

Efficacy and Safety of Low-Dose Cyclosporine Relative to Immunomodulatory Drugs Used in Atopic Dermatitis: A Systematic Review and Meta-Analysis
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Analysis
3. Results
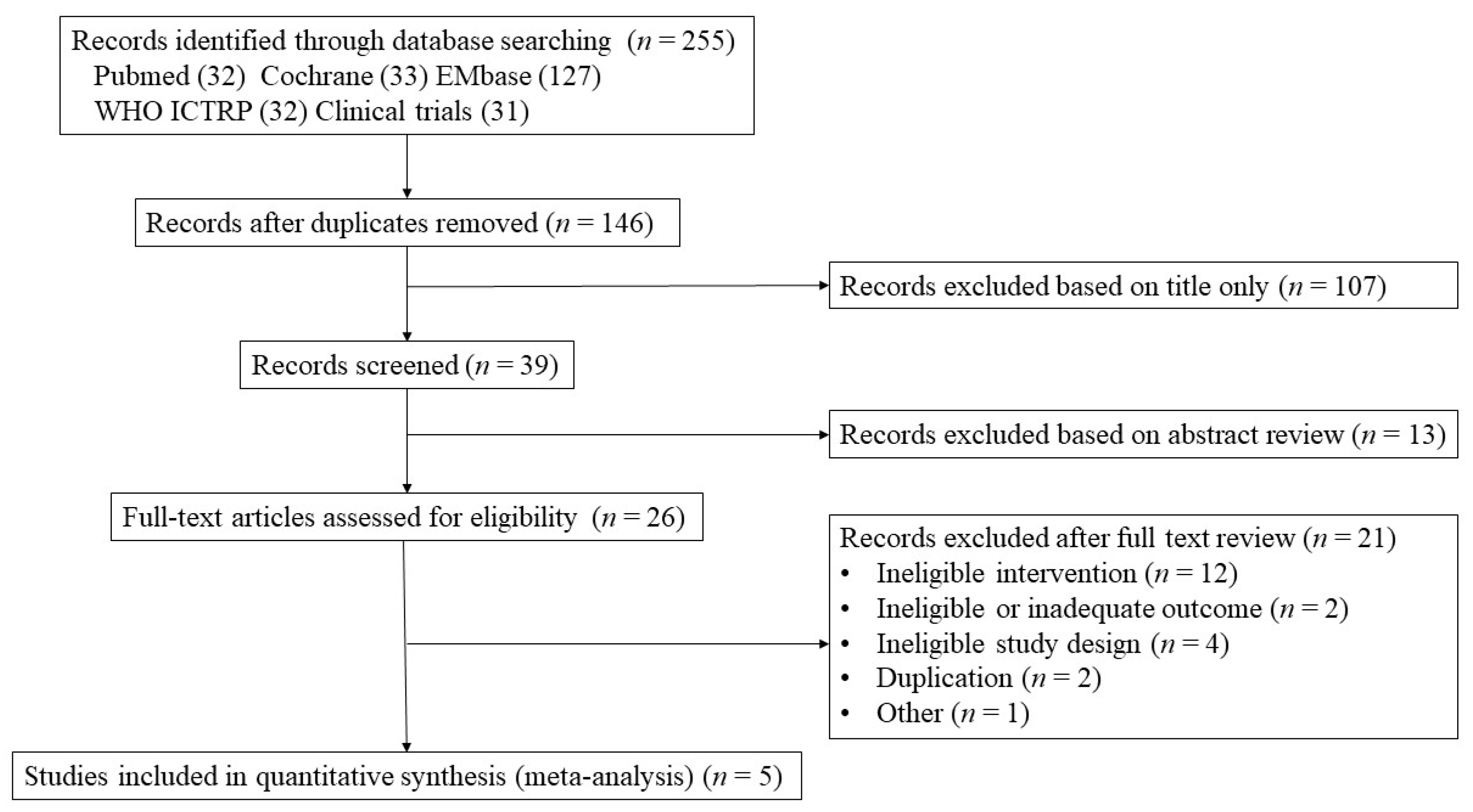
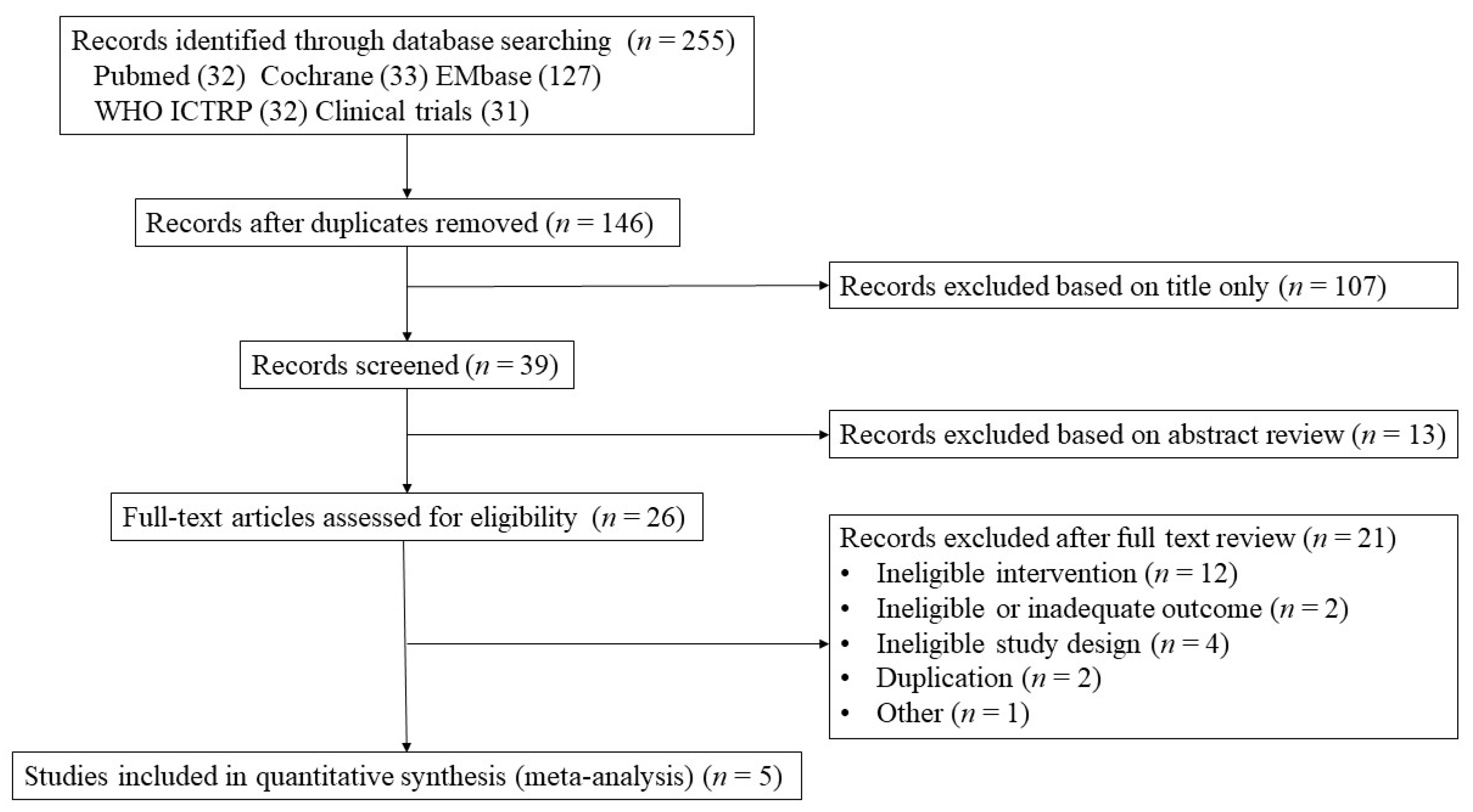
3.1. Study Selection
3.2. Study Characteristics
3.3. Outcome Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silverberg, J.I.; Simpson, E.L. Associations of childhood eczema severity: A US population-based study. Dermatitis 2014, 25, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Barbarot, S.; Auziere, S.; Gadkari, A.; Girolomoni, G.; Puig, L.; Simpson, E.L.; Margolis, D.J.; de Bruin-Weller, M.; Eckert, L. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy 2018, 73, 1284–1293. [Google Scholar] [CrossRef] [PubMed]
- Flohr, C.; Mann, J. New insights into the epidemiology of childhood atopic dermatitis. Allergy 2014, 69, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Sidbury, R.; Davis, D.M.; Cohen, D.E.; Cordoro, K.M.; Berger, T.G.; Bergman, J.N.; Chamlin, S.L.; Cooper, K.D.; Feldman, S.R.; Hanifin, J.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 3. Management and treatment with phototherapy and systemic agents. J. Am. Acad. Dermatol. 2014, 71, 327–349. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.; Swan, D.J.; Affleck, A.; Flohr, C.; Reynolds, N.J. Treatment of moderate-to-severe atopic eczema in adults within the U.K.: Results of a national survey of dermatologists. Br. J. Dermatol. 2017, 176, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Ariëns, L.F.M.; Gadkari, A.; van Os-Medendorp, H.; Ayyagari, R.; Terasawa, E.; Kuznik, A.; Chen, Z.; Bégo-Le Bagousse, G.; Lu, Y.; Rizova, E.; et al. Dupilumab Versus Cyclosporine for the Treatment of Moderate-to-Severe Atopic Dermatitis in Adults: Indirect Comparison Using the Eczema Area and Severity Index. Acta Derm. Venereol. 2019, 99, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Wollenberg, A.; Kinberger, M.; Arents, B.; Aszodi, N.; Avila Valle, G.; Barbarot, S.; Bieber, T.; Brough, H.A.; Calzavara Pinton, P.; Christen-Zäch, S.; et al. European guideline (EuroGuiDerm) on atopic eczema: Part I—Systemic therapy. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 1409–1431. [Google Scholar] [CrossRef]
- Siegels, D.; Heratizadeh, A.; Abraham, S.; Binnmyr, J.; Brockow, K.; Irvine, A.D.; Halken, S.; Mortz, C.G.; Flohr, C.; Schmid-Grendelmeier, P.; et al. Systemic treatments in the management of atopic dermatitis: A systematic review and meta-analysis. Allergy 2021, 76, 1053–1076. [Google Scholar] [CrossRef]
- Drucker, A.M.; Ellis, A.G.; Bohdanowicz, M.; Mashayekhi, S.; Yiu, Z.Z.N.; Rochwerg, B.; Di Giorgio, S.; Arents, B.W.M.; Burton, T.; Spuls, P.I.; et al. Systemic Immunomodulatory Treatments for Patients With Atopic Dermatitis: A Systematic Review and Network Meta-analysis. JAMA Dermatol. 2020, 156, 659–667. [Google Scholar] [CrossRef]
- Munro, C.S.; Levell, N.J.; Shuster, S.; Friedmann, P.S. Maintenance treatment with cyclosporin in atopic eczema. Br. J. Dermatol. 1994, 130, 376–380. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Goujon, C.; Viguier, M.; Staumont-Sallé, D.; Bernier, C.; Guillet, G.; Lahfa, M.; Ferrier Le Bouedec, M.C.; Cambazard, F.; Bottigioli, D.; Grande, S.; et al. Methotrexate Versus Cyclosporine in Adults with Moderate-to-Severe Atopic Dermatitis: A Phase III Randomized Noninferiority Trial. J. Allergy Clin. Immunol. Pract. 2018, 6, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Czech, W.; Bräutigam, M.; Weidinger, G.; Schöpf, E. A body-weight-independent dosing regimen of cyclosporine microemulsion is effective in severe atopic dermatitis and improves the quality of life. J. Am. Acad. Dermatol. 2000, 42, 653–659. [Google Scholar]
- Haeck, I.M.; Knol, M.J.; Ten Berge, O.; van Velsen, S.G.; de Bruin-Weller, M.S.; Bruijnzeel-Koomen, C.A. Enteric-coated mycophenolate sodium versus cyclosporin A as long-term treatment in adult patients with severe atopic dermatitis: A randomized controlled trial. J. Am. Acad. Dermatol. 2011, 64, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- El-Khalawany, M.A.; Hassan, H.; Shaaban, D.; Ghonaim, N.; Eassa, B. Methotrexate versus cyclosporine in the treatment of severe atopic dermatitis in children: A multicenter experience from Egypt. Eur. J. Pediatr. 2013, 172, 351–356. [Google Scholar] [CrossRef]
- Schmitt, J.; Schäkel, K.; Fölster-Holst, R.; Bauer, A.; Oertel, R.; Augustin, M.; Aberer, W.; Luger, T.; Meurer, M. Prednisolone vs. ciclosporin for severe adult eczema. An investigator-initiated double-blind placebo-controlled multicentre trial. Br. J. Dermatol. 2010, 162, 661–668. [Google Scholar] [CrossRef]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part II. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 850–878. [Google Scholar] [CrossRef]
- Schmitt, J.; Schmitt, N.; Meurer, M. Cyclosporin in the treatment of patients with atopic eczema—A systematic review and meta-analysis. J. Eur. Acad. Dermatol. Venereol. 2007, 21, 606–619. [Google Scholar] [CrossRef]
- Van der Schaft, J.; van Zuilen, A.D.; Deinum, J.; Bruijnzeel-Koomen, C.A.; de Bruin-Weller, M.S. Serum creatinine levels during and after long-term treatment with cyclosporine A in patients with severe atopic dermatitis. Acta Derm. Venereol. 2015, 95, 963–967. [Google Scholar] [CrossRef]
- Van Joost, T.; Heule, F.; Korstanje, M.; van den Broek, M.J.; Stenveld, H.J.; van Vloten, W.A. Cyclosporin in atopic dermatitis: A multicentre placebo-controlled study. Br. J. Dermatol. 1994, 130, 634–640. [Google Scholar] [CrossRef]
- Wahlgren, C.F.; Scheynius, A.; Hägermark, O. Antipruritic effect of oral cyclosporin A in atopic dermatitis. Acta Derm. Venereol. 1990, 70, 323–329. [Google Scholar] [PubMed]
- Zonneveld, I.M.; De Rie, M.A.; Beljaards, R.C.; Van Der Rhee, H.J.; Wuite, J.; Zeegelaar, J.; Bos, J.D. The long-term safety and efficacy of cyclosporin in severe refractory atopic dermatitis: A comparison of two dosage regimens. Br. J. Dermatol. 1996, 135 (Suppl. S48), 15–20. [Google Scholar] [CrossRef] [PubMed]
- Gerbens, L.A.A.; Hamann, S.A.S.; Brouwer, M.W.D.; Roekevisch, E.; Leeflang, M.M.G.; Spuls, P.I. Methotrexate and azathioprine for severe atopic dermatitis: A 5-year follow-up study of a randomized controlled trial. Br. J. Dermatol. 2018, 178, 1288–1296. [Google Scholar] [CrossRef] [PubMed]
- Dvorakova, V.; O’Regan, G.M.; Irvine, A.D. Methotrexate for Severe Childhood Atopic Dermatitis: Clinical Experience in a Tertiary Center. Pediatr. Dermatol. 2017, 34, 528–534. [Google Scholar] [CrossRef]
- Vestergaard, C.; Wollenberg, A.; Barbarot, S.; Christen-Zaech, S.; Deleuran, M.; Spuls, P.; Flohr, C.; Trzeciak, M.; von Kobyletzki, L.; Seneschal, J.; et al. European task force on atopic dermatitis position paper: Treatment of parental atopic dermatitis during preconception, pregnancy and lactation period. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1644–1659. [Google Scholar] [CrossRef]
- King, R.W.; Baca, M.J.; Armenti, V.T.; Kaplan, B. Pregnancy Outcomes Related to Mycophenolate Exposure in Female Kidney Transplant Recipients. Am. J. Transplant. 2017, 17, 151–160. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Characteristics | Control Group | Experimental Group | Considered Complications | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Country | STUDY PERIOD | Design | Population | AD Severity | n | Intervention | n | Intervention | ||
| Czech et al. (2000) [14] | Germany | Not described | RCT | Adults (≥18 years) | Severe | 53 | Start CsA 150 mg/day for 2 weeks and 50% reduced according to clinical response | 50 | Start CsA 300 mg/day for 2 weeks and 50% reduced according to clinical response | Skin disease, pain/nervous system disorder, GI disorder, metabolic disorder, cardiovascular disorder, gingival bleeding, others |
| Schmitt et al. (2010) [17] | Germany | February 2007 to November 2008 | RCT | Adults (18–55 years) | Severe | 17 | CsA 2.7–4.0 mg/kg/day for 6 weeks | 21 | Start prednisolone 0.5–0.8 mg/kg/d and tapered within 2 weeks | Exacerbation/rebound, common cold, hypertension, headache, weight gain, nausea/diarrhea, dysaesthesia, skin infection, dyslipidaemia, elevation of liver enzymes, elevation of creatinine |
| Haeck et al. (2011) [15] | Netherlands | November 2005 to November 2007 | RCT | Adults (≥18 years) | Severe | 26 | Start CsA 5 mg/kg/day for 6 weeks and reduced to 3 mg/kg/day for 30 weeks | 24 | Start CsA 5 mg/kg/day for 6 weeks and changed to MMF 1440 mg/day for 30 weeks | Nausea, altered defecation pattern, headache, fatigue, paraesthesia, muscle ache, infections, flu, hypertrichosis, gum hyperplasia, lower leg edema, creatinine increase, anemia, leucopenia, thrombopenia, liver enzyme increase, cholesterol increase, magnesium increase, hypertension |
| El-Khalawany et al. (2013) [16] | Egypt | Not described | RCT | Children (8–14 years) | Severe | 20 | CsA 2.5 mg/kg/day for 12 weeks | 20 | MTX 7.5 mg/week for 12 weeeks | GI disorder, hematologic disorder, elevated ESR, abnormal liver function tests, abnormal renal function tests, fever, fatigure, headache, hypertension, flu-like symptoms |
| Goujon et al. (2018) [13] | France | December 2008 to March 2012 | RCT | Adults (≥18 years) | Moderate to severe | 43 | CsA 2.5 mg/kg/day for 8 weeks and increased to 5 mg/kg/day for 16 weeks in poor response cases | 50 | MTX 15 mg/week for 8 weeeks and increased to 25 mg/week for 16 weeks in poor response cases | Infections, pain/nervous system disorder, GI disorder, hypertension, skin disease |
| Treatment | Number of Studies | Number of Observations | Estimate | 95% CI | p-Value |
|---|---|---|---|---|---|
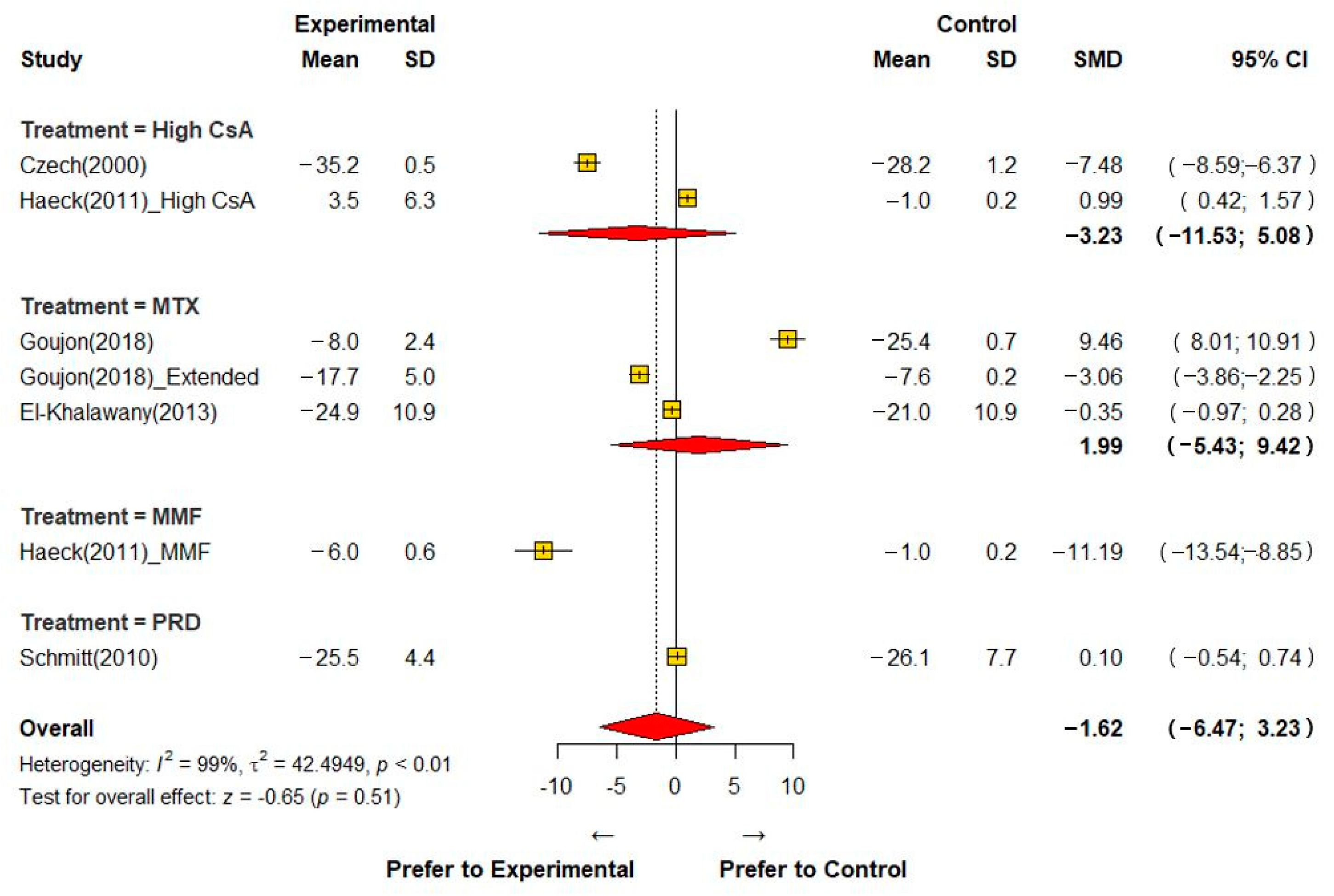
| Atopic Dermatitis Severity Score (SMD) | |||||
| High-dose CsA | 2 | 155 | −3.229 | (−11.534, −5.076) | <0.001 |
| MTX | 3 | 187 | 1.995 | (−5.435, 9.424) | 0.599 |
| MMF | 1 | 50 | −11.193 | (−13.540, −8.845) | <0.001 |
| PRD | 1 | 38 | 0.096 | (−0.543, 0.736) | 0.768 |
| Overall | 7 | 430 | −1.617 | (−6.468, 3.234) | 0.5135 |
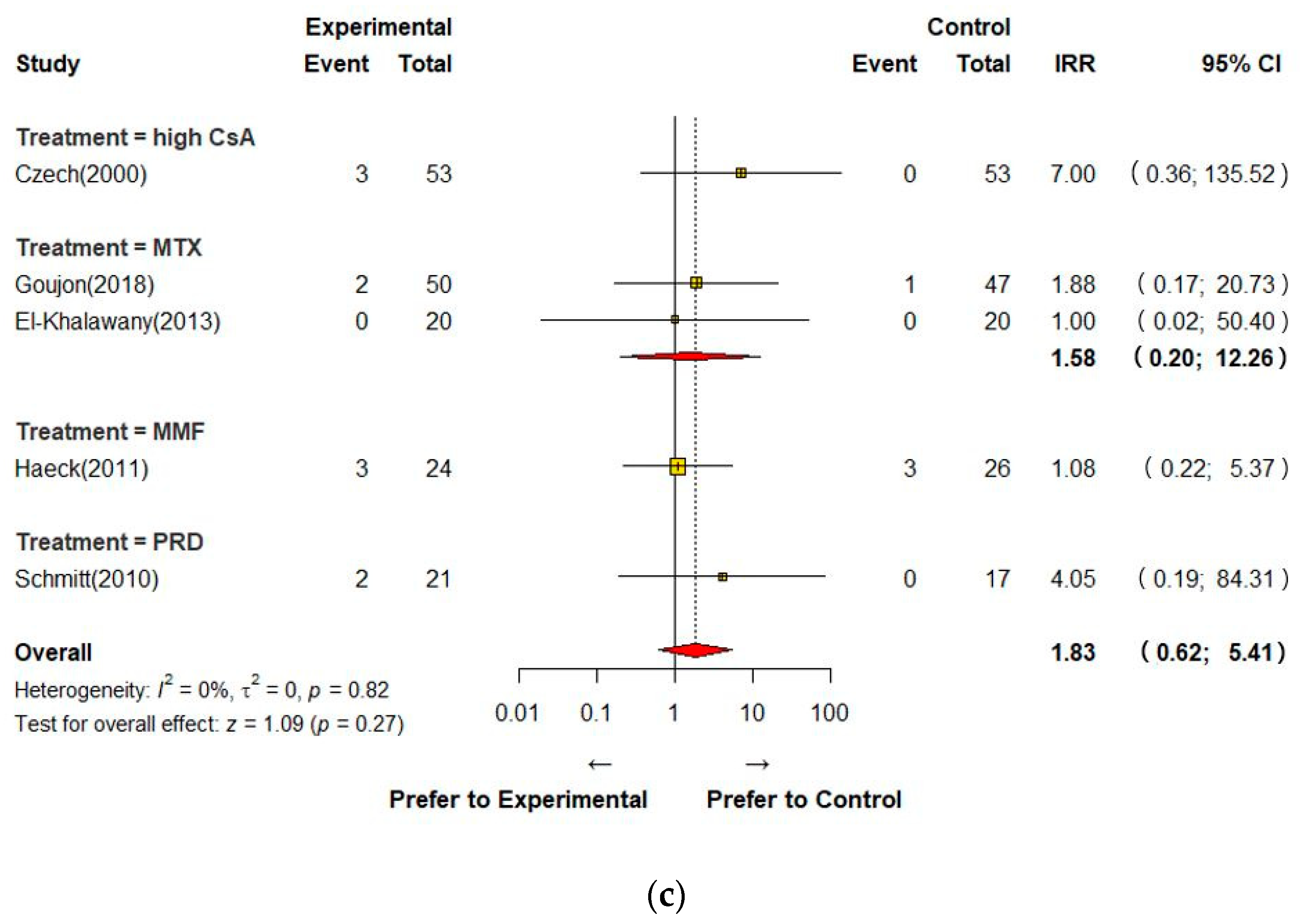
| Adverse Events (IRR) | |||||
| High-dose CsA | 1 | 106 | 1.2 | (0.663, 2.172) | 0.547 |
| MTX | 2 | 137 | 0.64 | (0.381, 1.076) | 0.092 |
| MMF | 1 | 50 | 0.634 | (0.444, 0.905) | 0.012 |
| PRD | 1 | 38 | 0.787 | (0.494, 1.253) | 0.313 |
| Overall | 5 | 331 | 0.725 | (0.564, 0.932) | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Kim, M.; Rhee, E.; Lee, M.-H.; Yang, H.-J.; Park, S.; Kim, H.S. Efficacy and Safety of Low-Dose Cyclosporine Relative to Immunomodulatory Drugs Used in Atopic Dermatitis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 1390. https://doi.org/10.3390/jcm12041390
Kim K, Kim M, Rhee E, Lee M-H, Yang H-J, Park S, Kim HS. Efficacy and Safety of Low-Dose Cyclosporine Relative to Immunomodulatory Drugs Used in Atopic Dermatitis: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(4):1390. https://doi.org/10.3390/jcm12041390
Chicago/Turabian StyleKim, Kyunghoon, Mina Kim, EunHee Rhee, Mi-Hee Lee, Hyeon-Jong Yang, Suyeon Park, and Hwan Soo Kim. 2023. "Efficacy and Safety of Low-Dose Cyclosporine Relative to Immunomodulatory Drugs Used in Atopic Dermatitis: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 4: 1390. https://doi.org/10.3390/jcm12041390
APA StyleKim, K., Kim, M., Rhee, E., Lee, M.-H., Yang, H.-J., Park, S., & Kim, H. S. (2023). Efficacy and Safety of Low-Dose Cyclosporine Relative to Immunomodulatory Drugs Used in Atopic Dermatitis: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(4), 1390. https://doi.org/10.3390/jcm12041390