

Endocarditis after Transcatheter Aortic Valve Replacement

Abstract
:
1. Introduction
2. Epidemiology
3. Risk Factors
3.1. Patient-Related Risk Factors
3.2. Procedure-Related Risk Factors
4. Microbiology
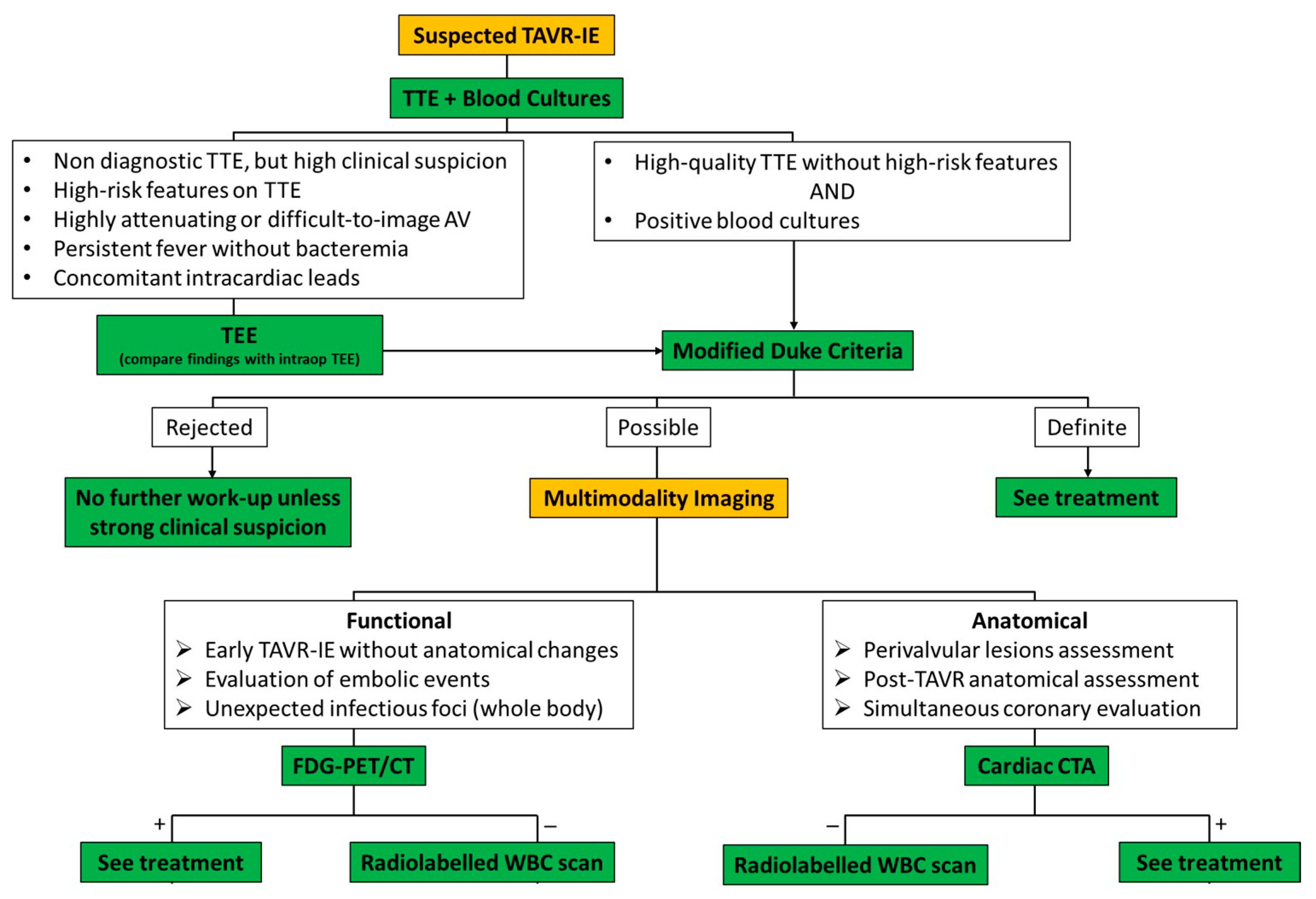
5. Presentations and Diagnosis
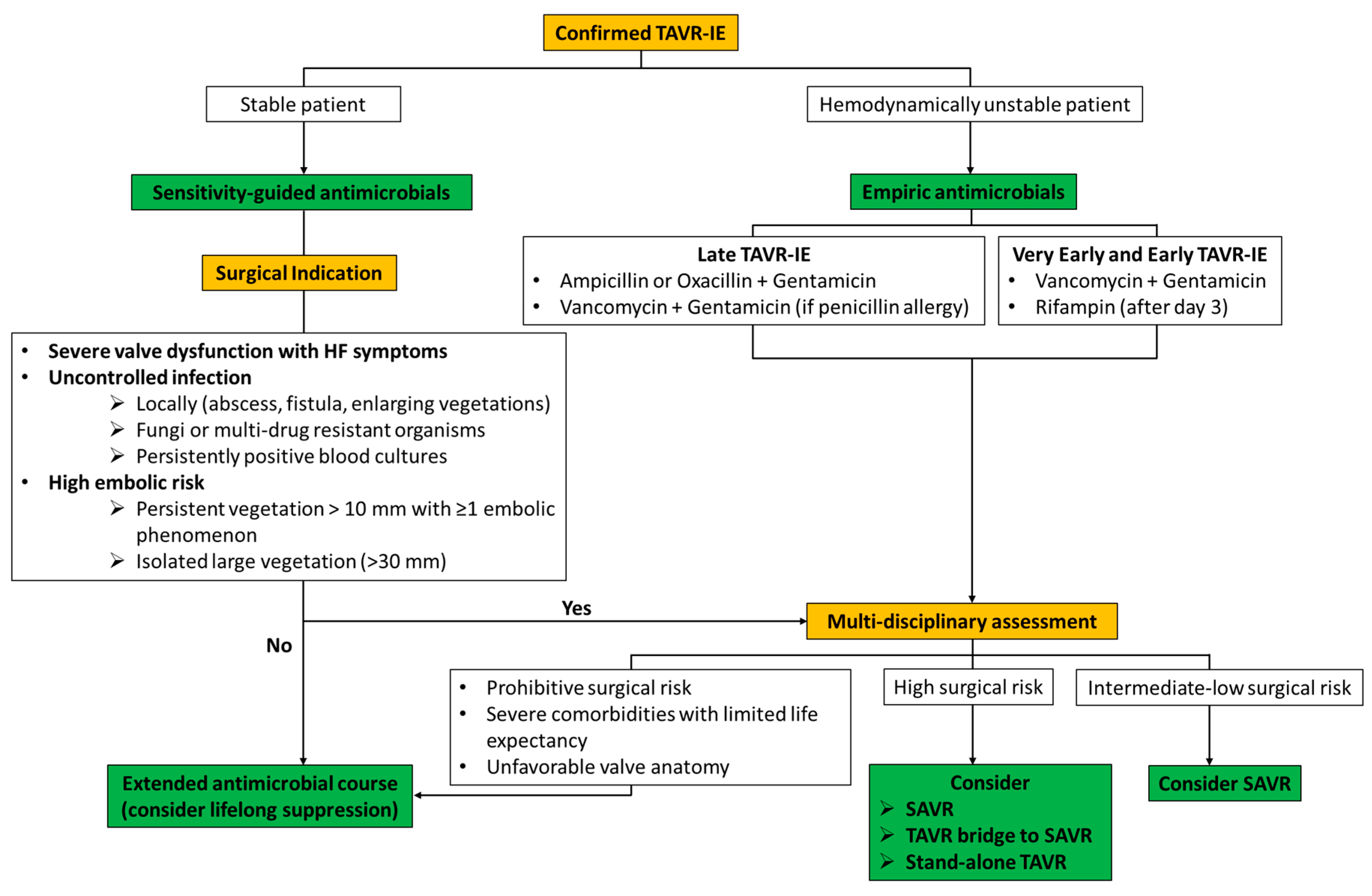
6. Management and Outcomes
7. Prevention
8. Future Perspectives
9. Gaps in Evidence
10. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Coffey, S.; Cairns, B.J.; Iung, B. The modern epidemiology of heart valve disease. Heart 2016, 102, 75–85. [Google Scholar] [CrossRef]
- Makkar, R.R.; Fontana, G.P.; Jilaihawi, H.; Kapadia, S.; Pichard, A.D.; Douglas, P.S.; Thourani, V.H.; Babaliaros, V.C.; Webb, J.G.; Herrmann, H.C.; et al. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N. Engl. J. Med. 2012, 366, 1696–1704. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef]
- Reardon, M.J.; Van Mieghem, N.M.; Popma, J.J.; Kleiman, N.S.; Sondergaard, L.; Mumtaz, M.; Adams, D.H.; Deeb, G.M.; Maini, B.; Gada, H.; et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2017, 376, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Mentias, A.; Saad, M.; Desai, M.Y.; Krishnaswamy, A.; Menon, V.; Horwitz, P.A.; Kapadia, S.; Sarrazin, M.V. Transcatheter Versus Surgical Aortic Valve Replacement in Patients with Rheumatic Aortic Stenosis. J. Am. Coll. Cardiol. 2021, 77, 1703–1713. [Google Scholar] [CrossRef]
- Mentias, A.; Saad, M.; Menon, V.; Reed, G.W.; Popovic, Z.; Johnston, D.; Rodriguez, L.; Gillinov, M.; Griffin, B.; Jneid, H.; et al. Transcatheter vs Surgical Aortic Valve Replacement in Pure Native Aortic Regurgitation. Ann. Thorac. Surg. 2023, 115, 870–876. [Google Scholar] [CrossRef]
- Summers, M.R.; Leon, M.B.; Smith, C.R.; Kodali, S.K.; Thourani, V.H.; Herrmann, H.C.; Makkar, R.R.; Pibarot, P.; Webb, J.G.; Leipsic, J.; et al. Prosthetic Valve Endocarditis After TAVR and SAVR: Insights from the PARTNER Trials. Circulation 2019, 140, 1984–1994. [Google Scholar] [CrossRef]
- Mentias, A.; Girotra, S.; Desai, M.Y.; Horwitz, P.A.; Rossen, J.D.; Saad, M.; Panaich, S.; Kapadia, S.; Sarrazin, M.V. Incidence, Predictors, and Outcomes of Endocarditis After Transcatheter Aortic Valve Replacement in the United States. JACC Cardiovasc. Interv. 2020, 13, 1973–1982. [Google Scholar] [CrossRef]
- Regueiro, A.; Linke, A.; Latib, A.; Ihlemann, N.; Urena, M.; Walther, T.; Husser, O.; Herrmann, H.C.; Nombela-Franco, L.; Cheema, A.N.; et al. Association Between Transcatheter Aortic Valve Replacement and Subsequent Infective Endocarditis and In-Hospital Death. JAMA 2016, 316, 1083–1092. [Google Scholar] [CrossRef]
- Kolte, D.; Goldsweig, A.; Kennedy, K.F.; Abbott, J.D.; Gordon, P.C.; Sellke, F.W.; Ehsan, A.; Sodha, N.; Sharaf, B.L.; Aronow, H.D. Comparison of Incidence, Predictors, and Outcomes of Early Infective Endocarditis after Transcatheter Aortic Valve Implantation Versus Surgical Aortic Valve Replacement in the United States. Am. J. Cardiol. 2018, 122, 2112–2119. [Google Scholar] [CrossRef] [PubMed]
- Fauchier, L.; Bisson, A.; Herbert, J.; Lacour, T.; Bourguignon, T.; Etienne, C.S.; Bernard, A.; Deharo, P.; Bernard, L.; Babuty, D. Incidence and outcomes of infective endocarditis after transcatheter aortic valve implantation versus surgical aortic valve replacement. Clin. Microbiol. Infect. 2020, 26, 1368–1374. [Google Scholar] [CrossRef]
- Medranda, G.A.; Rogers, T.; Ali, S.W.; Zhang, C.; Shea, C.; Sciandra, K.A.; Case, B.C.; Forrestal, B.J.; Sutton, J.A.; McFadden, E.P.; et al. Prosthetic valve endocarditis after transcatheter aortic valve replacement in low-risk patients. Catheter. Cardiovasc. Interv. 2022, 99, 896–903. [Google Scholar] [CrossRef]
- Durko, A.P.; Osnabrugge, R.L.; Van Mieghem, N.M.; Milojevic, M.; Mylotte, D.; Nkomo, V.T.; Pieter Kappetein, A. Annual number of candidates for transcatheter aortic valve implantation per country: Current estimates and future projections. Eur. Heart J. 2018, 39, 2635–2642. [Google Scholar] [CrossRef]
- Del Val, D.; Abdel-Wahab, M.; Linke, A.; Durand, E.; Ihlemann, N.; Urena, M.; Pellegrini, C.; Giannini, F.; Landt, M.; Auffret, V.; et al. Temporal Trends, Characteristics, and Outcomes of Infective Endocarditis After Transcatheter Aortic Valve Replacement. Clin. Infect. Dis. 2021, 73, e3750–e3758. [Google Scholar] [CrossRef] [PubMed]
- Stortecky, S.; Heg, D.; Tueller, D.; Pilgrim, T.; Muller, O.; Noble, S.; Jeger, R.; Toggweiler, S.; Ferrari, E.; Taramasso, M.; et al. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2020, 75, 3020–3030. [Google Scholar] [CrossRef] [PubMed]
- Mangner, N.; Woitek, F.; Haussig, S.; Schlotter, F.; Stachel, G.; Hollriegel, R.; Wilde, J.; Lindner, A.; Holzhey, D.; Leontyev, S.; et al. Incidence, Predictors, and Outcome of Patients Developing Infective Endocarditis Following Transfemoral Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2016, 67, 2907–2908. [Google Scholar] [CrossRef]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miro, J.M.; Fowler, V.G.; Jr Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef]
- Alexis, S.L.; Malik, A.H.; George, I.; Hahn, R.T.; Khalique, O.K.; Seetharam, K.; Bhatt, D.L.; Tang, G.H.L. Infective Endocarditis After Surgical and Transcatheter Aortic Valve Replacement: A State of the Art Review. J. Am. Heart Assoc. 2020, 9, e017347. [Google Scholar] [CrossRef]
- Regueiro, A.; Linke, A.; Latib, A.; Rodés-Cabau, J.; Anguita, M.; de la Figuera, M.; Cabeza, A.I.P.; Fernández, C.S.; Munoz-Garcia, E.; Munoz-Garcia, M. Infective Endocarditis Following Transcatheter Aortic Valve Replacement: Comparison of Balloon- Versus Self-Expandable Valves. Circ. Cardiovasc. Interv. 2019, 12, e007938. [Google Scholar] [CrossRef] [PubMed]
- Amat-Santos, I.J.; Messika-Zeitoun, D.; Eltchaninoff, H.; Kapadia, S.; Lerakis, S.; Cheema, A.N.; Gutierrez-Ibanes, E.; Munoz-Garcia, A.J.; Pan, M.; Webb, J.G.; et al. Infective endocarditis after transcatheter aortic valve implantation: Results from a large multicenter registry. Circulation 2015, 131, 1566–1574. [Google Scholar] [CrossRef]
- Prasitlumkum, N.; Vutthikraivit, W.; Thangjui, S.; Leesutipornchai, T.; Kewcharoen, J.; Riangwiwat, T.; Dworkin, J. Epidemiology of infective endocarditis in transcatheter aortic valve replacement: Systemic review and meta-analysis. J. Cardiovasc. Med. 2020, 21, 790–801. [Google Scholar] [CrossRef]
- Bjursten, H.; Rasmussen, M.; Nozohoor, S.; Gotberg, M.; Olaison, L.; Ruck, A.; Ragnarsson, S. Infective endocarditis after transcatheter aortic valve implantation: A nationwide study. Eur. Heart J. 2019, 40, 3263–3269. [Google Scholar] [CrossRef]
- Zakhour, J.; Allaw, F.; Kalash, S.; Wehbe, S.; Kanj, S.S. Infective Endocarditis after Transcatheter Aortic Valve Replacement: Challenges in the Diagnosis and Management. Pathogens 2023, 12, 255. [Google Scholar] [CrossRef]
- Tinica, G.; Tarus, A.; Enache, M.; Artene, B.; Rotaru, I.; Bacusca, A.; Burlacu, A. Infective endocarditis after TAVI: A meta-analysis and systematic review of epidemiology, risk factors and clinical consequences. Rev. Cardiovasc. Med. 2020, 21, 263–274. [Google Scholar] [PubMed]
- Cahill, T.J.; Baddour, L.M.; Habib, G.; Hoen, B.; Salaun, E.; Pettersson, G.B.; Schafers, H.J.; Prendergast, B.D. Challenges in Infective Endocarditis. J. Am. Coll. Cardiol. 2017, 69, 325–344. [Google Scholar] [CrossRef]
- Del Val, D.; Abdel-Wahab, M.; Mangner, N.; Durand, E.; Ihlemann, N.; Urena, M.; Pellegrini, C.; Giannini, F.; Gasior, T.; Wojakowski, W.; et al. Infective Endocarditis Caused by Staphylococcus aureus After Transcatheter Aortic Valve Replacement. Can. J. Cardiol. 2022, 38, 102–112. [Google Scholar] [CrossRef]
- Panagides, V.; Abdel-Wahab, M.; Mangner, N.; Durand, E.; Ihlemann, N.; Urena, M.; Pellegrini, C.; Giannini, F.; Scislo, P.; Huczek, Z.; et al. Very early infective endocarditis after transcatheter aortic valve replacement. Clin. Res. Cardiol. 2022, 111, 1087–1097. [Google Scholar] [CrossRef] [PubMed]
- Salaun, E.; Sportouch, L.; Barral, P.A.; Hubert, S.; Lavoute, C.; Casalta, A.C.; Pradier, J.; Ouk, D.; Casalta, J.P.; Lambert, M.; et al. Diagnosis of Infective Endocarditis After TAVR: Value of a Multimodality Imaging Approach. JACC Cardiovasc. Imaging 2018, 11, 143–146. [Google Scholar] [CrossRef]
- Del Val, D.; Abdel-Wahab, M.; Mangner, N.; Durand, E.; Ihlemann, N.; Urena, M.; Pellegrini, C.; Giannini, F.; Gasior, T.; Wojakowski, W.; et al. Stroke Complicating Infective Endocarditis After Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2021, 77, 2276–2287. [Google Scholar] [CrossRef] [PubMed]
- Perez-Vazquez, A.; Farinas, M.C.; Garcia-Palomo, J.D.; Bernal, J.M.; Revuelta, J.M.; Gonzalez-Macias, J. Evaluation of the Duke criteria in 93 episodes of prosthetic valve endocarditis: Could sensitivity be improved? Arch Intern Med 2000, 160, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Kappetein, A.P.; Head, S.J.; Genereux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. Eur. Heart J. 2012, 33, 2403–2418. [Google Scholar] [CrossRef]
- Kinno, M.; Cantey, E.P.; Rigolin, V.H. The transition from transesophageal to transthoracic echocardiography during transcatheter aortic valve replacement: An evolving field. J. Echocardiogr. 2019, 17, 25–34. [Google Scholar] [CrossRef]
- Wang, A.; Athan, E.; Pappas, P.A.; Fowler, V.G.; Jr Olaison, L.; Pare, C.; Almirante, B.; Munoz, P.; Rizzi, M.; Naber, C.; et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA 2007, 297, 1354–1361. [Google Scholar] [CrossRef]
- Dilsizian, V.; Budde, R.P.J.; Chen, W.; Mankad, S.V.; Lindner, J.R.; Nieman, K. Best Practices for Imaging Cardiac Device-Related Infections and Endocarditis: A JACC: Cardiovascular Imaging Expert Panel Statement. JACC Cardiovasc. Imaging 2022, 15, 891–911. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar]
- Wahadat, A.R.; Tanis, W.; Swart, L.E.; Scholtens, A.; Krestin, G.P.; van Mieghem, N.; Schurink, C.A.M.; van der Spoel, T.I.G.; van den Brink, F.S.; Vossenberg, T.; et al. Added value of (18)F-FDG-PET/CT and cardiac CTA in suspected transcatheter aortic valve endocarditis. J. Nucl. Cardiol. 2021, 28, 2072–2082. [Google Scholar] [CrossRef]
- Del Val, D.; Trottier, M.; Alperi, A.; Muntane-Carol, G.; Faroux, L.; Delarochelliere, R.; Paradis, J.M.; Dumont, E.; Kalavrouziotis, D.; Mohammadi, S.; et al. (18)F-Fluorodeoxyglucose Uptake Pattern in Noninfected Transcatheter Aortic Valves. Circ. Cardiovasc. Imaging 2020, 13, e011749. [Google Scholar] [CrossRef]
- Chen, W.; Sajadi, M.M.; Dilsizian, V. Merits of FDG PET/CT and Functional Molecular Imaging Over Anatomic Imaging with Echocardiography and CT Angiography for the Diagnosis of Cardiac Device Infections. JACC Cardiovasc. Imaging 2018, 11, 1679–1691. [Google Scholar] [CrossRef]
- Takemiya, K.; Ning, X.; Seo, W.; Wang, X.; Mohammad, R.; Joseph, G.; Titterington, J.S.; Kraft, C.S.; Nye, J.A.; Murthy, N.; et al. Novel PET and Near Infrared Imaging Probes for the Specific Detection of Bacterial Infections Associated With Cardiac Devices. JACC Cardiovasc. Imaging 2019, 12, 875–886. [Google Scholar] [CrossRef]
- De Cecco, C.N.; Bastarrika, G.; Arraiza, M.; Maurizi Enrici, M.; Pueyo, J.; Muscogiuri, G.; Fina, P.; Anselmi, A.; Di Girolamo, M.; David, V. Dual source CT: State of the art in the depiction of coronary arteries anatomy, anatomical variants and myocardial segments. Minerva Cardioangiol. 2012, 60, 133–146. [Google Scholar] [PubMed]
- Hryniewiecki, T.; Zatorska, K.; Abramczuk, E.; Zakrzewski, D.; Szymanski, P.; Kusmierczyk, M.; Michalowska, I. The usefulness of cardiac CT in the diagnosis of perivalvular complications in patients with infective endocarditis. Eur. Radiol. 2019, 29, 4368–4376. [Google Scholar] [CrossRef] [PubMed]
- Horgan, S.J.; Mediratta, A.; Gillam, L.D. Cardiovascular Imaging in Infective Endocarditis: A Multimodality Approach. Circ. Cardiovasc. Imaging 2020, 13, e008956. [Google Scholar] [CrossRef] [PubMed]
- Gomes, A.; Glaudemans, A.; Touw, D.J.; van Melle, J.P.; Willems, T.P.; Maass, A.H.; Natour, E.; Prakken, N.H.J.; Borra, R.J.H.; van Geel, P.P.; et al. Diagnostic value of imaging in infective endocarditis: A systematic review. Lancet Infect. Dis. 2017, 17, e1–e14. [Google Scholar] [CrossRef]
- Hyafil, F.; Rouzet, F.; Lepage, L.; Benali, K.; Raffoul, R.; Duval, X.; Hvass, U.; Iung, B.; Nataf, P.; Lebtahi, R.; et al. Role of radiolabelled leucocyte scintigraphy in patients with a suspicion of prosthetic valve endocarditis and inconclusive echocardiography. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 586–594. [Google Scholar] [CrossRef]
- Moriyama, N.; Laakso, T.; Biancari, F.; Raivio, P.; Jalava, M.P.; Jaakkola, J.; Dahlbacka, S.; Kinnunen, E.M.; Juvonen, T.; Husso, A.; et al. Prosthetic valve endocarditis after transcatheter or surgical aortic valve replacement with a bioprosthesis: Results from the FinnValve Registry. EuroIntervention 2019, 15, e500–e507. [Google Scholar] [CrossRef]
- Mangner, N.; Leontyev, S.; Woitek, F.J.; Kiefer, P.; Haussig, S.; Binner, C.; Mende, M.; Schlotter, F.; Stachel, G.; Hollriegel, R.; et al. Cardiac Surgery Compared with Antibiotics Only in Patients Developing Infective Endocarditis After Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2018, 7, e010027. [Google Scholar] [CrossRef]
- Latib, A.; Naim, C.; De Bonis, M.; Sinning, J.M.; Maisano, F.; Barbanti, M.; Parolari, A.; Lorusso, R.; Testa, L.; Actis Dato, G.M.; et al. TAVR-associated prosthetic valve infective endocarditis: Results of a large, multicenter registry. J. Am. Coll. Cardiol. 2014, 64, 2176–2178. [Google Scholar] [CrossRef]
- Oberbach, A.; Schlichting, N.; Feder, S.; Lehmann, S.; Kullnick, Y.; Buschmann, T.; Blumert, C.; Horn, F.; Neuhaus, J.; Neujahr, R.; et al. New insights into valve-related intramural and intracellular bacterial diversity in infective endocarditis. PLoS ONE 2017, 12, e0175569. [Google Scholar] [CrossRef]
- Oberbach, A.; Schlichting, N.; Hagl, C.; Lehmann, S.; Kullnick, Y.; Friedrich, M.; Kohl, U.; Horn, F.; Kumbhari, V.; Loffler, B.; et al. Four decades of experience of prosthetic valve endocarditis reflect a high variety of diverse pathogens. Cardiovasc. Res. 2023, 119, 410–428. [Google Scholar] [CrossRef]
- Jean, S.S.; Liu, I.M.; Hsieh, P.C.; Kuo, D.H.; Liu, Y.L.; Hsueh, P.R. Off-label use versus formal recommendations of conventional and novel antibiotics for the treatment of infections caused by multidrug-resistant bacteria. Int. J. Antimicrob. Agents 2023, 61, 106763. [Google Scholar] [CrossRef]
- Houard, V.; Porte, L.; Delon, C.; Carrie, D.; Delobel, P.; Galinier, M.; Lairez, O.; Lavie-Badie, Y. Prognostic value of residual vegetation after antibiotic treatment for infective endocarditis: A retrospective cohort study. Int. J. Infect. Dis. 2020, 94, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Del Val, D.; Panagides, V.; Mestres, C.A.; Miro, J.M.; Rodes-Cabau, J. Infective Endocarditis After Transcatheter Aortic Valve Replacement: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2023, 81, 394–412. [Google Scholar] [CrossRef] [PubMed]
- Del Val, D.; Linke, A.; Abdel-Wahab, M.; Latib, A.; Ihlemann, N.; Urena, M.; Won-Keun, K.; Husser, O.; Herrmann, H.C.; Nombela-Franco, L.; et al. Long-Term Outcomes After Infective Endocarditis After Transcatheter Aortic Valve Replacement. Circulation 2020, 142, 1497–1499. [Google Scholar] [CrossRef]
- Berrios-Torres, S.I.; Umscheid, C.A.; Bratzler, D.W.; Leas, B.; Stone, E.C.; Kelz, R.R.; Reinke, C.E.; Morgan, S.; Solomkin, J.S.; Mazuski, J.E.; et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017, 152, 784–791. [Google Scholar] [CrossRef]
- Gomes, B.; Geis, N.A.; Leuschner, F.; Meder, B.; Konstandin, M.; Katus, H.A.; Bekeredjian, R. Periprocedural antibiotic treatment in transvascular aortic valve replacement. J. Interv. Cardiol. 2018, 31, 885–890. [Google Scholar] [CrossRef]
- Conen, A.; Stortecky, S.; Moreillon, P.; Hannan, M.M.; Franzeck, F.C.; Jeger, R.; Widmer, A.F. A review of recommendations for infective endocarditis prevention in patients undergoing transcatheter aortic valve implantation. EuroIntervention 2021, 16, 1135–1140. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Incidence of TAVR-IE | |||
|---|---|---|---|
| Trial | Very Early | Early | Late |
| PARTNER 3 | |||
| TAVR | 0.0% | 0.2% | 0.2% |
| SAVR | 0.2% | 0.5% | 0.9% |
| PARTNER 2 | |||
| TAVR | 0.0% | 0.8% | 1.2% |
| SAVR | 0.0% | 0.7% | 0.7% |
| PARTNER 1 | |||
| TAVR | 0.0% | 1.0% | 1.5% |
| SAVR | 0.3% | 1.1% | 1.0% |
| Evolut Low-Risk Trial | |||
| TAVR | 0.1% | 0.2% | - |
| SAVR | 0.2% | 0.4% | - |
| Causative Organism | Incidence | Time from TAVR a | Risk Factors | Strength of Association b | Level of Evidence c |
|---|---|---|---|---|---|
| Most Common | |||||
| Staphylococcus | 22–30% | >1-year post-TAVR | Soft tissue infection, vascular access | High | B–NR |
| Streptococcus | 20–30% | >1-year post-TAVR | Dental procedures, low-risk TAVR | Low | B–NR |
| Enterococcus | 15–25% | <100 days post-TAVR | Groin colonization 1, frequent healthcare use, higher antibiotic exposure | Moderate | B–NR |
| Least common | |||||
| Gram negative | <5% | Median time—1.1 months | Nosocomial infections | N/A | C–EO |
| Fungal | 0.8–3% | Limited data | Drug abuse | N/A | C–LD |
| TAVR-IE Outcomes | |||||
|---|---|---|---|---|---|
| Study | Surgical Aortic Valve Explant | Mortality | |||
| Very Early | Early | Late | Very Late | ||
| Mentias et al., 2020 [10] | 3.8% | 18.5% | 45.6% | - | - |
| Stortecky et al., 2020 [17] | - | 26.0% | 43.7% | - | - |
| Fauchier et al., 2020 [13] | - | 18.7% | 32.8% | - | - |
| del Val et al., 2020 [55] | - | - | - | - | 62.5% |
| Regueiro et al., 2019 [21] | 10.8% | - | 52.0% | 67.0% | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Braghieri, L.; Kaur, S.; Black, C.K.; Cremer, P.C.; Unai, S.; Kapadia, S.R.; Mentias, A. Endocarditis after Transcatheter Aortic Valve Replacement. J. Clin. Med. 2023, 12, 7042. https://doi.org/10.3390/jcm12227042
Braghieri L, Kaur S, Black CK, Cremer PC, Unai S, Kapadia SR, Mentias A. Endocarditis after Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine. 2023; 12(22):7042. https://doi.org/10.3390/jcm12227042
Chicago/Turabian StyleBraghieri, Lorenzo, Simrat Kaur, Christopher K. Black, Paul C. Cremer, Shinya Unai, Samir R. Kapadia, and Amgad Mentias. 2023. "Endocarditis after Transcatheter Aortic Valve Replacement" Journal of Clinical Medicine 12, no. 22: 7042. https://doi.org/10.3390/jcm12227042
APA StyleBraghieri, L., Kaur, S., Black, C. K., Cremer, P. C., Unai, S., Kapadia, S. R., & Mentias, A. (2023). Endocarditis after Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine, 12(22), 7042. https://doi.org/10.3390/jcm12227042