

Evaluation of Mechanical Versus Manual Root Canal Preparation in Primary Molars—A Comparative In Vitro Study

 , ,
, ,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
- Distal, palatal, mesial and buccal roots of primary molars with a length of ≥7 mm;
- Radii > 5 mm.
- Resorption in the cervical or middle third of the root canals;
- Root caries;
- Previous endodontic treatment;
- Abnormality in tooth morphology.
- FlexMaster® (FM, 04 #30, VDW);
- Hyflex® EDM NiTi files (HF, 25/~ OneFile, Coltène);
- K-Files (KF, #15–35, Kerr).
2.2. Preliminary Tests
2.3. Root Canal Preparation
- FM (experimental group 1):
- Root canals were mechanically prepared with the established Crown-Down NiTi System FM system, according to the manufacturer’s instructions. The last file used was size 04 #30.
- HF (experimental group 2):
- After creating a straight coronal access, the Hyflex CM 25/0.08 file was used as an orifice opener. For the mechanical preparation of the root canals with HF, the following files were used according to the manufacturer’s instructions: 10/0.05 Glidepath File, 20/~ Hyflex EDM One File and 25/~ Hyflex EDM One File.
- KF (control group):
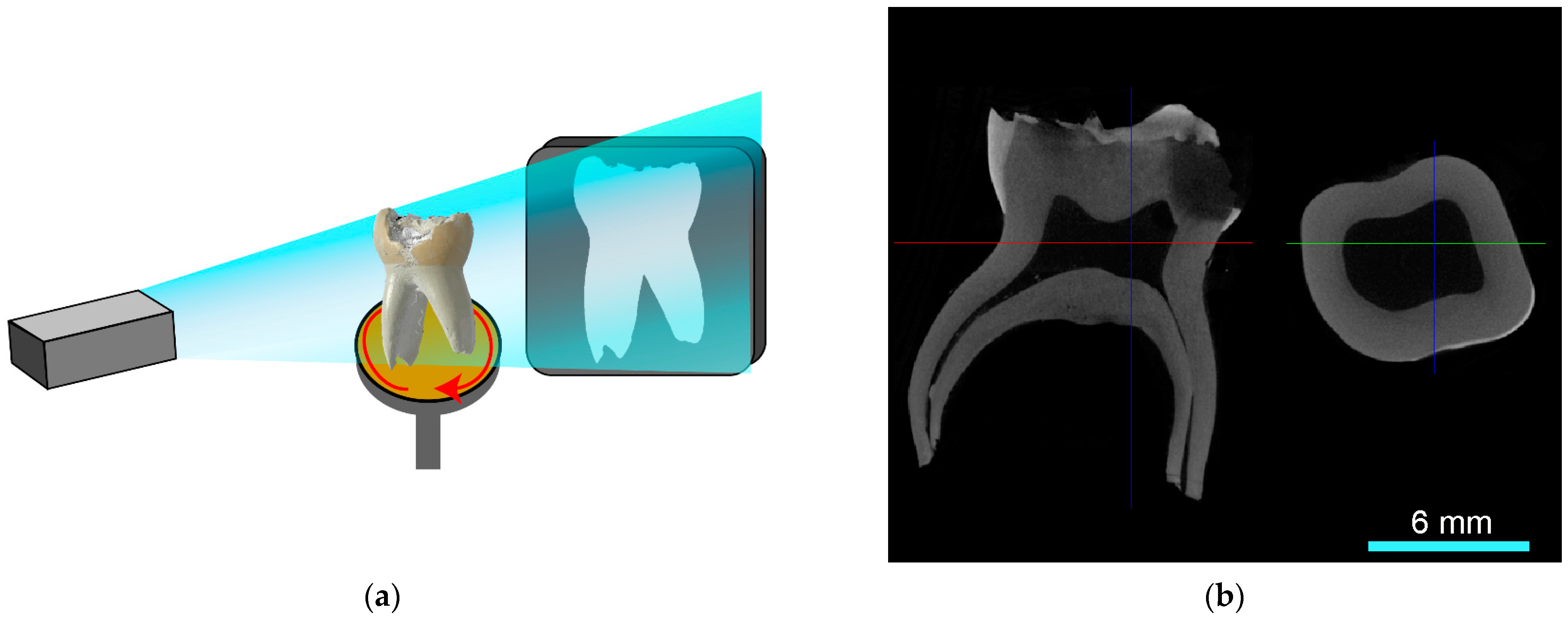
2.4. μ-CT Analysis
2.5. Statistics
3. Results
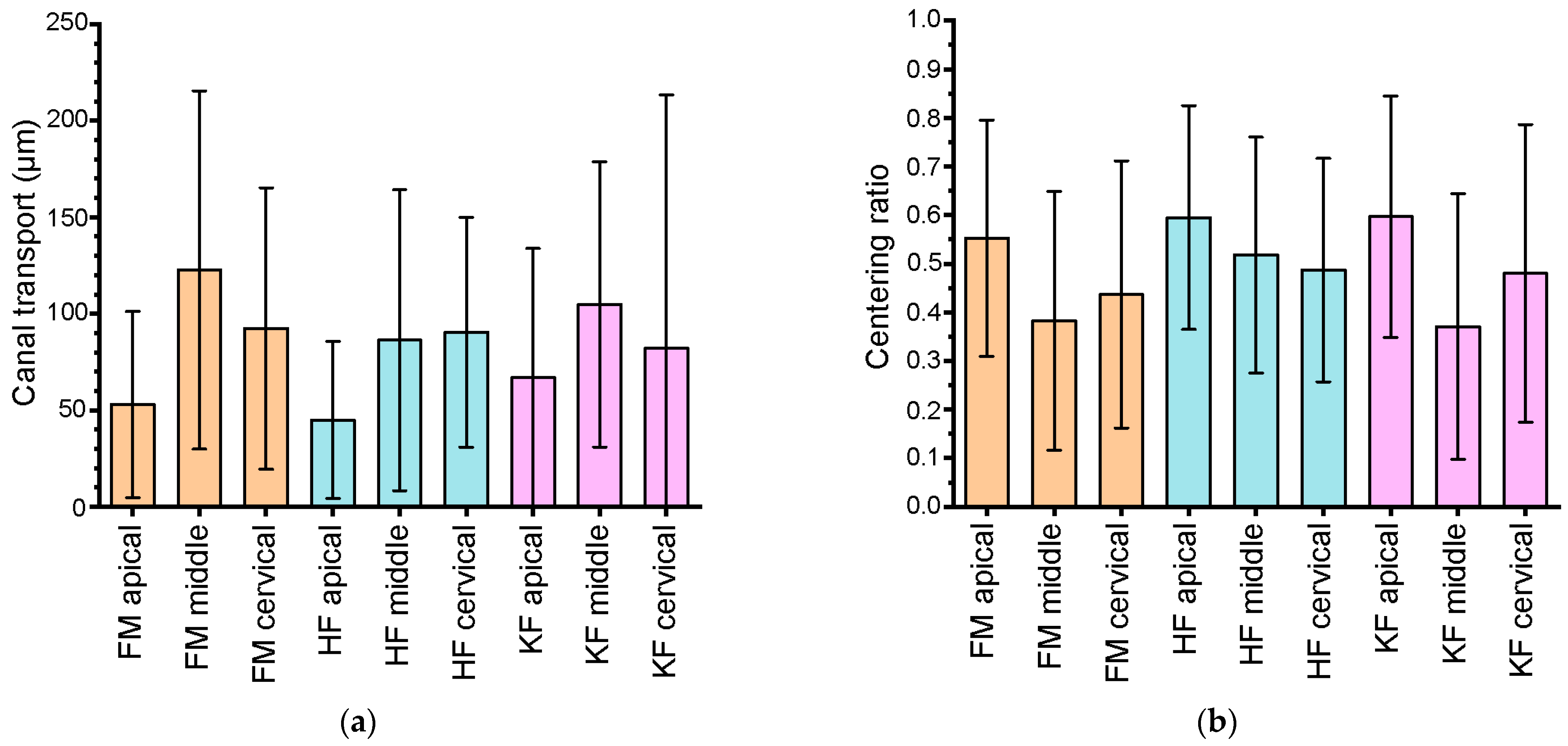
3.1. Root Canal Transport
3.2. Centering Ratio
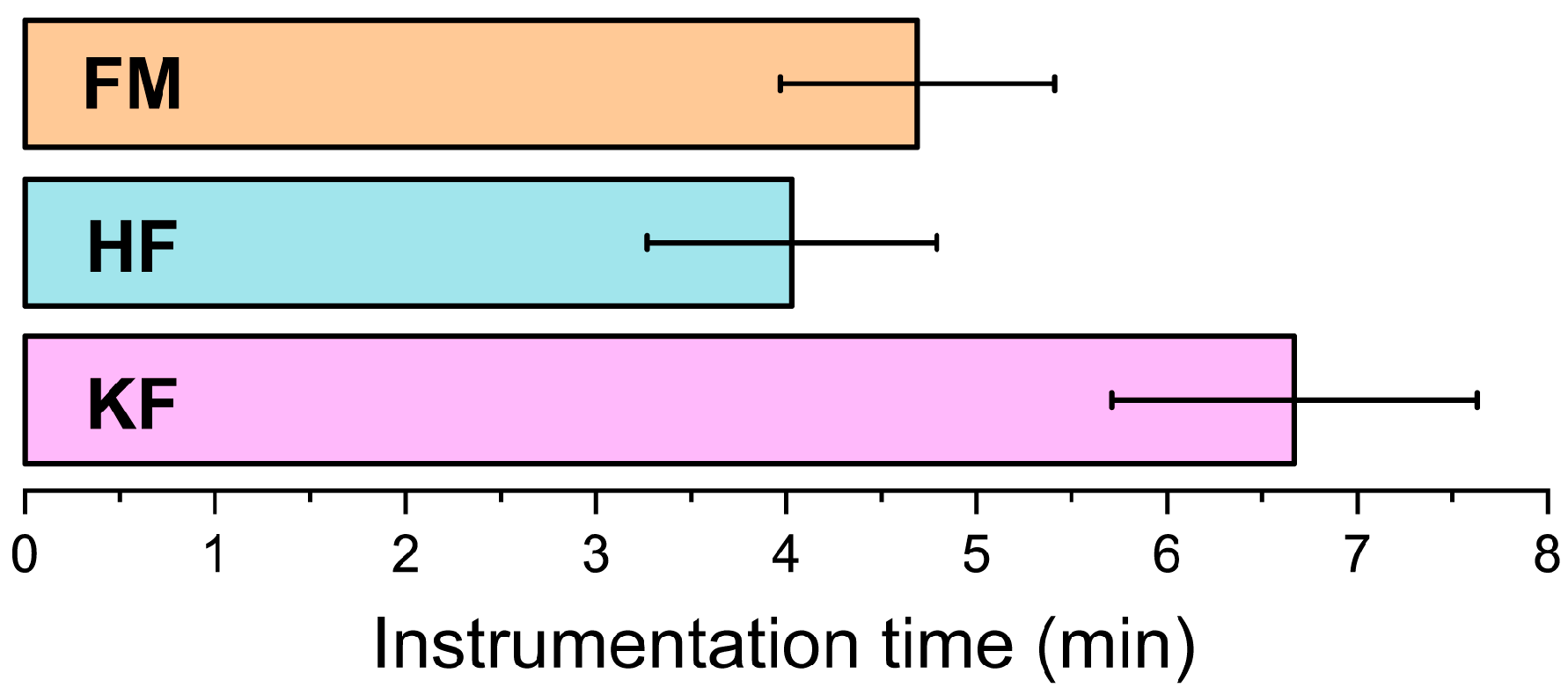
3.3. Instrumentation Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schmoeckel, J.; Santamaría, R.M.; Basner, R.; Schankath, E.; Splieth, C.H. Oral health trends in children: Results from the epidemiological surveys accompanying group prophylaxis in Germany. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Duggal, M.S.; Nooh, A.; High, A. Response of the primary pulp to inflammation: A review of the Leeds studies and challenges for the future. Eur. J. Paediatr. Dent. 2002, 3, 111–114. [Google Scholar] [PubMed]
- Harzer, W.; Hetzer, G.; Huth, K. Gemeinsame Stellungnahme der Deutschen Gesellschaft für ZMK, DGKFO und DGK. Indikation und Gestaltung von Lückenhaltern nach vorzeitigem Milchzahnverlust. DZZ 2004, 59, 1–4. [Google Scholar]
- Rodd, H.D.; Waterhouse, P.J.; Fuks, A.B.; Fayle, S.A.; Moffat, M.A. Pulp therapy for primary molars. Int. J. Paediatr. Dent. 2006, 16, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Poornima, P.; Disha, P.; Nagaveni, N.B.; Roopa, K.B.; Bharath, K.P.; Neena, I.E. Volumetric analysis of hand and rotary root canal instrumentation and filling in primary teeth using Spiral Computed Tomography’—An in vitro study. Int. J. Paediatr. Dent. 2016, 26, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, L.; Silva, L.; Leoni, G.B.; Mazzi-Chaves, J.F.; Carvalho, E.; Consolaro, A.; Sousa-Neto, M.D. Mechanical Preparation Showed Superior Shaping Ability than Manual Technique in Primary Molars—A Micro-Computed Tomography Study. Braz. Dent. J. 2017, 28, 453–460. [Google Scholar] [CrossRef]
- Selvakumar, H.; Kavitha, S.; Thomas, E.; Anadhan, V.; Vijayakumar, R. Computed Tomographic Evaluation of K3 Rotary and Stainless Steel K File Instrumentation in Primary Teeth. J. Clin. Diagn. Res. 2016, 10, Zc05–Zc08. [Google Scholar] [CrossRef]
- Moskovitz, M.T.N. Pulpectomy and root canal treatment (RCT) in primary teeth: Techniques and materials. In Pediatric Endodontics: Current Concepts in Pulp Therapy for Primary and Young Permanent Teeth, 1st ed.; Fuks, A.B., Ed.; Springer International Publishing: Berlin/Heidelberg, Germany, 2016; pp. 72–102. [Google Scholar]
- Reis, T.; Barbosa, C.; Franco, M.; Baptista, C.; Alves, N.; Castelo-Baz, P.; Martin-Cruces, J.; Martin-Biedma, B. 3D-Printed Teeth in Endodontics: Why, How, Problems and Future-A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 7966. [Google Scholar] [CrossRef]
- Shivashankar, M.B.; Niranjan, N.T.; Jayasheel, A.; Kenchanagoudra, M.G. Computed Tomography Evaluation of Canal Transportation and Volumetric Changes in Root Canal Dentin of Curved Canals Using Mtwo, ProTaper and ProTaper Next Rotary System-An In-vitro Study. J. Clin. Diagn. Res. 2016, 10, 10–14. [Google Scholar] [CrossRef]
- Puleio, F.; Bellezza, U.; Torre, A.; Giordano, F.; Lo Giudice, G. Apical Transportation of Apical Foramen by Different NiTi Alloy Systems: A Systematic Review. Appl. Sci. 2023, 13, 10555. [Google Scholar] [CrossRef]
- Panchal, V.; Jeevanandan, G.; Erulappan, S.M. Comparison between the Effectiveness of Rotary and Manual Instrumentation in Primary Teeth: A Systematic Review. Int. J. Clin. Pediatr. Dent. 2019, 12, 340–346. [Google Scholar] [CrossRef]
- Versiani, M.A.; Keleș, A. Applications of Micro-CT Technology in Endodontics. In Micro-Computed Tomography (Micro-CT) in Medicine and Engineering; Orhan, K., Ed.; Springer International Publishing: Cham, Switzerland, 2020; pp. 183–211. [Google Scholar]
- Fumes, A.C.; Sousa-Neto, M.D.; Leoni, G.B.; Versiani, M.A.; da Silva, L.A.; da Silva, R.A.; Consolaro, A. Root canal morphology of primary molars: A micro-computed tomography study. Eur. Arch. Paediatr. Dent. 2014, 15, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Barasuol, J.C.; Alcalde, M.P.; Bortoluzzi, E.A.; Duarte, M.A.H.; Cardoso, M.; Bolan, M. Shaping ability of hand, rotary and reciprocating files in primary teeth: A micro-CT study in vitro. Eur. Arch. Paediatr. Dent. 2021, 22, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Musale, P.K.; Mujawar, S.A. Evaluation of the efficacy of rotary vs. hand files in root canal preparation of primary teeth in vitro using CBCT. Eur. Arch. Paediatr. Dent. 2014, 15, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Cui, Z.; Yan, P.; Jiang, H. A comparison of the shaping ability of three nickel-titanium rotary instruments: A micro-computed tomography study via a contrast radiopaque technique in vitro. BMC Oral Health 2017, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Franco, V.; Fabiani, C.; Taschieri, S.; Malentacca, A.; Bortolin, M.; Del Fabbro, M. Investigation on the shaping ability of nickel-titanium files when used with a reciprocating motion. J. Endod. 2011, 37, 1398–1401. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Orhan, K.; Celikten, B.; Orhan, A.I.; Tufenkci, P.; Sevimay, S. Evaluation of the sealing ability of different root canal sealers: A combined SEM and micro-CT study. J. Appl. Oral Sci. 2018, 26, e20160584. [Google Scholar] [CrossRef]
- Zhao, D.; Shen, Y.; Peng, B.; Haapasalo, M. Micro-computed tomography evaluation of the preparation of mesiobuccal root canals in maxillary first molars with Hyflex CM, Twisted Files, and K3 instruments. J. Endod. 2013, 39, 385–388. [Google Scholar] [CrossRef]
- Venino, P.M.; Citterio, C.L.; Pellegatta, A.; Ciccarelli, M.; Maddalone, M. A Micro-computed Tomography Evaluation of the Shaping Ability of Two Nickel-titanium Instruments, HyFlex EDM and ProTaper Next. J. Endod. 2017, 43, 628–632. [Google Scholar] [CrossRef]
- Schäfer, E.; Lohmann, D. Efficiency of rotary nickel-titanium FlexMaster instruments compared with stainless steel hand K-Flexofile-Part 2. Cleaning effectiveness and instrumentation results in severely curved root canals of extracted teeth. Int. Endod. J. 2002, 35, 514–521. [Google Scholar] [CrossRef]
- Huang, Z.; Quan, J.; Liu, J.; Zhang, W.; Zhang, X.; Hu, X. A microcomputed tomography evaluation of the shaping ability of three thermally-treated nickel-titanium rotary file systems in curved canals. J. Int. Med. Res. 2019, 47, 325–334. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cervical Third 1 Mean (SD) (μm) | Middle Third 2 Mean (SD) (μm) | Apical Third 3 Mean (SD) (μm) | |
|---|---|---|---|
| FM | 80.98 (66.30) | 122.58 (92.64) | 53.00 (48.13) |
| HF | 85.02 (61.27) | 88.13 (80.60) | 39.91 (36.86) |
| KF | 69.44 (72.12) | 109.11 (81.85) | 67.42 (67.69) |
| Cervical Third 1 Mean (SD) (%) | Middle Third 2 Mean (SD) (%) | Apical Third 3 Mean (SD) (%) | |
|---|---|---|---|
| FM | 43.48 (27.16) | 38.64 (26.51) | 55.96 (24.97) |
| HF | 49.91 (23.67) | 51.49 (24.97) | 61.59 (22.87) |
| KF | 47.97 (30.93) | 37.40 (27.50) | 60.00 (24.98) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz-Weidner, N.; Wang, J.; Steinbart, J.; Windfelder, A.G.; Krombach, G.A.; Krämer, N.; Schlenz, M.A.; Scherberich, J. Evaluation of Mechanical Versus Manual Root Canal Preparation in Primary Molars—A Comparative In Vitro Study. J. Clin. Med. 2023, 12, 7718. https://doi.org/10.3390/jcm12247718
Schulz-Weidner N, Wang J, Steinbart J, Windfelder AG, Krombach GA, Krämer N, Schlenz MA, Scherberich J. Evaluation of Mechanical Versus Manual Root Canal Preparation in Primary Molars—A Comparative In Vitro Study. Journal of Clinical Medicine. 2023; 12(24):7718. https://doi.org/10.3390/jcm12247718
Chicago/Turabian StyleSchulz-Weidner, Nelly, Jiameng Wang, Jessica Steinbart, Anton G. Windfelder, Gabriele A. Krombach, Norbert Krämer, Maximiliane A. Schlenz, and Jan Scherberich. 2023. "Evaluation of Mechanical Versus Manual Root Canal Preparation in Primary Molars—A Comparative In Vitro Study" Journal of Clinical Medicine 12, no. 24: 7718. https://doi.org/10.3390/jcm12247718
APA StyleSchulz-Weidner, N., Wang, J., Steinbart, J., Windfelder, A. G., Krombach, G. A., Krämer, N., Schlenz, M. A., & Scherberich, J. (2023). Evaluation of Mechanical Versus Manual Root Canal Preparation in Primary Molars—A Comparative In Vitro Study. Journal of Clinical Medicine, 12(24), 7718. https://doi.org/10.3390/jcm12247718