
Association of Genetic Polymorphisms and Serum Levels of miR-1-3p with Postoperative Mortality following Abdominal Aortic Aneurysm Repair

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. SNP Selection
2.3. DNA Extraction and Genotyping
2.4. Quantitative Real-Time PCR (qRT-PCR)
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
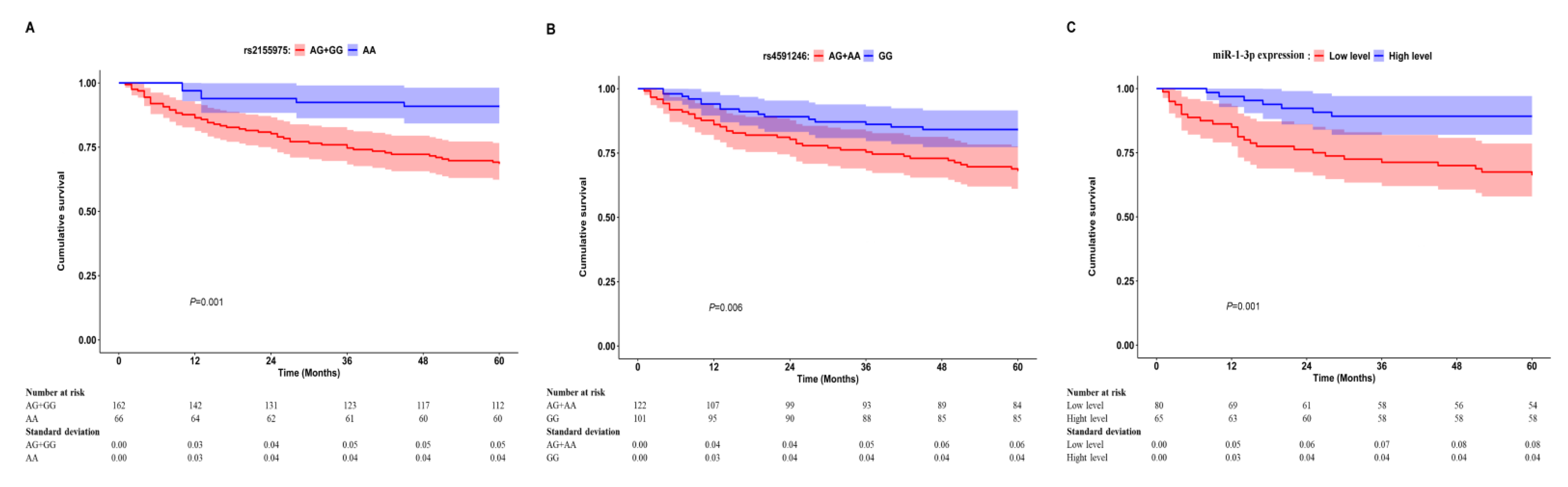
3.2. Association of the Studied SNPs with AAA Prognosis
3.3. Association of Serum miR-1-3p Expression with AAA Prognosis
3.4. Effects of rs2155975 and rs4591246 on the Expression of Serum miR-1-3p
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAA | abdominal aortic aneurysm |
| CHB | Chinese Han population |
| CI | confidence interval |
| EVAR | endovascular aneurysm repair |
| HR | hazard ratio |
| HWE | Hardy–Weinberg equilibrium |
| MAF | minor allele frequency |
| miRNA | microRNA |
| OAR | open aneurysm repair |
| pri-miRNA | primary miRNA |
| ROC | receiver operating characteristic |
| SD | standard deviation |
| SNP | single nucleotide polymorphism |
| VSMC | vascular smooth muscle cell |
References
- Anagnostakos, J.; Lal, B.K. Abdominal aortic aneurysms. Prog. Cardiovasc. Dis. 2021, 65, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Krishna, S.M.; Morton, S.K.; Li, J.; Golledge, J. Risk factors and mouse models of abdominal aortic aneurysm rupture. Int. J. Mol. Sci. 2020, 21, 7250. [Google Scholar] [CrossRef] [PubMed]
- Weaver, L.M.; Loftin, C.D.; Zhan, C.G. Development of pharmacotherapies for abdominal aortic aneurysms. Biomed. Pharmacother. 2022, 153, 113340. [Google Scholar] [CrossRef] [PubMed]
- Jauhiainen, S.; Kiema, M.; Hedman, M.; Laakkonen, J.P. Large vessel cell heterogeneity and plasticity: Focus in aortic aneurysms. Arterioscler. Thromb. Vasc. Biol. 2022, 42, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Isselbacher, E.M.; Preventza, O.; Hamilton Black, J., 3rd; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 acc/aha guideline for the diagnosis and management of aortic disease: A report of the american heart association/american college of cardiology joint committee on clinical practice guidelines. Circulation 2022, 146, e334–e482. [Google Scholar] [CrossRef]
- Golledge, J. Abdominal aortic aneurysm: Update on pathogenesis and medical treatments. Nat. Rev. Cardiol. 2019, 16, 225–242. [Google Scholar] [CrossRef]
- Chang, D.C.; Parina, R.P.; Wilson, S.E. Survival after endovascular vs. open aortic aneurysm repairs. JAMA Surg. 2015, 150, 1160–1166. [Google Scholar] [CrossRef]
- Kainth, A.S.; Sura, T.A.; Williams, M.S.; Wittgen, C.; Zakhary, E.; Smeds, M.R.; Participants, G. Outcomes after endovascular reintervention for aortic interventions. J. Vasc. Surg. 2022, 75, 877–883. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Kuno, T.; Takagi, H. Meta-analysis of phase-specific survival after elective endovascular versus surgical repair of abdominal aortic aneurysm from randomized controlled trials and propensity score-matched studies. J. Vasc. Surg. 2020, 72, 1464–1472. [Google Scholar] [CrossRef]
- Gurung, R.; Choong, A.M.; Woo, C.C.; Foo, R.; Sorokin, V. Genetic and epigenetic mechanisms underlying vascular smooth muscle cell phenotypic modulation in abdominal aortic aneurysm. Int. J. Mol. Sci. 2020, 21, 6334. [Google Scholar] [CrossRef]
- Hemingway, J.F.; French, B.; Caps, M.; Benyakorn, T.; Quiroga, E.; Tran, N.; Singh, N.; Starnes, B.W. Preoperative risk score accuracy confirmed in a modern ruptured abdominal aortic aneurysm experience. J. Vasc. Surg. 2021, 74, 1508–1518. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zou, Y.; Zhao, J.; Schneider, D.B.; Yang, Y.; Ma, Y.; Huang, B.; Yuan, D. The impact of frailty on outcomes of elderly patients after major vascular surgery: A systematic review and meta-analysis. Eur. J. Vasc. Endovasc. Surg. 2018, 56, 591–602. [Google Scholar] [CrossRef] [PubMed]
- Shaker, O.; Ayeldeen, G.; Abdelhamid, A. The impact of single nucleotide polymorphism in the long non-coding meg3 gene on microrna-182 and microrna-29 expression levels in the development of breast cancer in egyptian women. Front. Genet. 2021, 12, 683809. [Google Scholar] [CrossRef] [PubMed]
- Shirvani Samani, O.; Scherr, J.; Kayvanpour, E.; Haas, J.; Lehmann, D.H.; Gi, W.T.; Frese, K.S.; Nietsch, R.; Fehlmann, T.; Sandke, S.; et al. Marathon-induced cardiac strain as model for the evaluation of diagnostic micrornas for acute myocardial infarction. J. Clin. Med. 2021, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Yi, R.; Cullen, B.R. Recognition and cleavage of primary microrna precursors by the nuclear processing enzyme drosha. EMBO J. 2005, 24, 138–148. [Google Scholar] [CrossRef]
- Chen, Y.X.; Chen, J.; Yin, J.Y.; Zhou, H.H.; He, B.M.; Liu, Z.Q. Non-coding rna polymorphisms (rs2910164 and rs1333049) associated with prognosis of lung cancer under platinum-based chemotherapy. Front. Pharmacol. 2021, 12, 709528. [Google Scholar] [CrossRef]
- Radanova, M.; Levkova, M.; Mihaylova, G.; Manev, R.; Maneva, M.; Hadgiev, R.; Conev, N.; Donev, I. Single nucleotide polymorphisms in microrna genes and colorectal cancer risk and prognosis. Biomedicines 2022, 10, 156. [Google Scholar] [CrossRef]
- Ryan, B.M.; Robles, A.I.; Harris, C.C. Genetic variation in microrna networks: The implications for cancer research. Nat. Rev. Cancer 2010, 10, 389–402. [Google Scholar] [CrossRef]
- Qu, J.Y.; Xi, J.; Zhang, Y.H.; Zhang, C.N.; Song, L.; Song, Y.; Hui, R.T.; Chen, J.Z. Association of the microrna-146a snp rs2910164 with ischemic stroke incidence and prognosis in a Chinese population. Int. J. Mol. Sci. 2016, 17, 660. [Google Scholar] [CrossRef]
- Shin, K.M.; Jung, D.K.; Hong, M.J.; Kang, H.J.; Lee, W.K.; Yoo, S.S.; Lee, S.Y.; Cha, S.I.; Lee, J.; Kim, C.H.; et al. The pri-let-7a-2 rs1143770c>t is associated with prognosis of surgically resected non-small cell lung cancer. Gene 2016, 577, 148–152. [Google Scholar] [CrossRef]
- Mullany, L.E.; Herrick, J.S.; Wolff, R.K.; Slattery, M.L. Single nucleotide polymorphisms within micrornas, microrna targets, and microrna biogenesis genes and their impact on colorectal cancer survival. Genes Chromosomes Cancer 2017, 56, 285–295. [Google Scholar] [CrossRef]
- Gao, M.; Yu, T.; Liu, D.; Shi, Y.; Yang, P.; Zhang, J.; Wang, J.; Liu, Y.; Zhang, X. Sepsis plasma-derived exosomal mir-1-3p induces endothelial cell dysfunction by targeting serp1. Clin. Sci. 2021, 135, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Badacz, R.; Kleczynski, P.; Legutko, J.; Zmudka, K.; Gacon, J.; Przewlocki, T.; Kablak-Ziembicka, A. Expression of mir-1-3p, mir-16-5p and mir-122-5p as possible risk factors of secondary cardiovascular events. Biomedicines 2021, 9, 1055. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Chen, X.; Chen, L.; Chen, K.; Zhou, J.; Song, J. Mir-1-3p that correlates with left ventricular function of hcm can serve as a potential target and differentiate hcm from dcm. J. Transl. Med. 2018, 16, 161. [Google Scholar] [CrossRef]
- Jiang, Y.; Yin, H.; Zheng, X.L. Microrna-1 inhibits myocardin-induced contractility of human vascular smooth muscle cells. J. Cell. Physiol. 2010, 225, 506–511. [Google Scholar] [CrossRef]
- Sysol, J.R.; Chen, J.; Singla, S.; Zhao, S.; Comhair, S.; Natarajan, V.; Machado, R.F. Micro-rna-1 is decreased by hypoxia and contributes to the development of pulmonary vascular remodeling via regulation of sphingosine kinase 1. Am. J. Physiol. Lung Cell. Mol. Physiol. 2018, 314, L461–L472. [Google Scholar] [CrossRef]
- Nana, P.; Dakis, K.; Brodis, A.; Spanos, K.; Kouvelos, G. Circulating biomarkers for the prediction of abdominal aortic aneurysm growth. J. Clin. Med. 2021, 10, 1718. [Google Scholar] [CrossRef] [PubMed]
- Tenorio, E.J.R.; Braga, A.F.F.; Tirapelli, D.; Ribeiro, M.S.; Piccinato, C.E.; Joviliano, E.E. Expression in whole blood samples of mirna-191 and mirna-455-3p in patients with aaa and their relationship to clinical outcomes after endovascular repair. Ann. Vasc. Surg. 2018, 50, 209–217. [Google Scholar] [CrossRef]
- Major, M.; Long, G.W.; Eden, C.L.; Studzinski, D.M.; Callahan, R.E.; Brown, O.W. Long-term outcomes and interventions of postoperative type 1a endoleak following elective endovascular aortic aneurysm repair. J. Vasc. Surg. 2022, 75, 136–143. [Google Scholar] [CrossRef]
- Karthikesalingam, A.; Holt, P.J.; Vidal-Diez, A.; Bahia, S.S.; Patterson, B.O.; Hinchliffe, R.J.; Thompson, M.M. The impact of endovascular aneurysm repair on mortality for elective abdominal aortic aneurysm repair in england and the united states. J. Vasc. Surg. 2016, 64, 321–327. [Google Scholar] [CrossRef]
- Duan, R.; Pak, C.; Jin, P. Single nucleotide polymorphism associated with mature mir-125a alters the processing of pri-mirna. Hum. Mol. Genet. 2007, 16, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Kroliczewski, J.; Sobolewska, A.; Lejnowski, D.; Collawn, J.F.; Bartoszewski, R. Microrna single polynucleotide polymorphism influences on microrna biogenesis and mrna target specificity. Gene 2018, 640, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Du, M.; Li, Z.; Zhang, L.; Li, Q.; Xu, Z.; Li, B.; Wang, L.; Li, F.; Zhang, D.; et al. A genetic variant located in mir-146b promoter region is associated with prognosis of gastric cancer. Cancer Epidemiol. Biomark. Prev. 2018, 27, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Navickas, R.; Gal, D.; Laucevicius, A.; Taparauskaite, A.; Zdanyte, M.; Holvoet, P. Identifying circulating micrornas as biomarkers of cardiovascular disease: A systematic review. Cardiovasc. Res. 2016, 111, 322–337. [Google Scholar] [CrossRef]
- Jones, K.G.; Brull, D.J.; Brown, L.C.; Sian, M.; Greenhalgh, R.M.; Humphries, S.E.; Powell, J.T. Interleukin-6 (il-6) and the prognosis of abdominal aortic aneurysms. Circulation 2001, 103, 2260–2265. [Google Scholar] [CrossRef]
- Nejim, B.; Chau, M.; Ramirez Castello, C.; Aziz, F.; Flohr, T.R. Preoperative leukocytosis among female patients predicts poor postoperative outcomes following endovascular aneurysm repair for intact infrarenal abdominal aortic aneurysms. J. Vasc. Surg. 2021, 74, 1843–1852.e3. [Google Scholar] [CrossRef]
- Arnaoutoglou, E.; Kouvelos, G.; Tzimas, P.; Laou, E.; Bouris, V.; Papadopoulos, G.; Matsagkas, M. Relationship between normal preoperative white blood cell count and major adverse events after endovascular repair for abdominal aortic aneurysm: Results of a pilot study. J. Clin. Anesth. 2017, 36, 201–205. [Google Scholar] [CrossRef]
- Heidersbach, A.; Saxby, C.; Carver-Moore, K.; Huang, Y.; Ang, Y.S.; de Jong, P.J.; Ivey, K.N.; Srivastava, D. Microrna-1 regulates sarcomere formation and suppresses smooth muscle gene expression in the mammalian heart. eLife 2013, 2, e01323. [Google Scholar] [CrossRef]
- Sun, T.Y.; Li, Y.Q.; Zhao, F.Q.; Sun, H.M.; Gao, Y.; Wu, B.; Yang, S.; Ji, F.Q.; Zhou, D.S. Mir-1-3p and mir-124-3p synergistically damage the intestinal barrier in the aging colon. J. Crohns. Colitis 2021, 16, 656–666. [Google Scholar] [CrossRef]
- Ginckels, P.; Holvoet, P. Oxidative stress and inflammation in cardiovascular diseases and cancer: Role of non-coding rnas. Yale J. Biol. Med. 2022, 95, 129–152. [Google Scholar]
- Wang, T.; Yang, Y.; Wang, Z.; Zhang, X.; Li, D.; Wei, J. A snp of mir-146a is involved in bladder cancer relapse by affecting the function of bladder cancer stem cells via the mir-146a signallings. J. Cell. Mol. Med. 2020, 24, 8545–8556. [Google Scholar] [CrossRef] [PubMed]
- Du, M.; Lu, D.; Wang, Q.; Chu, H.; Tong, N.; Pan, X.; Qin, C.; Yin, C.; Wang, M.; Zhang, Z. Genetic variations in micrornas and the risk and survival of renal cell cancer. Carcinogenesis 2014, 35, 1629–1635. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Alive Group (n = 173) | Dead Group (n = 57) | p Value |
|---|---|---|---|
| Age, years | 66.36 ± 9.84 | 71.75 ± 9.13 | <0.001 |
| <65 years, n (%) | 68 (39.3%) | 12 (21.1%) | 0.016 |
| ≥65 years, n (%) | 105 (60.7%) | 45 (78.9%) | |
| Male sex, n (%) | 137 (79.2%) | 48 (84.2%) | 0.449 |
| Smoking, n (%) | 64 (37.0%) | 25 (43.9%) | 0.433 |
| Drinking, n (%) | 34 (19.7%) | 8 (14.0%) | 0.431 |
| BMI, kg/m2 | 24.06 ± 3.62 | 23.40 ± 3.51 | 0.239 |
| Comorbidities | |||
| Coronary artery disease, n (%) | 33 (19.1%) | 12 (21.0%) | 0.847 |
| Cerebrovascular disease, n (%) | 18 (10.4%) | 10 (17.5%) | 0.165 |
| Peripheral artery disease, n (%) | 40 (23.1%) | 16 (28.1%) | 0.479 |
| Renal insufficiency, n (%) | 17 (9.8%) | 15 (26.3%) | 0.004 |
| Atrial fibrillation, n (%) | 9 (5.2%) | 4 (7.0%) | 0.741 |
| Hypertension, n (%) | 109 (63.0%) | 42 (73.7%) | 0.151 |
| Diabetes, n (%) | 21 (12.1%) | 12 (21.1%) | 0.122 |
| Dyslipidemia, n (%) | 106 (61.3%) | 33 (57.9%) | 0.864 |
| Maximum AAA diameter, cm | 5.70 ± 1.52 | 6.41 ± 2.13 | 0.010 |
| <5.0 cm, n (%) | 46 (26.6%) | 10 (17.5%) | 0.213 |
| ≥5.0 cm, n (%) | 127 (73.4%) | 47 (82.5%) | |
| Presence of surgical complications, n (%) | 20 (11.6%) | 12 (21.1%) | 0.081 |
| Presence of postoperative renal dysfunction, n (%) | 8 (4.6%) | 6 (10.5%) | 0.117 |
| Presence of postoperative respiratory impairment, n (%) | 13 (7.5%) | 7 (12.3%) | 0.283 |
| Presence of reoperation, n (%) | 20 (11.6%) | 8 (14.0%) | 0.643 |
| Surgical type | |||
| EVAR, n (%) | 137 (79.2%) | 49 (86.0%) | 0.333 |
| OAR, n (%) | 36 (20.8%) | 8 (14.0%) | |
| Cause of death | |||
| Aneurysm-related death, n (%) | / | 11 (19.3%) | / |
| Cardiac death, n (%) | / | 9 (15.8%) | / |
| Others, n (%) | / | 37 (64.9%) | / |
| SNP Genotypes | Alive | Dead | Univariate | Multivariate a | ||
|---|---|---|---|---|---|---|
| p Value | HR (95% CI) | p Value | HR (95% CI) | |||
| rs2155975 | n = 171 | n = 57 | ||||
| AA | 60 | 6 | 1 (Ref) | 1 (Ref) | ||
| AG | 80 | 35 | 0.003 | 3.783 (1.591–8.997) | 0.004 | 3.591 (1.489–8.658) |
| GG | 31 | 16 | 0.002 | 4.376 (1.711–11.191) | 0.010 | 3.590 (1.358–9.487) |
| AG + GG vs. AA | 0.001 | 3.955 (1.697–9.217) | 0.003 | 3.668 (1.560–8.627) | ||
| GG vs. AG + AA | 0.100 | 1.623 (0.911–2.893) | 0.169 | 1.516 (0.838–2.743) | ||
| rs4591246 | n = 168 | n = 55 | ||||
| GG | 85 | 16 | 1 (Ref) | 1 (Ref) | ||
| AG | 70 | 30 | 0.019 | 2.073 (1.130–3.804) | 0.016 | 2.117 (1.150–3.898) |
| AA | 13 | 9 | 0.013 | 2.806 (1.239–6.355) | 0.039 | 2.737 (1.043–5.400) |
| AG + AA vs. GG | 0.007 | 2.213 (1.236–3.960) | 0.007 | 2.225 (1.240–3.992) | ||
| AA vs. AG + GG | 0.089 | 1.859 (0.910–3.800) | 0.107 | 1.811 (0.880–3.726) | ||
| rs9989532 | n = 172 | n = 57 | ||||
| TT | 142 | 47 | 1 (Ref) | 1 (Ref) | ||
| TC | 27 | 9 | 0.938 | 1.029 (0.504–2.099) | 0.615 | 0.825 (0.390–1.745) |
| CC | 3 | 1 | 0.930 | 1.092 (0.151–7.918) | 0.962 | 1.051 (0.141–7.843) |
| TC + CC vs. TT | 0.923 | 1.034 (0.523–2.047) | 0.646 | 0.846 (0.416–1.726) | ||
| CC vs. TC + TT | 0.935 | 1.086 (0.150–7.848) | 0.934 | 1.088 (0.147–8.064) | ||
| Variable | Alive | Dead | Serum miR-1-3p Expression | |||
|---|---|---|---|---|---|---|
| Alive | Dead | p Value | ||||
| Overall | n = 111 | n = 34 | 1.27 ± 0.92 | 0.89 ± 0.60 | 0.011 | |
| Age | <65 years | 41 | 6 | 1.36 ± 1.13 | 0.44 ± 0.21 | 0.008 |
| ≥65 years | 70 | 28 | 1.22 ± 0.79 | 0.98 ± 0.62 | 0.151 | |
| Sex | Male | 88 | 26 | 1.29 ± 0.96 | 0.92 ± 0.65 | 0.065 |
| Female | 23 | 8 | 1.21 ± 0.81 | 0.79 ± 0.42 | 0.168 | |
| AAA size | <5.0 cm | 25 | 6 | 1.43 ± 0.97 | 0.86 ± 0.23 | 0.166 |
| ≥5.0 cm | 86 | 28 | 1.23 ± 0.91 | 0.89 ± 0.66 | 0.075 | |
| Surgical type | EVAR | 90 | 26 | 1.27 ± 0.88 | 0.98 ± 0.65 | 0.120 |
| OAR | 21 | 8 | 1.28 ± 1.11 | 0.58 ± 0.28 | 0.093 | |
| Cause of death | Aneurysm-related death | 111 | 9 | 1.27 ± 0.92 | 0.57 ± 0.44 | 0.026 |
| Cardiac death | 111 | 6 | 1.27 ± 0.92 | 0.54 ± 0.14 | 0.008 | |
| Others | 111 | 19 | 1.27 ± 0.92 | 1.15 ± 0.64 | 0.566 | |
| Variable | Univariate | Multivariate a | ||
|---|---|---|---|---|
| p Value | HR (95% CI) | p Value | HR (95% CI) | |
| miR-1-3p expression per unit increase | 0.024 | 0.507 (0.281–0.914) | 0.030 | 0.496 (0.264–0.933) |
| miR-1-3p expression | ||||
| High levels | 1 (Ref) | 1 (Ref) | ||
| Low levels | 0.002 | 3.624 (1.577–8.324) | 0.004 | 3.498 (1.478–8.276) |
| Variable | rs2155975 | p Value | rs4591246 | p Value | ||
|---|---|---|---|---|---|---|
| AA | AG + GG | GG | AG + AA | |||
| miR-1-3p expression | 1.17 ± 0.67 | 1.19 ± 0.95 | 0.905 | 1.18 ± 0.81 | 1.18 ± 0.93 | 0.969 |
| High levels, n (%) | 26 (59.1%) | 39 (38.6%) | 0.029 | 36 (55.4%) | 29 (36.3%) | 0.029 |
| Low levels, n (%) | 18 (40.9%) | 62 (61.4%) | 29 (44.6%) | 51 (63.8%) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, T.; Jiang, B.; Wu, Y.; Yang, J.; Ma, C.; Yuan, Y. Association of Genetic Polymorphisms and Serum Levels of miR-1-3p with Postoperative Mortality following Abdominal Aortic Aneurysm Repair. J. Clin. Med. 2023, 12, 946. https://doi.org/10.3390/jcm12030946
Li T, Jiang B, Wu Y, Yang J, Ma C, Yuan Y. Association of Genetic Polymorphisms and Serum Levels of miR-1-3p with Postoperative Mortality following Abdominal Aortic Aneurysm Repair. Journal of Clinical Medicine. 2023; 12(3):946. https://doi.org/10.3390/jcm12030946
Chicago/Turabian StyleLi, Tan, Bo Jiang, Yijun Wu, Jun Yang, Chunyan Ma, and Yuan Yuan. 2023. "Association of Genetic Polymorphisms and Serum Levels of miR-1-3p with Postoperative Mortality following Abdominal Aortic Aneurysm Repair" Journal of Clinical Medicine 12, no. 3: 946. https://doi.org/10.3390/jcm12030946
APA StyleLi, T., Jiang, B., Wu, Y., Yang, J., Ma, C., & Yuan, Y. (2023). Association of Genetic Polymorphisms and Serum Levels of miR-1-3p with Postoperative Mortality following Abdominal Aortic Aneurysm Repair. Journal of Clinical Medicine, 12(3), 946. https://doi.org/10.3390/jcm12030946