
Cross-Cultural Adaptation and Validation of the Methotrexate Intolerance Severity Score Questionnaire in Portuguese (Brazil) for Children and Adolescents with Juvenile Idiopathic Arthritis
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Translation and Transcultural Adaptation
2.2. Statistical Analysis
3. Results
3.1. Descriptive Data
3.2. Cross-Cultural Adaptation
3.3. Psychometric Issues
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barut, K.; Adrovic, A.; Şahin, S.; Kasapçopur, Ö. Juvenile Idiopathic Arthritis. Balkan Med. J. 2017, 34, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Hūgle, B.; Horneff, G. The role of synthetic drugs in the biologic era: Therapeutic strategies for treating juvenile idiopathic arthritis. Expert Opin. Pharmacother. 2016, 17, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Braun, J. Methotrexate: Optimizing the efficacy in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2011, 3, 151–158. [Google Scholar] [CrossRef]
- Ramanan, A.V.; Whitworth, P.; Baildam, E.M. Use of methotrexate in juvenile idiopathic arthritis. Arch. Dis. Child. 2003, 88, 197–200. [Google Scholar] [CrossRef]
- Canhão, H.; Fonseca, J.E.; Romão, V.C. Old drugs, old problems: Where do we stand in prediction of rheumatoid arthritis responsiveness to methotrexate and other synthetic DMARDs? BMC Med. 2013, 11, 17. [Google Scholar]
- Blazina, S.; Markelj, G.; Avramovic, M.Z.; Toplak, N.; Avcin, T. Management of Juvenile Idiopathic Arthritis: A Clinical Guide. Paediatr. Drugs 2016, 18, 397–412. [Google Scholar] [CrossRef]
- Van der Meer, A.; Wulfraat, N.M.; Prakken, B.j.; Gijsbers, B.; Rademaker, C.M.; Sinnema, G. Psychological side effect of MTX treatment in juvenile idiopathic arthritis: A pilot study. Clin. Exp. Rheumatol. 2007, 25, 480–485. [Google Scholar]
- Bulatovic, M.; Heijstek, M.W.; Verkaaik, M.; van Dijkhuizen, E.H.; Ambrust, W.; Hoppenreijis, E.P.; Kamphuis, S.; Kuis, W.; Egberts, T.C.; Sinnema, G.; et al. High prevalence of methotrexate intolerance in juvenile idiopathic arthritis: Development and validation of a methotrexate intolerance severity score. Arthritis Rheum. 2011, 63, 2007–2013. [Google Scholar] [CrossRef]
- Ćalasan, M.B.; van den Bosch, O.F.; Creemers, M.C.; Custers, M.; Heurkens, A.H.; van Woerkom, J.M.; Wulffraat, N.M. Prevalence of methotrexate intolerance in rheumatoid arthritis and psoriatic arthritis. Arthritis Res Ther. 2013, 15, R217. [Google Scholar] [CrossRef]
- Van Dijkhuizen, E.H.P.; Wulffraat, N.M. Early predictors of prognosis in juvenile idiopathic arthritis: A systematic literature review. Ann. Rheum. Dis. 2014, 74, 12–51. [Google Scholar] [CrossRef]
- Van Dijkhuizen, E.H.; Ćalasan, M.B.; Pluijm, S.M.; de Rotte, M.C.; Vastert, S.; Kamphuis, S.; de Jonge, R.; Wulffraat, N. Prediction of methotrexate intolerance in juvenile idiopathic arthritis: A prospective, observational cohort study. Pediatr. Rheumatol. 2015, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Fatimah, N.; Salim, B.; Nasim, A.; Hussain, K.; Gul, H.; Niazi, S. Frequency of methotrexate intolerance in rheumatoid arthritis patients using the metrotrexate intolerance severity score (MISS questionnaire). Clin. Rheumatol. 2016, 35, 1341–1345. [Google Scholar] [CrossRef] [PubMed]
- Sceuern, A.; Tyrrel, P.N.; Haas, J.P.; Hugle, B. Countermeasures against methotrexate intolerance in juvenile idiopathic arthritis by parents show no effect. Rheumatology 2017, 58, 901–906. [Google Scholar] [CrossRef]
- Fránová, J.; Fingerhutová, S.; Kobrová, K.; Srp, R.; Nemcová, D.; Hoza, J.; Brunner, H.; Haas, J.P.; Hugle, B. Methotrexate efficacy, but not its intolerance, is associated with the dose and route of administration. Pediatr. Rheumatol. Online J. 2016, 14, 36. [Google Scholar] [CrossRef] [PubMed]
- Scheuern, A.; Fischer, N.; McDonald, J.; Haas, J.-P.; Hügle, B. Mutations in the MTHFR gene are not associated with methotrexate intolerance in patients with juvenile idiopathic arthritis. Pediatr. Rheumatol. Online J. 2016, 14, 11. [Google Scholar] [CrossRef]
- Chausset, A.; Fargeix, T.; Pereira, B.; Echaubard, S.; Duquesne, A.; Desjonquères, M. Miss questionnaire in French version: A good tool for children and parentes to assess methotrexate intolerance. Clin. Rheumatol. 2017, 36, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Amaral, J.M.; Brito, M.J.M.; Kakehasi, A.M. Cultural Adaptation and Validation of the Methotrexate Intolerance Severity Score in Brazilian Portuguese for Adults with Rheumatoid Arthritis. J. Clin. Rheumatol. 2021, 27, S168–S172. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.-M.; et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390. [Google Scholar]
- Atilgan, H. Sample Size for Estimation of G and Phi Coefficients in Generalizability Theory. Eurasian J. Educ. Res. 2013, 51, 215–228. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis: A Global Perspective, 7th ed; Pearson Education: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Rejano-Campo, M.; Ferre-Peña, R.; Urraca-Gesto, M.A.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Stuge, B.; Plaza-Manzano, G. Transcultural adaptation and psychometric validation of a Spanish-language version of the PelvicGirdle “Questionnaire”. Health Qual. Life Outcomes 2017, 15, 30. [Google Scholar] [CrossRef] [PubMed]
- Kothari, C.R. Research Methodology: Methods and Techniques, 2nd ed.; New Age International Publishers: New Delhi, India, 2004. [Google Scholar]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. J. Clin. Epidemiol. 2011, 64, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Kaya Akca, U.; Farisogullari, B.; Yardimci, G.K.; Sag, E.; Atalay, E.; Kasap Cuceoglu, M.; Basaran, O.; Kilic, L.; Ozen, S.; Bilginer, Y. Real-world data on MTX tolerance with regimens used in children versus adults. Clin. Rheumatol. 2021, 40, 5095–5102. [Google Scholar] [CrossRef]
- Van Dijkhuizen, E.H.; Pouw, J.N.; Scheuern, A.; Hügle, B.; Hardt, S.; Ganser, G.; Kümmerle-Deschner, J.B.; Horneff, G.; Holzinger, D.; Bulatović Ćalasan, M.; et al. Methotrexate intolerance in oral and subcutaneous administration in patients with juvenile idiopathic arthritis: A cross-sectional, observational study. Clin. Exp. Rheumatol. 2016, 34, 148–154. [Google Scholar] [CrossRef] [PubMed][Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Total Item Correlation | Cronbach’s Alpha |
|---|---|---|
| 1 | 0.62 | 0.87 |
| 2 | 0.46 | 0.78 |
| 3 | 0.64 | 0.76 |
| 4 | 0.72 | 0.75 |
| 5 | 0.67 | 0.76 |
| 6 | 0.68 | 0.75 |
| 7 | 0.61 | 0.76 |
| 8 | 0.47 | 0.77 |
| 9 | 0.66 | 0.75 |
| 10 | 0.56 | 0.88 |
| 11 | 0.69 | 0.87 |
| 12 | 0.76 | 0.87 |
| Items | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
| 1 | 1 | |||||||||||
| 2 | 0.40 ** | 1 | ||||||||||
| 3 | 0.54 ** | 0.45 | 1 | |||||||||
| 4 | 0.56 ** | 0.32 | 0.41 | 1 | ||||||||
| 5 | 0.39 ** | 0.42 | 0.40 | 0.56 | 1 | |||||||
| 6 | 0.42 ** | 0.40 | 0.43 | 0.64 | 0.55 | 1 | ||||||
| 7 | 0.38 ** | 0.31 | 0.34 | 0.51 | 0.50 | 0.38 | 1 | |||||
| 8 | 0.24 ** | 0.28 | 0.20 | 0.18 | 0.39 | 0.26 | 0.43 | 1 | ||||
| 9 | 0.37 ** | 0.22 | 0.34 | 0.42 | 0.37 | 0.39 | 0.32 | 0.32 | 1 | |||
| 10 | 0.16 * | 0.16 | 0.29 | 0.26 | 0.32 | 0.28 | 0.41 | 0.50 | 0.43 | 1 | ||
| 11 | 0.30 ** | 0.23 | 0.38 | 0.43 | 0.40 | 0.43 | 0.30 | 0.34 | 0.69 | 0.57 | 1 | |
| 12 | 0.46 ** | 0.27 | 0.43 | 0.51 | 0.49 | 0.50 | 0.42 | 0.31 | 0.60 | 0.49 | 0.65 | 1 |
| Item | Kappa |
|---|---|
| 1 | 0.87 |
| 2 | 0.81 |
| 3 | 0.76 |
| 4 | 0.88 |
| 5 | 0.86 |
| 6 | 0.80 |
| 7 | 0.95 |
| 8 | 1.0 |
| 9 | 1.0 |
| 10 | 0.92 |
| 11 | 0.81 |
| 12 | 0.84 |
| Item | Kappa | Agreement Percentage (%) |
|---|---|---|
| 1 | 0.66 | 82 |
| 2 | 0.50 | 79 |
| 3 | 0.66 | 84 |
| 4 | 0.83 | 91 |
| 5 | 0.86 | 90 |
| 6 | 0.70 | 96 |
| 7 | 0.94 | 95 |
| 8 | 0.81 | 94 |
| 9 | 0.46 | 89 |
| 10 | 0.90 | 90 |
| 11 | 0.50 | 89 |
| 12 | 0.80 | 95 |
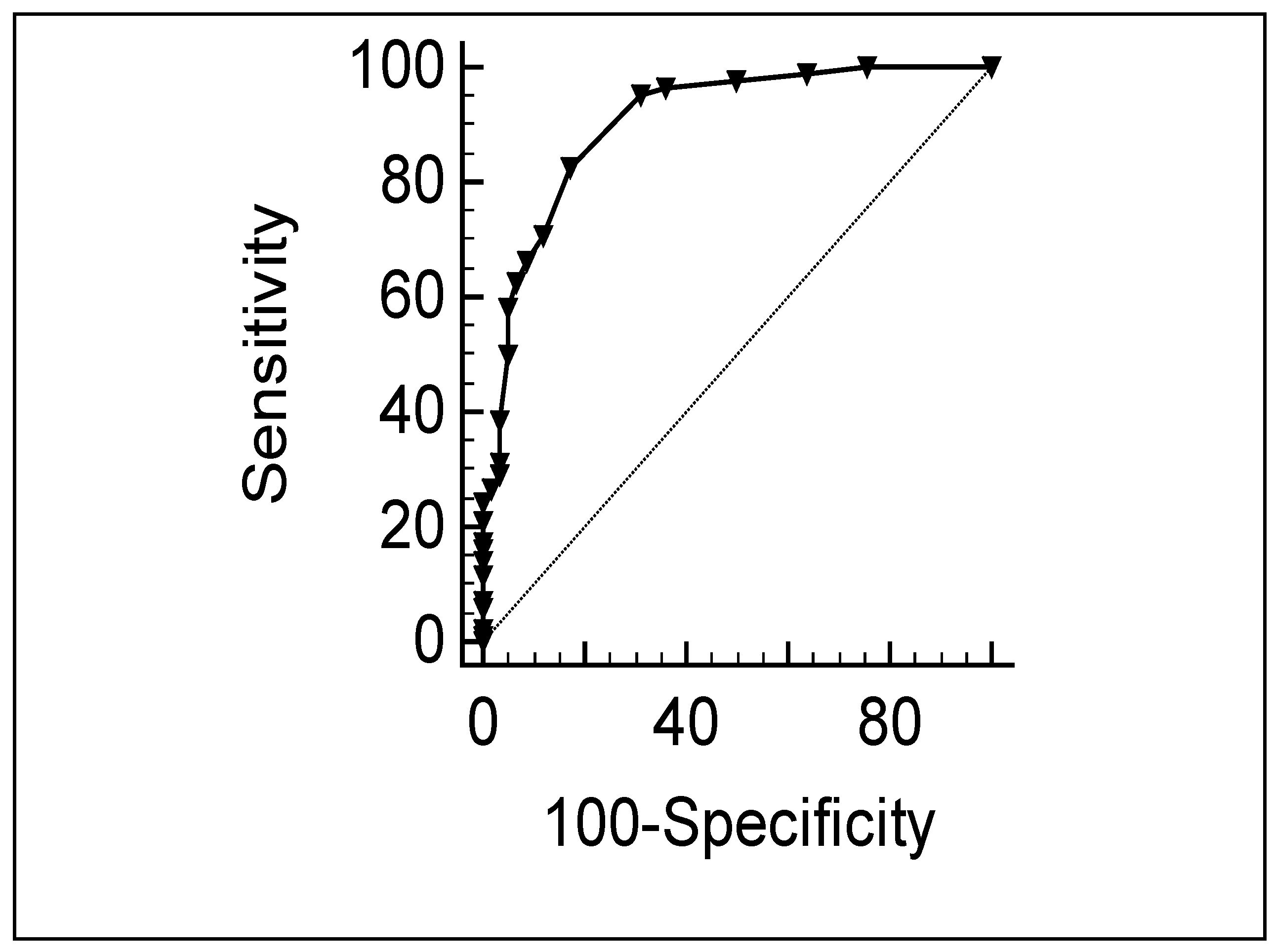
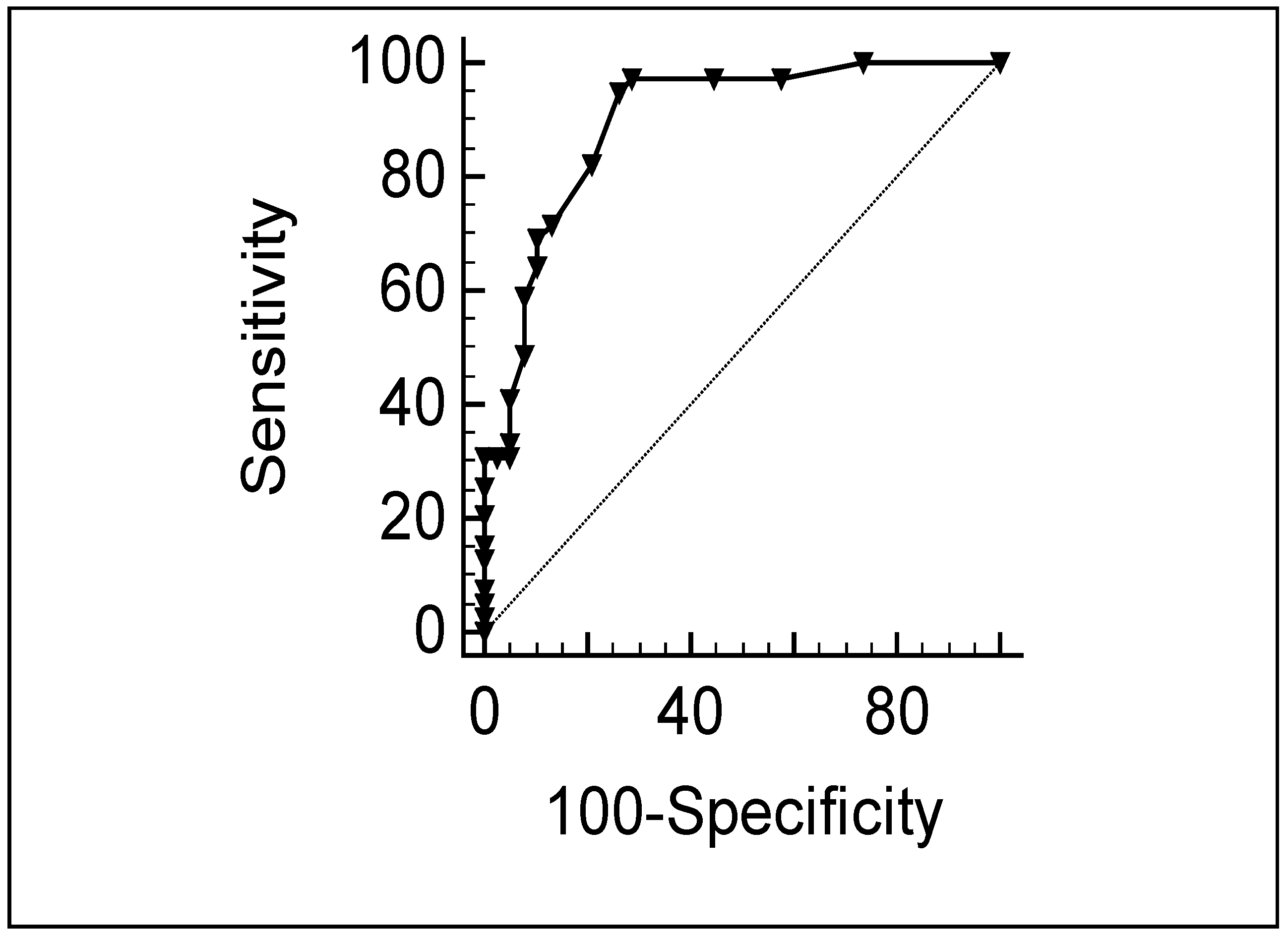
| Cut-Off Scores | Sensitivity | Specificity |
|---|---|---|
| 2 | 98 | 50 |
| 3 | 96 | 64 |
| 4 | 95 | 68 |
| 5 | 84 | 80 |
| 6 | 71 | 87 |
| 7 | 66 | 91 |
| 8 | 63 | 93 |
| 9 | 58 | 95 |
| 10 | 50 | 96 |
| 11 | 40 | 98 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Londe, A.C.; de Amorim, J.C.; Julio, P.R.; Wulffraat, N.M.; Marini, R.; Appenzeller, S. Cross-Cultural Adaptation and Validation of the Methotrexate Intolerance Severity Score Questionnaire in Portuguese (Brazil) for Children and Adolescents with Juvenile Idiopathic Arthritis. J. Clin. Med. 2023, 12, 1116. https://doi.org/10.3390/jcm12031116
Londe AC, de Amorim JC, Julio PR, Wulffraat NM, Marini R, Appenzeller S. Cross-Cultural Adaptation and Validation of the Methotrexate Intolerance Severity Score Questionnaire in Portuguese (Brazil) for Children and Adolescents with Juvenile Idiopathic Arthritis. Journal of Clinical Medicine. 2023; 12(3):1116. https://doi.org/10.3390/jcm12031116
Chicago/Turabian StyleLonde, Ana Carolina, Jaqueline Cristina de Amorim, Paulo Rogério Julio, Nico M. Wulffraat, Roberto Marini, and Simone Appenzeller. 2023. "Cross-Cultural Adaptation and Validation of the Methotrexate Intolerance Severity Score Questionnaire in Portuguese (Brazil) for Children and Adolescents with Juvenile Idiopathic Arthritis" Journal of Clinical Medicine 12, no. 3: 1116. https://doi.org/10.3390/jcm12031116
APA StyleLonde, A. C., de Amorim, J. C., Julio, P. R., Wulffraat, N. M., Marini, R., & Appenzeller, S. (2023). Cross-Cultural Adaptation and Validation of the Methotrexate Intolerance Severity Score Questionnaire in Portuguese (Brazil) for Children and Adolescents with Juvenile Idiopathic Arthritis. Journal of Clinical Medicine, 12(3), 1116. https://doi.org/10.3390/jcm12031116