


Association between Type 1 Diabetes Mellitus and Periodontal Diseases

 ,
,  , ,
, ,
Abstract
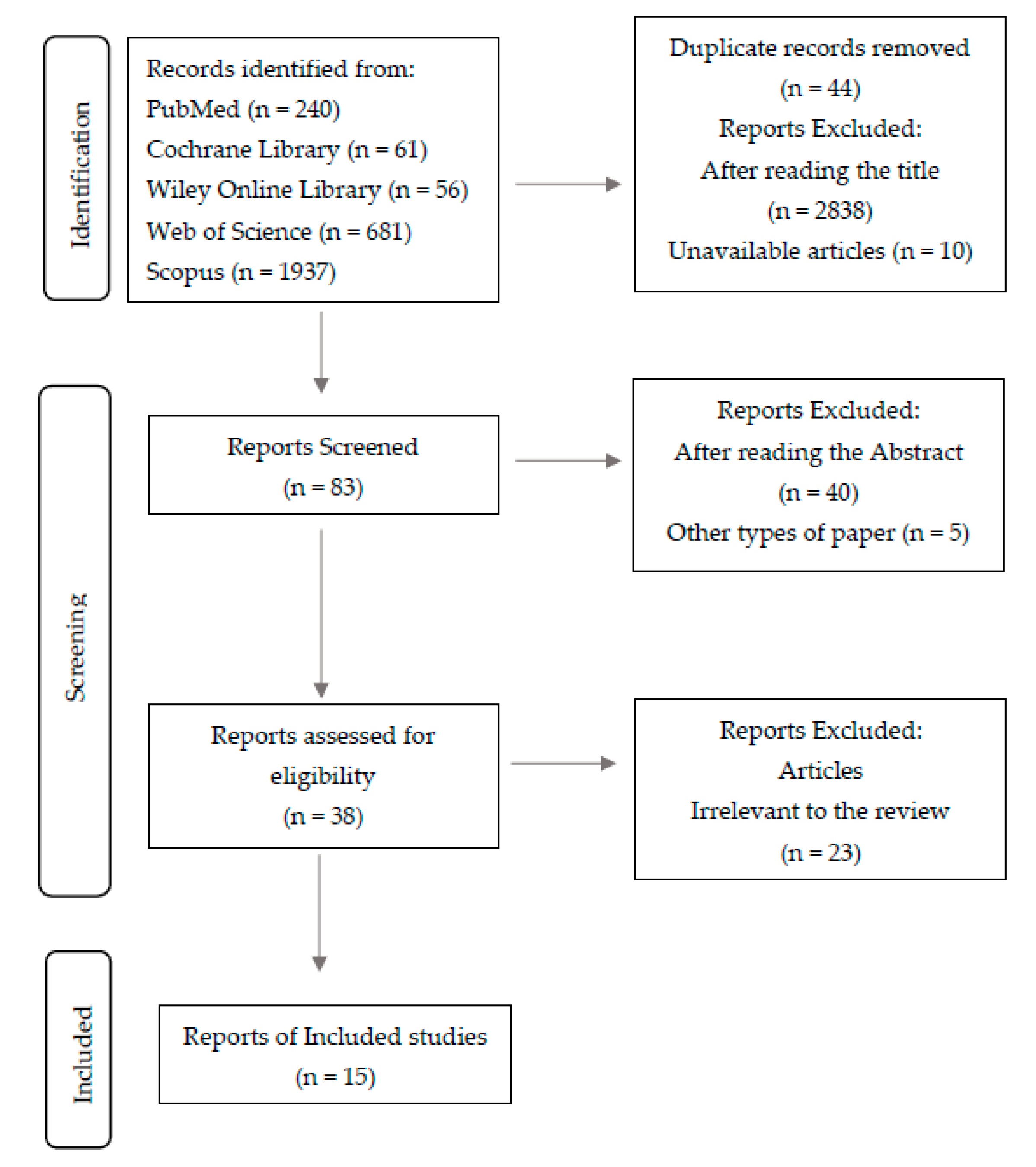
:1. Introduction
2. Materials and Methods
- − P (population): Type 1 Diabetic patients;
- − I (intervention/exposure): Periodontal disease;
- − C (comparison): Patients without periodontal disease;
- − O (outcome): to analyze the association between type 1 diabetes mellitus and periodontal disease.
2.1. Extraction of Sample Data
2.2. Study Quality and Risk of Bias
3. Results
3.1. Characterization of the Sample for the Quality of the Study

{kind=link}
| Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies. | 1. Were the Criteria for Inclusion in the Sample Clearly Defined? | 2. Were the Study Subjects and the Setting Described in Detail? | 3. Was the Exposure Measured in a Valid and Reliable Way? | 4. Were Objective, Standard Criteria Used for Measurement of the Condition? | 5. Were Confounding Factors Identified? | 6. Were Strategies to Deal with Confounding Factors Stated? | 7. Were the Outcomes Measured in a Valid and Reliable Way? | 8. Was Appropriate Statistical Analysis Used? |
|---|---|---|---|---|---|---|---|---|
| Antonoglou et al. [18], 2013 | Y | Y | Y | Y | N | UN | Y | Y |
| Dakovic et al. [9], 2013 | Y | Y | Y | Y | N | UN | Y | Y |
| Poplawska-Kita et al. [7], 2014 | Y | Y | Y | Y | Y | UN | Y | Y |
| Jindal et al. [29], 2015 | Y | Y | Y | Y | N | UN | Y | Y |
| Lappin et al. [23], 2015 | Y | Y | Y | Y | Y | Y | Y | Y |
| Ismail et al. [24], 2017 | N | Y | Y | Y | Y | Y | Y | Y |
| Roy et al. [25], 2019 | Y | Y | Y | Y | Y | Y | Y | UN |
| Dicembrini et al. [11], 2021 | Y | Y | Y | Y | Y | Y | Y | Y |
| Jensen et al. [26], 2021 | Y | Y | Y | Y | Y | UN | Y | Y |
| Joanna Briggs Institute Critical Appraisal Checklist for Case Control Studies. | 1. Were the Groups Comparable other than the Presence of Disease in Cases or the Absence of Disease in Controls? | 2. Were Cases and Controls Matched Appropriately? | 3. Were the Same Criteria Used for Identification of Cases and Controls? | 4. Was Exposure Measured in a Standard, Valid, and Reliable Way? | 5. Was Exposure Measured in the Same Way for Cases and Controls? | 6. Were Confounding Factors Identified? | 7. Were Strategies to Deal with Confounding Factors Stated? | 8. Were Outcomes Assessed in a Standard, Valid, and Reliable Way for Cases and Controls? | 9. Was the Exposure Period of Interest Long Enough to be Meaningful? | 10. Was Appropriate Statistical Analysis Used? |
|---|---|---|---|---|---|---|---|---|---|---|
| Zizzi et al. [27], 2013 | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Linhartova et al. [28], 2018 | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Keles et al. [30], 2020 | Y | Y | Y | Y | Y | UN | UN | Y | Y | Y |
| Sereti et al. [3], 2021 | Y | Y | Y | Y | Y | UN | UN | Y | Y | Y |
| Joanna Briggs Institute Critical Appraisal Checklist for Randomized Controlled Trials. | 1. Was True Randomization Used for Assignment of Participants to Treatment Groups? | 2. Was Allocation to Treatment Groups Concealed? | 3. Were Treatment Groups Similar at the Baseline? | 4. Were Participants Blind to Treatment Assignment? | 5. Were Those Delivering Treatment Blind to Treatment Assignment? | 6. Were Outcomes Assessors Blind to Treatment Assignment? | 7. Were Treatment Groups Treated Identically Other than the Intervention of Interest? | 8. Was Follow up Complete and If Not, Were Differences between Groups in Terms of Their Follow up Adequately Described and Analyzed? | 9. Were Participants Analyzed in the Groups to Which They Were Randomized? | 10. Were Outcomes Measured in the Same Way for Treatment Groups? | 11. Were Outcomes Measured in a Reliable Way? | 12. Was Appropriate Statistical Analysis Used? | 13. Was the Trial Design Appropriate, and any Deviations from the Standard RCT Design (Individual Randomization, Parallel Groups) Accounted for in the Conduct and Analysis of the Trial? |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ajita et al. [8], 2013 | N | Y | NA | N | NA | N | NA | N | N | NA | N | NA | NA |
| Joanna Briggs Institute Critical Appraisal Checklist for Cohort Studies. | 1. Were the Two Groups Similar and Recruited from the Same Population? | 2. Were the Exposures Measured Similarly to Assign People to both Exposed and Unexposed Groups? | 3. Was the Exposure Measured in a Valid and Reliable Way? | 4. Were Confounding Factors Identified? | 5. Were Strategies to Deal with Confounding Factors Stated? | 6. Were the Groups/Participants Free of the Outcome at the Start of the Study (or at the Moment of Exposure)? | 7. Were the Outcomes Measured in a Valid and Reliable Way? | 8. Was the Follow up Time Reported and Sufficient to Be Long Enough for Outcomes to Occur? | 9. Was Follow up Complete, and If Not, Were the Reasons to Loss to Follow up Described and Explored? | 10. Were Strategies to Address Incomplete Follow up Utilized? | 11. Was Appropriate Statistical Analysis Used? |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sun et al. [20], 2019 | Y | Y | Y | Y | Y | Y | Y | Y | NA | NA | Y |
3.2. Characteristics of the Included Studies
4. Discussion
4.1. Glycemic Control
4.2. Advanced Glycated-End Products
4.3. Pro-Inflammatory Mediators
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Y.-Y.; Xiao, E.; Graves, D.T. Diabetes mellitus related bone metabolism and periodontal disease. Int. J. Oral Sci. 2015, 72, 63–72. [Google Scholar] [CrossRef]
- Reddy, M.; Gopalkrishna, P. Type 1 diabetes and periodontal disease: A literature review. Can. J. Dent. Hyg. 2022, 56, 22–30. [Google Scholar]
- Sereti, M.; Roy, M.; Zekeridou, A.; Gastaldi, G.; Giannopoulou, C. Gingival crevicular fluid biomarkers in type 1 diabetes mellitus: A case–control study. Clin. Exp. Dent. Res. 2021, 7, 170–178. [Google Scholar] [CrossRef]
- Graves, D.T.; Ding, Z.; Yang, Y. The impact of diabetes on periodontal diseases. Periodontology 2000 2020, 82, 214–224. [Google Scholar] [CrossRef]
- Mahalakshmi, K.; Arangannal, P.; Santoshkumari. Frequency of putative periodontal pathogens among type 1 diabetes mellitus: A case-control study. BMC Res. Notes 2019, 12, 328. [Google Scholar] [CrossRef]
- Daković, D.; Mileusnić, I.; Hajduković, Z.; Čakić, S.; Hadži-Mihajlović, M. Gingivitis and Periodontitis in children and adolescents suffering from type 1 diabetes mellitus. Vojnosanit. Pregl. 2015, 72, 265–273. [Google Scholar] [CrossRef]
- Popławska-Kita, A.; Siewko, K.; Szpak, P.; Król, B.; Telejko, B.; Klimiuk, P.A.; Stokowska, W.; Górska, M.; Szelachowska, M. Association between type 1 diabetes and periodontal health. Adv. Med. Sci. 2014, 59, 126–131. [Google Scholar] [CrossRef]
- Ajita, M.; Karan, P.; Vivek, G.; Anand, M.S.; Anuj, M. Periodontal disease and type 1 diabetes mellitus: Associations with glycemic control and complications: An Indian perspective. Diabetes Metab. Syndr. 2013, 7, 61–63. [Google Scholar] [CrossRef]
- Dakovic, D.; Colic, M.; Cakic, S.; Mileusnic, I.; Hajdukovic, Z.; Stamatovic, N. Salivary interleukin-8 levels in children suffering from Type 1 diabetes mellitus. J. Clin. Pediatr. Dent. 2013, 37, 377–380. [Google Scholar] [CrossRef]
- Adda, G.; Aimetti, M.; Citterio, F.; Consoli, A.; Di Bartolo, P.; Landi, L.; Lione, L.; Luzi, L. Consensus report of the joint workshop of the Italian Society of Diabetology, Italian Society of Periodontology and Implantology, Italian Association of Clinical Diabetologists (SID-SIdP-AMD). Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2515–2525. [Google Scholar] [CrossRef]
- Dicembrini, I.; Barbato, L.; Serni, L.; Caliri, M.; Pala, L.; Cairo, F.; Mannucci, E. Glucose variability and periodontal disease in type 1 diabetes: A cross-sectional study—The “PAROdontopatia e DIAbete” (PARODIA) project. Acta Diabetol. 2021, 58, 1367–1371. [Google Scholar] [CrossRef]
- Chee, B.; Park, B.; Bartold, P.M. Periodontitis and type II diabetes: A two-way relationship. Int. J. Evid. Based Healthc. 2013, 11, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Duque, C.; João, M.F.D.; Camargo, G.A.D.C.G.; Teixeira, G.S.; Machado, T.S.; Azevedo, R.D.S.; Mariano, F.S.; Colombo, N.H.; Vizoto, N.L.; Mattos-Graner, R.D.O. Microbiological, lipid and immunological profiles in children with gingivitis and type 1 diabetes mellitus. J. Appl. Oral Sci. 2017, 25, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Bui, F.Q.; Almeida-da-Silva, C.L.C.; Huynh, B.; Trinh, A.; Liu, J.; Woodward, J.; Asadi, H.; Ojcius, D.M. Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Duda-Sobczak, A.; Zozulinska-Ziolkiewicz, D.; Wyganowska-Swiatkowska, M. Type 1 Diabetes and Periodontal Health. Clin. Ther. 2018, 40, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Sima, C.; Glogauer, M. Diabetes mellitus and periodontal diseases. Curr. Diabetes Rep. 2013, 13, 445–452. [Google Scholar] [CrossRef]
- Şurlin, P.; Oprea, B.; Solomon, S.M.; Popa, S.G.; Moţa, M.A.R.I.A.; Mateescu, G.O.; Rauten, A.M.; Popescu, D.M.; Dragomir, L.P.; Puiu, I.; et al. Matrix metalloproteinase-7,-8,-9 and-13 in gingival tissue of patients with type 1 diabetes and periodontitis. Rom. J. Morphol. Embryol. 2014, 55, 1137–1141. [Google Scholar]
- Antonoglou, G.; Knuuttila, M.; Nieminen, P.; Vainio, O.; Hiltunen, L.; Raunio, T.; Niemelä, O.; Hedberg, P.; Karttunen, R.; Tervonen, T. Serum osteoprotegerin and periodontal destruction in subjects with type 1 diabetes mellitus. J. Clin. Periodontol. 2013, 40, 765–770. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef]
- Sun, K.T.; Chen, S.C.; Lin, C.L.; Hsu, J.T.; Chen, I.A.; Wu, I.T.; Palanisamy, K.; Shen, T.C.; Li, C.Y. The association between Type 1 diabetes mellitus and periodontal diseases. J. Formos. Med. Assoc. 2019, 118, 1047–1054. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Porritt, K.; Gomersall, J.; Lockwood, C. JBI’s Systematic Reviews: Study selection and critical appraisal. Am. J. Nurs. 2014, 114, 47–52. [Google Scholar] [CrossRef]
- Lappin, D.F.; Robertson, D.; Hodge, P.; Treagus, D.; Awang, R.A.; Ramage, G.; Nile, C.J. Evaluation of Serum Glycated Haemoglobin, IL-6, IL-8 and CXCL5 in TIDM with and without Periodontitis and Effects of Advanced Glycation End Products and Porphyromonas Gingivalis Lipopolysaccharide on IL-6, IL-8 and CXCL5 Expression by Oral Epithelial Cell. J. Periodontol. 2015, 86, 1249–1259. [Google Scholar] [CrossRef]
- Ismail, A.F.; McGrath, C.P.; Yiu, C.K.Y. Oral health status of children with type 1 diabetes: A comparative study. J. Pediatr. Endocrinol. Metab. 2017, 30, 1155–1159. [Google Scholar] [CrossRef]
- Roy, M.; Gastaldi, G.; Courvoisier, D.S.; Mombelli, A.; Giannopoulou, C. Periodontal health in a cohort of subjects with type 1 diabetes mellitus. Clin. Exp. Dent. Res. 2019, 5, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Jensen, E.D.; Selway, C.A.; Allen, G.; Bednarz, J.; Weyrich, L.S.; Gue, S.; Peña, A.S.; Couper, J. Early markers of periodontal disease and altered oral microbiota are associated with glycemic control in children with type 1 diabetes. Pediatr. Diabetes 2021, 22, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Zizzi, A.; Tirabassi, G.; Aspriello, S.D.; Piemontese, M.; Rubini, C.; Lucarini, G. Gingival advanced glycation end-products in diabetes mellitus-associated chronic periodontitis: An immunohistochemical study. J. Periodontal. Res. 2013, 48, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Borilova Linhartova, P.; Kavrikova, D.; Tomandlova, M.; Poskerova, H.; Rehka, V.; Dušek, L.; Izakovicova Holla, L. Differences in interleukin-8 plasma levels between diabetic patients and healthy individuals independently on their periodontal status. Int. J. Mol. Sci. 2018, 19, 3214. [Google Scholar] [CrossRef]
- Jindal, A.; Parihar, A.S.; Sood, M.; Singh, P.; Singh, N. Relationship between severity of periodontal disease and control of diabetes (glycated hemoglobin) in patients with type 1 diabetes mellitus. J. Int. Oral Health 2015, 7, 17–20. [Google Scholar]
- Keles, S.; Anik, A.; Cevik, O.; Abas, B.I.; Anik, A. Gingival crevicular fluid levels of interleukin-18 and tumor necrosis factor-alpha in type 1 diabetic children with gingivitis. Clin. Oral Investig. 2020, 24, 3623–3631. [Google Scholar] [CrossRef]
- Chakraborty, P.; Mukhopadhyay, P.; Bhattacharjee, K.; Chakraborty, A.; Chowdhury, S.; Ghosh, S. Periodontal disease in type 1 diabetes mellitus: Influence of pubertal stage and glycemic control. Endocr. Pract. 2021, 27, 765–768. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis:Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Bascones-Martínez, A.; Muñoz-Corcuera, M.; Bascones-Ilundain, J. Diabetes y periodontitis: Una relación bidireccional [Diabetes and periodontitis: A bidirectional relationship]. Med. Clin. 2015, 145, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Babatzia, A.; Papaioannou, W.; Stavropoulou, A.; Pandis, N.; Kanaka-Gantenbein, C.; Papagiannoulis, L.; Gizani, S. Clinical and microbial oral health status in children and adolescents with type 1 diabetes mellitus. Int. Dent. J. 2020, 70, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Ceriello, A.; Buysschaert, M.; Chapple, I.; Demmer, R.T.; Graziani, F.; Herrera, D.; Jepsen, S.; Lione, L.; Madianos, P.; et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International diabetes Federation and the European Federation of Periodontology. Diabetes Res. Clin. Pract. 2018, 137, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Mishra, L.; Mohanty, R.; Nayak, R. Diabetes and gum disease: The diabolic duo. Diabetes Metab. Syndr. Clin. Res. Rev. 2014, 8, 255–258. [Google Scholar] [CrossRef]

| Authors | Study Design | Study Aim | Inclusion Criteria | Exclusion Criteria | Sample Size | Age Group | Study Duration | Outcome Measures | Results |
|---|---|---|---|---|---|---|---|---|---|
| Antonoglou et al. [18], 2013 | Cross-sectional study | To explore the associations between the extent of periodontal destruction and circulating levels of RANKL and OPG. | Subjects from a primary health care diabetes unit in the City of Oulu, Finland and others from the Clinic of Internal Medicine, Oulu University Hospital, Oulu, Finland. - Subjects examined clinically by a periodontal specialist at the Specialist Dental Health Care Unit, Oulu (Finland). | Subjects needing prophylactic antibiotic medication in association with periodontal probing; subjects who used immunosuppressive medication or had had antibiotics during the past 4 months. | 80 DM1 patients (46 Female; 34 Male) No or mild periodontitis (n = 40) Moderate periodontitis (n = 28) Severe periodontitis (n = 12) | 18–74 years (38 ± 12.3) | NR | - AL (Attachment Loss) - OPG - RANKL - Duration of DM | Subject characteristics presented as mean values/subject (±SD) in different periodontal disease categories: Patients with no or mild periodontitis: - Total of 16 sites (16.4 ± 14.5) presented with bleeding and PPD ≥ 4 mm - 0.7 sites (0.7 ± 1.0) with AL ≥ 4 mm. - OPG: 96.0 pg/mL - The sRANKL: 18.1 pg/mL - The sRANKL/OPG ratio: 0.2 ± 0.1 Patients with severe periodontitis: - Total of 16 sites (39.6 ± 21.9) - sites with attachment loss (AL) ≥ 4 mm (38.8 ± 18.5) - OPG was 135 pg/mL - The RANKL—33.2 pg/mL - The RANKL/OPG ratio: 0.1 ± 0.1 The results showed a positive association between AL ≥ 4 mm and severity of periodontitis and the level of serum OPG. - The results did not find any association between serum sRANKL level or sRANKL/OPG ratio and periodontal variables. - This study showed a strong correlation between the age of the subjects and the duration of DM (r = 0.530, p ≤ 0.001). |
| Ajita et al. [8], 2013 | Randomized, controlled clinical study | To determine the relationship between DM1 an PD and to analyse how diabetes metabolic control, complications and duration are related with periodontal parameters. | Subjects aged between 18 and 50 years; DM1 patients diagnosed for more than 3 years; Subjects without any active infection; Individuals with >14 natural teeth present and at least 5 teeth with PPD ≥ 5 mm and CAL ≥ 3 mm and who had not had any periodontal treatment in the last 6 months. | If they had non-type 1 DM; Pregnancy and lactation; Subjects with any inflammatory disease, chronic liver disease, or patients taking antibiotics, immunosuppressants, and antiepileptics. | DM1 patients (n = 20 [14 Males/6 Females]) Non-DM1 (n = 20 [14 Males/6 Females]) | 18–50 years | NR | - PPD - CAL - BI - Duration of DM | - BI: significantly higher in DM1 patients (2.708 ± 0.390) (mean ± SD) when compared to non-diabetic (1.760 ± 0.434). Relationship between periodontal parameters in PMC patients vs. GMC patients: (mean ± SD) PPD (6.429 ± 0.723) vs. (5.814 ± 0.693) BI (2.646 ± 0.402) vs. (1.129 ± 0.362) CAL (4.356 ± 0.688) vs. (2.214 ± 0.679) significant differences were recorded in PPD (p < 0.001), BI (p < 0.001), and CAL (p = 0.001) between those groups. - DM1 patients vs. non-diabetic patients: (mean ± SD) CAL (4.337 ± 0.648) vs. (2.300 ± 0.557) (p = 0.001) BI (2.708 ± 0.390) vs. (1.760 ± 0.434) (p < 0.001) PPD (6.337 ± 0.650) vs. (5.181 ± 0.705) (p < 0.001) - The results showed a correlation between the bleeding index and disease severity in patients diagnosed with diabetes in a short period of time (4–7 years) (1.760 ± 0.434). |
| Dakovic et al. [9], 2013 | Cross-sectional study | To investigate the differences between the salivary levels of IL-8 in patients with DM1 with or without concomitant periodontitis and healthy patients. | - Patients attending the Outpatient Diabetes Clinic at the Mother and Child Healthcare Institute of Serbia, over 5 month period. - DM1 patients treated only with multiple daily insulin injections. - Healthy patients aged 7–18 attending the Clinic of Dental Medicine, Military Medical Academy (Belgrade) for a dental check-up. | Children that were undergoing active orthodontic therapy, had other systemic disease, or had received systemic antibiotic therapy in 6 months prior to the study. | Children DM1 (n = 20 [9 Males/11 Females]): - with periodontitis (n = 10) - without periodontitis (n = 10) Healthy children and adolescents N = 20 [8 Males/12 Females]) | 7–18 years | NR | - PPD - BOP - CAL - Salivary IL-8 level | Periodontal measurements in DM1 children vs. healthy children (Group control): (mean ± SD) CAL (0.89 ± 0.57) vs. (0.89 ± 0.24) (p = 0.95) PPD (1.69 ± 0.41) vs. (1.45 ± 0.32) (p = 0.05) BOP (0.65 ± 0.33) vs. (0.26 ± 0.28) (p = 0.0001) - PPD and BOP were substantially higher in DM1 group compared to the healthy patients group. - Periodontal measurements in DM1 children with periodontitis vs. DM1 children without periodontitis (mean ± SD) - CAL (1.31 ± 0.49) vs. (0.47 ± 0.22) (p = 0.0001); - PPD (2.05 ± 0.18) vs. (1.33 ± 0.19) (p = 0.0001); - BOP (0.88 ± 0.33) vs. (0.43 ± 0.56) (p = 0.0004) There was a statistically significant difference for PPD, CAL, and BOP between DM1 subjects with periodontitis and DM1 without periodontitis. - DM1 patients exhibited a significantly higher level of salivary IL-8 when compared to the control group (p < 0.005). No differences in the level of salivary IL-8 between DM1 patients with periodontitis and DM1 patients without periodontitis. Correlations between clinical parameters and salivary IL-8 levels in DM1 children PPD (r = 0.07, p = 0.78); CAL (r = 0.04, p = 0.85), BOP (r = −0.19, p = 0.43) A correlation between the levels of salivary IL-8 and clinical parameters was not found. |
| Zizzi et al. [27], 2013 | Case-Control Study | To evaluate the expression of AGEs in DM-associated periodontitis. | Age > 35 years; the presence of at least 20 teeth; - For periodontitis subjects a diagnosis of generalized, severe, chronic periodontitis made on the basis of the presence of more than 30% of measured sites with >5 mm of CAL; - For DM patients, the diagnosis of the type of DM is made at least 12 months before the study; - For nondiabetic subjects, HbA1c in the nondiabetic range (<6.1%) and plasma glycemia lower than 100 mg/dL; - For healthy subjects, PD < 3 mm, GI = 0 without clinical inflammation and CAL < 2 mm. | Presence of any important disease other than DM in the groups of diabetic subjects; Being smoker; having taken antibiotics, corticosteroids, or nonsteroidal anti-inflammatory drugs within the 6 months before treatment; having undergone periodontal treatment within the previous 2 years. | Healthy subjects (CT, n = 16 [12 Male/4 female]); Subjects DM1 suffering from generalized, severe CP (PD-DM1, n = 16 [11 Male/5 Female]) Systematically healthy individuals affected by periodontitis (PD-S, n = 16 [9 Males/7 females]. | CT: 55 ± 1.76 * p < 0.05 PD-S 56.5 ± 1.32 * p < 0.05 PD-DM1 46.1 ± 0.70 * p < 0.05 vs. PD-DM1 | 2005–2011 | - PPD - CAL - BL - AGEs | Periodontal parameters of CT vs. PD-S vs. PD-DM1 subjects: (median [interquartile range, IQR] GI: ((0) [0–0]) vs. (1.6 [1.4–2.3]) and (1.9 [1.4–2.6]) PPD (2.6 [2.2–2.8]) vs. (7.1 [7–7.3]) and (6.9 [6.9–7.1], CAL (1.1 [0.8–1.3]) vs. (6.6 [6.4–6.7]) and (6.6 [6.2–6.7] BL (5 [4–6.7]), vs. (60.5 [58.2–62]) and (59 [58.2–62.7]) There were statistically significant differences between healthy subjects (CT) in comparison to the group of systematically healthy individuals affected by periodontitis (PD-S) and DM1 subjects affected by periodontitis (PD-DM1) (p < 0.05) - PD-DM1: epithelium AGE % (90 [75–93.7]); [IQR] vessels AGE % (74 ± 2.38) (mean ± SD) - CT: Epithelium AGE% (62.5 [46.2–73.7]) (p < 0.05) Vessels AGE % (51.8 ± 2.88) (p < 0.05) - PD-S: Epithelium AGE% (70 [61.2–70]) (p < 0.05) Vessels AGE% (58.7 ± 4.19) (p < 0.05) On the gingival tissue from PD-DM1, there was found a significant increase in the number of AGE-positive cells in the epithelium and in vessels when compared to the CT and PD-S group. - AGE-positivity cells were not fund in fibroblast and in inflammatory infiltrates in subjects of the CT and PD-S group. - A positive correlation was found in PD-DM1 subjects between the duration of DM and the percentage of AGE-positive cells in epithelium (r: 0.610; p: 0.012), vessels (0.635; p: 0.008), and fibroblasts (r = 0.589; p: 0.016). |
| Popławska-Kita et al. [7], 2014 | Cross-sectional study | The role of hyperglycemia in the development of periodontal disease. | NR | Presence of systemic diseases other than DM1; subjects taking immunosuppressive drugs, steroids, or non-steroidal anti-inflammatory drugs, pregnancy and fixed orthodontic appliances. | - 40 Subjects Group Control (GC) According to the metabolic control: - 107 DM1 subjects DM1+HbA1c ≤ 6.5% (n = 22 [4 Males/14 Females]) DM1+HbA1c ≥ 6.5%; (n = 85 [50 Males/35 Females]) According to the presence of periodontitis: DM1+No-periodonti tis (n = 45) DM1+Periodontitis (n = 62) GC+No-periodontitis (n = 3 4) GC+periodontitis (n = 6) | According to the metabolic control: DM1 subjects with HbA1c ≤ 6.5%: 34.8 ± 10.9 HbA1c ≥ 6.5%; 37.9 ± 3.7 Control: 32.3 ± 1.0 According to the presence of periodontitis: DM1+periodontitis: 42 ± 12.7 DM1+no-periodontitis: 30.7 ± 11.1 GC+no-periodontitis: 29.4 ± 9.5 GC+periodontitis: 48 ± 2.1 | NR | - HbA1c - CRP - (TNF)-α - Fibrinogen - OHI | Periodontitis was found in: - 15% of the controls - 57.9% of DM1 patients - 59.5% of DM1 with PMC. The incidence of periodontitis is increased in DM1, especially in those with poor metabolic control Biochemical characteristics of the GMC vs. PMC vs. CT (mean ± SD) CRP (ng/mL) (4.8 ± 1.2) vs. (10.9 ± 23.2) vs. (7.1 ± 8.5) TNF-α (pg/mL) (1.0 ± 0.6) vs. (1.25 ± 1.06) vs. (1.5 ± 1.6) GMC had the lowest concentration of CPR among all groups. The clinical characteristics of GMC vs. PMC (mean ± SD) - HbA1c (6.0 ± 0.6) (p < 0.01) vs. (9.8 ± 2.4) - Fasting glucose level (mg/dl) (126 ± 60.9) (p < 0.05), vs. (172.83 ± 72.4) (p < 0.01); PMC group exhibited significantly higher HbA1c and fasting glucose level. DM1 with periodontitis showed: Higher: (mean ± SD) - Fibrinogen (371.3 ± 114.7) (p < 0.01) - TNF-α (1.6 ± 1.2) (p < 0.001) - OHI (2.1 ± 0.7) Lower: - Teeth number (p < 0.001) - CPI 0/fibrinogen (r = −0.272; p < 0.05) - CPI 0/TNF-α (r = - 0.233; p < 0.05) - CPI 3/TNF-α (r = 0.348; p < 0.01) - CPI 3/fasting/glucose (r = 0.217; p < 0.05) The number of sextants without signs of periodontal disease (CPI 0) was correlated negatively with fibrinogen (p < 0.05), whereas the number of sextants with 4–5 mm deep pathologic pockets (CPI3) were correlated positively with TNF-α (p < 0.01) and fasting glucose level (r = 0.217; p < 0.05) |
| Jindal et al. [29], 2015 | Cross-sectional study | To investigate the relationship between severity of periodontal disease and glycemic control in patients with DM1 in a hospital-based study. | Age between 12 and 25 years and with diagnosis of DM1 for more than 3 months duration. | Patients non-DM1, undergoing active orthodontic treatment; patients with any chronic inflammatory disease and on long-term medications that could influence the studied parameters such us antibiotics and antiepileptic or immunosuppressive drugs. | 50 DM1 patients [32 Males/18 females]: - Group A- Good (HbA1c ≤ 7) n = 15 - Group B- Fair (HbA1c = 7–8) n = 16 - Group c- Poor (HbA1c > 8): 19 | Between 12 and 25 | NR | - PPD - CAL - PI - GI | Mean standard derivation of periodontal parameters between: GMC vs. Fair Metabolic control vs. PMC: (mean ± SD) - PPD (2.93 ± 0.59) vs. (3.81 ± 0.75) vs. (5.31 ± 0.20) - CAL (3.33 ± 0.48) vs. (4.43 ± 0.62) vs. (6.15 ± 1.38) - PI (1.25 ± 0.20) vs. (1.82 ± 0.45) vs. (2.39 ± 0.18) - GI (1.25 ± 0.34) vs. (1.43 ± 0.33) vs. (2.01 ± 0.29) (p < 0.05) DM1 with poor metabolic control exhibited increased GI, PI, PPD, and CAL when compared to other groups. |
| Lappin et al. [23], 2015 | Cross-sectional study | To compare circulating levels of IL-6, IL-8 and CXCL5 in patients DM1, with or without periodontitis to control groups of systemically healthy, non-smoking, individuals with and without periodontitis. To determine the effect of AGE, in the presence and absence of Pg LPS, on IL-6, IL-8 and CXCL5 expression by THP-1 monocytes and OKF6/TERT-2 cells. | Diabetic subjects were diagnosed by trained clinicians and had been attending the outpatient clinic for monitoring of glycated hemoglobin for more than 2 years. In the periodontitis group, the participants had to have a minimum of two sites with probing depth and attachment loss ≥ 5 mm. None of the subjects were receiving periodontal treatment at the time of diagnosis. | No history of smoking within the past 5 years; pregnancy at the time of the recruitment; taking immunosuppressive drugs antibiotics or anti-inflammatory drugs within 6 weeks of recruitment; individual with less than 20 teeth and subjects who were unable to consent. | 104 Subjects: Healthy volunteers (H n = 19 [63%Males/37%females]. Patients with periodontitis (PD n = 23 [46%Males/54% females]. DM1 patients (DM1n = 28 [36% Males/64% females]. DM1 patients with periodontitis (DM1+p n = 34 [45%Males/55%females]. | H: 33 ± 8 PD: 40 ± 11 DM1: 35 ± 10 DM1+P: 36 ± 9 | NR | - PPD - AL - BOP - Plasma IL-8 levels - Plasma IL-6 levels | - HbA1c: (mean ± SD) DM1+P (73.8 ± 17.0) DM1 (71.6 ± 16.3) H (32.2 ± 1.1) PD (33.3 ± 1.1) - Diabetic patients with or without periodontitis showed higher levels of glycated hemoglobin when compared to the healthy group or even with the group of periodontitis subjects. - Not significant difference between the diabetic and non-diabetic groups: The mean of sites with PPD of ≥5 mm, the number of teeth with PPD ≥ 5 mm, number of sites with AL ≥ 5 mm, teeth with AL ≥ 5 mm and the proportion of sites with BOP. - Plasma IL-6 levels did not o differ between the four groups; - Plasma levels of IL-8 were higher in periodontitis group, when compared to the healthy group (p < 0.001). - DM1 group and DM1+p group exhibited higher levels of IL-8 than healthy volunteers (p < 0.001, for both); - Patients with DM1+p showed higher levels of IL-8 when compared to patients with periodontitis (p < 0.05). |
| Ismail et al. [24], 2017 | Cross-sectional study | To compare the caries experience and periodontal health status between children with DM1 and healthy age- and sex-matched controls. | DM1 patients, who are members of the Honk Kong Juvenile Diabetes Association; People that sign the consent form; | Patients who did not have any systemic disease or problems with manual dexterity; were not undergoing active orthodontic treatment, and had not received any dental treatment for the past 1 year. | 64 Children: - DM1 (n = 32 [16 Males/ 16 Females]) - Control group (n = 32 [16 Males/ 16 Females]) | (12 ± 4 years) | NR | - Plaque - GI - Gingivitis - PI - BI - CI - HbA1c | Periodontal health status between DM1 vs. Non-DM1: Mean (SD) Plaque: 0.66 (0.46) vs. 0.43 (0.16) (p = 0.01) PI: 0.76 (0.40) vs. 0.46 (0.14) (p < 0.01) BI: 0.20 (0.18) vs. 0.16(0.11) (p > 0.05) CI: 0.14(0.15) vs. 0.13(0.15) (p > 0.05) Gingivitis: 0.50(0.35) vs. 0.51(0.22) (p > 0.05) The Children with DM1 exhibited significantly greater plaque deposits (p = 0.01), a higher mean plaque index (p < 0.01), also had a greater percentage of sites with bleeding on probing (p > 0.05), when compared to non-diabetics. The percentage of sites with calculus deposits and gingivitis was similar in both groups (p > 0.05) |
| Linhartova et al. [28], 2018 | Case-Control Study | To determine IL-8 plasma levels; IL-8 (−251A/T, rs4073) and its receptor 2 (CXCR2, +1208C/T, rs112679) polymorphisms; the presence of the selected bacteria in DM1 and DM2 patients and systemically healthy controls (HC) with periodontal status. | - The willingness to participate, compliance with the diagnostic criteria for Chronic periodontitis and or Diabetes Mellitus, and for the control group systemic and periodontal health. - Patients examined by a periodontist and did not receive any treatment before measuring periodontal indices. | - Patients that declined the periodontal treatment for periodontitis; - patients having immunodeficiency disorders, current pregnancy or lactation, immunosuppression attributable to medication or current illness; taking antibiotics or anti-inflammatory drugs with 6 weeks of recruitment; - Subjects with <20 teeth (only in healthy controls) and the inability to consent. | 153 Patients: - DM1 subjects+CP (n = 36, 44.4% Males) -DM2 patients with CP (40.9% Males) - From HC+CP (n = 32, 26.8% Males) - Non-periodontitis NP-HC (n = 41, 31.3% Males) | The mean age was similar for patients with DM1+CP and HC | NR | - GI - PPD - AL - IL-8 plasma levels | Clinical periodontal parameters between NP-HC vs. HC+CP vs. DM1+CP: (mean ± SD) GI (0.3 ± 0.2) vs. (0.9 ± 0.3) vs. (1 ± 0.3) (p < 0.01) N of sites with PPD ≥ 5 mm (0) vs. (18 ± 17) vs. (20 ± 19) (p < 0.01) N of teeth with PPD ≥ 5 mm (0) vs. (10 ± 7) vs. (11 ± 7) (p < 0.01) N of sites with AL ≥ 5 mm (0) vs. (32 ± 21) vs. (38 ± 28) (p < 0.01) N of teeth with AL ≥ 5 mm (0) vs. (15 ± 7) vs. (15 ± 7) (p < 0.01) - HC+CP vs. DM1+CP, similar numbers were found (p > 0.05) There were statistically significant differences between non-periodontitis HC in comparison to HC+CP and DM1+CP in which concerns the GI (p < 0.01); and numbers of sites and teeth with a pocket depth ≥5 mm and attachment loss ≥ 5 mm (p < 0.01). - IL8 plasma levels and clinical parameters: median [interquartile range, IQR] DM1+CP vs. HC+CP: 15.09 pg/mL [9.73–20.32] vs. 11.02 pg/mL [6.47–15.17], (p ≤ 0.05) - NP- HC vs. HC+CP, (10.53 pg/mL [8.48–12.58] vs. 11.02 pg/mL [6.47–15.17] DM1 patients had significantly higher levels of IL-8 than did HC+CP individuals (p ≤ 0.05). The groups of non-periodontitis HC and HC+CP, exhibited similar IL-8 plasma levels. - IL-8 plasma levels in DM1 GMC vs. DM1 PMC: 12.68 pg/mL [10.52–40.56] vs. 14.04 pg/mL [10.05–19.67], (p > 0.05) Concentrations of circulating IL-8 levels were not significantly associated with the level of glycemic control (blood glucose and HbA1c and clinical parameters like GI, PPD and AL (p > 0.05). However, patients with DM1 showed higher circulating IL-8 plasma levels than HC+CP/non-periodontitis HC. |
| Roy et al. [25], 2019 | Cross-sectional study | To evaluate the periodontal clinical conditions and oral health behaviour in a cohort of subjects DM1 and in a control group matched for age, sex and smoking status. | Subjects diagnosed with DM1 for more than a year and have at least 10 natural remaining teeth. | Individuals who had taken antibiotics in the previous 3 months. Subjects with history of systemic disease like cancer, HIV, bone metabolic disease, history of radiation or immunosuppressive/modulating therapy; disorders that compromise wound healing. | Patients group control: (n = 50 [30 Males/ 20 Females]) Patients DM1: (n = 50 [30 Males/ 20 Females]) | 18–85 year-aged | July 2016–July 2018 | - GI - PI - PPD - BOP - CAL - REC - HbA1c | Dental examination results of Control vs. DM1: (%±SD) GI: 0.4 (0.4) vs. 1.1 (0.7) (p = 0.000) BOP: 29.4 (16.4) vs. 40.5 (22.2) (p = 0.009) Number of sites PI > 1, 13.8 (14.5) vs. 23.9 (27.2) (p = 0.047) Number of sites GI > 1, 18.8 (23.1) vs. 59.2 (57.6) (p = 0.001) The mean presence of plaque, GI, BOP, and the mean sites with GI score ≥ 1, were appreciably higher in DM1 group than in the control group. - PPD, REC, AL and the mean number of sites with a PI score of ≥1 and mean number of sites with PPD > 4 mm that bleed upon probing did not differ between the groups. Periodontal status Control vs. DM1: n (%) Gingivitis: 30 (60.0) vs. 34 (68.0) Periodontitis: 14 (28.0) vs. 15 (30.0) Gingivitis was present in 68% of the diabetics. - Periodontal parameters between controls vs. diabetics: mean ± SD younger (<40 years old) subjects PI 0.3 (0.2) vs. 0.6 (0.4) (p = 0.004) GI 0.3 (0.3) vs. 1.1 (0.7) (p = 0.000) Older (>40 years old) subjects PI 0.4(0.3) vs. 0.5(0.4) (p = 0.260) GI 0.5(0.4) vs. 1.0(0.6) (p = 0.003) Diabetics <40 years old had significantly more plaque (p = 0.004) and inflammation (GI; p < 0.001) compared with their matched controls. In the older group (>40 years old), gingival inflammation was markedly higher in diabetic patients compared with controls (p = 0.003) Mixed effects logistic regression for odds of periodontitis: Univariable OR [95% CI] Age 1.10 [1.05, 11.17], (p < 0.001) BOP 1.04 [1.02, 1.09], (p = 0.009) The only variables identified as determinants of the periodontal condition in both diabetic and control were age (p < 0.001) and BOP (0.009). Mixed effects logistic regression for odds of periodontitis among diabetic patients: Age 1.09 [1.04,1.16], (p = 0.003) HbA1c 0.53 [0.27,0.89], (p = 0.04) BOP 1.03 [1.00,1.06], (p = 0.048) Examining the associations of the parameters with periodontitis only among diabetic patients age, HbA1c, BOP were significantly associated with periodontitis. |
| Sun et al. [20], 2019 | Cohort study | To determine the quantified risk of PD and the influence of emergency visits and hospitalizations in PD development in DM1 patients. | DM1 patients aged <40 years with newly diagnosed DM1 (ICD [International Classification of Diseases]- 9 codes 250.x1 and 250.x3) within the RCIPD (Registry Catastrophic Illnesses Patient Database) from 1 January 1998 to 31 December 2011. The non-DM1 cohort identified subjects without DM1 during (1998–2011) | Individuals with any history of PDs before the index date (ICD-9 Code 523). | 4248 DM1 patients [2122 Males/2126 Females] 16992 non-DM1 patients [8504 Males/8488 Females] | <40 years | 1998–2011 | - Emergency room visits - Annual hospitalizations - Gingivitis - Periodontitis | DM1 patients vs. Non-DM1: (adjusted hazard ratio—aHR (95%CI) - Risk to PD = 1.45 (1.35–1.56); (p < 0.001). - Average number of annual Emergency room visit for DM1 ≥ 2 = 13.0 (11.1–15.2) (p < 0.001) - Average number of annual hospitalizations for DM1 ≥ 2 = 13.2 (11.5–15.1) (p < 0.001) - Risk to develop gingivitis = 1.47 (1.36–1.59) (p < 0.001) - Risk to develop periodontitis = 1.66 (1.41–1.96) (p < 0.001) The risk of PD was 1.13 (06–1.21) (p < 0.001) in patients aged <20 Gingivitis rate DM1 vs. Control (<20 Y): 43.9 vs. 31.4 (20–40 Y): 33.1 vs. 22.9 Periodontitis rate DM1 vs. Control: (<20 Y): 7.75 vs. 5.50 (20–40 Y): 15.2 vs. 8.13 People 20–40 aged have a lower incidence of gingivitis and a higher incidence of periodontitis than those with age < 20 in both case and control groups. |
| Keles et al. [30], 2020 | Case-control study | To compare the Gingival Crevicular Fluid IL-18 and [TNF]-α levels in children with or without DM1 or gingivitis; To investigate whether GCF IL-18 and [TNF]-α are useful markers for gingivitis in patients with DM1. | Age between 8 and 14 years; diagnosed with DM1 by a pediatric endocrinologist at least 12 months prior to the study, with an HbA1c level < 7.5%; having fully erupted caries-free maxillary and mandibular first molars and incisors; do not have any systemic diseases (healthy group). | Having any other known systemic chronic illnesses; HbA1c level > 7.5%; having any destructive periodontal disease or periodontal therapy involved antimicrobial or anti-inflammatory drugs in the past 6 months; having restorative and endodontic therapy requirement; taking immunosuppressive drugs in the past 6 months; taking any medication regularly; having orthodontic treatment and having clinical attachment loss. | 44 Systemically healthy children [20 Males/24 females]: Systematic and Periodontally healthy children (H, n = 22) Systematic healthy children with Gingivitis (G, N = 22) 44 Children with DM1 [19 Males/25 females]: Periodontally healthy children with DM1(DM1+H, n = 22) DM1 Children with gingivitis (DM1+G, n = 22) | 8–14 years | April–June 2019 | - HbA1c - PI - PPD - GI - GCF volume - (TNF)-α - IL-18 | TNF-α and IL-18 values in DM1 vs. H Children: mean ± SD TNF-α total amount (pg/sample): 3.49 (0.94–5.35) vs. 3.30 (3.62–4.77) IL-18 (pg/sample):0.51 (0.36–0.92) vs. 0.52 (0.42–0.63) (p > 0.05). No significant differences in the IL-18 and TNF-α total amounts between the group of DM1 children and the systemically healthy children (p > 0.05). H vs. G vs. DM1+H vs. DM1+G: mean ± SD PI 0.30 (0.0–0.60) vs. 1.90 (1.00–2.00) vs. 0.30 (0.0–0.5) vs. 1.89 (0.9–2.79) (p < 0.0001) GI (0.54 ± 0.17) vs. (2.07 ± 0.38) vs. (0.51 ± 0.19) vs. (2.24 ± 0.40) (p < 0.0001) PPD (mm)—(0.93 ± 0.35) vs. (2.03 ± 0.34) vs. (1.0 ± 0.31) vs. (2.23 ± 0.46) (p < 0.0001) TNF-α (pg/μL)—47.93 (24.23–125.30) vs. 15.37 (1.06–33.4) vs. 43.65 (11.66–231.76) vs. 17.39 (8.96–33.40) (p < 0.0001) IL-18 (pg/μL): 8.53 (3.76–19.54) vs. 2.05(0.16–3.90) vs. 7.21 (2.79–40.12) vs. 2.49 (1.04–5.45) (p < 0.0001) The gingivitis subgroups showed a significantly higher PI, GI, PPD, GCF volume, and TNF-α total amounts than the H subgroups (p < 0.0001). - IL-18 concentrations were significantly higher in the periodontally healthy subgroups than in gingivitis subgroups. - TNF-α were positively correlated with PI, GI, PPD, GCF volumes and IL-18 concentration (r = 0.552, p = 0.01; r = 0.579, p = 0.01; r = 0.534, p = 0.01, respectively). - There was a negative correlation between the IL-18 concentration and the TNF-α (−0.524, p = 0.01). |
| Dicembrini et al. [11], 2021 | Cross-sectional study | To investigate the prevalence of PD in patients DM1 and its association with glycemic control and glucose variability. | - DM1 patients aged ≥ 18 years and currently treated with multiple daily insulin injections or continuous subcutaneous insulin infusion, who provided their written informed consent and had been continuously using for the last three months the FreeStyle Libre Flash Glucose Monitoring (FGM) system. | Individuals with history of cancer, HIV, bone metabolic disease, history of radiation or immunosuppressive/modulating therapy; those who had taken antibiotics, corticosteroids, or non-steroidal anti-inflammatory drugs in the previous 3 months. | 136 DM1 patients [60 Male/76 Female] | 19–81 years | 12 months | - CAL - PPD - CV - HbA1c | - The prevalence of periodontal disease was 63% (Stage I n = 14; stage II n = 20; stage III n = 43; stage IV n = 9) - A significant correlation was found between mean CAL/CV (r = 0.31, p = 0.002), but not HbA1c (r = 0.038 p = 0.673). - Mean PPD/CV but not with HbA1c (r = 0.27 and 0.044; p = 0.007 and 0.619, respectively). - Multiple linear regression model: assuming the mean CAL as dependent variable, age, CV, and smoking habit resulted significantly associated (r = 0.23, p = 0.013; r = 0.33, p = 0.001; r = 0.34, p < 0.001, respectively). - PPD as a dependent variable showed a significant association with glucose CV and smoking habits only (r = 0.23, p = 0.019; r = 0.33, p = 0.001, respectively). |
| Sereti et al. [3], 2021 | Case-control study | To evaluate the GCF levels of MMP-8, IL-8 and AGEs in DM1 patients with different glycemic levels and to compare them to healthy controls. | Individuals DM1 aged between 18 and 85 years old, presented at least 10 natural teeth and were diagnosed for DM1 for more than 1 year. | NR | DM1 patients (n = 50 [30 Males/ 20 Females]) Non-diabetic patients (n = 50 [30 Males/ 20 Females]) | 18–85 years | NR | - HbA1c - MMP-8 - IL-8 - AGEs - PI - GI - BOP | Dental and biochemical parameters between DM1 vs. Non-DM1: mean ± SD GI: 1.1 (0.7) vs. 0.4 (0.4) (p < 0.001) BOP: 40.5 (22.2) vs. 29.4 (16.4) (p = 0.009) Number of sites PI > 1: 23.9 (27.2) vs. 13.8 (14.5) (p = 0.047) IL-8: 220 pg/mL vs. 225 pg/mL, (p = 0.433) MMP-8: 32.1 μg/mL vs. 38.3 μg/mL, (p = 0.538) AGEs: 3.4 μg/mL vs. 5.8 μg/mL, (p = 0.905) - The median GCF levels of MMP-8, IL-8 and AGEs did not differ significantly between groups. - No significant differences were seen in younger (<40 Y) and older (>40 Y) cohorts, in which concern the GCF levels of MMP-8, IL8 and AGEs, between diabetics and controls. - The diabetic group was divided in two sub-groups according to their glycaemic status (HbA1c 6.1–8, and >8%), and no significant differences were observed in GCF between the diabetic subgroups and the controls. |
| Jensen et al. [26], 2021 | Cross-sectional study | To characterize periodontal risk markers (Plaque Index (PI), gingival index (GI), bleeding on probing (BOP) and PPD; To determine the relationship between periodontal risk markers and glycemic control; To determine the relationship between the oral microbiota and both glycemic control and periodontal risk markers. | Individuals aged between 8 and 18 years, who had been previously diagnosed with DM1 by detectable islet cell autoantibodies. | Subjects diagnosed with diabetes other than DM1 or inadequate English language skills to understand the information sheet. Subjects who had an intercurrent fever or infection, diabetic ketosis, or those who were taking antibiotics on the scheduled day of the dental examination were rescheduled. | 77 Patients [37 Males/39 Females] | 13 ± 2.6 years | February 2018–March 2019 | - PI - GI - BOP - PPD - HbA1c | - Median HbA1c of 8.5% (range 5.8–13.3) - 49% had early markers of PD - 1% increase in HbA1c was independently associated with an average increase in BOP OF 25% (p = 0.002) an increase in the rate of sites with PPD > 3 mm of 54% (p = 0.003) - HbA1c was positively correlated with PI (Rho = 0.34; p = 0.002), GI (Rho = 0.30; p = 0.009), BOP (Rho = 0.44; p = 0.0001), PPD > 3 mm (Rho = 0.21; p = 0.06). The worsening of glycemic control is associated with increased severity of early markers of periodontal disease in children and adolescents with DM1. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, R.; Ríos-Carrasco, B.; Monteiro, L.; López-Jarana, P.; Carneiro, F.; Relvas, M. Association between Type 1 Diabetes Mellitus and Periodontal Diseases. J. Clin. Med. 2023, 12, 1147. https://doi.org/10.3390/jcm12031147
Costa R, Ríos-Carrasco B, Monteiro L, López-Jarana P, Carneiro F, Relvas M. Association between Type 1 Diabetes Mellitus and Periodontal Diseases. Journal of Clinical Medicine. 2023; 12(3):1147. https://doi.org/10.3390/jcm12031147
Chicago/Turabian StyleCosta, Rosana, Blanca Ríos-Carrasco, Luís Monteiro, Paula López-Jarana, Filipa Carneiro, and Marta Relvas. 2023. "Association between Type 1 Diabetes Mellitus and Periodontal Diseases" Journal of Clinical Medicine 12, no. 3: 1147. https://doi.org/10.3390/jcm12031147
APA StyleCosta, R., Ríos-Carrasco, B., Monteiro, L., López-Jarana, P., Carneiro, F., & Relvas, M. (2023). Association between Type 1 Diabetes Mellitus and Periodontal Diseases. Journal of Clinical Medicine, 12(3), 1147. https://doi.org/10.3390/jcm12031147