
Iron Deficiency and Anemia in Male and Female Adolescent Athletes Who Engage in Ball Games
 ,
, 
Abstract
1. Introduction
2. Methods Section
2.1. Study Design
2.1.1. Participants
2.1.2. Primary Outcome Measures
2.2. Statistical Methods
2.3. Ethical Approval
3. Results
3.1. Blood Count and Iron Status among Adolescent Athletes
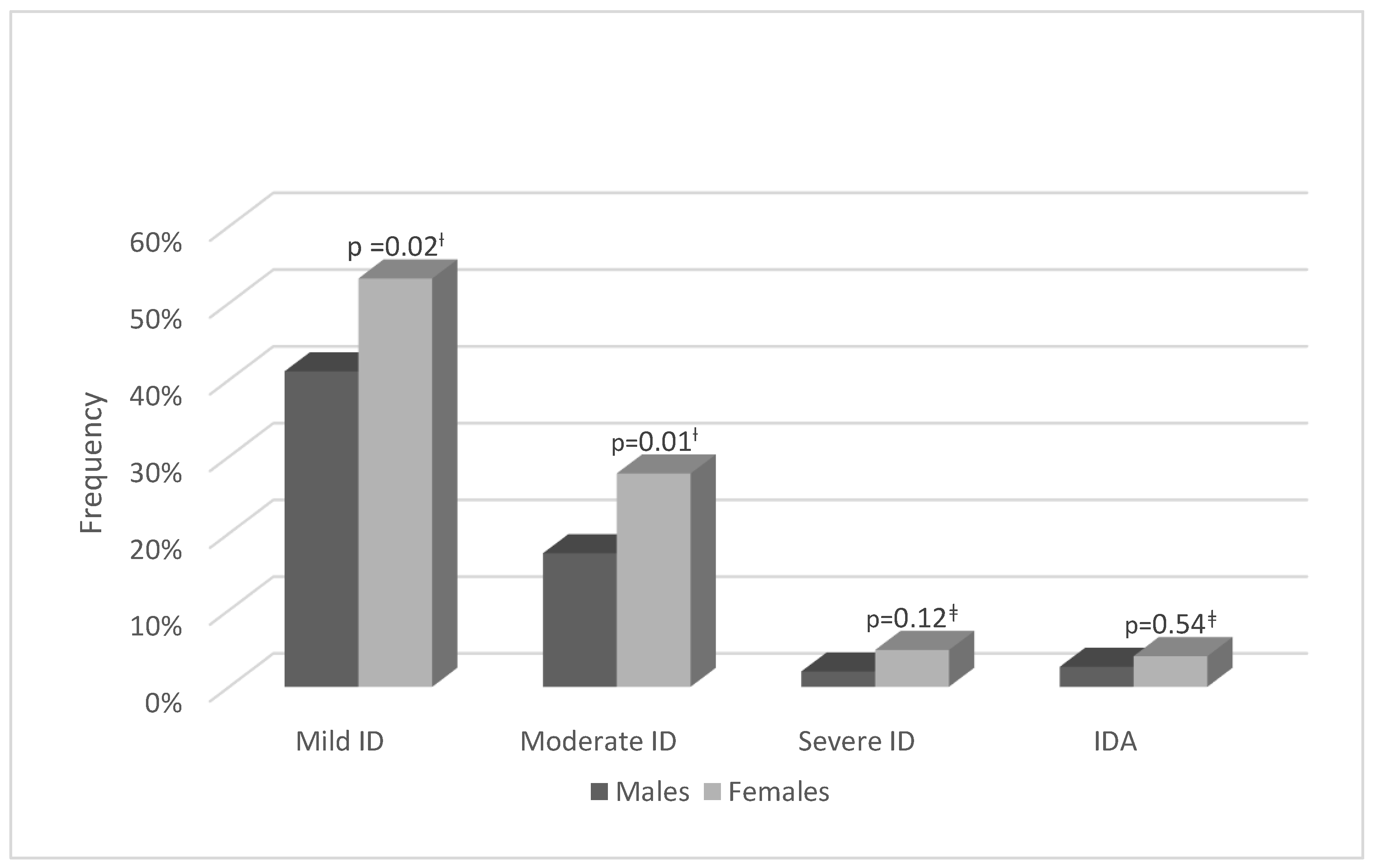
3.2. Comparison between Males and Females
3.3. Sub-Analysis according to Age Groups
4. Discussion
5. Study Limitations
6. Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO (Database Online) Archived. Iron Deficiency Anemia: Assessment, Prevention, and Control. WHO. 2004. Available online: http://www.who.int/nutrition/publications/micronutrients/anaemia_iron_deficiency/WHO_NHD_01.3/en/ (accessed on 4 January 2023).
- Camaschella, C. Iron-Deficiency Anemia. N. Engl. J. Med. 2015, 372, 1832–1843. [Google Scholar] [CrossRef]
- Harrison, T.; Kasper, D. Harrison’s Principles of Internal Medicine; McGraw-Hill Medical Publ. Division: New York, NY, USA, 2015. [Google Scholar]
- Clénin, G.; Cordes, M.; Huber, A.; Schumacher, Y.O.; Noack, P.; Scales, J.; Kriemler, S. Iron deficiency in sports—Definition, influence on performance and therapy. Swiss Med. Wkly. 2015, 145, w14196. [Google Scholar] [CrossRef]
- Lopez, A.; Cacoub, P.; Macdougall, I.C.; Peyrin-Biroulet, L. Iron deficiency anaemia. Lancet 2016, 387, 907–916. [Google Scholar] [CrossRef]
- Shoemaker, M.E.; Gillen, Z.; McKay, B.; Koehler, K.; Cramer, J.T. High Prevalence of Poor Iron Status Among 8- to 16-Year-Old Youth Athletes: Interactions among Biomarkers of Iron, Dietary Intakes, and Biological Maturity. J. Am. Coll. Nutr. 2019, 39, 155–162. [Google Scholar] [CrossRef]
- Toivo, K.; Kannus, P.; Kokko, S.; Alanko, L.; Heinonen, O.J.; Korpelainen, R.; Savonen, K.; Selänne, H.; Vasankari, T.; Kannas, L.; et al. Haemoglobin, iron status and lung function of adolescents participating in organised sports in the Finnish Health Promoting Sports Club Study. BMJ Open Sport Exerc. Med. 2020, 6, e000804. [Google Scholar] [CrossRef]
- Burden, R.J.; Morton, K.; Richards, T.; Whyte, G.P.; Pedlar, C. Is iron treatment beneficial in, iron-deficient but non-anaemic (IDNA) endurance athletes? A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Desbrow, B. Youth Athlete Development and Nutrition. Sports Med. 2021, 51 (Suppl. S1), 3–12. [Google Scholar] [CrossRef]
- Coates, A.; Mountjoy, M.; Burr, J. Incidence of Iron Deficiency and Iron Deficient Anemia in Elite Runners and Triathletes. Clin. J. Sport Med. 2017, 27, 493–498. [Google Scholar] [CrossRef]
- Rubeor, A.; Goojha, C.; Manning, J.; White, J. Does Iron Supplementation Improve Performance in Iron-Deficient Nonanemic Athletes? Sports Health Multidiscip. Approach 2018, 10, 400–405. [Google Scholar] [CrossRef]
- Sandström, G.; Rödjer, S.; Jacobsson, S.; Nelson, D.; Börjesson, M. Increased Level of Serum Hepcidin in Female Adolescent Athletes. Clin. J. Sport Med. 2018, 28, 180–183. [Google Scholar] [CrossRef]
- Pedlar, C.R.; Brugnara, C.; Bruinvels, G.; Burden, R. Iron balance and iron supplementation for the female athlete: A practical approach. Eur. J. Sport Sci. 2018, 18, 295–305. [Google Scholar] [CrossRef]
- Sim, M.; Garvican-Lewis, L.A.; Cox, G.R.; Govus, A.; McKay, A.K.A.; Stellingwerff, T.; Peeling, P. Iron considerations for the athlete: A narrative review. Eur. J. Appl. Physiol. 2019, 119, 1463–1478. [Google Scholar] [CrossRef]
- Eliakim, A.; Nemet, D.; Constantini, N. Screening blood tests in members of the Israeli National Olympic team. J. Sports Med. Phys. Fit. 2002, 42, 250–255. [Google Scholar]
- Merkel, D.; Moran, D.S.; Yanovich, R.; Evans, R.K.; Finestone, A.S.; Constantini, N.; Israeli, E. The Association between Hematological and Inflammatory Factors and Stress Fractures among Female Military Recruits. Med. Sci. Sports Exerc. 2008, 40 (Suppl. S11), S691–S697. [Google Scholar] [CrossRef]
- Parks, R.B.; Hetzel, S.J.; Brooks, M.A. Iron Deficiency and Anemia among Collegiate Athletes: A Retrospective Chart Review. Med. Sci. Sports Exerc. 2017, 49, 1711–1715. [Google Scholar] [CrossRef]
- Rowland, T. Iron Deficiency in Athletes: An Update. Am. J. Lifestyle Med. 2012, 6, 319–327. [Google Scholar] [CrossRef]
- Soppi, E.T. Iron deficiency without anemia—A clinical challenge. Clin. Case Rep. 2018, 6, 1082–1086. [Google Scholar] [CrossRef]
- DellaValle, D.M.; Haas, J.D. Impact of Iron Depletion Without Anemia on Performance in Trained Endurance Athletes at the Beginning of a Training Season: A Study of Female Collegiate Rowers. Int. J. Sport Nutr. Exerc. Metab. 2011, 21, 501–506. [Google Scholar] [CrossRef]
- DellaValle, D.M.; Haas, J.D. Iron Supplementation Improves Energetic Efficiency in Iron-Depleted Female Rowers. Med. Sci. Sports Exerc. 2014, 46, 1204–1215. [Google Scholar] [CrossRef]
- Haas, J.D.; Brownlie, T., 4th. Iron Deficiency and Reduced Work Capacity: A Critical Review of the Research to Determine a Causal Relationship. J. Nutr. 2001, 131, 676S–690S. [Google Scholar] [CrossRef]
- National Institute of Health. Iron–Fact Sheet for Health Professionals; Office of Dietary Supplements, NIH: Washington, DC, USA; U.S. Government Printing Office: Washington, DC, USA, 2001. [Google Scholar]
- Arthur-Cameselle, J.; Sossin, K.; Quatromoni, P. A qualitative analysis of factors related to eating disorder onset in female collegiate athletes and non-athletes. Eat. Disord. 2017, 25, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Watts, E. Athletes’ anaemia. A review of possible causes and guidelines on investigation. Br. J. Sports Med. 1989, 23, 81–83. [Google Scholar] [CrossRef]
- Peeling, P.; Sim, M.; Badenhorst, C.E.; Dawson, B.; Govus, A.; Abbiss, C.; Swinkels, D.W.; Trinder, D. Iron Status and the Acute Post-Exercise Hepcidin Response in Athletes. PLoS ONE 2014, 9, e93002. [Google Scholar] [CrossRef]
- Lev, B.; Rosenberg, E. Health Behaviors; Ministry of Health: Jerusalem, Israel, 2011. [Google Scholar]
- Sandström, G.; Börjesson, M.; Rödjer, S. Iron Deficiency in Adolescent Female Athletes—Is Iron Status Affected by Regular Sporting Activity? Clin. J. Sport Med. 2012, 22, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, L.; Hulten, L.; Lindstedt, G.; Lundberg, P.-A.; Mark, A.; Purens, J.; Svanberg, B.; Swolin, B. Prevalence of Iron Deficiency in Swedish Adolescents. Pediatr. Res. 1993, 34, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Israel. Mabat Youth–Second Israeli National Health and Nutrition Survey in 7th–12th Grade Students; ICDC: Jerusalem, Israel, 2017. [Google Scholar]
- Merkel, D.; Huerta, M.; Grotto, I.; Blum, D.; Tal, O.; Rachmilewitz, E.; Fibach, E.; Epstein, Y.; Shpilberg, O. Prevalence of iron deficiency and anemia among strenuously trained adolescents. J. Adolesc. Health 2005, 37, 220–223. [Google Scholar] [CrossRef]
- DellaValle, D.M. Iron supplementation for female athletes: Effects on iron status and performance outcomes. Curr. Sports Med. Rep. 2013, 12, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Dubnov, G.; Foldes, A.J.; Mann, G.; Magazanik, A.; Siderer, M.; Constantini, N. High Prevalence of Iron Deficiency and Anemia in Female Military Recruits. Mil. Med. 2006, 171, 866–869. [Google Scholar] [CrossRef]
- Pasricha, S.-R.; Low, M.; Thompson, J.; Farrell, A.; De-Regil, L.-M. Iron Supplementation Benefits Physical Performance in Women of Reproductive Age: A Systematic Review and Meta-Analysis. J. Nutr. 2014, 144, 906–914. [Google Scholar] [CrossRef]
- Dubnov, G.; Constantini, N.W. Prevalence of iron depletion and anemia in top-level basketball players. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 30–37. [Google Scholar] [CrossRef]
- Peeling, P.; McKay, A.K.A.; Pyne, D.B.; Guelfi, K.J.; McCormick, R.H.; Laarakkers, C.M.; Swinkels, D.W.; Garvican-Lewis, L.A.; Ross, M.L.R.; Sharma, A.P.; et al. Factors influencing the post-exercise hepcidin-25 response in elite athletes. Eur. J. Appl. Physiol. 2017, 117, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- CDCP. Recommendations to Prevent and Control Iron Deficiency in the United States. Morbidity and Mortality Weekly Report–Centers for Disease Control and Prevention Web Site. 2001. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00051880.htm (accessed on 4 January 2023).
- Sekhar, D.L.; Murray-Kolb, L.E.; Wang, L.; Kunselman, A.R.; Paul, I.M. Adolescent Anemia Screening During Ambulatory Pediatric Visits in the United States. J. Community Health 2015, 40, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Menal-Puey, S.; Martínez-Biarge, M.; Marques-Lopes, I. Developing a Food Exchange System for Meal Planning in Vegan Children and Adolescents. Nutrients 2018, 11, 43. [Google Scholar] [CrossRef] [PubMed]
- Constantini, N.W.; Eliakim, A.; Zigel, L.; Yaaron, M.; Falk, B. Iron status of highly active adolescents: Evidence of depleted iron stores in gymnasts. Int. J. Sport Nutr. Exerc. Metab. 2000, 10, 62–70. [Google Scholar] [CrossRef]


{kind=link}
| Gender | Age (Years) | HB (g/dL) | HCT (%) | RBC (M/μL) | MCV (fL) | MCH (pg) | Serum Ferritin (ng/mL) | |
|---|---|---|---|---|---|---|---|---|
| Male | n | 350 | 347 | 346 | 347 | 347 | 347 | 350 |
| Mean | 14.6 | 14.2 | 42.7 | 5.0 | 85.3 | 28.4 | 43.2 | |
| Median | 15.0 | 14.2 | 42.7 | 5.0 | 85.1 | 28.4 | 35.2 | |
| Standard Deviation | 1.7 | 1.0 | 2.9 | 0.3 | 4.3 | 1.6 | 30.8 | |
| Minimum | 11.0 | 9.3 | 29.7 | 4.0 | 68.0 | 21.0 | 8.0 | |
| Maximum | 18.0 | 17.7 | 50.8 | 6.0 | 97.0 | 32.8 | 260.0 | |
| Female | n | 126 | 125 | 77 | 90 | 77 | 76 | 126 |
| Mean | 14.8 | 13.0 | 39.5 | 4.6 | 86.1 | 28.3 | 35.1 | |
| Median | 15.0 | 13.1 | 39.4 | 4.6 | 87.3 | 28.5 | 30.0 | |
| Standard Deviation | 1.3 | 1.0 | 2.7 | 0.3 | 5.8 | 2.2 | 26.4 | |
| Minimum | 12.0 | 9.7 | 31.6 | 3.8 | 61.0 | 18.8 | 4.9 | |
| Maximum | 18.0 | 15.7 | 45.7 | 5.5 | 96.0 | 31.8 | 165.0 | |
| Mild ID (%) | Moderate ID (%) | Severe ID (%) | ID Anemia (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | FM | p-Value | M | FM | p-Value | M | FM | p-Value | M | FM | p-Value | |
| Age ≤ 14 years | 51.8 | 60.0 | 0.29 † | 23.5 | 29.1 | 0.4 † | 3.6 | 5.5 | 0.69 ‡ | 3.6 | 5.5 | 0.69 ‡ |
| Age ≥ 15 years | 31.5 | 47.9 | 0.01 † | 12.0 | 26.8 | 0.01 † | 0.5 | 4.2 | 0.06 ‡ | 1.7 | 2.9 | 0.62 ‡ |
| Author | n/Study Population | Participants’ Ages | Sport Types | Definition of ID | Prevalence of ID |
|---|---|---|---|---|---|
| Toivo et al., 2020 [7] | 261 | 14–17 | Various sports (11 types) | sFer < 30 µg/L | 27% |
| Shoemaker et al., 2019 [6] | 69 | 8–16 | School- or club-sponsored sport | sFer < 30 µg/L | 65% |
| Constantini et al., 2000 [35] | 43 | 12–18 | Gymnasts, swimmers, and tennis and table-tennis players | sFer < 20 µg/L | 36% in gymnasts,20% in the rest |
| Dubnov and Constantini, 2004 [36] | 32 | 14–18 | Basketball | sFer < 20 µg/L | 19% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicotra, D.; Arieli, R.; Redlich, N.; Navot-Mintzer, D.; Constantini, N.W. Iron Deficiency and Anemia in Male and Female Adolescent Athletes Who Engage in Ball Games. J. Clin. Med. 2023, 12, 970. https://doi.org/10.3390/jcm12030970
Nicotra D, Arieli R, Redlich N, Navot-Mintzer D, Constantini NW. Iron Deficiency and Anemia in Male and Female Adolescent Athletes Who Engage in Ball Games. Journal of Clinical Medicine. 2023; 12(3):970. https://doi.org/10.3390/jcm12030970
Chicago/Turabian StyleNicotra, Daniela, Rakefet Arieli, Noam Redlich, Dalya Navot-Mintzer, and Naama W. Constantini. 2023. "Iron Deficiency and Anemia in Male and Female Adolescent Athletes Who Engage in Ball Games" Journal of Clinical Medicine 12, no. 3: 970. https://doi.org/10.3390/jcm12030970
APA StyleNicotra, D., Arieli, R., Redlich, N., Navot-Mintzer, D., & Constantini, N. W. (2023). Iron Deficiency and Anemia in Male and Female Adolescent Athletes Who Engage in Ball Games. Journal of Clinical Medicine, 12(3), 970. https://doi.org/10.3390/jcm12030970