
Combined Inositols, α-Lactalbumin, Gymnema Sylvestre and Zinc Improve the Lipid Metabolic Profile of Patients with Type 2 Diabetes Mellitus: A Randomized Clinical Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Study Outcomes
2.3. Statistical Analysis
3. Results
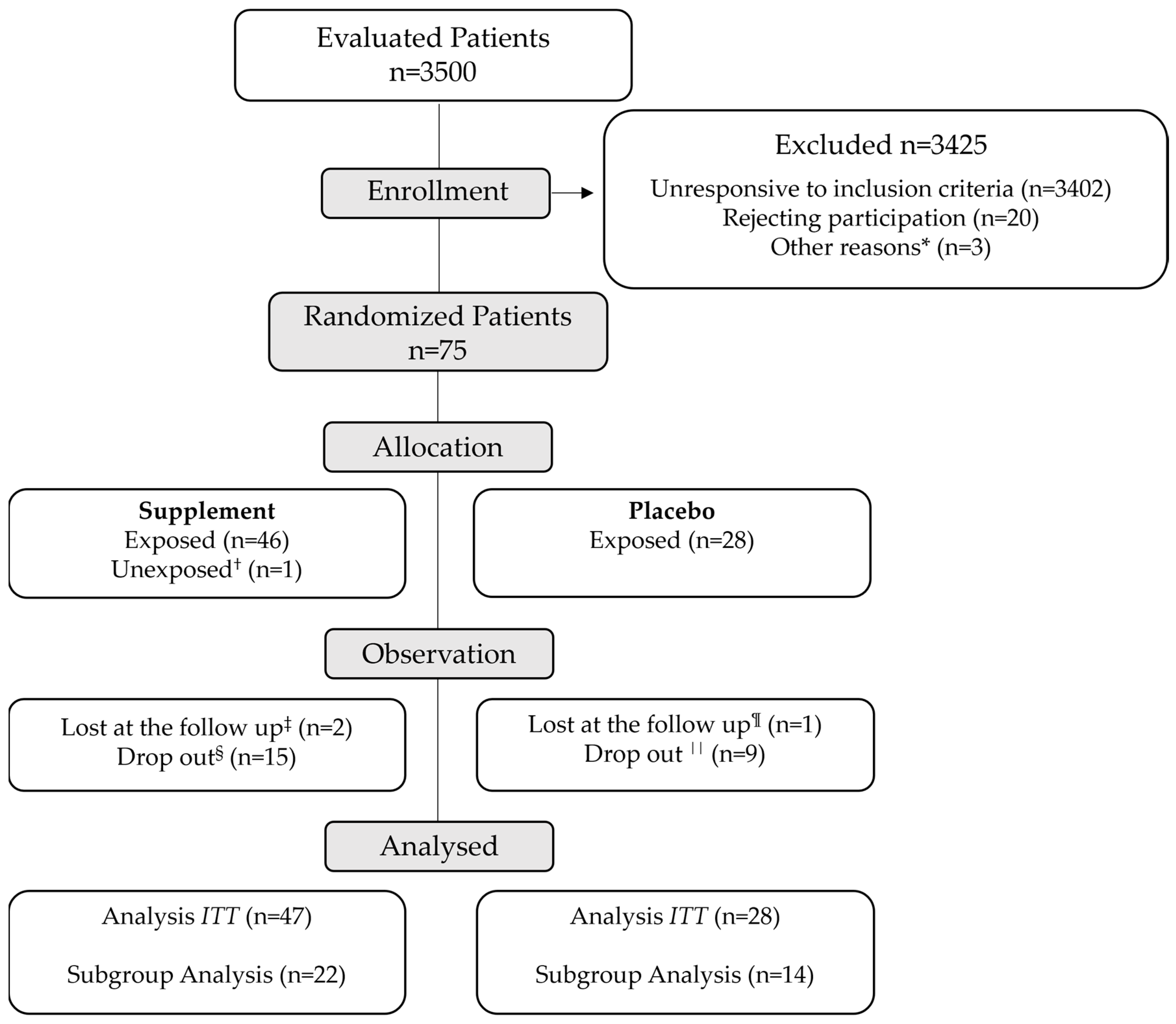
3.1. Patients, Follow-up and Futility Analysis
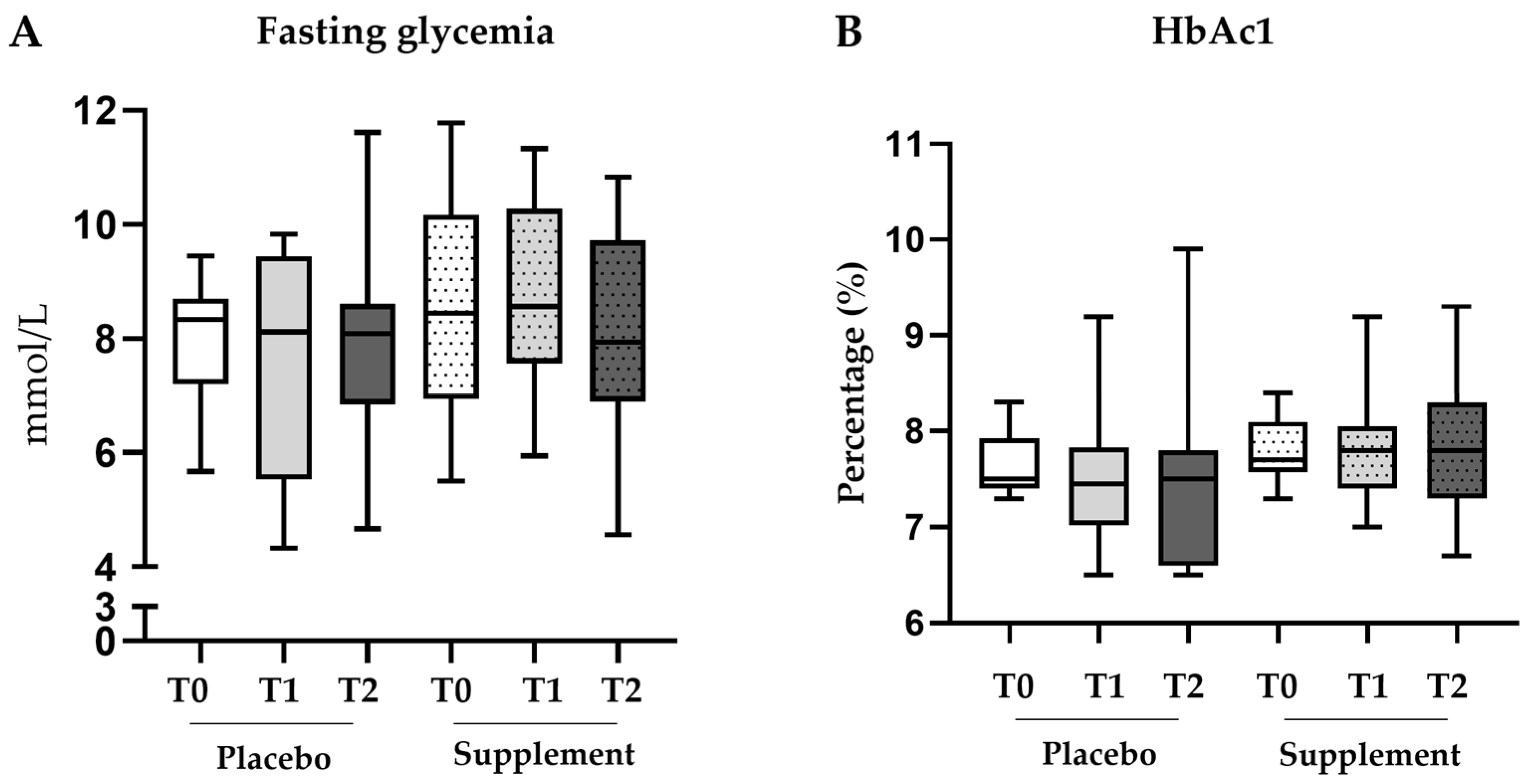
3.2. Glucose Metabolism
3.2.1. ITT Analysis
3.2.2. Subgroup Analysis
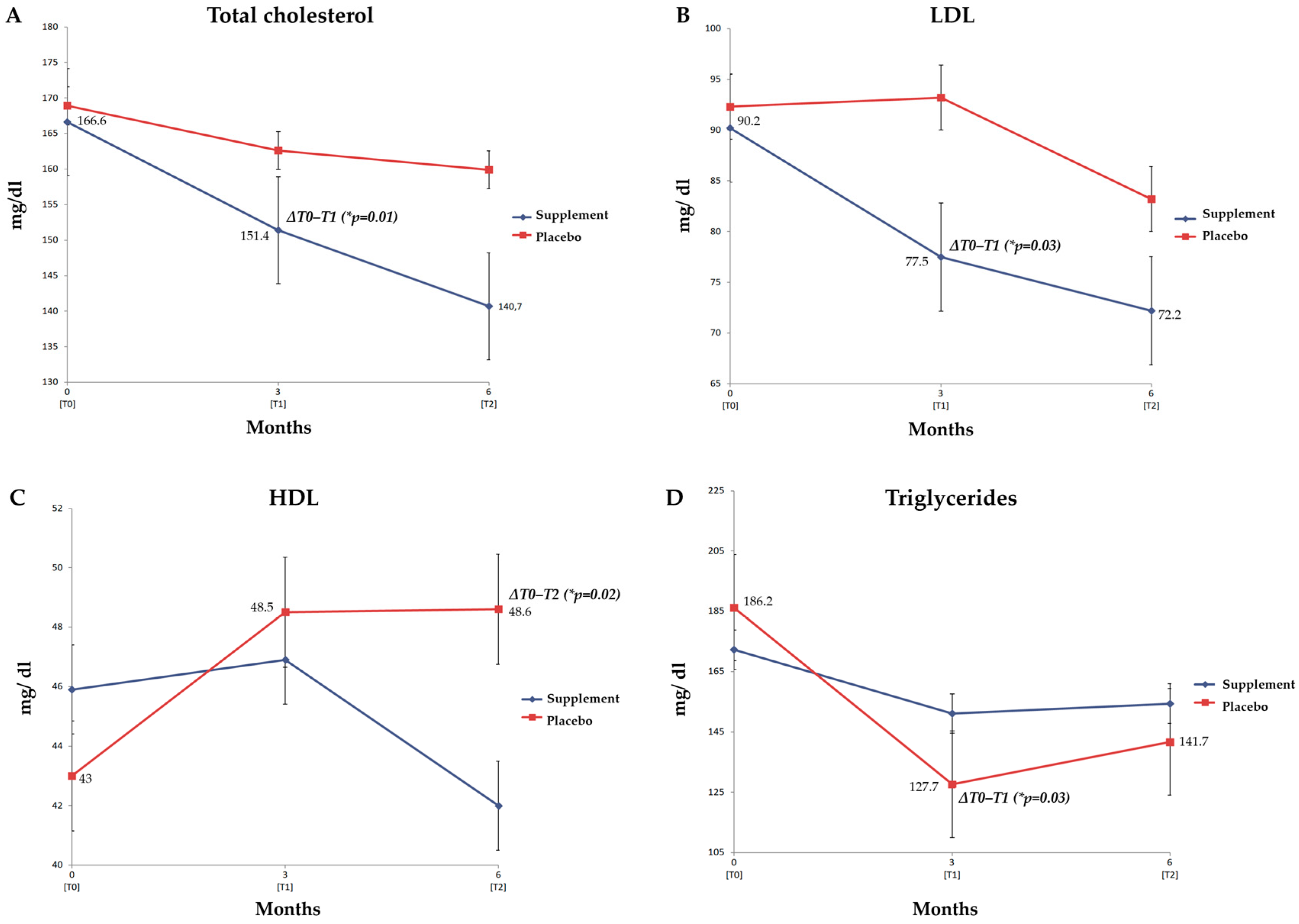
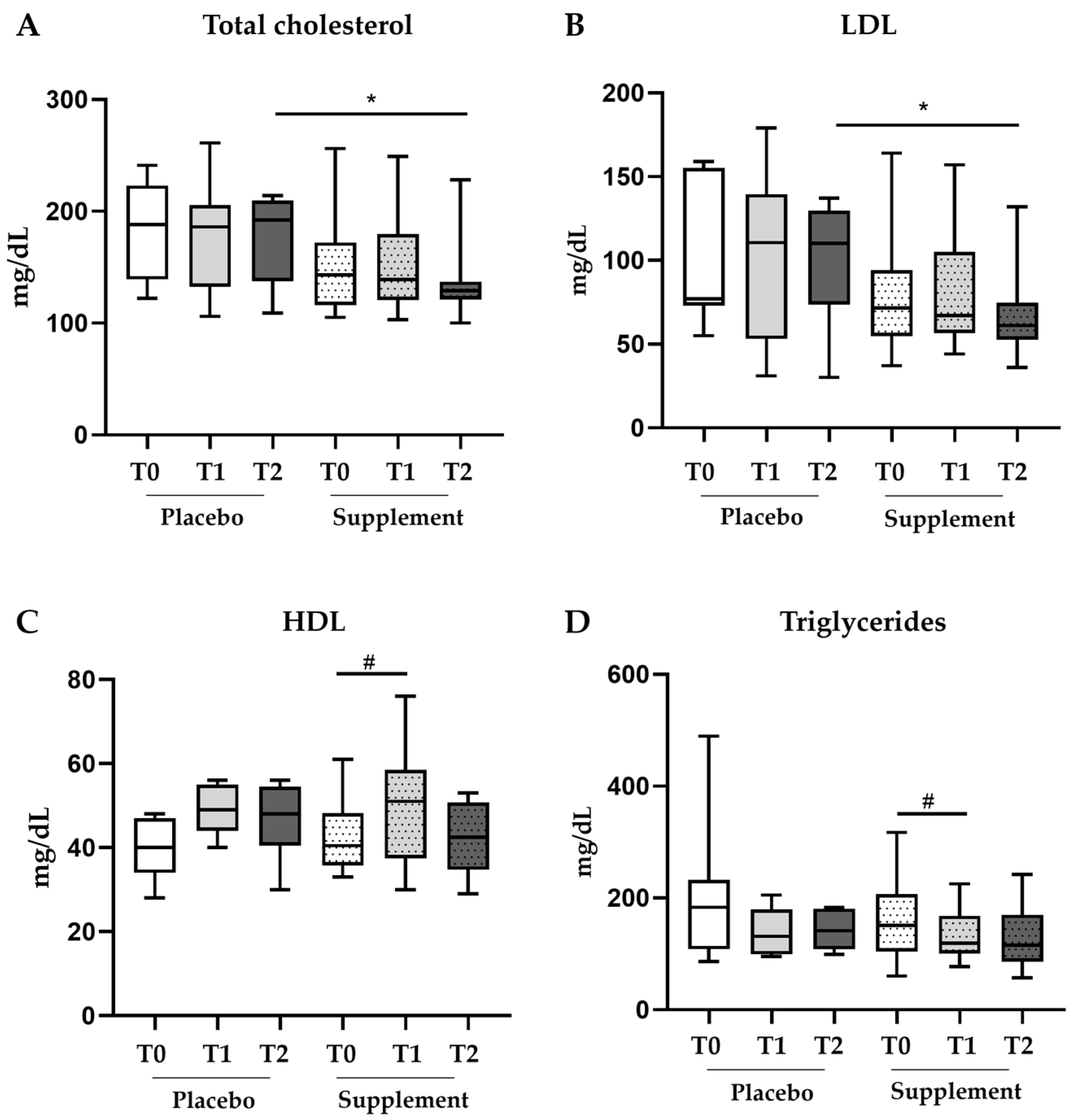
3.3. Lipid Metabolism and Body Weight
3.3.1. ITT Analysis
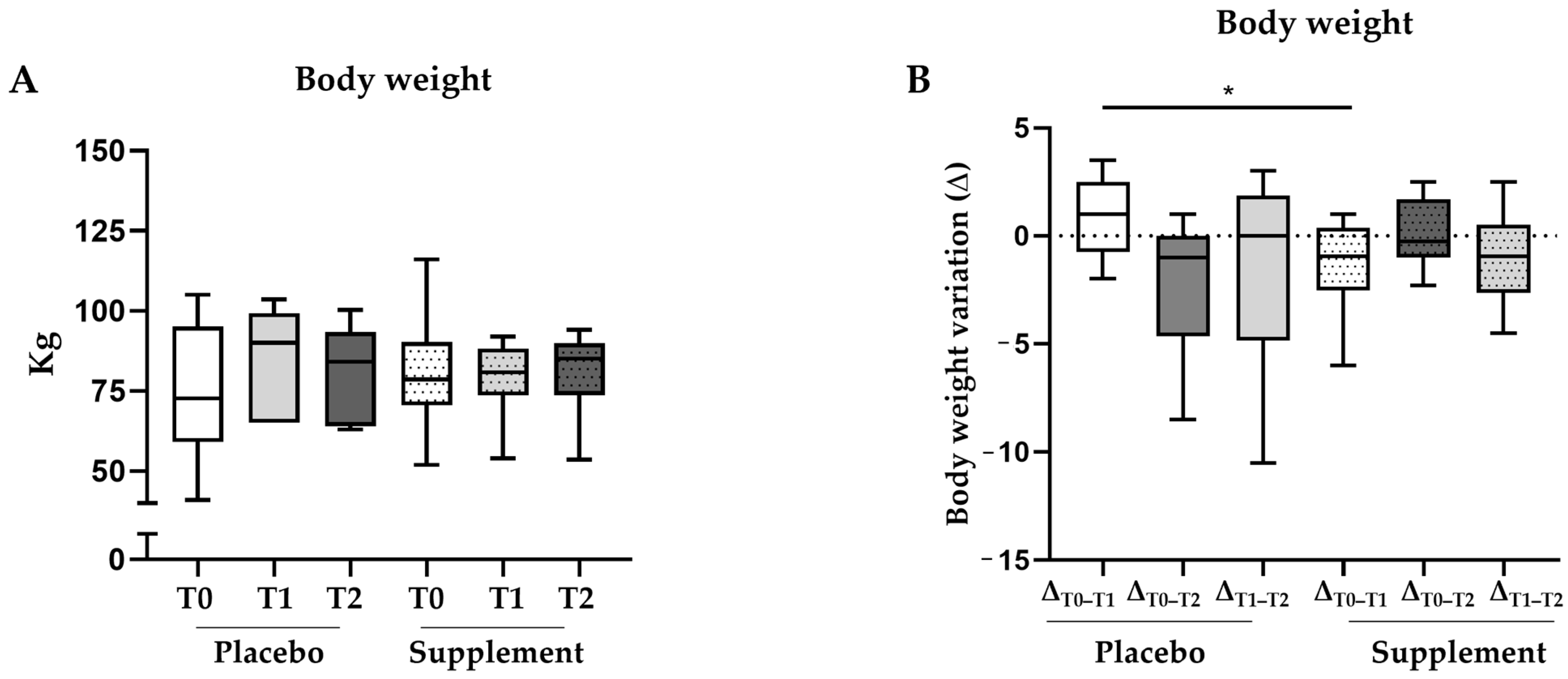
3.3.2. Subgroup Analysis
3.4. Safety Profile
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xu, G.; Liu, B.; Sun, Y.; Du, Y.; Snetselaar, L.G.; Hu, F.B.; Bao, W. Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: Population based study. BMJ 2018, 362, k1497. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Samuel, V.T.; Shulman, G.I. Mechanisms for insulin resistance: Common threads and missing links. Cell 2012, 148, 852–871. [Google Scholar] [CrossRef] [PubMed]
- Farmer, J.A. Diabetic dyslipidemia and atherosclerosis: Evidence from clinical trials. Curr. Diabetes Rep. 2008, 8, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraghavan, K. Treatment of dyslipidemia in patients with type 2 diabetes. Lipids Health Dis. 2010, 9, 144. [Google Scholar] [CrossRef] [PubMed]
- Vergès, B. Pathophysiology of diabetic dyslipidaemia: Where are we? Diabetologia 2015, 58, 886–899. [Google Scholar] [CrossRef] [PubMed]
- Turner, R.C.; Millns, H.; Neil, H.A.; Stratton, I.M.; Manley, S.E.; Matthews, D.R.; Holman, R.R. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23). BMJ 1998, 316, 823–828. [Google Scholar] [CrossRef]
- Taskinen, M.R.; Borén, J. New insights into the pathophysiology of dyslipidemia in type 2 diabetes. Atherosclerosis 2015, 239, 483–495. [Google Scholar] [CrossRef]
- Chapman, M.J.; Ginsberg, H.N.; Amarenco, P.; Andreotti, F.; Borén, J.; Catapano, A.L.; Descamps, O.S.; Fisher, E.; Kovanen, P.T.; Kuivenhoven, J.A.; et al. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: Evidence and guidance for management. Eur. Heart J. 2011, 32, 1345–1361. [Google Scholar] [CrossRef]
- Cook, M.N.; Girman, C.J.; Stein, P.P.; Alexander, C.M. Initial monotherapy with either metformin or sulphonylureas often fails to achieve or maintain current glycaemic goals in patients with Type 2 diabetes in UK primary care. Diabet. Med. 2007, 24, 350–358. [Google Scholar] [CrossRef]
- Tomic, D.; Shaw, J.E.; Magliano, D.J. The burden and risks of emerging complications of diabetes mellitus. Nat. Rev. Endocrinol. 2022, 18, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. Introduction: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S1–S2. [Google Scholar] [CrossRef] [PubMed]
- Dinicola, S.; Unfer, V.; Facchinetti, F.; Soulage, C.O.; Greene, N.D.; Bizzarri, M.; Laganà, A.S.; Chan, S.Y.; Bevilacqua, A.; Pkhaladze, L.; et al. Inositols: From Established Knowledge to Novel Approaches. Int. J. Mol. Sci. 2021, 22, 575. [Google Scholar] [CrossRef]
- Sun, T.H.; Heimark, D.B.; Nguygen, T.; Nadler, J.L.; Larner, J. Both myo-inositol to chiro-inositol epimerase activities and chiro-inositol to myo-inositol ratios are decreased in tissues of GK type 2 diabetic rats compared to Wistar controls. Biochem. Biophys. Res. Commun. 2002, 293, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, A.; Dragotto, J.; Giuliani, A.; Bizzarri, M. Myo-inositol and D-chiro-inositol (40:1) reverse histological and functional features of polycystic ovary syndrome in a mouse model. J. Cell Physiol. 2019, 234, 9387–9398. [Google Scholar] [CrossRef] [PubMed]
- Pintaudi, B.; Di Vieste, G.; Bonomo, M. The Effectiveness of Myo-Inositol and D-Chiro Inositol Treatment in Type 2 Diabetes. Int. J. Endocrinol. 2016, 2016, 9132052. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Garrido, M.A.; Tena-Sempere, M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Mol. Metab. 2020, 35, 100937. [Google Scholar] [CrossRef] [PubMed]
- Benelli, E.; Del Ghianda, S.; Di Cosmo, C.; Tonacchera, M. A Combined Therapy with Myo-Inositol and D-Chiro-Inositol Improves Endocrine Parameters and Insulin Resistance in PCOS Young Overweight Women. Int. J. Endocrinol. 2016, 2016, 3204083. [Google Scholar] [CrossRef]
- Minozzi, M.; Nordio, M.; Pajalich, R. The Combined therapy myo-inositol plus D-Chiro-inositol, in a physiological ratio, reduces the cardiovascular risk by improving the lipid profile in PCOS patients. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 537–540. [Google Scholar]
- Nordio, M.; Proietti, E. The combined therapy with myo-inositol and D-chiro-inositol reduces the risk of metabolic disease in PCOS overweight patients compared to myo-inositol supplementation alone. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 575–581. [Google Scholar]
- Zarezadeh, M.; Dehghani, A.; Faghfouri, A.H.; Radkhah, N.; Naemi Kermanshahi, M.; Hamedi Kalajahi, F.; Mohammadzadeh Honarvar, N.; Ghoreishi, Z.; Ostadrahimi, A.; Ebrahimi Mamaghani, M. Inositol supplementation and body mass index: A systematic review and meta-analysis of randomized clinical trials. Obes. Sci. Pract. 2022, 8, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, R.; Ostadmohammadi, V.; Lankarani, K.B.; Peymani, P.; Akbari, M.; Kolahdooz, F.; Asemi, Z. The effects of inositol supplementation on lipid profiles among patients with metabolic diseases: A systematic review and meta-analysis of randomized controlled trials. Lipids Health Dis. 2018, 17, 123. [Google Scholar] [CrossRef] [PubMed]
- Lepore, E.; Lauretta, R.; Bianchini, M.; Mormando, M.; Di Lorenzo, C.; Unfer, V. Inositols Depletion and Resistance: Principal Mechanisms and Therapeutic Strategies. Int. J. Mol. Sci. 2021, 22, 6796. [Google Scholar] [CrossRef]
- Monastra, G.; Sambuy, Y.; Ferruzza, S.; Ferrari, D.; Ranaldi, G. Alpha-lactalbumin Effect on Myo-inositol Intestinal Absorption: In vivo and In vitro. Curr. Drug Deliv. 2018, 15, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Ranaldi, G.; Ferruzza, S.; Natella, F.; Unfer, V.; Sambuy, Y.; Monastra, G. Enhancement of D-chiro-inositol transport across intestinal cells by alpha-Lactalbumin peptides. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 10143–10154. [Google Scholar] [CrossRef] [PubMed]
- Montanino Oliva, M.; Buonomo, G.; Calcagno, M.; Unfer, V. Effects of myo-inositol plus alpha-lactalbumin in myo-inositol-resistant PCOS women. J. Ovarian Res. 2018, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Kamenov, Z.; Gateva, A.; Dinicola, S.; Unfer, V. Comparing the Efficacy of Myo-Inositol Plus α-Lactalbumin vs. Myo-Inositol Alone on Reproductive and Metabolic Disturbances of Polycystic Ovary Syndrome. Metabolites 2023, 13, 717. [Google Scholar] [CrossRef]
- Boscaini, S.; Cabrera-Rubio, R.; Speakman, J.R.; Cotter, P.D.; Cryan, J.F.; Nilaweera, K.N. Dietary α-lactalbumin alters energy balance, gut microbiota composition and intestinal nutrient transporter expression in high-fat diet-fed mice. Br. J. Nutr. 2019, 121, 1097–1107. [Google Scholar] [CrossRef]
- Pothuraju, R.; Sharma, R.K.; Chagalamarri, J.; Jangra, S.; Kumar Kavadi, P. A systematic review of Gymnema sylvestre in obesity and diabetes management. J. Sci. Food Agric. 2014, 94, 834–840. [Google Scholar] [CrossRef]
- Khan, F.; Sarker, M.M.R.; Ming, L.C.; Mohamed, I.N.; Zhao, C.; Sheikh, B.Y.; Tsong, H.F.; Rashid, M.A. Comprehensive Review on Phytochemicals, Pharmacological and Clinical Potentials of Gymnema sylvestre. Front. Pharmacol. 2019, 10, 1223. [Google Scholar] [CrossRef]
- Zuñiga, L.Y.; González-Ortiz, M.; Martínez-Abundis, E. Effect of Gymnema sylvestre Administration on Metabolic Syndrome, Insulin Sensitivity, and Insulin Secretion. J. Med. Food 2017, 20, 750–754. [Google Scholar] [CrossRef]
- Kumar, V.; Bhandari, U.; Tripathi, C.D.; Khanna, G. Evaluation of antiobesity and cardioprotective effect of Gymnema sylvestre extract in murine model. Indian J. Pharmacol. 2012, 44, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Farooq, D.M.; Alamri, A.F.; Alwhahabi, B.K.; Metwally, A.M.; Kareem, K.A. The status of zinc in type 2 diabetic patients and its association with glycemic control. J. Fam. Community Med. 2020, 27, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Jayawardena, R.; Ranasinghe, P.; Galappatthy, P.; Malkanthi, R.; Constantine, G.; Katulanda, P. Effects of zinc supplementation on diabetes mellitus: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2012, 4, 13. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Wathurapatha, W.S.; Ishara, M.H.; Jayawardana, R.; Galappatthy, P.; Katulanda, P.; Constantine, G.R. Effects of Zinc supplementation on serum lipids: A systematic review and meta-analysis. Nutr. Metab. 2015, 12, 26. [Google Scholar] [CrossRef]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The Diabetes Mellitus-Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int. J. Mol. Sci. 2020, 21, 1835. [Google Scholar] [CrossRef]
- Parhofer, K.G. Interaction between Glucose and Lipid Metabolism: More than Diabetic Dyslipidemia. Diabetes Metab. J. 2015, 39, 353–362. [Google Scholar] [CrossRef]
- Jiang, K.; Luan, H.; Pu, X.; Wang, M.; Yin, J.; Gong, R. Association Between Visceral Adiposity Index and Insulin Resistance: A Cross-Sectional Study Based on US Adults. Front. Endocrinol. 2022, 13, 921067. [Google Scholar] [CrossRef]
- Basciani, S.; Nordio, M.; Dinicola, S.; Unfer, V.; Gnessi, L. Diet Plus Inositols, α-Lactalbumin and Gymnema sylvestre: The Successful Combo to Restore Body Weight and Metabolic Profile in Obese and Dysmetabolic Patients. Nutrients 2023, 15, 3142. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; O’Keefe, J.H. Myo-inositol for insulin resistance, metabolic syndrome, polycystic ovary syndrome and gestational diabetes. Open Heart 2022, 9, e001989. [Google Scholar] [CrossRef]
- Monastra, G.; Gambioli, R.; Unfer, V.; Forte, G.; Maymo-Masip, E.; Comitato, R. D-Chiro-Inositol and Myo-Inositol Induce WAT/BAT Trans-Differentiation in Two Different Human Adipocyte Models (SGBS and LiSa-2). Int. J. Mol. Sci. 2023, 24, 7421. [Google Scholar] [CrossRef]
- Gao, J.; Song, J.; Du, M.; Mao, X. Bovine α-Lactalbumin Hydrolysates (α-LAH) Ameliorate Adipose Insulin Resistance and Inflammation in High-Fat Diet-Fed C57BL/6J Mice. Nutrients 2018, 10, 242. [Google Scholar] [CrossRef]
- Devangan, S.; Varghese, B.; Johny, E.; Gurram, S.; Adela, R. The effect of Gymnema sylvestre supplementation on glycemic control in type 2 diabetes patients: A systematic review and meta-analysis. Phytother. Res. 2021, 35, 6802–6812. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, V.; Lepore, E.; Basciani, S.; Artale, S.; Nordio, M.; Bizzarri, M.; Unfer, V. Positive Effects of α-Lactalbumin in the Management of Symptoms of Polycystic Ovary Syndrome. Nutrients 2022, 14, 3220. [Google Scholar] [CrossRef]
- Tiwari, P.; Ahmad, K.; Baig, M.H. Gymnema sylvestre for Diabetes: From Traditional Herb to Future’s Therapeutic. Curr. Pharm. Des. 2017, 23, 1667–1676. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, N.; Asano, R.; Shimosaka, M.; Okazaki, M. Effect of administration with the extract of Gymnema sylvestre R. Br leaves on lipid metabolism in rats. Biol. Pharm. Bull. 2001, 24, 713–717. [Google Scholar] [CrossRef] [PubMed]
- DasNandy, A.; Patil, V.S.; Hegde, H.V.; Harish, D.R.; Roy, S. Elucidating type 2 diabetes mellitus risk factor by promoting lipid metabolism with gymnemagenin: An in vitro and in silico approach. Front. Pharmacol. 2022, 13, 1074342. [Google Scholar] [CrossRef]
- Sinha, S.; Sen, S. Status of zinc and magnesium levels in type 2 diabetes mellitus and its relationship with glycemic status. Int. J. Diabetes Dev. Ctries. 2014, 34, 220–223. [Google Scholar] [CrossRef]
- Olechnowicz, J.; Tinkov, A.; Skalny, A.; Suliburska, J. Zinc status is associated with inflammation, oxidative stress, lipid, and glucose metabolism. J. Physiol. Sci. 2018, 68, 19–31. [Google Scholar] [CrossRef]
- Costarelli, L.; Muti, E.; Malavolta, M.; Cipriano, C.; Giacconi, R.; Tesei, S.; Piacenza, F.; Pierpaoli, S.; Gasparini, N.; Faloia, E.; et al. Distinctive modulation of inflammatory and metabolic parameters in relation to zinc nutritional status in adult overweight/obese subjects. J. Nutr. Biochem. 2010, 21, 432–437. [Google Scholar] [CrossRef]
- Payahoo, L.; Ostadrahimi, A.; Mobasseri, M.; Khaje Bishak, Y.; Farrin, N.; Asghari Jafarabadi, M.; Mahluji, S. Effects of zinc supplementation on the anthropometric measurements, lipid profiles and fasting blood glucose in the healthy obese adults. Adv. Pharm. Bull. 2013, 3, 161–165. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Supplement (n = 47) | Placebo (n = 28) | p-Value |
|---|---|---|---|
| Age (years) | 67 [62–74] | 68.5 [62.3–76] | 0.9 |
| Gender (%) | |||
| Male | 70.2 | 71.4 | |
| Female | 29.8 | 28.6 | |
| Ethnicity (%) | |||
| Caucasian | 89.4 | 92.8 | |
| Other | 10.6 | 7.1 | |
| Body weight (kg) | 77.7 [70–90] | 89.5 [70.5–96.8] | 0.2 |
| BMI (kg/m2) | 28 [24.2–30.6] | 29.3 [25.2–32.9] | 0.2 |
| BMI classes (%) | 0.45 | ||
| <25 kg/m2 | 27.6 | 21.4 | |
| ≥25 ∧ <30 kg/m2 | 40.4 | 32.1 | |
| ≥30 kg/m2 | 31.9 | 46.4 | |
| Fasting glycemia (mmol/L) | 9.3 [7.3–10.2] | 8.6 [7.7–9.4] | 0.3 |
| HbA1c (%) | 7.7 [7.5–8.1] | 7.6 [7.4–8.3] | 0.7 |
| Total cholesterol (mg/dL) | 160 [128.5–201.5] | 170.5 [139.3–188.8] | 0.8 |
| HDL (mg/dL) | 44 [35–56] | 41.5 [33.3–49.5] | 0.4 |
| LDL (mg/dL) | 84 [57–122] | 90.5 [68.5–111] | 0.7 |
| Triglycerides (mg/dL) | 154 [98–206] | 156 [125.5–208.5] | 0.8 |
| Parameter | 3 Months (T1) | 6 Months (T2) | ||||
|---|---|---|---|---|---|---|
| Supplement (n = 46) | Placebo (n = 28) | p-Value | Supplement (n = 46) | Placebo (n = 28) | p-Value | |
| Body weight (kg) | 77.5 [72–85] | 87 [71.5–94.3] | 0.10 | 77.5 [72.9–87.9] | 84.5 [73.8–90] | 0.49 |
| Fasting glycemia (mmol/L) | 8.6 [7.5–10.1] | 8.8 [7–9.6] | 0.7 | 8.6 [7.1–9.7] | 8.3 [7.2–10] | 0.99 |
| HbA1c (%) | 7.8 [7.1–8] | 7.7 [7–8.2] | 0.66 | 7.8 [7.4–8.2] | 7.5 [6.6–8] | 0.15 |
| Total cholesterol (mg/dL) | 140 [119.8–165.8] | 149 [120.5–203.5] | 0.48 | 133 [111.5–168.5] | 154 [119–200] | 0.11 |
| HDL (mg/dL) | 48.5 [33.8–57.5] | 48.5 [40.8–56] | 0.54 | 40 [33.8–48.5] | 49 [41–54] | 0.09 |
| LDL (mg/dL) | 67.5 [55–89.3] | 83 [51.5–129.5] | 0.33 | 64 [45.5–92] | 87 [54–118] | 0.26 |
| Triglycerides (mg/dL) | 124 [101–174] | 108.5 [92–169] | 0.5 | 129 [98–171.3] | 127 [102.3–181.3] | 0.97 |
| Parameter | Supplement (n = 22) | Placebo (n = 14) | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Fasting glycemia (mmol/L) | 8.4 [6.9–10.2] | 8.6 [7.6–10.3] | 7.9 [6.9–9.8] | 8.3 [7.2–8.7] | 8.1 [5.5–9.4] | 8.1 [6.8–8.6] |
| HbA1c (%) | 7.7 [7.6–8.1] | 7.8 [7.4–8.1] | 7.8 [7.3–8.3] | 7.5 [7.4–7.9] | 7.45 [7.0–7.8] | 7.5 [6.6–7.8] |
| Parameter | Supplement (n = 22) | Placebo (n = 14) | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Total cholesterol (mg/dL) | 143 [116–172] | 139 [120.5–179.5] | 129 [121–137] | 188 [139–223] | 186 [132.5–205.5] | 192 [137.5–209.5] |
| LDL (mg/dL) | 71.5 [54.8–94.8] | 67 [56.5–105] | 61 [52.5–74.8] | 77 [73–155] | 110.5 [53–139.5] | 110 [73.5–129.5] |
| HDL (mg/dL) | 40.5 [35.8–48.3] | 51 [37.5–58.5] | 42.5 [34.8–50.8] | 40 [34–47] | 49 [44–55] | 48 [40.5–54.5] |
| Triglycerides (mg/dL) | 151 [104–206.5] | 119 [100.5–168] | 115 [86–169.5] | 183 [108–232] | 131 [99–179] | 141 [108–180.5] |
| Body weight (kg) | 78 [73.5–90] | 76.5 [73–86.5] | 80 [70.6–88.3] | 87 [64.1–99] | 90 [69–96.5] | 83.5 [71–96.5] |
| Body weight variation (Δ) | ΔT0–T1 −0.95 [−2.5–0.4] | ΔT0–T2 −0.3 [−1–1.7] | ΔT1–T2 −0.95 [−2.6–0.5] | ΔT0–T1 1 [−0.8–2.5] | ΔT0–T2 −1 [−4.7–0] | ΔT1–T2 0 [−4.9–1.9] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nani, A.; Bertuzzi, F.; Meneghini, E.; Mion, E.; Pintaudi, B. Combined Inositols, α-Lactalbumin, Gymnema Sylvestre and Zinc Improve the Lipid Metabolic Profile of Patients with Type 2 Diabetes Mellitus: A Randomized Clinical Trial. J. Clin. Med. 2023, 12, 7650. https://doi.org/10.3390/jcm12247650
Nani A, Bertuzzi F, Meneghini E, Mion E, Pintaudi B. Combined Inositols, α-Lactalbumin, Gymnema Sylvestre and Zinc Improve the Lipid Metabolic Profile of Patients with Type 2 Diabetes Mellitus: A Randomized Clinical Trial. Journal of Clinical Medicine. 2023; 12(24):7650. https://doi.org/10.3390/jcm12247650
Chicago/Turabian StyleNani, Alessandro, Federico Bertuzzi, Elena Meneghini, Elena Mion, and Basilio Pintaudi. 2023. "Combined Inositols, α-Lactalbumin, Gymnema Sylvestre and Zinc Improve the Lipid Metabolic Profile of Patients with Type 2 Diabetes Mellitus: A Randomized Clinical Trial" Journal of Clinical Medicine 12, no. 24: 7650. https://doi.org/10.3390/jcm12247650
APA StyleNani, A., Bertuzzi, F., Meneghini, E., Mion, E., & Pintaudi, B. (2023). Combined Inositols, α-Lactalbumin, Gymnema Sylvestre and Zinc Improve the Lipid Metabolic Profile of Patients with Type 2 Diabetes Mellitus: A Randomized Clinical Trial. Journal of Clinical Medicine, 12(24), 7650. https://doi.org/10.3390/jcm12247650