crit. Care Med. 2017, 195, 302–313. [Google Scholar] [CrossRef]
- Carr, T.F.; Zeki, A.A.; Kraft, M. Eosinophilic and Noneosinophilic Asthma. Am. J. Respir. Crit. Care Med. 2018, 197, 22–37. [Google Scholar] [CrossRef]
- Fowler, S.J.; Tavernier, G.; Niven, R. High blood eosinophil counts predict sputum eosinophilia in patients with severe asthma. J. Allergy Clin. Immunol. 2015, 135, 822–824.e2. [Google Scholar]
- Wagener, A.H.; de Nijs, S.B.; Lutter, R.; Sousa, A.R.; Weersink, E.J.; Bel, E.H.; Sterk, P.J. External validation of blood eosinophils, FE(NO) and serum periostin as surrogates for sputum eosinophils in asthma. Thorax 2015, 70, 115–120. [Google Scholar] [CrossRef]
- Hastie, A.T.; Moore, W.C.; Li, H.; Rector, B.M.; Ortega, V.E.; Pascual, R.M.; Peters, S.P.; Meyers, D.A.; Bleecker, E.R. Biomarker surrogates do not accurately predict sputum eosinophil and neutrophil percentages in asthmatic subjects. J. Allergy Clin. Immunol. 2013, 132, 72–80.e12. [Google Scholar] [CrossRef] [PubMed]
- Ulrik, C.S.; Frederiksen, J. Mortality and markers of risk of asthma death among 1,075 outpatients with asthma. Chest 1995, 108, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Kupczyk, M.; Haque, S.; Middelveld, R.J.; Dahlén, B.; Dahlén, S.E. Phenotypic predictors of response to oral glucocorticosteroids in severe asthma. Respir. Med. 2013, 107, 1521–1530. [Google Scholar] [CrossRef] [PubMed]
- Malinovschi, A.; Fonseca, J.A.; Jacinto, T.; Alving, K.; Janson, C. Exhaled nitric oxide levels and blood eosinophil counts independently associate with wheeze and asthma events in National Health and Nutrition Examination Survey subjects. J. Allergy Clin. Immunol. 2013, 132, 821–827.e5. [Google Scholar] [CrossRef]
- Wark, P.A.; McDonald, V.M.; Gibson, P.G. Adjusting prednisone using blood eosinophils reduces exacerbations and improves asthma control in difficult patients with asthma. Respirology 2015, 20, 1282–1284. [Google Scholar] [CrossRef]
- Corren, J.; Weinstein, S.; Janka, L.; Zangrilli, J.; Garin, M. Phase 3 Study of Reslizumab in Patients With Poorly Controlled Asthma: Effects Across a Broad Range of Eosinophil Counts. Chest 2016, 150, 799–810. [Google Scholar] [CrossRef]
- Goldman, M.; Hirsch, I.; Zangrilli, J.G.; Newbold, P.; Xu, X. The association between blood eosinophil count and benralizumab efficacy for patients with severe, uncontrolled asthma: Subanalyses of the Phase III SIROCCO and CALIMA studies. Curr. Med Res. Opin. 2017, 33, 1605–1613. [Google Scholar] [CrossRef]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N. Engl. J. Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef]
- FitzGerald, J.M.; Bleecker, E.R.; Nair, P.; Korn, S.; Ohta, K.; Lommatzsch, M.; Ferguson, G.T.; Busse, W.W.; Barker, P.; Sproule, S.; et al. An anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2016, 388, 2128–2141. [Google Scholar] [CrossRef]
- Bleecker, E.R.; FitzGerald, J.M.; Chanez, P.; Papi, A.; Weinstein, S.F.; Barker, P.; Sproule, S.; Gilmartin, G.; Aurivillius, M.; Werkström, V.; et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β(2)-agonists (SIROCCO): A randomised, multicentre, placebo-controlled phase 3 trial. Lancet 2016, 388, 2115–2127. [Google Scholar] [CrossRef]
- Vedel-Krogh, S.; Nielsen, S.F.; Lange, P.; Vestbo, J.; Nordestgaard, B.G. Association of Blood Eosinophil and Blood Neutrophil Counts with Asthma Exacerbations in the Copenhagen General Population Study. Clin. Chem. 2017, 63, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Price, D.B.; Rigazio, A.; Campbell, J.D.; Bleecker, E.R.; Corrigan, C.J.; Thomas, M.; Wenzel, S.E.; Wilson, A.M.; Small, M.B.; Gopalan, G.; et al. Blood eosinophil count and prospective annual asthma disease burden: A UK cohort study. Lancet Respir. Med. 2015, 3, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Zeiger, R.S.; Schatz, M.; Dalal, A.A.; Chen, W.; Sadikova, E.; Suruki, R.Y.; Kawatkar, A.A.; Qian, L. Blood Eosinophil Count and Outcomes in Severe Uncontrolled Asthma: A Prospective Study. J. Allergy Clin. Immunol. Pr. 2017, 5, 144–153.e8. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.-G.; Chang, C.-Y.; Yen, C.-Y.; Lai, C.-C. Associations between environmental heavy metal exposure and childhood asthma: A population-based study. J. Microbiol. Immunol. Infect. 2019, 52, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Menke, A.; Guallar, E.; Cowie, C.C. Metals in Urine and Diabetes in U.S. Adults. Diabetes 2016, 65, 164–171. [Google Scholar] [CrossRef]
- Zeng, X.; Xu, X.; Zheng, X.; Reponen, T.; Chen, A.; Huo, X. Heavy metals in PM2.5 and in blood, and children’s respiratory symptoms and asthma from an e-waste recycling area. Environ. Pollut. 2016, 210, 346–353. [Google Scholar] [CrossRef]
- Wang, I.J.; Karmaus, W.J.J.; Yang, C.C. Lead exposure, IgE, and the risk of asthma in children. J. Exp. Sci. Environ. Epidemiol. 2017, 27, 478–483. [Google Scholar] [CrossRef]
- Lehmann, I. Environmental pollutants as adjuvant factors of immune system derived diseases. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 2017, 60, 592–596. [Google Scholar] [CrossRef]
- Feiler, M.O.; Pavia, C.J.; Frey, S.M.; Parsons, P.J.; Thevenet-Morrison, K.; Canfield, R.L.; Jusko, T.A. Early life blood lead levels and asthma diagnosis at age 4–6 years. Environ. Health Prev. Med. 2021, 26, 108. [Google Scholar] [CrossRef]
- Park, S.; Lee, E.-H.; Kho, Y. The association of asthma, total IgE, and blood lead and cadmium levels. J. Allergy Clin. Immunol. 2016, 138, 1701–1703.e6. [Google Scholar] [CrossRef]
- Huang, X.; Xie, J.; Cui, X.; Zhou, Y.; Wu, X.; Lu, W.; Shen, Y.; Yuan, J.; Chen, W. Association between Concentrations of Metals in Urine and Adult Asthma: A Case-Control Study in Wuhan, China. PloS ONE 2016, 11, e0155818. [Google Scholar]
- Rosa, M.J.; Benedetti, C.; Peli, M.; Donna, F.; Nazzaro, M.; Fedrighi, C.; Zoni, S.; Marcon, A.; Zimmerman, N.; Wright, R.; et al. Association between personal exposure to ambient metals and respiratory disease in Italian adolescents: A cross-sectional study. BMC Pulm. Med. 2016, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Urushidate, S.; Matsuzaka, M.; Okubo, N.; Iwasaki, H.; Hasebe, T.; Tsuya, R.; Iwane, K.; Inoue, R.; Yamai, K.; Danjo, K.; et al. Association between concentration of trace elements in serum and bronchial asthma among Japanese general population. J. Trace Elements Med. Biol. 2010, 24, 236–242. [Google Scholar]
- Huang, C.-H.; Hsieh, C.-Y.; Wang, C.-W.; Tu, H.-P.; Chen, S.-C.; Hung, C.-H.; Kuo, C.-H. Associations and Interactions between Heavy Metals with White Blood Cell and Eosinophil Count. Int. J. Med Sci. 2022, 19, 331–337. [Google Scholar] [CrossRef]
- Oulhote, Y.; Shamim, Z.; Kielsen, K.; Weihe, P.; Grandjean, P.; Ryder, L.P.; Heilmann, C. Children’s white blood cell counts in relation to developmental exposures to methylmercury and persistent organic pollutants. Reprod. Toxicol. 2017, 68, 207–214. [Google Scholar]
- Cornwell, C.R.; Egan, K.B.; Zahran, H.S.; Mirabelli, M.C.; Hsu, J.; Chew, G.L. Associations of blood lead levels with asthma and blood eosinophils in US children. Pediatr. Allergy Immunol. 2020, 31, 695–699. [Google Scholar]
- Min, K.-B.; Min, J.-Y. Environmental lead exposure and increased risk for total and allergen-specific IgE in US adults. J. Allergy Clin. Immunol. 2015, 135, 275–277. [Google Scholar] [CrossRef]
- Bellanger, A.-P.; Bosch-Cano, F.; Millon, L.; Ruffaldi, P.; Franchi, M.; Bernard, N. Reactions of airway epithelial cells to birch pollen grains previously exposed to in situ atmospheric Pb concentrations: A preliminary assay of allergenicity. Biol. Trace Element Res. 2012, 150, 391–395. [Google Scholar] [CrossRef]
- Farkhondeh, T.; Boskabady, M.H.; Kohi, M.K.; Sadeghi-Hashjin, G.; Moin, M. Lead exposure affects inflammatory mediators, total and differential white blood cells in sensitized guinea pigs during and after sensitization. Drug Chem. Toxicol. 2014, 37, 329–335. [Google Scholar] [CrossRef]
- Guardiola, F.A.; Cuesta, A.; Meseguer, J.; Martínez, S.; Martínez-Sánchez, M.J.; Pérez-Sirvent, C.; Esteban, M.A. Accumulation, histopathology and immunotoxicological effects of waterborne cadmium on gilthead seabream (Sparus aurata). Fish Shellfish. Immunol. 2013, 35, 792–800. [Google Scholar]
- Kim, J.H.; Lee, K.-H.; Hong, S.-C.; Lee, H.-S.; Lee, J.; Kang, J.W. Association between serum mercury concentration and leukocyte differential count in children. Pediatr. Hematol. Oncol. 2015, 32, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.H.; Liu, P.J.; Hsia, S.; Chuang, C.J.; Chen, P.C. Role of certain trace minerals in oxidative stress, in-flam-mation, CD4/CD8 lymphocyte ratios and lung function in asthmatic patients. Ann. Clin. Biochem. 2011, 48 Pt 4, 344–351. [Google Scholar] [PubMed]
- Zeiger, R.S.; Schatz, M.; Li, Q.; Chen, W.; Khatry, D.B.; Gossage, D.; Tran, T.N. The association of blood eo-sinophil counts to future asthma exacerbations in children with persistent asthma. J. Allergy Clin. Immunol. In Pract. 2015, 3, 283–287.e4. [Google Scholar] [CrossRef]
- Foster, P.S.; Hogan, S.P.; Yang, M.; Mattes, J.; Young, I.G.; Matthaei, K.I.; Kumar, R.K.; Mahalingam, S.; Webb, D.C. Interleukin-5 and eosinophils as therapeutic targets for asthma. Trends Mol. Med. 2002, 8, 162–167. [Google Scholar] [PubMed]
- Casciano, J.; Krishnan, J.A.; Small, M.B.; Buck, P.O.; Gopalan, G.; Li, C.; Kemp, R.; Dotiwala, Z. Burden of asthma with elevated blood eosinophil levels. BMC Pulm. Med. 2016, 16, 100. [Google Scholar] [CrossRef]
- Anderson, H.M.; Lemanske, R.F., Jr.; Arron, J.R.; Holweg, C.T.J.; Rajamanickam, V.; Gangnon, R.E.; Gern, J.E.; Jackson, D.J. Relationships among aeroallergen sensitization, peripheral blood eosinophils, and periostin in pediatric asthma development. J. Allergy Clin. Immunol. 2017, 139, 790–796. [Google Scholar] [PubMed]
- Nakagome, K.; Nagata, M. Involvement and Possible Role of Eosinophils in Asthma Exacerbation. Front. Immunol. 2018, 9, 2220. [Google Scholar]
- Thomson, C.D.; Wickens, K.; Miller, J.; Ingham, T.; Lampshire, P.; Epton, M.J.; Town, G.I.; Pattemore, P.; Crane, J. Selenium status and allergic disease in a cohort of New Zealand children. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2012, 42, 560–567. [Google Scholar]
- Li, X.; Fan, Y.; Zhang, Y.; Huang, X.; Huang, Z.; Yu, M.; Xu, Q.; Han, X.; Lu, C.; Wang, X. Association be-tween selected urinary heavy metals and asthma in adults: A retrospective cross-sectional study of the US National Health and Nutrition Examination Survey. Environ. Sci. Pollut. Res. Int. 2021, 28, 5833–5844. [Google Scholar] [CrossRef]
- Mishra, K.P. Lead exposure and its impact on immune system: A review. Toxicol. Vitr. 2009, 23, 969–972. [Google Scholar]
- Min, J.-Y.; Min, K.-B.; Kim, R.; Cho, S.-I.; Paek, M. Blood lead levels and increased bronchial responsiveness. Biol. Trace Element Res. 2008, 123, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Wells, E.M.; Bonfield, T.L.; Dearborn, D.G.; Jackson, L.W. The relationship of blood lead with immunoglobulin E, eosinophils, and asthma among children: NHANES 2005–2006. Int. J. Hyg. Environ. Health 2014, 217, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.R.; Cui, S.M.; Lu, X.X.; Chen, X.M.; Yang, X.; Cui, J.P.; Zhang, G.H. Effects of occupational cadmium exposure on workers’ cardiovascular system. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi Zhonghua Laodong Weisheng Zhiyebing Zazhi/Chin. J. Ind. Hyg. Occup. Dis. 2018, 36, 474–477. [Google Scholar]
- Huo, J.; Huang, Z.; Li, R.; Song, Y.; Lan, Z.; Ma, S.; Wu, Y.; Chen, J.; Zhang, L. Dietary cadmium exposure assessment in rural areas of Southwest China. PLoS ONE 2018, 13, e0201454. [Google Scholar] [CrossRef] [PubMed]
- Nyland, J.F.; Fillion, M.; Barbosa, F., Jr.; Shirley, D.L.; Chine, C.; Lemire, M.; Mergler, D.; Silbergeld, E.K. Bi-omarkers of methylmercury exposure immunotoxicity among fish consumers in Amazonian Brazil. Environ. Health Perspect. 2011, 119, 1733–1738. [Google Scholar] [CrossRef]
- Kim, K.-N.; Bae, S.; Park, H.Y.; Kwon, H.-J.; Hong, Y.C. Low-level Mercury Exposure and Risk of Asthma in School-age Children. Epidemiology 2015, 26, 733–739. [Google Scholar] [CrossRef]
- Schaefer, A.M.; Stavros, H.-C.W.; Bossart, G.D.; Fair, P.A.; Goldstein, J.D.; Reif, J.S. Associations between mercury and hepatic, renal, endocrine, and hematological parameters in Atlantic bottlenose dolphins (Tursiops truncatus) along the eastern coast of Florida and South Carolina. Arch. Environ. Contam. Toxicol. 2011, 61, 688–695. [Google Scholar] [CrossRef]
- Rayman, M.P. Selenium and human health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Q1 | Q2 | Q3 | Q4 | p-Value | |
|---|---|---|---|---|---|
| Gender (%) | 0.039 | ||||
| Male | 37.41 (26.44, 49.85) | 37.87 (32.63, 43.41) | 39.27 (33.83, 44.98) | 46.96 (42.24, 51.74) | |
| Female | 62.59 (50.15, 73.56) | 62.13 (56.59, 67.37) | 60.73 (55.02, 66.17) | 53.04 (48.26, 57.76) | |
| Age, mean (95% CI) (years) | 45.46 (41.40, 49.52) | 43.48 (41.89, 45.06) | 45.41 (43.54, 47.28) | 46.64 (44.97, 48.30) | 0.038 |
| Race/ethnicity (%) | 0.361 | ||||
| Mexican American | 4.73 (1.52, 13.79) | 4.91 (3.34, 7.16) | 6.13 (4.14, 8.99) | 7.03 (4.96, 9.88) | |
| Other Hispanic | 6.84 (2.44, 17.76) | 6.14 (4.17, 8.96) | 7.20 (5.22, 9.86) | 6.56 (4.61, 9.24) | |
| Non-Hispanic White | 63.01 (44.80, 78.14) | 67.54 (60.54, 73.84) | 66.28 (59.36, 72.58) | 68.35 (63.38, 72.93) | |
| Non-Hispanic Black | 20.79 (12.00, 33.56) | 13.01 (9.69, 17.26) | 11.36 (8.75, 14.64) | 10.40 (7.98, 13.46) | |
| Other race | 4.63 (1.79, 11.40) | 8.40 (5.51, 12.61) | 9.02 (6.42, 12.54) | 7.66 (5.75, 10.13) | |
| Education (%) | 0.502 | ||||
| Less than high school | 16.70 (9.34, 28.08) | 10.86 (8.44, 13.86) | 14.20 (10.82, 18.42) | 13.28 (9.82, 17.72) | |
| High school | 23.31 (12.86, 38.51) | 20.27 (16.29, 24.92) | 19.30 (14.90, 24.63) | 22.88 (18.43, 28.03) | |
| More than high school | 59.98 (44.64, 73.59) | 68.88 (63.79, 73.55) | 66.49 (60.71, 71.82) | 63.84 (57.45, 69.79) | |
| Marital status (%) | 0.501 | ||||
| Married | 45.22 (31.88, 59.29) | 50.45 (45.43, 55.46) | 46.76 (41.46, 52.14) | 51.84 (47.29, 56.35) | |
| Single | 50.68 (36.51, 64.74) | 41.19 (36.81, 45.73) | 46.01 (40.48, 51.64) | 40.95 (37.12, 44.89) | |
| Living with a partner | 4.10 (1.21, 13.00) | 8.36 (5.87, 11.77) | 7.22 (4.98, 10.36) | 7.21 (5.06, 10.19) | |
| Poverty-to-income ratio, mean (95% CI) | 2.60 (2.07, 3.13) | 2.88 (2.68, 3.08) | 2.65 (2.43, 2.88) | 2.75 (2.53, 2.96) | 0.241 |
| BMI, mean (95% CI) (kg/m2) | 28.05 (25.90, 30.20) | 29.41 (28.55, 30.26) | 31.03 (29.96, 32.10) | 31.70 (30.80, 32.59) | 0.001 |
| Smoked at least 100 cigarettes in life (%) | 0.224 | ||||
| Yes | 50.51 (34.88, 66.05) | 43.61 (37.64, 49.77) | 45.57 (39.23, 52.06) | 51.05 (44.87, 57.20) | |
| No | 49.49 (33.95, 65.12) | 56.39 (50.23, 62.36) | 54.43 (47.94, 60.77) | 48.95 (42.80, 55.13) | |
| Hypertension (%) | 0.003 | ||||
| Yes | 36.62 (23.68, 51.82) | 29.25 (24.35, 34.68) | 37.71 (32.22, 43.53) | 41.20 (36.32, 46.25) | |
| No | 63.38 (48.18, 76.32) | 70.75 (65.32, 75.65) | 62.29 (56.47, 67.78) | 58.80 (53.75, 63.68) | |
| Diabetes (%) | 0.394 | ||||
| Yes | 13.66 (6.13, 27.72) | 8.60 (6.62, 11.09) | 12.50 (9.65, 16.04) | 13.57 (10.14, 17.92) | |
| No | 82.01 (66.25, 91.36) | 88.34 (84.69, 91.22) | 85.06 (80.97, 88.39) | 84.24 (79.54, 88.03) | |
| Borderline | 4.33 (0.98, 17.18) | 3.06 (1.32, 6.94) | 2.44 (1.26, 4.67) | 2.19 (1.29, 3.70) | |
| BUN, mean (95% CI) (mmol/L) | 4.72 (4.20, 5.24) | 4.65 (4.50, 4.80) | 4.79 (4.58, 5.00) | 4.97 (4.80, 5.15) | 0.075 |
| Cr, mean (95% CI) (umol/L) | 73.95 (69.17, 78.72) | 74.05 (72.23, 75.86) | 77.18 (74.93, 79.42) | 80.06 (77.99, 82.13) | 0.0002 |
| Blood cotinine, mean (95% CI) (ng/mL) | 94.98 (52.24, 137.72) | 53.90 (38.51, 69.29) | 61.44 (49.13, 73.75) | 68.29 (51.47, 85.12) | 0.200 |
| Blood Pb, mean (95% CI) (ug/dL) | 1.20 (0.92, 1.49) | 1.00 (0.91, 1.08) | 1.03 (0.94, 1.13) | 1.17 (1.06, 1.28) | 0.007 |
| Blood Cd, mean (95% CI) (ug/dL) | 0.56 (0.42, 0.71) | 0.46 (0.37, 0.55) | 0.49 (0.44, 0.54) | 0.59 (0.50, 0.69) | 0.106 |
| Blood Hg, mean (95% CI) (ug/dL) | 1.53 (1.00, 2.06) | 1.40 (1.14, 1.65) | 1.24 (1.05, 1.42) | 1.13 (0.88, 1.37) | 0.126 |
| Blood Se, mean (95% CI) (ug/dL) | 197.90 (190.03, 205.77) | 194.14 (191.52, 196.75) | 192.45 (189.50, 195.40) | 194.60 (191.24, 197.97) | 0.567 |
| Blood Mn, mean (95% CI) (ug/dL) | 9.62 (8.37, 10.88) | 10.15 (9.81, 10.49) | 10.10 (9.77, 10.42) | 9.72 (9.39, 10.06) | 0.179 |
| Non-Adjusted Model | Minimally Adjusted Model | Fully Adjusted Model | |
|---|---|---|---|
| β (95% CI) p value | β (95% CI) p value | β (95% CI) p value | |
| Log blood Pb (ug/dL) | 24.76 (8.22, 41.30) 0.005 | 17.66 (−0.78, 36.09) 0.066 | 25.39 (6.91, 43.88) 0.010 |
| Log blood Cd (ug/dL) | 4.18 (−7.55, 15.91) 0.487 | 7.18 (−5.56, 19.92) 0.274 | 17.51 (−0.43, 35.45) 0.063 |
| Log blood Hg (ug/dL) | −1.91 (−11.32, 7.50) 0.693 | −4.35 (−14.13, 5.43) 0.387 | −3.23 (−13.20, 6.75) 0.530 |
| Log blood Se (ug/dL) | 14.48 (−68.49, 97.45) 0.734 | −6.99 (−86.32, 72.35) 0.864 | −7.60 (−82.84, 67.64) 0.844 |
| Log blood Mn (ug/dL) | −14.27 (−40.80, 12.26) 0.296 | −6.18 (−37.67, 25.31) 0.702 | −5.87 (−37.43, 25.68) 0.717 |
| β (95% CI) p-Value | |
|---|---|
| Model I | |
| Linear effect | 25.39 (10.53, 40.26) 0.001 |
| Model II | |
| Inflection point (K) | −0.87 |
| Log blood Pb < K | 56.23 (−5.73, 118.19) 0.075 |
| Log blood Pb > K | 21.30 (4.43, 38.18) 0.013 |
| Log likelihood ratio | 0.312 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wen, J.; Giri, M.; Xu, L.; Guo, S. Association between Exposure to Selected Heavy Metals and Blood Eosinophil Counts in Asthmatic Adults: Results from NHANES 2011–2018. J. Clin. Med. 2023, 12, 1543. https://doi.org/10.3390/jcm12041543
Wen J, Giri M, Xu L, Guo S. Association between Exposure to Selected Heavy Metals and Blood Eosinophil Counts in Asthmatic Adults: Results from NHANES 2011–2018. Journal of Clinical Medicine. 2023; 12(4):1543. https://doi.org/10.3390/jcm12041543
Chicago/Turabian StyleWen, Jun, Mohan Giri, Li Xu, and Shuliang Guo. 2023. "Association between Exposure to Selected Heavy Metals and Blood Eosinophil Counts in Asthmatic Adults: Results from NHANES 2011–2018" Journal of Clinical Medicine 12, no. 4: 1543. https://doi.org/10.3390/jcm12041543
APA StyleWen, J., Giri, M., Xu, L., & Guo, S. (2023). Association between Exposure to Selected Heavy Metals and Blood Eosinophil Counts in Asthmatic Adults: Results from NHANES 2011–2018. Journal of Clinical Medicine, 12(4), 1543. https://doi.org/10.3390/jcm12041543