

Antithrombotic Management for Transcatheter Aortic Valve Implantation


Abstract
:1. Introduction
1.1. Background
1.2. Methods
2. Scientific Evidence
2.1. Premedication in TAVI
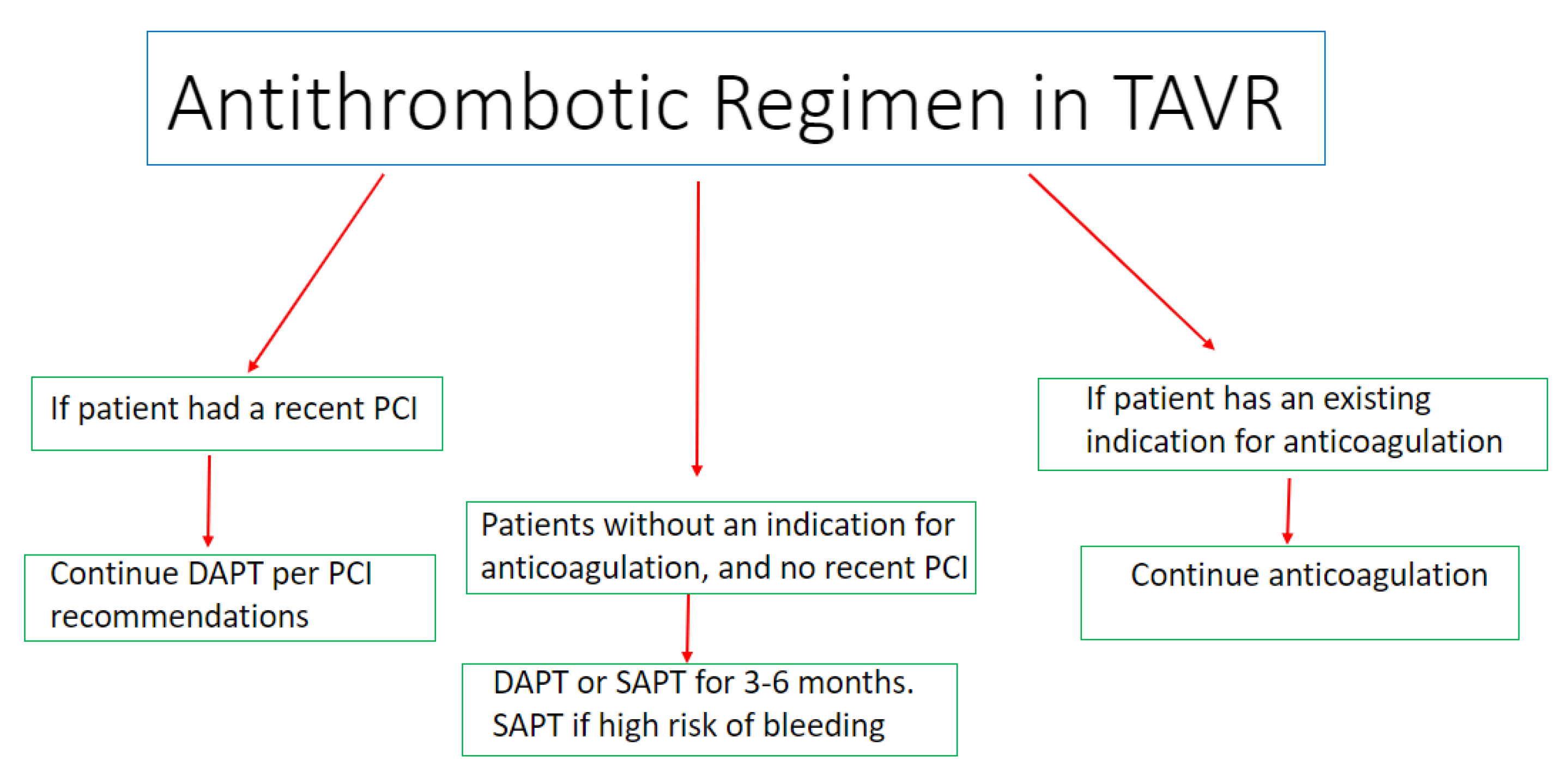
2.2. Antiplatelet Therapy in Patients without an Indication for Anticoagulation Post TAVI
2.3. Antiplatelet Therapy in Patients with an Indication for Anticoagulation Post TAVI
2.4. Anticoagulants versus Antiplatelets in Patients without an Indication for Anticoagulation
2.5. Pharmacodynamics and Antiplatelet Therapy in TAVI
3. Current Guidelines
4. Current Knowledge Gaps and Future Directions
5. Conclusions
Funding
Conflicts of Interest
References
- Hioki, H.; Watanabe, Y.; Kozuma, K.; Nara, Y.; Kawashima, H.; Kataoka, A.; Yamamoto, M.; Takagi, K.; Araki, M.; Tada, N.; et al. Pre-procedural dual antiplatelet therapy in patients undergoing transcatheter aortic valve implantation increases risk of bleeding. Heart 2017, 103, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Nijenhuis, V.J.; Ten Berg, J.M.; Hengstenberg, C.; Lefèvre, T.; Windecker, S.; Hildick-Smith, D.; Kupatt, C.; Van Belle, E.; Tron, C.; Hink, H.U.; et al. Usefulness of Clopidogrel Loading in Patients Who Underwent Transcatheter Aortic Valve Implantation (from the BRAVO-3 Randomized Trial). Am. J. Cardiol. 2019, 123, 1494–1500. [Google Scholar] [CrossRef] [PubMed]
- Ussia, G.P.; Scarabelli, M.; Mulè, M.; Barbanti, M.; Sarkar, K.; Cammalleri, V.; Immè, S.; Aruta, P.; Pistritto, A.M.; Gulino, S.; et al. Dual antiplatelet therapy versus aspirin alone in patients undergoing transcatheter aortic valve implantation. Am. J. Cardiol. 2011, 108, 1772–1776. [Google Scholar] [CrossRef] [PubMed]
- Stabile, E.; Pucciarelli, A.; Cota, L.; Sorropago, G.; Tesorio, T.; Salemme, L.; Popusoi, G.; Ambrosini, V.; Cioppa, A.; Agrusta, M.; et al. SAT-TAVI (Single Antiplatelet Therapy for TAVI) study: A pilot randomized study comparing double to single antiplatelet therapy for transcatheter aortic valve implantation. Int. J. Cardiol. 2014, 174, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Rodés-Cabau, J.; Masson, J.B.; Welsh, R.C.; Garcia Del Blanco, B.; Pelletier, M.; Webb, J.G.; Al-Qoofi, F.; Généreux, P.; Maluenda, G.; Thoenes, M.; et al. Aspirin versus Aspirin Plus Clopidogrel as Antithrombotic Treatment Following Transcatheter Aortic Valve Replacement with a Balloon-Expandable Valve: The ARTE (Aspirin versus Aspirin + Clopidogrel Following Transcatheter Aortic Valve Implantation) randomized clinical trial. JACC Cardiovasc. Interv. 2017, 10, 1357–1365. [Google Scholar] [PubMed]
- Brouwer, J.; Nijenhuis, V.J.; Delewi, R.; Hermanides, R.S.; Holvoet, W.; Dubois, C.L.F.; Frambach, P.; De Bruyne, B.; van Houwelingen, G.K.; Van Der Heyden, J.A.S.; et al. Aspirin with or without clopidogrel after transcatheter aortic-valve implantation. N. Engl. J. Med. 2020, 383, 1447–1457. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, J.; Nijenhuis, V.J.; Rodés-Cabau, J.; Stabile, E.; Barbanti, M.; Costa, G.; Mahmoodi, B.K.; Ten Berg, J.M. Aspirin Alone Versus Dual Antiplatelet Therapy After Transcatheter Aortic Valve Implantation: A Systematic Review and Patient-Level Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e019604. [Google Scholar] [CrossRef] [PubMed]
- Nijenhuis, V.J.; Brouwer, J.; Delewi, R.; Hermanides, R.S.; Holvoet, W.; Dubois, C.L.F.; Frambach, P.; De Bruyne, B.; van Houwelingen, G.K.; Van Der Heyden, J.A.S.; et al. Anticoagulation with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N. Engl. J. Med. 2020, 382, 1696–1707. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; Unverdorben, M.; Hengstenberg, C.; Möllmann, H.; Mehran, R.; López-Otero, D.; Nombela-Franco, L.; Moreno, R.; Nordbeck, P.; Thiele, H.; et al. Edoxaban versus Vitamin K Antagonist for Atrial Fibrillation after TAVR. N. Engl. J. Med. 2021, 385, 2150–2160. [Google Scholar] [CrossRef]
- Dangas, G.D.; Tijssen, J.G.P.; Wöhrle, J.; Søndergaard, L.; Gilard, M.; Möllmann, H.; Makkar, R.R.; Herrmann, H.C.; Giustino, G.; Baldus, S.; et al. A controlled trial of rivaroxaban after transcatheter aortic-valve replacement. N. Engl. J. Med. 2020, 382, 120–129. [Google Scholar] [CrossRef]
- De Backer, O.; Dangas, G.D.; Jilaihawi, H.; Leipsic, J.A.; Terkelsen, C.J.; Makkar, R.; Kini, A.S.; Veien, K.T.; Abdel-Wahab, M.; Kim, W.K.; et al. Reduced Leaflet Motion after Transcatheter Aortic-Valve Replacement. N. Engl. J. Med. 2020, 382, 130–139. [Google Scholar] [CrossRef]
- Collet, J.P.; Van Belle, E.; Thiele, H.; Berti, S.; Lhermusier, T.; Manigold, T.; Neumann, F.J.; Gilard, M.; Attias, D.; Beygui, F.; et al. Apixaban vs. standard of care after transcatheter aortic valve implantation: The ATLANTIS trial. Eur. Heart J. 2022, 43, 2783–2797. [Google Scholar] [CrossRef] [PubMed]
- Overtchouk, P.; Guedeney, P.; Rouanet, S.; Verhoye, J.P.; Lefevre, T.; Van Belle, E.; Eltchaninoff, H.; Gilard, M.; Leprince, P.; Iung, B.; et al. Long-term mortality and early valve dysfunction according to anticoagulation use: The FRANCE TAVI Registry. J. Am. Coll. Cardiol. 2019, 73, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Park, D.W.; Ahn, J.M.; Kang, D.Y.; Kim, K.W.; Koo, H.J.; Yang, D.H.; Jung, S.C.; Kim, B.; Wong, Y.T.A.; Lam, C.C.S.; et al. Edoxaban Versus Dual Antiplatelet Therapy for Leaflet Thrombosis and Cerebral Thromboembolism After TAVR: The ADAPT-TAVR Randomized Clinical Trial. Circulation 2022, 146, 466–479. [Google Scholar] [CrossRef] [PubMed]
- Elbadawi, A.; Dang, A.T.; Sedhom, R.; Hamed, M.; Eid, M.; Golwala, H.; Goel, S.S.; Mamas, M.A.; Elgendy, I.Y. Direct Oral Anticoagulants versus Antiplatelet Therapy After Transcatheter Aortic Valve Replacement: A Meta-Analysis of Randomized Trials. Circ. Cardiovasc. Interv. 2022, 15, e012194. [Google Scholar] [CrossRef] [PubMed]
- Jimenez Diaz, V.A.; Tello-Montoliu, A.; Moreno, R.; Cruz Gonzalez, I.; Baz Alonso, J.A.; Romaguera, R.; Molina Navarro, E.; Juan Salvadores, P.; Paredes Galan, E.; De Miguel Castro, A.; et al. Assessment of Platelet REACtivity after Transcatheter Aortic Valve Replacement: The REAC-TAVI Trial. JACC Cardiovasc. Interv. 2019, 12, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P.; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C.; et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: Executive summary: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef]
- Ten Berg, J.; Sibbing, D.; Rocca, B.; Van Belle, E.; Chevalier, B.; Collet, J.P.; Dudek, D.; Gilard, M.; Gorog, D.A.; Grapsa, J.; et al. Management of antithrombotic therapy in patients undergoing transcatheter aortic valve implantation: A consensus document of the ESC Working Group on Thrombosis and the European Association of Percutaneous Cardiovascular Interventions (EAPCI), in collaboration with the ESC Council on Valvular Heart Disease. Eur. Heart J. 2021, 42, 2265–2269. [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the Management of Valvular Heart Disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef]
- Chakravarty, T.; Søndergaard, L.; Friedman, J.; De Backer, O.; Berman, D.; Kofoed, K.F.; Jilaihawi, H.; Shiota, T.; Abramowitz, Y.; Jørgensen, T.H.; et al. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: An observational study. Lancet 2017, 389, 2383–2392. [Google Scholar] [CrossRef]
- Midha, P.A.; Raghav, V.; Sharma, R.; Condado, J.F.; Okafor, I.U.; Rami, T.; Kumar, G.; Thourani, V.H.; Jilaihawi, H.; Babaliaros, V.; et al. The Fluid Mechanics of Transcatheter Heart Valve Leaflet Thrombosis in the Neosinus. Circulation 2017, 136, 1598–1609. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.; Simonato, M.; Latib, A.; Goleski, P.J.; Allali, A.; Kaur, J.; Azadani, A.N.; Horlick, E.; Testa, L.; Orvin, K.; et al. Clinical Valve Thrombosis after Transcatheter Aortic Valve-in-Valve Implantation. Circ. Cardiovasc. Interv. 2018, 11, e006730. [Google Scholar] [CrossRef]
- Milojevic, M.; Nikolic, A.; Micovic, S.; Jeppsson, A. Oral anticoagulation following bioprosthetic SAVR in patients with atrial fibrillation: What’s the current status of NOACs? Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac112. [Google Scholar] [CrossRef]
- Siddiqi, T.J.; Usman, M.S.; Shahid, I.; Ahmed, J.; Khan, S.U.; Ya’qoub, L.; Rihal, C.S.; Alkhouli, M. Utility of the CHA2DS2-VASc score for predicting ischaemic stroke in patients with or without atrial fibrillation: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2022, 29, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Dvir, D.; Généreux, P.; Barbash, I.M.; Kodali, S.; Ben-Dor, I.; Williams, M.; Torguson, R.; Kirtane, A.J.; Minha, S.; Badr, S.; et al. Acquired thrombocytopenia after transcatheter aortic valve replacement: Clinical correlates and association with outcomes. Eur. Heart J. 2014, 35, 2663–2671. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study, Year | Number of Patients | Antithrombotic Regimen | Major Findings |
|---|---|---|---|
| POPULAR-TAVI, cohort A, 2020 [6] | 665 | Aspirin 80–100 mg daily versus 3 months of DAPT with aspirin 80–100 mg daily + clopidogrel 75 mg daily | Aspirin monotherapy was associated with lower bleeding (15.1% vs. 26.6%; p = 0.001) and non–procedure-related bleeding (15.1% vs. 24.9%; p = 0.005) than DAPT; There was no difference in ischemic event rates and valve function between the groups |
| POPULAR-TAVI, cohort B, 2020 [7] | 313 | Oral anticoagulation alone versus oral anticoagulation with clopidogrel 75 mg daily for 3 months | Bleeding occurred in 21.7% receiving oral anticoagulation alone and in 34.6% receiving oral anticoagulation plus clopidogrel (p = 0.01); There was no difference in the ischemic events, including cardiovascular death, stroke and myocardial infarction, between the groups |
| ENVISAGE-TAVI AF trial, 2021 [8] | 1426 | Edoxaban versus vitamin K antagonist | No difference in the rates of death or stroke between the two groups, with evidence of higher gastrointestinal bleeding in the Edoxaban group |
| GALILEO, 2020 [9] | 1644 | Rivaroxaban 10 mg daily (with aspirin 75–100 mg daily for 3 months) versus aspirin 75–100 mg daily (with clopidogrel 75 mg daily for 3 months) | Rivaroxaban 10 mg/d (plus aspirin for the first 3 months) was associated with a higher risk of thromboembolic complications and death compared with DAPT |
| ATLANTIS trial, 2022 [10] | 1510 | Full dose apixaban versus vitamin K antagonist or antiplatelet therapy | Full dose apixaban was not superior to standard-of-care therapy, whether it was a vitamin K antagonist or antiplatelet therapy |
| ADAPT-TAVR, 2022 [13] | 229 | Edoxaban versus DAPT | There was a trend toward a lower incidence of leaflet thrombosis in the Edoxaban group compared with the dual antiplatelet therapy (9.8% vs. 18.4%; p = 0.076). No difference in new cerebral thromboembolism and neurological or neurocognitive function between the groups |
| Guidelines | Recommendation | Class of Recommendation | Level of Evidence |
|---|---|---|---|
| 2021 ACC/AHA | DAPT with aspirin 75–100 mg daily and clopidogrel 75 mg daily may be reasonable for 3–6 months after valve implantation in patients at a low risk of bleeding [17] | IIB | B-NR |
| SAPT with aspirin 75–100 mg daily as a reasonable option in patients undergoing TAVI in the absence of other indications for oral anticoagulation [17] | IIA | B-NR | |
| Novel oral anticoagulation as an effective alternative to vitamin K antagonist for patients with an elevated CHA2DS2-VASc score and atrial fibrillation who received a bioprosthetic valve [17] | I | A | |
| Vitamin K antagonists to achieve an INR of 2.5 may be reasonable for at least 3 months in patients with low risk of bleeding [17] | IIB | B-NR | |
| Low-dose rivaroxaban (10 mg daily) plus ASA (75–100 mg daily) is contraindicated in the absence of other indications for oral anticoagulation | III | B-NR | |
| 2021 ESC/EACTS | Lifelong SAPT (aspirin 75–100 mg daily or clopidogrel 75 mg daily) after TAVI in patients with no baseline indication for oral anticoagulation | I | A |
| Oral anticoagulation lifelong for TAVI in patients who have other indications for oral anticoagulation | I | B | |
| Routine use of oral anticoagulation is not recommended in patients with no baseline indication for OAC | III | B |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ya’Qoub, L.; Arnautovic, J.; Sharkawi, M.; AlAasnag, M.; Jneid, H.; Elgendy, I.Y. Antithrombotic Management for Transcatheter Aortic Valve Implantation. J. Clin. Med. 2023, 12, 7632. https://doi.org/10.3390/jcm12247632
Ya’Qoub L, Arnautovic J, Sharkawi M, AlAasnag M, Jneid H, Elgendy IY. Antithrombotic Management for Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine. 2023; 12(24):7632. https://doi.org/10.3390/jcm12247632
Chicago/Turabian StyleYa’Qoub, Lina, Jelena Arnautovic, Musa Sharkawi, Mirvat AlAasnag, Hani Jneid, and Islam Y. Elgendy. 2023. "Antithrombotic Management for Transcatheter Aortic Valve Implantation" Journal of Clinical Medicine 12, no. 24: 7632. https://doi.org/10.3390/jcm12247632
APA StyleYa’Qoub, L., Arnautovic, J., Sharkawi, M., AlAasnag, M., Jneid, H., & Elgendy, I. Y. (2023). Antithrombotic Management for Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine, 12(24), 7632. https://doi.org/10.3390/jcm12247632