

Clinicopathological and Treatment Patterns of Combined Small-Cell Lung Carcinoma with Future Insight to Treatment: A Population-Based Study

 ,
, 
 , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Characteristics
3.2. Tumor Characteristics
3.3. Lymph Node Status and Metastasis at the Time of Diagnosis
3.4. Treatment Characteristics
3.5. Survival Characteristics by Treatment Modality
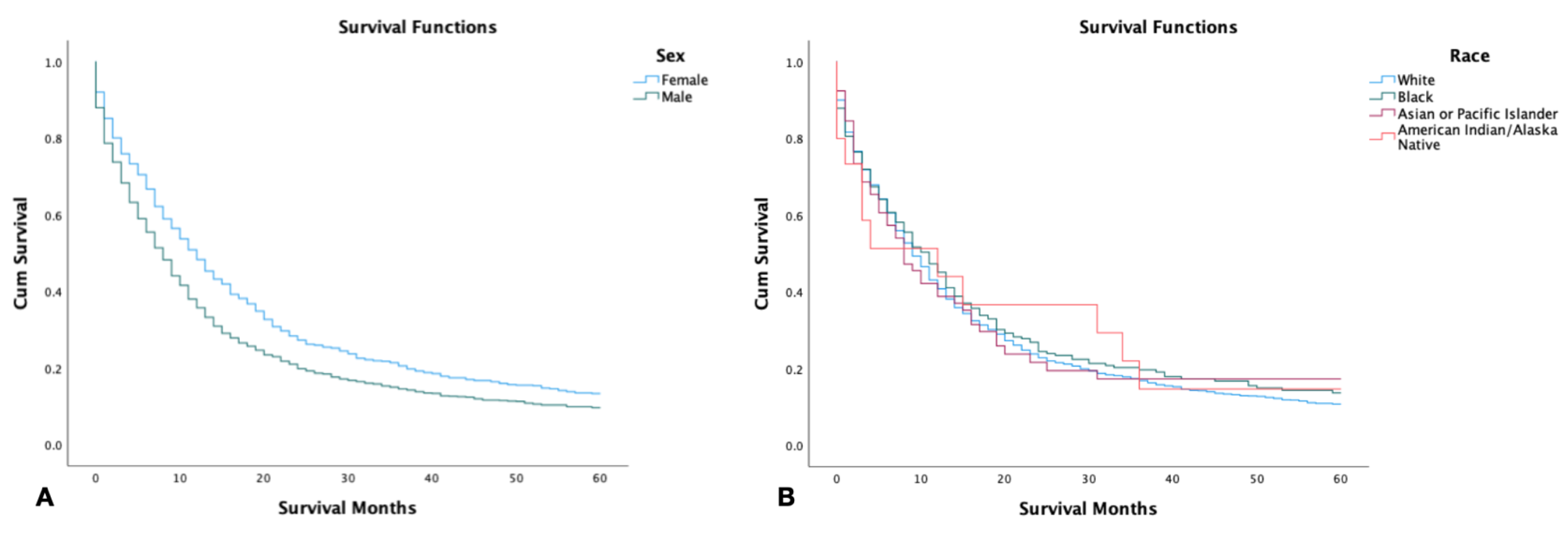
3.6. Survival by Gender and Race
3.7. Survival by Tumor Size, Grading, and Stage
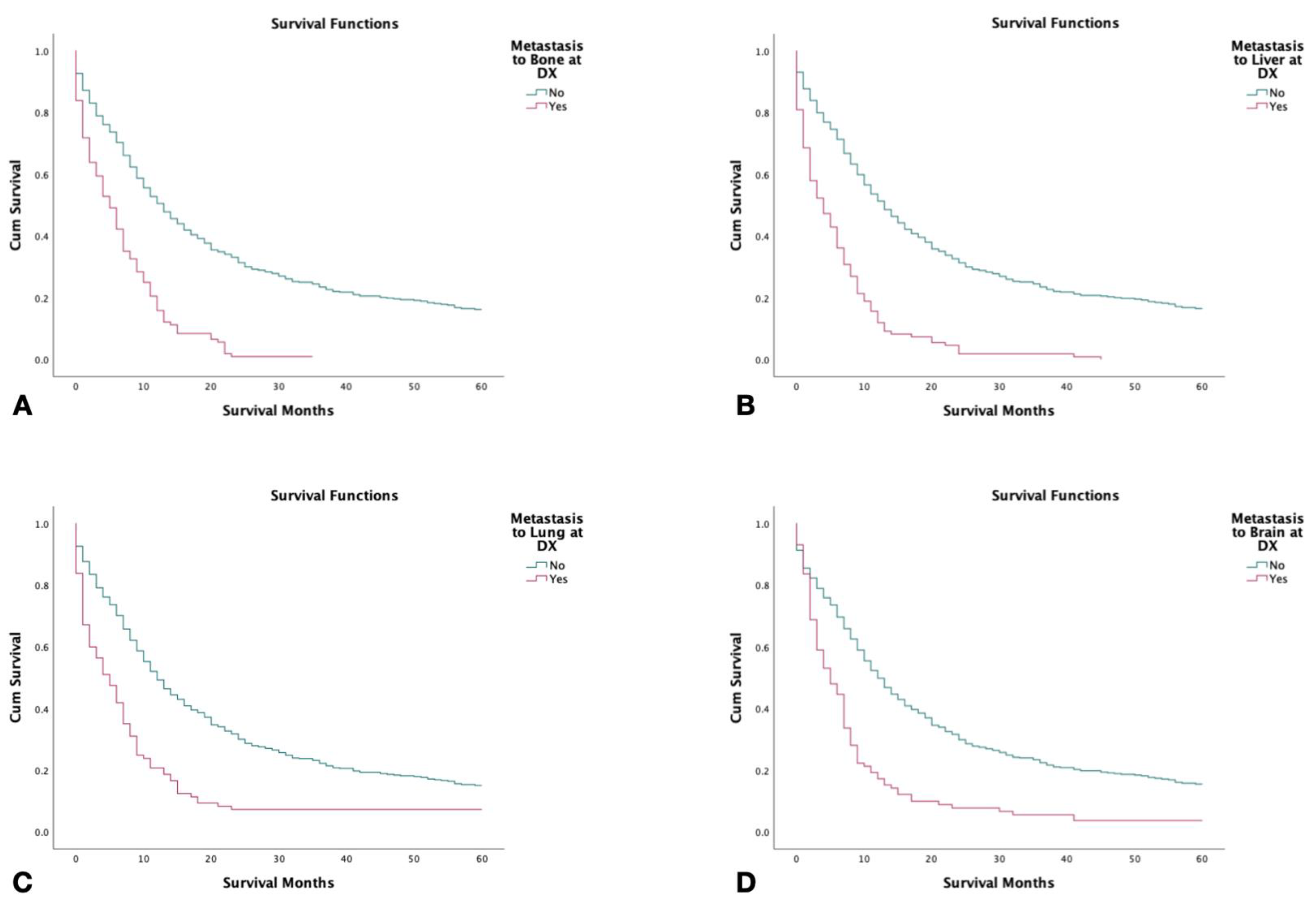
3.8. Survival with Metastasis to Liver, Bone, Brain, and Lung
3.9. Multivariate Analysis
4. Discussion
Genomic and Treatment Landscape of Combined Small-Cell Lung Cancer
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mbeje, N.P.; Ginindza, T.; Jafta, N. Epidemiological Study of Risk Factors for Lung Cancer in KwaZulu-Natal, South Africa. Int. J. Environ. Res. Public Health 2022, 19, 6752. [Google Scholar] [CrossRef]
- Loukeri, A.A.; Kampolis, C.F.; Ntokou, A.; Tsoukalas, G.; Syrigos, K. Metachronous and Synchronous Primary Lung Cancers: Diagnostic Aspects, Surgical Treatment, and Prognosis. Clin. Lung Cancer 2015, 16, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Thoracic Tumours WHO Classification of Tumours, 5th ed.WHO Classification of Tumours Editorial Board (Ed.) IARC Publications: Lyon, France, 2021; Volume 5, Available online: https://publications.iarc.fr/Book-And-Report-Series/Who-Classification-Of-Tumours/Thoracic-Tumours-2021 (accessed on 21 October 2022).
- Govindan, R.; Page, N.; Morgensztern, D.; Read, W.; Tierney, R.; Vlahiotis, A.; Spitznagel, E.L.; Piccirillo, J. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: Analysis of the surveillance, epidemiologic, and end results database. J. Clin. Oncol. 2006, 24, 4539–4544. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Lu, H. Combined small-cell lung carcinoma. OncoTargets Ther. 2018, 11, 3505–3511. [Google Scholar] [CrossRef] [PubMed]
- Babakoohi, S.; Fu, P.; Yang, M.; Linden, P.A.; Dowlati, A. Combined SCLC Clinical and Pathologic Characteristics. Clin. Lung Cancer 2013, 14, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Wallace, A.S.; Arya, M.; Frazier, S.R.; Westgate, S.; Wang, Z.; Doll, D. Combined small-cell lung carcinoma: An institutional experience. Thorac. Cancer 2014, 5, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Yang, H.; Zhao, H.; Lang, B.; Yu, X.; Xiao, P.; Zhang, X. Clinical outcomes of surgically resected combined small cell lung cancer: A two-institutional experience. J. Thorac. Dis. 2017, 9, 151–158. Available online: https://pubmed.ncbi.nlm.nih.gov/28203418 (accessed on 21 October 2022). [CrossRef] [PubMed]
- Nicholson, S.A.; Beasley, M.B.; Brambilla, E.; Hasleton, P.S.; Colby, T.V.; Sheppard, M.N.; Falk, R.; Travis, W.D. Small cell lung carcinoma (SCLC): A clinicopathologic study of 100 cases with surgical specimens. Am. J. Surg. Pathol. 2002, 26, 1184–1197. [Google Scholar] [CrossRef]
- Siegele, B.J.; Shilo, K.; Chao, B.H.; Carbone, D.P.; Zhao, W.; Ioffe, O.; Franklin, W.A.; Edelman, M.J.; Aisner, D.L. Epidermal growth factor receptor (EGFR) mutations in small cell lung cancers: Two cases and a review of the literature. Lung Cancer 2016, 95, 65–72. Available online: https://pubmed.ncbi.nlm.nih.gov/27040854 (accessed on 25 October 2022). [CrossRef]
- Lu, H.-Y.; Mao, W.-M.; Cheng, Q.-Y.; Chen, B.; Cai, J.-F.; Wang, X.-J.; Wang, Z.; Xie, F.-J. Mutation status of epidermal growth factor receptor and clinical features of patients with combined small cell lung cancer who received surgical treatment. Oncol. Lett. 2012, 3, 1288–1292. [Google Scholar] [CrossRef]
- Quan, A.L.; Videtic, G.M.M.; Suh, J.H. Brain metastases in small cell lung cancer. Oncology 2004, 18, 961–972; discussion 974, 979–980, 987. [Google Scholar]
- NCCN Guidelines. Available online: https://www.nccn.org/guidelines/category_1 (accessed on 4 February 2022).
- Wang, X.; Jiang, R.; Li, K. Prognostic Significance of Pretreatment Laboratory Parameters in Combined Small-Cell Lung Cancer. Cell Biochem. Biophys. 2014, 69, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Men, Y.; Department of Radiation Oncology; Hui, Z.; Liang, J.; Feng, Q.; Chen, D.; Zhang, H.; Xiao, Z.; Zhou, Z.; Yin, W.; et al. Further understanding of an uncommon disease of combined small cell lung cancer: Clinical features and prognostic factors of 114 cases. Chin. J. Cancer Res. 2016, 28, 486–494. Available online: https://pubmed.ncbi.nlm.nih.gov/27877007 (accessed on 25 October 2022). [CrossRef] [PubMed]
- Guo, Y.; Yang, L.; Liu, L.; Wei, J.; Teng, F.; Zhang, J.; Zhu, Y.; Xing, P.; Li, J. Comparative study of clinicopathological characteristics and prognosis between combined and pure small cell lung cancer (SCLC) after surgical resection. Thorac. Cancer 2020, 11, 2782–2792. [Google Scholar] [CrossRef] [PubMed]
- Simbolo, M.; Centonze, G.; Ali, G.; Garzone, G.; Taormina, S.; Sabella, G.; Ciaparrone, C.; Mafficini, A.; Grillo, F.; Mangogna, A.; et al. Integrative molecular analysis of combined small-cell lung carcinomas identifies major subtypes with different therapeutic opportunities. ESMO Open 2021, 7, 100308. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; written on behalf of the AME Lung Cancer Collaborative Group; Zhang, L.; Luo, J.; Ge, T.; Fan, P.; Sun, L.; Hou, L.; Li, J.; Yu, H.; et al. Comprehensive genomic profiling of combined small cell lung cancer. Transl. Lung Cancer Res. 2021, 10, 636–650. [Google Scholar] [CrossRef]
- My Cancer Genome. Combined Small Cell Lung Carcinoma. Available online: https://www.mycancergenome.org/content/disease/combined-small-cell-lung-carcinoma/ (accessed on 13 February 2022).
- Niitsu, T.; Shiroyama, T.; Miyake, K.; Noda, Y.; Kido, K.; Hara, R.; Enomoto, T.; Adachi, Y.; Amiya, S.; Suga, Y.; et al. Combined small cell lung carcinoma harboring ALK rearrangement: A case report and literature review. Thorac. Cancer 2020, 11, 3625–3630. [Google Scholar] [CrossRef]
- Gan, Y.; Liu, P.; Luo, T. Successful Treatment of an Elderly Patient With Combined Small Cell Lung Cancer Receiving Anlotinib: A Case Report. Front. Oncol. 2021, 11, 775201. [Google Scholar] [CrossRef]
- AstraZeneca. NCT03345810: Durvalumab (MEDI4736) in Frail and Elder Patients with Metastatic NSCLC. Available online: https://clinicaltrials.gov/ct2/show/NCT03345810 (accessed on 13 February 2022).
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-Line Atezolizumab plus Chemotherapy in Extensive-Stage Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H.; et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): A randomised, controlled, open-label, phase 3 trial. Lancet 2019, 394, 1929–1939. [Google Scholar] [CrossRef] [PubMed]
- US Food & Drug Administration. FDA Grants Accelerated Approval to Lurbinectedin for Metastatic Small Cell Lung Cancer. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-grants-accelerated-approval-lurbinectedin-metastatic-small-cell-lung-cancer (accessed on 13 February 2022).
- Scott, S.C.; Hann, C.L. Immunotherapy for small cell lung cancer: Established applications and novel approaches. Clin. Adv. Hematol. Oncol. 2021, 19, 654–663. [Google Scholar] [PubMed]
- Hiddinga, B.I.; Raskin, J.; Janssens, A.; Pauwels, P.; Van Meerbeeck, J.P. Recent developments in the treatment of small cell lung cancer. Eur. Respir. Rev. 2021, 30, 210079. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.; Ullah, A.; Munagala, R.; Singh, K.; Kozman, D.; Mattox, S.; Keshavamurthy, J.; Patel, N. Small cell carcinoma of the lung in a patient with previously treated synchronous adenocarcinoma and squamous cell carcinoma. Lung India 2021, 38, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wang, S.; Zhang, Y.; Wei, H.; Yu, J. Efficacy and safety of immune checkpoint inhibitors (ICIs) in extensive-stage small cell lung cancer (SCLC). J. Cancer Res. Clin. Oncol. 2020, 147, 593–606. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | |
|---|---|
| n (%) | 2126 (100.0) |
| Age (Mean ± SD) | 68.2 ± 10.1 |
| Gender | |
| Male | 1192 (56.1) |
| Female | 934 (43.9) |
| Race n (%) | |
| White | 1796 (84.5) |
| African American | 248 (11.7) |
| Asian or Pacific Islander | 66 (3.1) |
| American Indian/Alaskan Native | 15 (0.7) |
| Unknown | 1 (0.04) |
| Overall | |
|---|---|
| n (%) | 2126 (100.0) |
| Stage n (%) | |
| Localized | 279 (13.1) |
| Regional | 576 (27.1) |
| Distant | 1094 (51.5) |
| Unstaged/Unknown | 177 (8.3) |
| Tumor Size n (%) | |
| 0–3 cm | 460 (21.6) |
| 3.1–5 cm | 272 (12.8) |
| 5.1–7 cm | 155 (7.3) |
| >7 cm | 175 (8.2) |
| Lymph Node Status | |
|---|---|
| Known n (%) | 758 (35.7) |
| Positive Lymph Node n (%) | 464 (21.8) |
| Negative Lymph Node n (%) | 294 (13.8) |
| Unknown n (%) | 1368 (64.3) |
| Distant Metastasis | |
| Liver Metastasis n (%) | 147 (6.9) |
| Bone Metastasis n (%) | 143 (6.7) |
| Brain Metastasis n (%) | 130 (6.1) |
| Lung Metastasis n (%) | 117 (5.5) |
| Overall | |
|---|---|
| n (%) | 2126 (100.0) |
| Treatment n (%) | |
| Surgery Only | 362 (17.0) |
| Radiation Prior to Surgery | 9 (0.4) |
| Radiation After Surgery | 212 (10.0) |
| Radiation Before and After Surgery | 3 (0.1) |
| Chemotherapy | 964 (45.3) |
| Combination of Surgery and Chemotherapy | 219 (10.3) |
| Unknown | 357 (16.8) |
| Overall Mortality n (%) | 1841 (86.6) |
| Cancer-Specific Mortality n (%) | 1504 (70.7) |
| Survival | Overall % (95% C.I) | Cause- Specific % (95% C.I) | Surgery % (95% C.I) | Radiation % (95% C.I) | Chemotherapy % (95% C.I) | Combined Surgery and Chemotherapy % (95% C.I) |
|---|---|---|---|---|---|---|
| 1 year | 44.2 (41.6–46.7) | 46.4 (43.7–48.9) | 76.9 (72.1–81.0) | 60.4 (53.2–66.8) | 55 (51.7–58.2) | 80.8 (74.8–85.5) |
| 2 years | 24.9 (22.7–27.2) | 26.9 (24.5–29.3) | 57.8 (52.3–62.9) | 37.8 (31.0–44.6) | 29.9 (26.9–33.0 | 55.8 (48.7–62.3) |
| 3 years | 18.6 (16.6–20.7) | 21.0 (18.8–23.2) | 49.5 (43.9–54.8) | 29.7 (23.3–36.4) | 22.3 (19.5–25.2) | 46.4 (39.3–53.3) |
| 4 years | 14.5 (12.7–16.4) | 17.2 (15.1–19.3) | 43.1 (37.5–48.5) | 25.9 (19.8–32.5) | 17.5 (14.9–20.2) | 40.3 (33.2–47.2) |
| 5 years | 12.4 (10.7–14.3) | 15.2 (13.2–17.3) | 38.3 (32.7–43.8) | 22.2 (16.3–28.7) | 15.2 (12.7–17.9) | 34.7 (27.7–41.7) |
| Variables | Univariate Analysis | Multivariate Analysis | |
|---|---|---|---|
| ANOVA F Value (p-Value) | Hazard Ratio (p-Value) | Confidence Interval | |
| Male Sex | 25.1 (<0.001) | 1.2 (<0.001) | 1.1–1.3 |
| Undifferentiated Grade | 14.9 (<0.001) | 1.9 (0.042) | 1.0–3.6 |
| Regional Extent of Disease | 267.5 (<0.001) | 1.7 (<0.001) | 1.4–2.1 |
| Distant Extent of Disease | 3.7 (<0.001) | 3.1–4.4 | |
| Liver Metastasis | 25.9 (<0.001) | 3.5 (0.007) | 1.4–8.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, A.; Saeed, O.; Karki, N.R.; Goodbee, M.; Yasinzai, A.Q.K.; Waheed, A.; Heneidi, S.; Thomas, A.; Karim, N.A.; Johnson, J.; et al. Clinicopathological and Treatment Patterns of Combined Small-Cell Lung Carcinoma with Future Insight to Treatment: A Population-Based Study. J. Clin. Med. 2023, 12, 991. https://doi.org/10.3390/jcm12030991
Ullah A, Saeed O, Karki NR, Goodbee M, Yasinzai AQK, Waheed A, Heneidi S, Thomas A, Karim NA, Johnson J, et al. Clinicopathological and Treatment Patterns of Combined Small-Cell Lung Carcinoma with Future Insight to Treatment: A Population-Based Study. Journal of Clinical Medicine. 2023; 12(3):991. https://doi.org/10.3390/jcm12030991
Chicago/Turabian StyleUllah, Asad, Omer Saeed, Nabin Raj Karki, Mya Goodbee, Abdul Qahar Khan Yasinzai, Abdul Waheed, Saleh Heneidi, Anish Thomas, Nagla Abdel Karim, Joyce Johnson, and et al. 2023. "Clinicopathological and Treatment Patterns of Combined Small-Cell Lung Carcinoma with Future Insight to Treatment: A Population-Based Study" Journal of Clinical Medicine 12, no. 3: 991. https://doi.org/10.3390/jcm12030991
APA StyleUllah, A., Saeed, O., Karki, N. R., Goodbee, M., Yasinzai, A. Q. K., Waheed, A., Heneidi, S., Thomas, A., Karim, N. A., Johnson, J., Del Rivero, J., & Khan, J. (2023). Clinicopathological and Treatment Patterns of Combined Small-Cell Lung Carcinoma with Future Insight to Treatment: A Population-Based Study. Journal of Clinical Medicine, 12(3), 991. https://doi.org/10.3390/jcm12030991