
Choroidal and Retinal Imaging Biomarkers in Different Types of Macular Neovascularization

 ,
,  ,
,  ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Imaging Protocol
2.3. OCT Analysis
2.4. OCTA Analysis
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Patients Included in the Analysis
3.2. SD-OCT and OCTA Parameters
3.3. Correlation Network Analysis for MNV Types
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nickla, D.L.; Wallman, J. The Multifunctional Choroid. Prog. Retin. Eye Res. 2010, 29, 144–168. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.E.; Kang, S.W.; Lee, J.H.; Kim, Y.T. Choroidal Thickness in Polypoidal Choroidal Vasculopathy and Exudative Age-Related Macular Degeneration. Ophthalmology 2011, 118, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, H.; Yamagishi, T.; Yamazaki, T.; Kawasaki, R.; Kinoshita, S. Subfoveal Choroidal Thickness in Typical Age-Related Macular Degeneration and Polypoidal Choroidal Vasculopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Mullins, R.F.; Johnson, M.N.; Faidley, E.A.; Skeie, J.M.; Huang, J. Choriocapillaris Vascular Dropout Related to Density of Drusen in Human Eyes with Early Age-Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2011, 52, 1606. [Google Scholar] [CrossRef]
- Kim, J.; Jun, J.; Lee, S.; Lee, M. Retinal Microvasculature and Choriocapillaris Impairments according to the Stage of Dry Age-Related Macular Degeneration. Clin. Exp. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Drexler, W.; Fujimoto, J. State-of-The-Art Retinal Optical Coherence Tomography. Prog. Retin. Eye Res. 2008, 27, 45–88. [Google Scholar] [CrossRef]
- Kishi, S. Impact of Swept Source Optical Coherence Tomography on Ophthalmology. Taiwan J. Ophthalmol. 2016, 6, 58–68. [Google Scholar] [CrossRef]
- Ruiz-Medrano, J.; Ruiz-Moreno, J.M.; Goud, A.; Vupparaboina, K.K.; Jana, S.; Chhablani, J. Age-Related Changes in Choroidal Vascular Density of Healthy Subjects Based on Image Binarization of Swept-Source Optical Coherence Tomography. Retina 2018, 38, 508–515. [Google Scholar] [CrossRef]
- Iwata, A.; Mitamura, Y.; Niki, M.; Semba, K.; Egawa, M.; Katome, T.; Sonoda, S.; Sakamoto, T. Binarization of Enhanced Depth Imaging Optical Coherence Tomographic Images of an Eye with Wyburn-Mason Syndrome: A Case Report. BMC Ophthalmol. 2015, 15, 19. [Google Scholar] [CrossRef]
- Tian, J.; Marziliano, P.; Baskaran, M.; Tun, T.A.; Aung, T. Automatic Segmentation of the Choroid in Enhanced Depth Imaging Optical Coherence Tomography Images. Biomed. Opt. Express 2013, 4, 397. [Google Scholar] [CrossRef]
- Agrawal, R.; Gupta, P.; Tan, K.-A.; Cheung, C.M.G.; Wong, T.-Y.; Cheng, C.-Y. Choroidal Vascularity Index as a Measure of Vascular Status of the Choroid: Measurements in Healthy Eyes from a Population-Based Study. Sci. Rep. 2016, 6, 21090. [Google Scholar] [CrossRef]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Uchino, E.; Kawano, H.; Yoshihara, N.; Terasaki, H.; Shirasawa, M.; Tomita, M.; Ishibashi, T. Luminal and Stromal Areas of Choroid Determined by Binarization Method of Optical Coherence Tomographic Images. Am. J. Ophthalmol. 2015, 159, 1123–1131.e1. [Google Scholar] [CrossRef]
- Sonoda, S.; Sakamoto, T.; Yamashita, T.; Shirasawa, M.; Uchino, E.; Terasaki, H.; Tomita, M. Choroidal Structure in Normal Eyes and after Photodynamic Therapy Determined by Binarization of Optical Coherence Tomographic Images. Investig. Opthalmol. Vis. Sci. 2014, 55, 3893. [Google Scholar] [CrossRef]
- Toto, L.; Ruggeri, M.L.; Evangelista, F.; Viggiano, P.; D’Aloisio, R.; De Nicola, C.; Falconio, G.; Di Nicola, M.; Porreca, A.; Mastropasqua, R. Choroidal Modifications Assessed by Means of Choroidal Vascularity Index after Oral Eplerenone Treatment in Chronic Central Serous Chorioretinopathy. Eye 2022. [Google Scholar] [CrossRef]
- Breher, K.; Terry, L.; Bower, T.; Wahl, S. Choroidal Biomarkers: A Repeatability and Topographical Comparison of Choroidal Thickness and Choroidal Vascularity Index in Healthy Eyes. Transl. Vis. Sci. Technol. 2020, 9, 8. [Google Scholar] [CrossRef]
- Iovino, C.; Pellegrini, M.; Bernabei, F.; Borrelli, E.; Sacconi, R.; Govetto, A.; Vagge, A.; Di Zazzo, A.; Forlini, M.; Finocchio, L.; et al. Choroidal Vascularity Index: An In-Depth Analysis of This Novel Optical Coherence Tomography Parameter. J. Clin. Med. 2020, 9, 595. [Google Scholar] [CrossRef]
- Jonas, J.B.; Forster, T.M.; Steinmetz, P.; Schlichtenbrede, F.C.; Harder, B.C. Choroidal Thickness in Age-Related Macular Degeneration. Retina 2014, 34, 1149–1155. [Google Scholar] [CrossRef]
- Viggiano, P.; Toto, L.; Ferro, G.; Evangelista, F.; Porreca, A.; Mastropasqua, R. Choroidal Structural Changes in Different Intermediate AMD Patterns. Eur. J. Ophthalmol. 2021, 32, 460–467. [Google Scholar] [CrossRef]
- Corvi, F.; Souied, E.H.; Capuano, V.; Costanzo, E.; Benatti, L.; Querques, L.; Bandello, F.; Querques, G. Choroidal Structure in Eyes with Drusen and Reticular Pseudodrusen Determined by Binarisation of Optical Coherence Tomographic Images. Br. J. Ophthalmol. 2016, 101, 348–352. [Google Scholar] [CrossRef]
- Giannaccare, G.; Pellegrini, M.; Sebastiani, S.; Bernabei, F.; Moscardelli, F.; Iovino, C.; Napoli, P.E.; Campos, E. Choroidal Vascularity Index Quantification in Geographic Atrophy Using Binarization of Enhanced-Depth Imaging Optical Coherence Tomographic Scans. Retina 2020, 40, 960–965. [Google Scholar] [CrossRef]
- Wei, X.; Ting, D.S.W.; Ng, W.Y.; Khandelwal, N.; Agrawal, R.; Cheung, C.M.G. Choroidal Vascularity Index. Retina 2017, 37, 1120–1125. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, A.; Benatti, E.; Cozzi, M.; Erba, S.; Vaishnavi, S.; Vupparaboina, K.K.; Staurenghi, G.; Chhablani, J.; Gillies, M.; Viola, F. Choroidal Structural Changes Correlate with Neovascular Activity in Neovascular Age Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2018, 59, 3836. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Ding, J.; Sen, P.; Rousselot, A.; Chan, A.; Nivison-Smith, L.; Wei, X.; Mahajan, S.; Kim, R.; Mishra, C.; et al. Exploring Choroidal Angioarchitecture in Health and Disease Using Choroidal Vascularity Index. Prog. Retin. Eye Res. 2020, 77, 100829. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Jaffe, G.J.; Sarraf, D.; Freund, K.B.; Sadda, S.R.; Staurenghi, G.; Waheed, N.K.; Chakravarthy, U.; Rosenfeld, P.J.; Holz, F.G.; et al. Consensus Nomenclature for Reporting Neovascular Age-Related Macular Degeneration Data. Ophthalmology 2020, 127, 616–636. [Google Scholar] [CrossRef]
- Mastropasqua, R.; Evangelista, F.; Amodei, F.; D’Aloisio, R.; Pinto, F.; Doronzo, E.; Viggiano, P.; Porreca, A.; Di Nicola, M.; Parravano, M.; et al. Optical Coherence Tomography Angiography in Macular Neovascularization: A Comparison between Different OCTA Devices. Transl. Vis. Sci. Technol. 2020, 9, 6. [Google Scholar] [CrossRef]
- Corvi, F.; Cozzi, M.; Barbolini, E.; Nizza, D.; Belotti, M.; Staurenghi, G.; Giani, A. Comparison between Several Optical Coherence Tomography Angiography Devices and Indocyanine Green Angiography of Choroidal Neovascularization. Retina 2020, 40, 873–880. [Google Scholar] [CrossRef]
- Velaga, S.B.; Nittala, M.G.; Vupparaboina, K.K.; Jana, S.; Chhablani, J.; Haines, J.; Pericak-Vance, M.A.; Stambolian, D.; Sadda, S.R. Choroidal Vascularity Index and Choroidal Thickness In Eyes with Reticular Pseudodrusen. Retina 2019, 40, 612–617. [Google Scholar] [CrossRef]
- Koh, L.H.L.; Agrawal, R.; Khandelwal, N.; Sai Charan, L.; Chhablani, J. Choroidal Vascular Changes in Age-Related Macular Degeneration. Acta Ophthalmol. 2017, 95, e597–e601. [Google Scholar] [CrossRef]
- Temel, E.; Asikgarip, N. Choroidal Structural Changes Determined by the Binarization Method after Intravitreal Aflibercept Treatment in Neovascular Age-Related Macular Degeneration. Int. J. Ophthalmol. 2021, 14, 1213–1217. [Google Scholar] [CrossRef]
- Pellegrini, M.; Bernabei, F.; Mercanti, A.; Sebastiani, S.; Peiretti, E.; Iovino, C.; Casini, G.; Loiudice, P.; Scorcia, V.; Giannaccare, G. Short-Term Choroidal Vascular Changes after Aflibercept Therapy for Neovascular Age-Related Macular Degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 259, 911–918. [Google Scholar] [CrossRef]
- Toto, L.; Ruggeri, M.L.; D’Aloisio, R.; De Nicola, C.; Trivigno, C.; Cerino, L.; Di Marzio, G.; Di Nicola, M.; Porreca, A.; Mastropasqua, R. Brolucizumab Intravitreal Injection in Macular Neovascularization Type 1: VA, SD-OCT and OCTA Parameters Changes during a 16-Weeks Follow Up. Ophthalmic Res. 2022, 66, 218–227. [Google Scholar] [CrossRef]
- Chun, H.; Suh, H.; Kim, J.Y.; Kwak, J.H.; Kim, R.Y.; Kim, M.; Park, Y.-G.; Park, Y.-H. Choroidal Vascularity Index Change in Macular Telangiectasia Type 2. PLoS ONE 2022, 17, e0262112. [Google Scholar] [CrossRef]
- Karasu, B.; Celebi, A.R.C. Choroidal Vascularity Index: An Enhanced Depth Optical Coherence Tomography-Based Parameter to Determine Vascular Status in Patients with Proliferative and Non-Proliferative Macular Telangiectasia. Int. Ophthalmol. 2021, 41, 3505–3513. [Google Scholar] [CrossRef]
- Chhablani, J.; Kozak, I.; Jonnadula, G.B.; Venkata, A.; Narayanan, R.; Pappuru, R.R.; Rao, P.S. Choroidal Thickness in Macular Telangiectasia Type 2. Retina 2014, 34, 1819–1823. [Google Scholar] [CrossRef]
- Melrose, M.A.; Magargal, L.E.; Goldberg, R.E.; Annesley, W., Jr. Subretinal Neovascular Membranes Associated with Choroidal Nonperfusion and Retinal Ischemia. Ann. Ophtalmol. 1987, 19, 396–399. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | MNV Type 1 | MNV Type 2 | MNV Type 3 | p-Value |
|---|---|---|---|---|
| n = 37 | n = 52 | n = 16 | ||
| Gender, n (%) | 0.222 a | |||
| Female | 15 (40.5) | 20 (38.5) | 10 (62.5) | |
| Male | 22 (59.5) | 32 (61.5) | 6 (37.5) | |
| Age (years) median [q1;q3] | 75.0 [70.0;80.0] | 78.0 [71.0;81.0] | 73.0 [69.8;81.0] | 0.709 b |
| Variables | MNV Type 1 | MNV Type 2 | MNV Type 3 | p-Value |
|---|---|---|---|---|
| n = 37 | n = 52 | n = 16 | ||
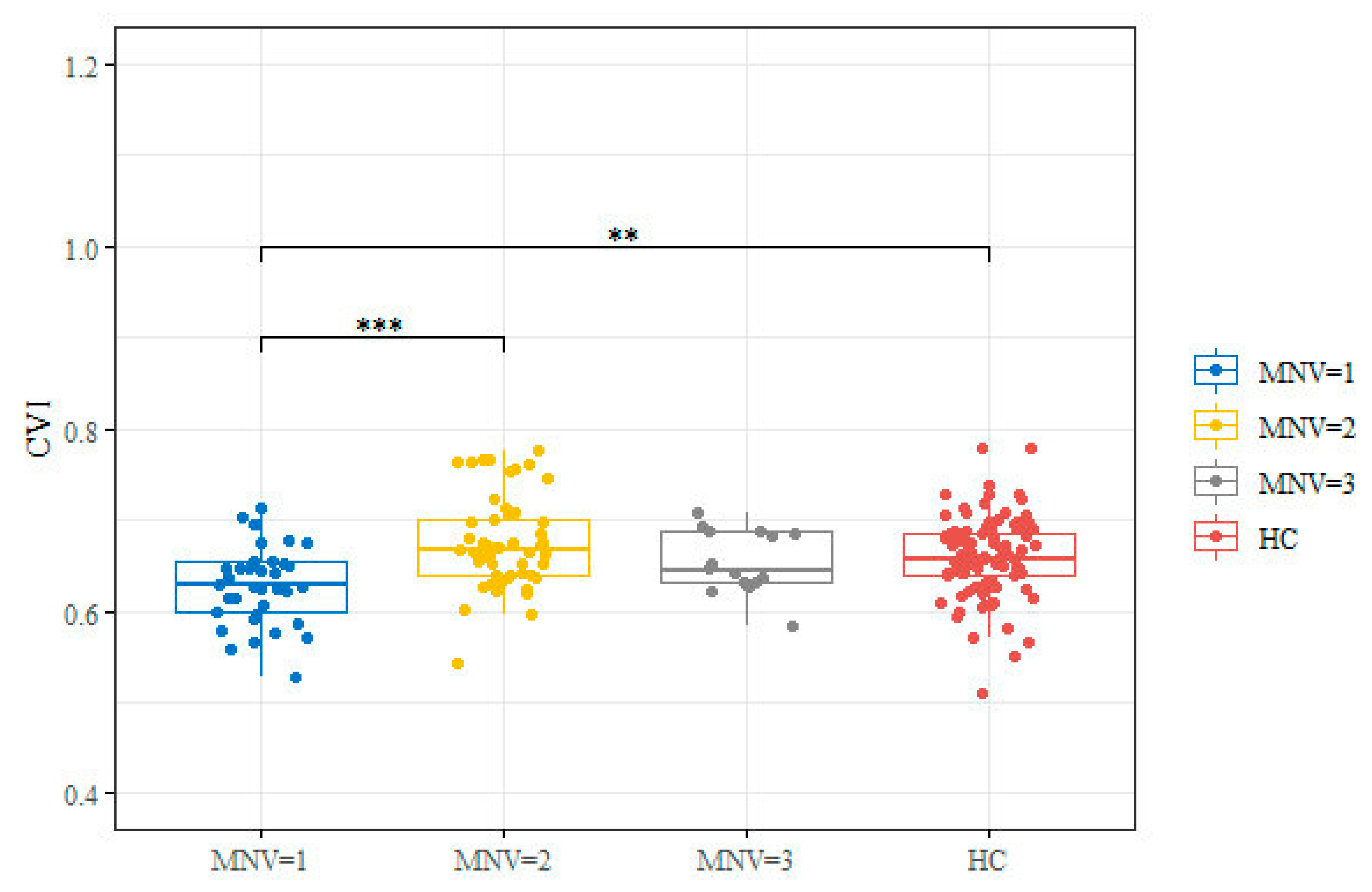
| CVI | 0.63 [0.60;0.65] | 0.67 [0.64;0.70] | 0.64 [0.63;0.69] | <0.001 |
| Subfoveal CT (μm) | 176.00 [142.00;234.00] | 172.00 [140.00;212.00] | 146.00 [136.00;210.00] | 0.458 |
| CMT (μm) | 345.00 [319.00;417.00] | 442.00 [352.00;547.00] | 388.00 [306.00;482.00] | 0.006 |
| ORCCFA (mm2) | 0.18 [0.12;0.22] | 0.14 [0.10;0.18] | 0.17 [0.12;0.20] | 0.032 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toto, L.; Ruggeri, M.L.; Evangelista, F.; Trivigno, C.; D’Aloisio, R.; De Nicola, C.; Viggiano, P.; Doronzo, E.; Di Nicola, M.; Porreca, A.; et al. Choroidal and Retinal Imaging Biomarkers in Different Types of Macular Neovascularization. J. Clin. Med. 2023, 12, 1140. https://doi.org/10.3390/jcm12031140
Toto L, Ruggeri ML, Evangelista F, Trivigno C, D’Aloisio R, De Nicola C, Viggiano P, Doronzo E, Di Nicola M, Porreca A, et al. Choroidal and Retinal Imaging Biomarkers in Different Types of Macular Neovascularization. Journal of Clinical Medicine. 2023; 12(3):1140. https://doi.org/10.3390/jcm12031140
Chicago/Turabian StyleToto, Lisa, Maria Ludovica Ruggeri, Federica Evangelista, Chiara Trivigno, Rossella D’Aloisio, Chiara De Nicola, Pasquale Viggiano, Emanuele Doronzo, Marta Di Nicola, Annamaria Porreca, and et al. 2023. "Choroidal and Retinal Imaging Biomarkers in Different Types of Macular Neovascularization" Journal of Clinical Medicine 12, no. 3: 1140. https://doi.org/10.3390/jcm12031140
APA StyleToto, L., Ruggeri, M. L., Evangelista, F., Trivigno, C., D’Aloisio, R., De Nicola, C., Viggiano, P., Doronzo, E., Di Nicola, M., Porreca, A., & Mastropasqua, R. (2023). Choroidal and Retinal Imaging Biomarkers in Different Types of Macular Neovascularization. Journal of Clinical Medicine, 12(3), 1140. https://doi.org/10.3390/jcm12031140