
Evaluation of Dysfunctional HDL by Myeloperoxidase/Paraoxonase Ratio in Unexplained Infertility Patients Undergoing IVF/ICSI
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
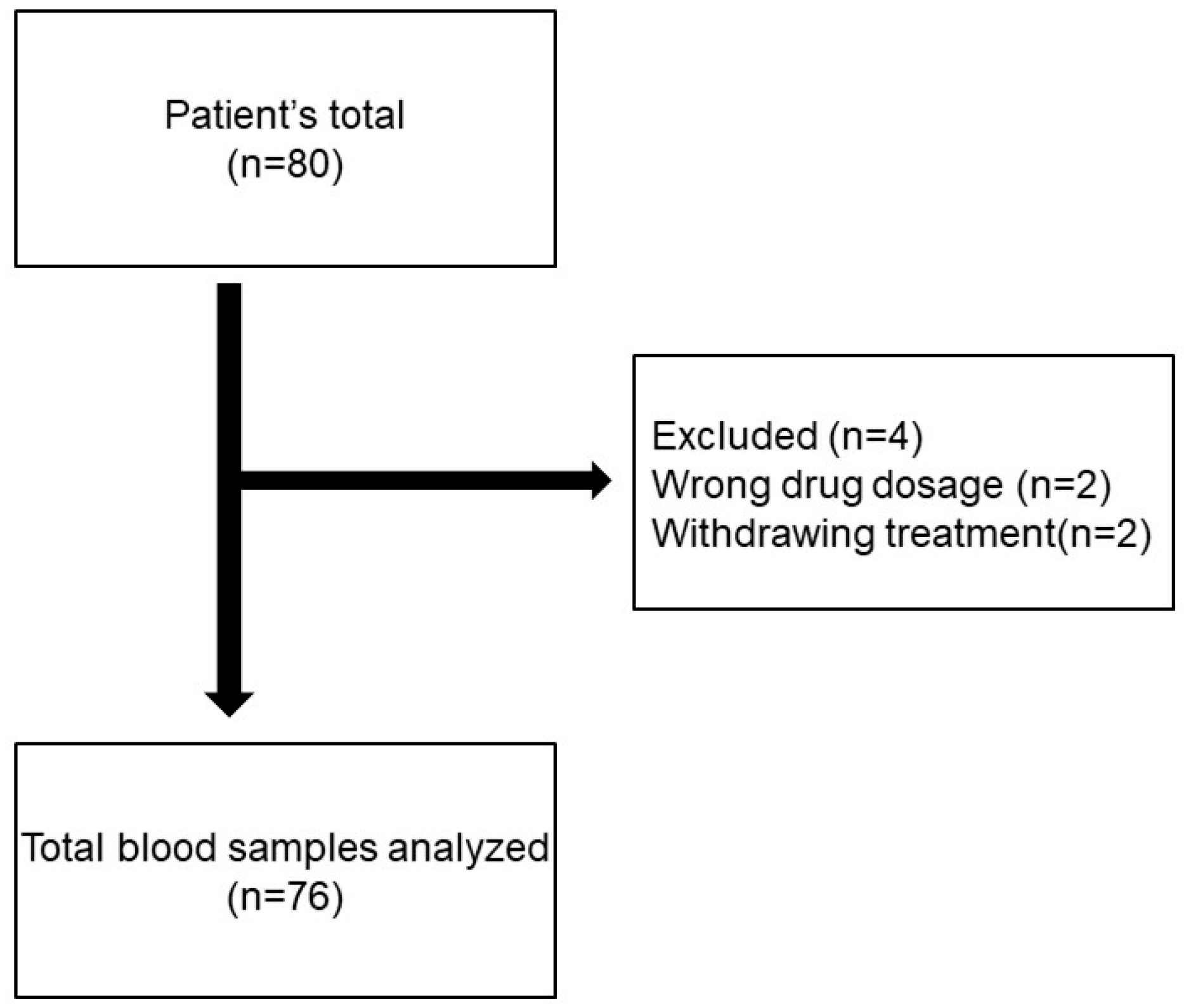
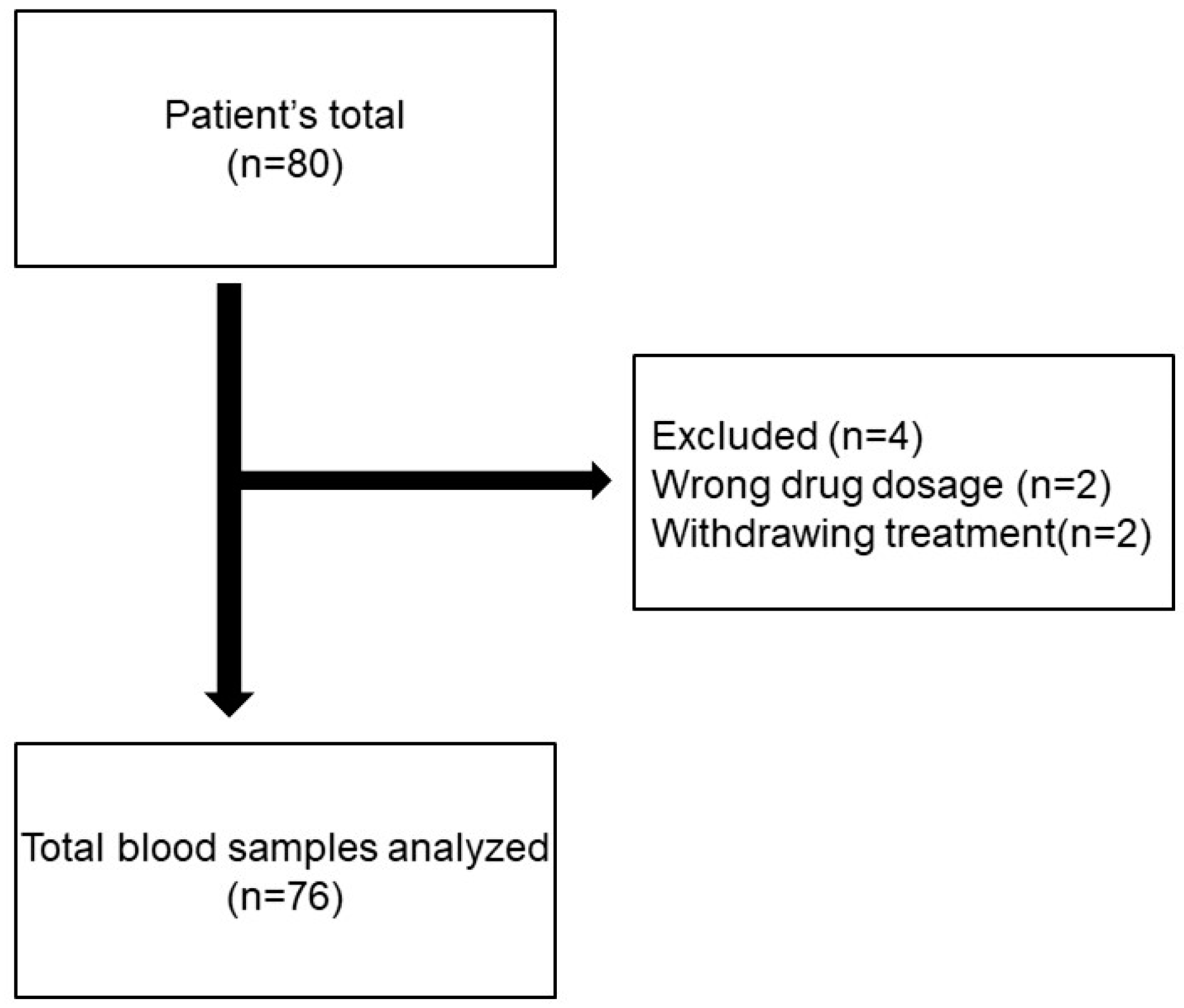
2.1. Study Design
2.2. Controlled Ovarian Stimulation (COS)
2.3. Collection of Blood Samples
2.4. Measurement of PON Activity
2.5. Measurement of MPO Level
2.6. Determination of Dysfunctional HDL
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Zegers-Hochschild, F.; Adamson, G.D.; Dyer, S.; Racowsky, C.; de Mouzon, J.; Sokol, R.; Rienzi, L.; Sunde, A.; Schmidt, L.; Cooke, I.D.; et al. The International Glossary on Infertility and Fertility Care. Fertil. Steril. 2017, 108, 393–406. [Google Scholar] [CrossRef]
- Mol, B.W.; Hart, R.J. Unexplained Infertility. Semin. Reprod Med. 2020, 38, 1–2. [Google Scholar] [CrossRef]
- Penzias, A.; Bendikson, K.; Falcone, T.; Hansen, K.; Hill, M.; Jindal, S.; Mersereau, J.; Racowsky, C.; Rebar, R.; Steiner, A.Z.; et al. Evidence-based treatments for couples with unexplained infertility: A guideline. Fertil. Steril. 2020, 113, 305–322. [Google Scholar] [CrossRef]
- Rehman, R.; Rajpar, H.I.; Ashraf, M.; Iqbal, N.T.; Lalani, S.; Alam, F. Role of oxidative stress and altered thyroid hormones in unexplained infertility. J. Pak. Med. Assoc. 2020, 70, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Ghulmiyyah, J.; Sharma, R.; Halabi, J.; Agarwal, A. Power of proteomics in linking oxidative stress and female infertility. BioMed Res. Int. 2014, 2014, 916212. [Google Scholar] [CrossRef]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. Biological Consequences of Dysfunctional HDL. Curr. Med. Chem. 2019, 26, 1644–1664. [Google Scholar] [CrossRef] [PubMed]
- Riwanto, M.; Rohrer, L.; von Eckardstein, A.; Landmesser, U. Dysfunctional HDL: From structure-function-relationships to biomarkers. Handb Exp. Pharmacol. 2015, 224, 337–366. [Google Scholar] [PubMed]
- Khirfan, G.; Li, M.; Wang, X.; DiDonato, J.A.; Dweik, R.A.; Heresi, G.A. Abnormal levels of apolipoprotein A-I in chronic thromboembolic pulmonary hypertension. Pulm. Circ. 2021, 11, 20458940211010371. [Google Scholar] [CrossRef] [PubMed]
- Zuin, M.; Trentini, A.; Marsillach, J.; D’Amuri, A.; Bosi, C.; Roncon, L.; Passaro, A.; Zuliani, G.; Mackness, M.; Cervellati, C. Paraoxonase-1 (PON-1) Arylesterase Activity Levels in Patients with Coronary Artery Disease: A Meta-Analysis. Dis. Markers 2022, 10, 4264314. [Google Scholar] [CrossRef]
- Tangeten, C.; Zouaoui Boudjeltia, K.; Delporte, C.; Van Antwerpen, P.; Korpak, K. Unexpected Role of MPO-Oxidized LDLs in Atherosclerosis: In between Inflammation and Its Resolution. Antioxidants 2022, 11, 874. [Google Scholar] [CrossRef]
- Ndrepepa, G. Myeloperoxidase—A bridge linking inflammation and oxidative stress with cardiovascular disease. Clin. Chim. Acta 2019, 493, 36–51. [Google Scholar] [CrossRef]
- Emami Razavi, A.; Basati, G.; Varshosaz, J.; Abdi, S. Association between HDL particles size and myeloperoxidase/ paraoxonase-1 (MPO/PON1) ratio in patients with acute coronary syndrome. Acta Med. Iran. 2013, 51, 365–371. [Google Scholar]
- Haraguchi, Y.; Toh, R.; Hasokawa, M.; Nakajima, H.; Honjo, T.; Otsui, K.; Mori, K.; Miyamoto-Sasaki, M.; Shinohara, M.; Nishimura, K.; et al. Serum myeloperoxidase/paraoxonase 1 ratio as potential indicator of dysfunctional high-density lipoprotein and risk stratification in coronary artery disease. Atherosclerosis 2014, 234, 288–294. [Google Scholar] [CrossRef]
- Balaban, B.; Brison, D.; Calderon, G.; Catt, J.; Conaghan, J.; Cowan, L.; Ebner, T.; Gardner, D.; Hardarson, T.; Lundin, K.; et al. Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Hum. Reprod. 2011, 26, 1270–1283. [Google Scholar]
- Rehman, K.S.; Bukulmez, O.; Langley, M.; Carr, B.R.; Nackley, A.C.; Doody, K.M.; Doody, K.J. Late stages of embryo progression are a much better predictor of clinical pregnancy than early cleavage in intracytoplasmic sperm injection and in vitro fertilization cycles with blastocyst-stage transfer. Fertil. Steril. 2007, 87, 1041–1052. [Google Scholar] [CrossRef]
- Lambalk, C.B.; Banga, F.R.; Huirne, J.A.; Toftager, M.; Pinborg, A.; Homburg, R.; van der Veen, F.; van Wely, M. GnRH antagonist versus long agonist protocols in IVF: A systematic review and meta-analysis accounting for patient type. Hum. Reprod. Update 2017, 23, 560–579. [Google Scholar] [CrossRef] [PubMed]
- Gardner, D.K. In-Vitro Culture of Human Blastocyst. In Towards Reproductive Certainty: Infertility and Genetics Beyond; Parthenon Press: Nashville, Tennessee, 1999; pp. 378–388. [Google Scholar]
- Eckerson, H.W.; Wyte, C.M.; La Du, B.N. The human serum paraoxonase/arylesterase polymorphism. Am. J. Hum. Genet. 1983, 35, 1126–1138. [Google Scholar] [PubMed]
- Mendes, S.; Timóteo-Ferreira, F.; Almeida, H.; Silva, E. New Insights into the Process of Placentation and the Role of Oxidative Uterine Microenvironment. Oxid. Med. Cell. Longev. 2019, 25, 9174521. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Aponte-Mellado, A.; Premkumar, B.J.; Shaman, A.; Gupta, S. The effects of oxidative stress on female reproduction: A review. Reprod. Biol. Endocrinol. 2012, 10, 49. [Google Scholar] [CrossRef]
- Ertek, S. High-density Lipoprotein (HDL) Dysfunction and the Future of HDL. Curr. Vasc. Pharmacol. 2018, 16, 490–498. [Google Scholar] [CrossRef]
- Nagy, R.A.; van Montfoort, A.P.A.; Groen, H.; Homminga, I.; Andrei, D.; Mistry, R.H.; Anderson, J.L.C.; Hoek, A.; Tietge, U.J.F. Anti-oxidative function of follicular fluid HDL and outcomes of modified natural cycle-IVF. Sci. Rep. 2019, 9, 12817. [Google Scholar] [CrossRef] [PubMed]
- Şentürk, R.; Tola, E.N.; Bozkurt, M.; Doğuç, D.K. The role of oxidant status on the etiopathogenesis of unexplained infertility and intracytoplasmic sperm injection—Embryo transfer success: A case-control study. J. Obstet. Gynaecol. 2022, 42, 1312–1318. [Google Scholar] [CrossRef]
- Verit, F.F.; Yildiz Zeyrek, F.; Zebitay, A.G.; Akyol, H. Cardiovascular risk may be increased in women with unexplained infertility. Clin. Exp. Reprod. Med. 2017, 44, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Pekel, A.; Gönenç, A.; Turhan, N.; Kafalı, H. Changes of sFas and sFasL, oxidative stress markers in serum and follicular fluid of patients undergoing IVF. J. Assist. Reprod. Genet. 2014, 32, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Younis, A.; Hawkins, K.; Mahini, H.; Butler, W.; Garelnabi, M. Serum tumor necrosis factor-α, interleukin-6, monocyte chemotactic protein-1 and paraoxonase-1 profiles in women with endometriosis, PCOS, or unexplained infertility. J. Assist. Reprod. Genet. 2014, 31, 1445–1451. [Google Scholar] [CrossRef]
- Homer, H.A. The Role of Oocyte Quality in Explaining “Unexplained” Infertility. Semin. Reprod. Med. 2020, 38, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Cajas, Y.N.; Cañón-Beltrán, K.; Ladrón de Guevara, M.; Millán de la Blanca, M.G.; Ramos-Ibeas, P.; Gutiérrez-Adán, A.; Rizos, D.; González, E.M. Antioxidant Nobiletin Enhances Oocyte Maturation and Subsequent Embryo Development and Quality. Int. J. Mol. Sci. 2020, 21, 5340. [Google Scholar] [CrossRef]
- Bedaiwy, M.; Agarwal, A.; Said, T.M.; Goldberg, J.M.; Sharma, R.K.; Worley, S.; Falcone, T. Role of total antioxidant capacity in the differential growth of human embryos in vitro. Fertil. Steril. 2006, 86, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Velthut, A.; Zilmer, M.; Zilmer, K.; Kaart, T.; Karro, H.; Salumets, A. Elevated blood plasma antioxidant status is favourable for achieving IVF/ICSI pregnancy. Reprod. Biomed. Online 2013, 26, 345–352. [Google Scholar] [CrossRef]
- Hatırnaz, Ş.; Kanat, P.M. Day 3 embryo transfer versus day 5 blastocyst transfers: A prospective randomized controlled trial. Turk. J. Obstet. Gynecol. 2017, 14, 82–88. [Google Scholar] [CrossRef]
- Zech, N.H.; Lejeune, B.; Puissant, F.; Vanderzwalmen, S.; Zech, H.; Vanderzwalmen, P. Prospective evaluation of the optimal time for selecting a single embryo for transfer: Day 3 versus day 5. Fertil. Steril. 2007, 88, 244–246. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Parameters | Control Group (n = 36) | Study Group (n = 40) | p Values |
|---|---|---|---|
| Maternal age (years) * | 31.92 ± 3.99 | 32.2 ± 3.85 | 0.494 |
| Paternal age (years) * | 33.06 ± 5.81 | 34.78 ± 4.19 | 0.196 |
| BMI (kg/m2) | 25.48 ± 5.05 | 25.83 ± 4.16 | 0.203 |
| D3 FSH (mIU/mL) ** | 6.62 (5.63–13.2) | 6.18 (4.7–8.6) | 0.925 |
| D3 LH (mIU/mL) * | 6.87 ± 3.55 | 7.03 ± 3.08 | 0.181 |
| D3 E2 (pg/mL) ** | 34.35 (12.9–70.2) | 36.8 (20.8–263) | 0.171 |
| Total AF count ** | 13.5 (8–30) | 11 (5–30) | 0.06 |
| Number of cycles ** | 2 (1–4) | 2.5 (1–4) | 0.163 |
| Duration of infertility (month) * | 64.5 ± 39.4 | 75 ± 22.14 | 0.058 |
| Duration of stimulation (day) * | 10 ± 1.21 | 10.3 ± 1.06 | 0.529 |
| Total dosages of gonadotropin * | 1792.71 ± 654.58 | 1863.75 ± 556.23 | 0.033 *** |
| Parameters | Control Group (n = 36) | Study Group (n = 40) | p Values |
|---|---|---|---|
| Retrieved oocyte count ** | 8.5 (1–17) | 7 (5–24) | 0.337 |
| MII oocyte count * | 7.25 ± 4.48 | 6.4 ± 2.32 | 0.437 |
| Number of Grade 1 embryo ** | 1 (0–6) | 0.5 (0–2) | 0.024 *** |
| Number of Grade 2 embryo ** | 0.5 (0–2) | 1 (0–2) | 0.752 |
| Number of Grade 3 embryo ** | 0.5 (0–3) | 0.5 (0–2) | 0.888 |
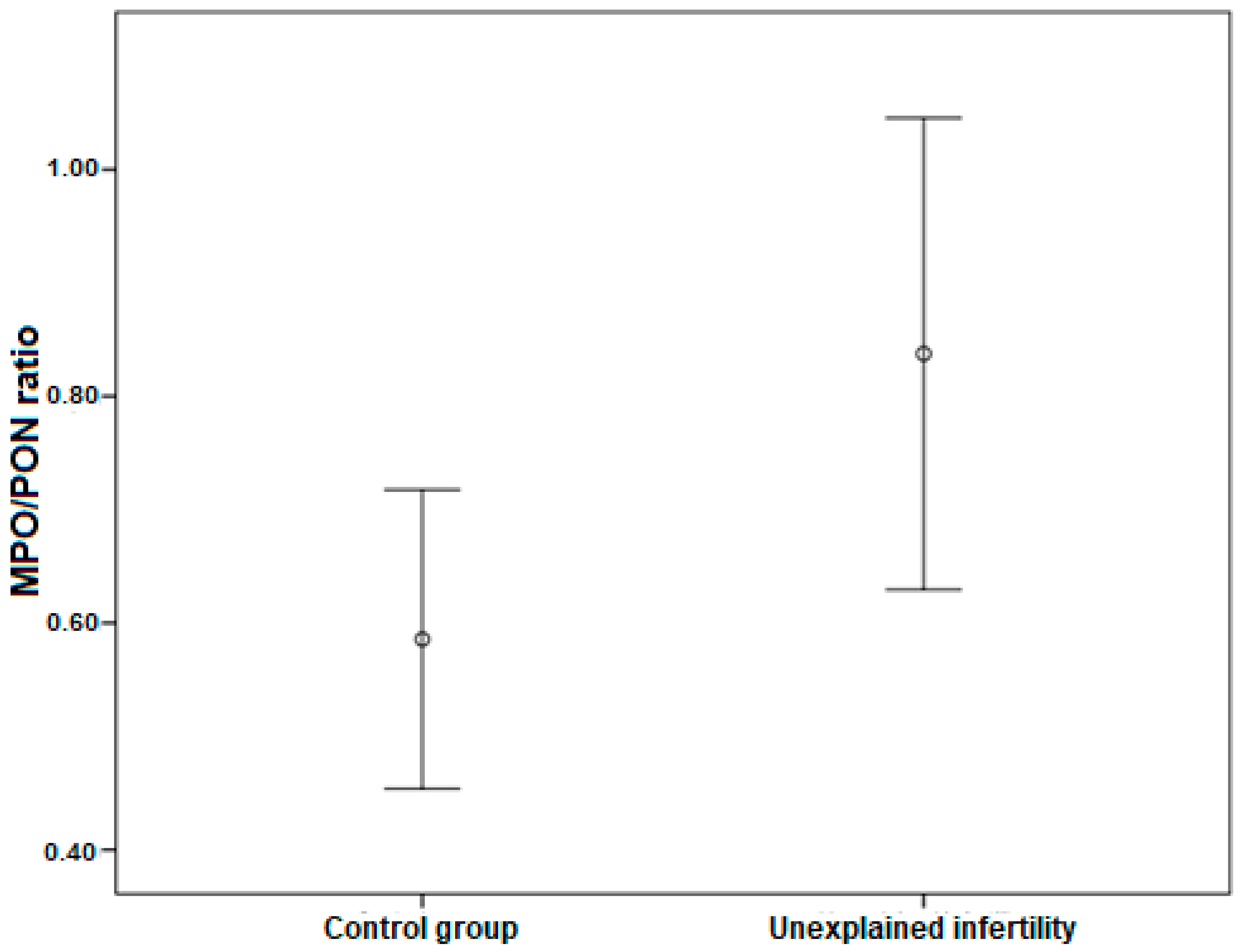
| Serum MPO/PON ratio * | 0.63 ± 0.32 | 1.04 ± 0.65 | 0.042 *** |
| MPO * | 76.44 ± 25.24 | 125.18 ± 79.48 | 0.010 *** |
| PON ** | 102.4 (82.27–880.76) | 117.55 (95.4–159.12) | 0.015 *** |
| BQS * | 32.11 ± 11.82 | 18.63 ± 9.57 | 0.020 *** |
| Clinical pregnancy (%) | 42.9% | 50% | 0.491 |
| Parameters | Control Group (n = 36) | Study Group (n = 40) | p Values | |
|---|---|---|---|---|
| Clinical pregnancy (%) | Day 3 ET | 0 | 50 | 0.725 |
| Day 5 ET | 66.7 | 50 | 0.028 * |
| Model I (R2 = 0.068) | Model II (R2 = 0.145) | Model III (R2 = 0.262) | ||||
|---|---|---|---|---|---|---|
| β | p | β | p | β | p | |
| Serum MPO/PON ratio | 0.291 | 0.030 * | 0.297 | 0.025 * | 0.314 | 0.012 * |
| BMI | 0.259 | 0.049 * | 0.356 | 0.006 * | ||
| Basal D3 FSH | 0.356 | 0.006 * | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erdoğan, K.; Sanlier, N.T.; Özen, E.U.; Erol, S.; Kahyaoğlu, I.; Neselioglu, S.; Erel, Ö.; Akar, S.; Üstün, Y.E. Evaluation of Dysfunctional HDL by Myeloperoxidase/Paraoxonase Ratio in Unexplained Infertility Patients Undergoing IVF/ICSI. J. Clin. Med. 2023, 12, 1506. https://doi.org/10.3390/jcm12041506
Erdoğan K, Sanlier NT, Özen EU, Erol S, Kahyaoğlu I, Neselioglu S, Erel Ö, Akar S, Üstün YE. Evaluation of Dysfunctional HDL by Myeloperoxidase/Paraoxonase Ratio in Unexplained Infertility Patients Undergoing IVF/ICSI. Journal of Clinical Medicine. 2023; 12(4):1506. https://doi.org/10.3390/jcm12041506
Chicago/Turabian StyleErdoğan, Kadriye, Nazli Tunca Sanlier, Emine Utlu Özen, Süleyman Erol, Inci Kahyaoğlu, Salim Neselioglu, Özcan Erel, Serra Akar, and Yaprak Engin Üstün. 2023. "Evaluation of Dysfunctional HDL by Myeloperoxidase/Paraoxonase Ratio in Unexplained Infertility Patients Undergoing IVF/ICSI" Journal of Clinical Medicine 12, no. 4: 1506. https://doi.org/10.3390/jcm12041506
APA StyleErdoğan, K., Sanlier, N. T., Özen, E. U., Erol, S., Kahyaoğlu, I., Neselioglu, S., Erel, Ö., Akar, S., & Üstün, Y. E. (2023). Evaluation of Dysfunctional HDL by Myeloperoxidase/Paraoxonase Ratio in Unexplained Infertility Patients Undergoing IVF/ICSI. Journal of Clinical Medicine, 12(4), 1506. https://doi.org/10.3390/jcm12041506