
Donor Age, Sex, and Cause of Death and Their Relationship to Heart Transplant Recipient Cardiac Death

 ,
,
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Methods
2.1. Database
2.2. Patient Population
2.3. Statistical Analysis
3. Results
3.1. Donor and Recipient Characteristics
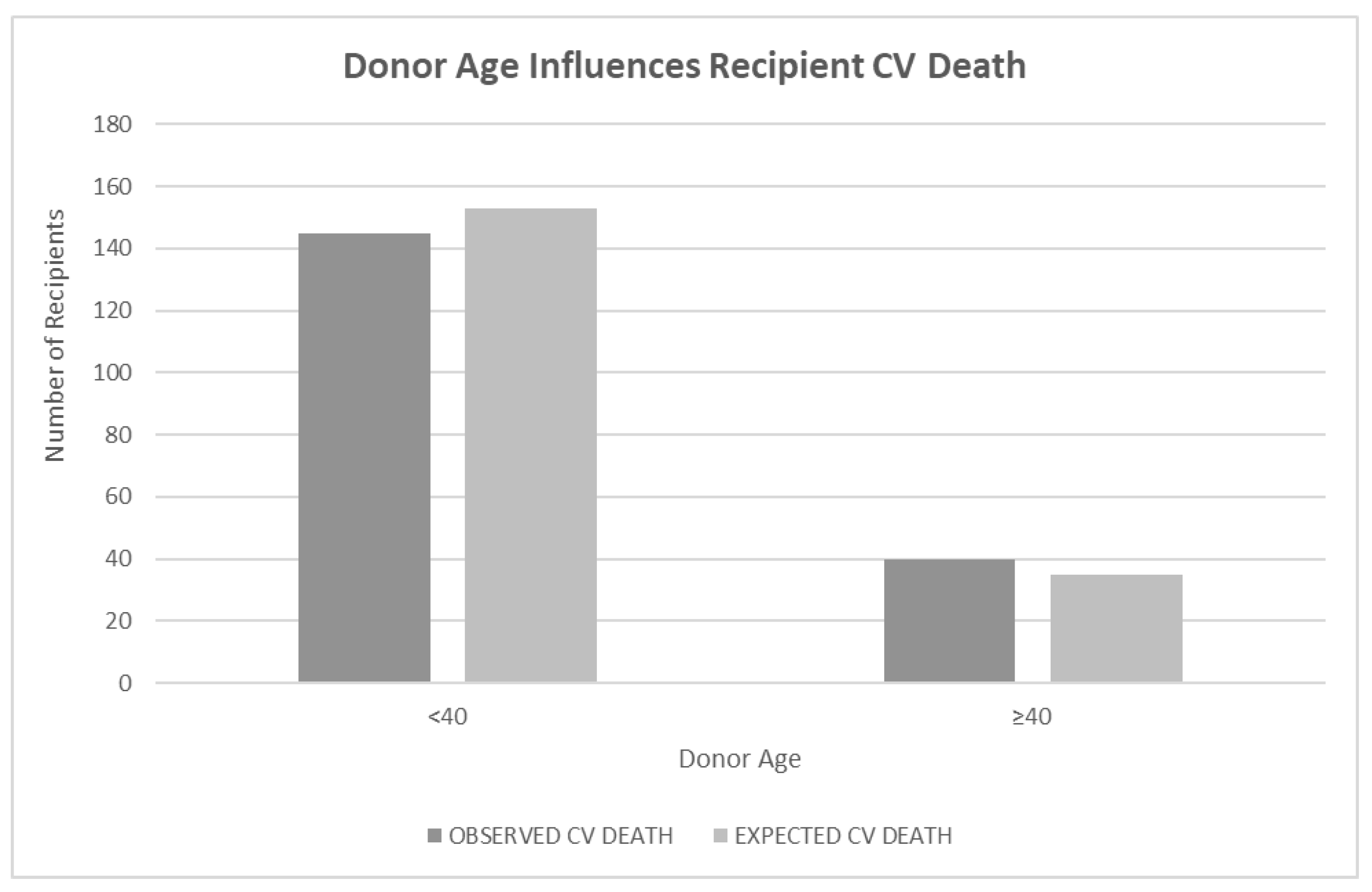
3.2. Effect of Donor Age on Recipient CV Death
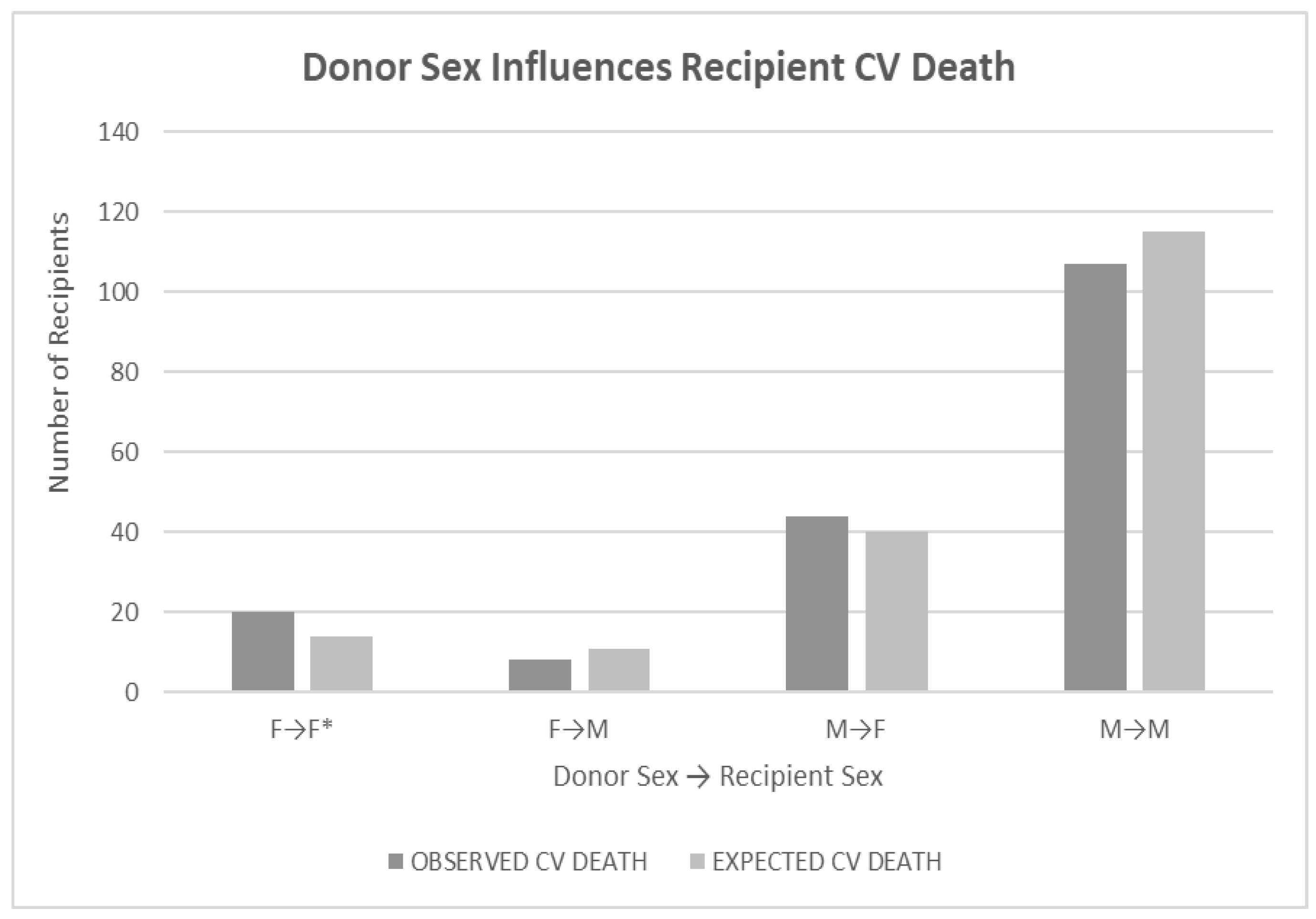
3.3. Effect of Donor Sex on Recipient CV Death
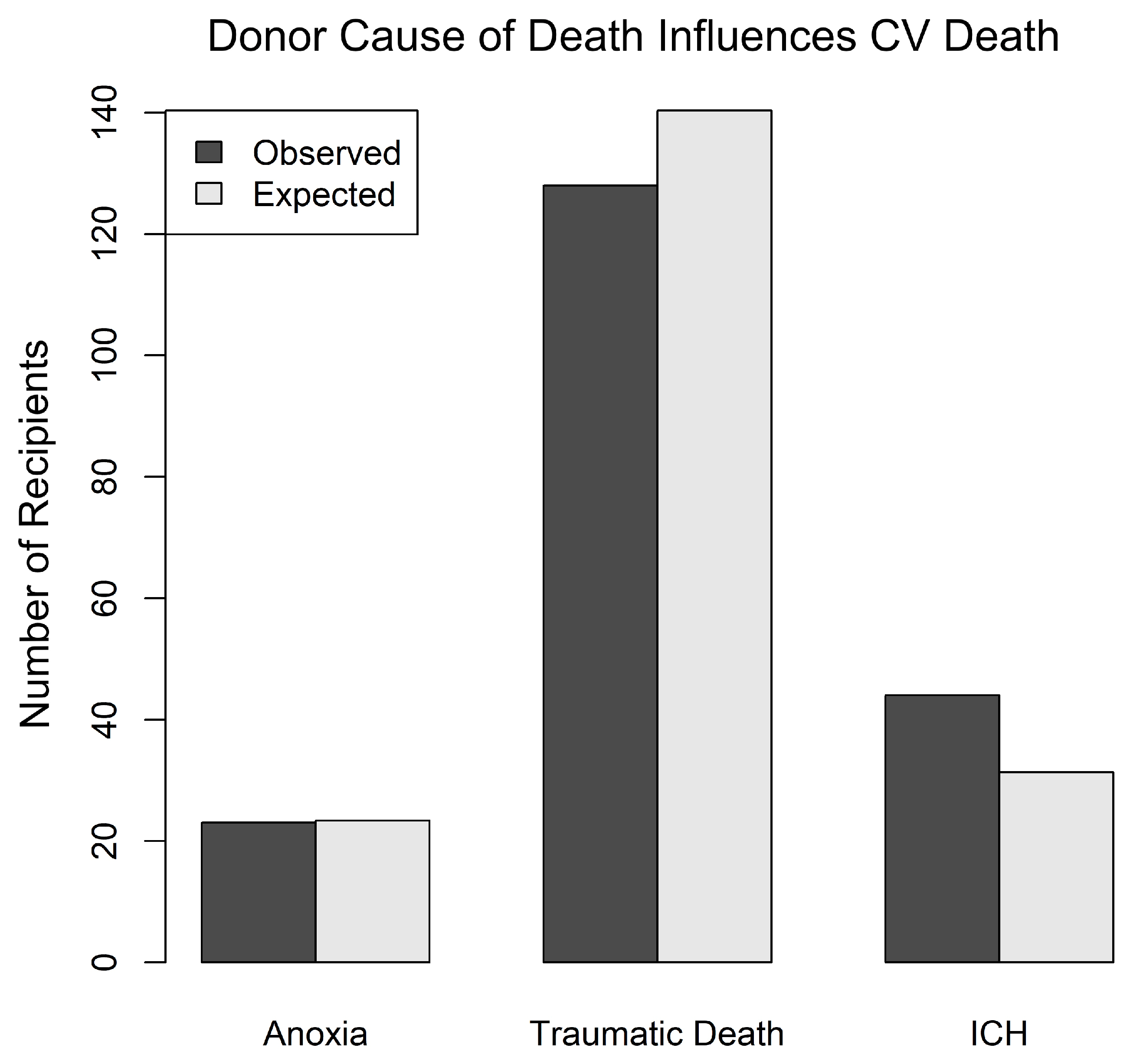
3.4. Effect of Donor COD on Recipient CV Death
4. Discussion
5. Continued Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kittleson, M.M.; Kobashigawa, J.A. Cardiac Transplantation: Current Outcomes and Contemporary Controversies. JACC Heart Fail. 2017, 5, 857–868. [Google Scholar] [CrossRef] [PubMed]
- Hsich, E.M.; Blackstone, E.H.; Thuita, L.W.; McNamara, D.M.; Rogers, J.G.; Yancy, C.W.; Goldberg, L.R.; Valapour, M.; Xu, G.; Ishwaran, H. Heart Transplantation: An In-Depth Survival Analysis. JACC Heart Fail. 2020, 8, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Pober, J.S.; Chih, S.; Kobashigawa, J.; Madsen, J.C.; Tellides, G. Cardiac allograft vasculopathy: Current review and future research directions. Cardiovasc. Res. 2021, 117, 2624–2638. [Google Scholar] [CrossRef] [PubMed]
- Land, W.G.; Agostinis, P.; Gasser, S.; Garg, A.D.; Linkermann, A. Transplantation and damage-associated molecular patterns (DAMPs). Am. J. Transplant. 2016, 16, 3338–3361. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Dejana, E.; Fiocchi, C. Immune regulation by microvascular endothelial cells: Directing innate and adaptive immunity, coagulation, and inflammation. J. Immunol. 2007, 178, 6017–6022. [Google Scholar] [CrossRef] [PubMed]
- Pober, J.S.; Jane-wit, D.; Qin, L.; Tellides, G. Interacting mechanisms in the pathogenesis of cardiac allograft vasculopathy. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1609–1614. [Google Scholar] [CrossRef]
- Millington, T.M.; Madsen, J.C. Innate immunity and cardiac allograft rejection. Kidney Int. Suppl. 2010, 119, S18–S21. [Google Scholar] [CrossRef]
- Silvis, M.J.M.; Kaffka Genaamd Dengler, S.E.; Odille, C.A.; Mishra, M.; van der Kaaij, N.P.; Doevendans, P.A.; Sluijter, J.P.G.; de Kleijn, D.P.V.; de Jager, S.C.A.; Bosch, L.; et al. Damage-Associated Molecular Patterns in Myocardial Infarction and Heart Transplantation: The Road to Translational Success. Front. Immunol. 2020, 11, 599511. [Google Scholar] [CrossRef]
- Barac, Y.D.; Jawitz, O.K.; Klapper, J.; Schroder, J.; Daneshmand, M.A.; Patel, C.; Hartwig, M.G.; Sweitzer, N.K.; Milano, C.A. Heart Transplantation Survival and the Use of Traumatically Brain-Injured Donors: UNOS Registry Propensity-Matched Analysis. J. Am. Heart Assoc. 2019, 8, e012894. [Google Scholar] [CrossRef]
- Van den Hoogen, P.; Huibers, M.M.; Sluijter, J.P.; de Weger, R.A. Cardiac allograft vasculopathy: A donor or recipient induced pathology? J. Cardiovasc. Transl. Res. 2015, 8, 106–116. [Google Scholar] [CrossRef]
- Singhal, A.K.; Sheng, X.; Drakos, S.G.; Stehlik, J. Impact of donor cause of death on transplant outcomes: UNOS registry analysis. Transplant. Proc. 2009, 41, 3539–3544. [Google Scholar] [CrossRef] [PubMed]
- Nagji, A.S.; Hranjec, T.; Swenson, B.R.; Kern, J.A.; Bergin, J.D.; Jones, D.R.; Kron, I.L.; Lau, C.L.; Ailawadi, G. Donor age is associated with chronic allograft vasculopathy after adult heart transplantation: Implications for donor allocation. Ann. Thorac. Surg. 2010, 90, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, J.R.; Cheng, A.; Ising, M.; Lenneman, A.; Birks, E.; Slaughter, M.S. Heart Transplant Survival Based on Recipient and Donor Risk Scoring: A UNOS Database Analysis. ASAIO J. 2016, 62, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Kfoury, A.G.; Stehlik, J.; Renlund, D.G.; Snow, G.; Seaman, J.T.; Gilbert, E.M.; Stringham, J.S.; Long, J.W.; Hammond, M.E.H. Impact of repetitive episodes of antibody-mediated or cellular rejection on cardiovascular mortality in cardiac transplant recipients: Defining rejection patterns. J. Heart Lung Transplant. 2006, 25, 1277–1282. [Google Scholar] [CrossRef]
- Hammond, M.E.H.; Revelo, M.P.; Miller, D.V.; Snow, G.L.; Budge, D.; Stehlik, J.; Molina, K.M.; Selzman, C.H.; Drakos, S.G.; Alharethi, R.A.; et al. ISHLT pathology antibody mediated rejection score correlates with increased risk of cardiovascular mortality: A retrospective validation analysis. J. Heart Lung Transplant. 2016, 35, 320–325. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org/ (accessed on 1 June 2023).
- Farrar, C.A.; Kupiec-Weglinski, J.W.; Sacks, S.H. The innate immune system and transplantation. Cold Spring Harb. Perspect. Med. 2013, 3, a015479. [Google Scholar] [CrossRef]
- Hammond, M.E.H.; Kfoury, A.G. Antibody-mediated rejection in the cardiac allograft: Diagnosis, treatment and future considerations. Curr. Opin. Cardio 2017, 32, 326–335. [Google Scholar] [CrossRef]
- Halloran, P.F.; Madill-Thomsen, K.S. The Molecular Microscope Diagnostic System: Assessment of Rejection and Injury in Heart Transplant Biopsies. Transplantation 2023, 107, 27–44. [Google Scholar] [CrossRef]
- Grupper, A.; Nestorovic, E.M.; Daly, R.C.; Milic, N.M.; Joyce, L.D.; Stulak, J.M.; Joyce, D.L.; Edwards, B.S.; Pereira, N.L.; Kushwaha, S.S. Sex Related Differences in the Risk of Antibody-Mediated Rejection and Subsequent Allograft Vasculopathy Post-Heart Transplantation: A Single-Center Experience. Transplant. Direct. 2016, 2, e106. [Google Scholar] [CrossRef]
- Kovats, S. Estrogen receptors regulate innate immune cells and signaling pathways. Cell Immunol. 2015, 294, 63–69. [Google Scholar] [CrossRef]
- Ćuruvija, I.; Stanojević, S.; Arsenović-Ranin, N.; Blagojević, V.; Dimitrijević, M.; Vidić-Danković, B.; Vujić, V. Sex Differences in Macrophage Functions in Middle-Aged Rats: Relevance of Estradiol Level and Macrophage Estrogen Receptor Expression. Inflammation 2017, 40, 1087–1101. [Google Scholar] [CrossRef] [PubMed]
- Laffont, S.; Seillet, C.; Guéry, J.C. Estrogen Receptor-Dependent Regulation of Dendritic Cell Development and Function. Front. Immunol. 2017, 8, 108. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.K.; Yoon, B.K. Controversies regarding hormone therapy: Insights from inflammation and hemostasis. Cardiovasc. Res. 2006, 70, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Furman, D.; Hejblum, B.P.; Simon, N.; Jojic, V.; Dekker, C.L.; Thiebaut, R.; Tibshirani, R.J.; Davis, M.M. Systems analysis of sex differences reveals an immunosuppressive role for testosterone in the response to influenza vaccination. Proc. Natl. Acad. Sci. USA 2014, 111, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Bergenfeldt, H.; Lund, L.H.; Stehlik, J.; Andersson, B.; Hoglund, P.; Nilsson, J. Time-dependent prognostic effects of recipient and donor age in adult heart transplantation. J. Heart Lung Transplant. 2019, 38, 174–183. [Google Scholar] [CrossRef]
- Pence, B.D.; Yarbro, J.R. Classical monocytes maintain ex vivo glycolytic metabolism and early but not later inflammatory responses in older adults. Immun. Ageing 2019, 16, 3. [Google Scholar] [CrossRef]
- Franceschi, C.; Garagnani, P.; Parini, P.; Giuliani, C.; Santoro, A. Inflammaging: A new immune-metabolic viewpoint for age-related diseases. Nat. Rev. Endocrinol. 2018, 14, 576–590. [Google Scholar] [CrossRef]
- Ladecola, C.; Buckwalter, M.S.; Anrather, J. Immune responses to stroke: Mechanisms, modulation, and therapeutic potential. J. Clin. Investig. 2020, 130, 2777–2788. [Google Scholar] [CrossRef]
- Chamorro, A.; Meisel, A.; Planas, A.M.; Urra, X.; van de Beek, D.; Veltkamp, R. The immunology of acute stroke. Nat. Rev. Neurol. 2012, 8, 401–410. [Google Scholar] [CrossRef]
- Schanze, N.; Bode, C.; Duerschmied, D. Platelet Contributions to Myocardial Ischemia/Reperfusion Injury. Front. Immunol. 2019, 10, 1260. [Google Scholar] [CrossRef]
- Janakiram, N.B.; Valerio, M.S.; Goldman, S.M.; Dearth, C.L. The Role of the Inflammatory Response in Mediating Functional Recovery Following Composite Tissue Injuries. Int. J. Mol. Sci. 2021, 22, 13552. [Google Scholar] [CrossRef] [PubMed]
- Huber-Lang, M.; Lambris, J.D.; Ward, P.A. Innate immune responses to trauma. Nat. Immunol. 2018, 19, 327–341. [Google Scholar] [CrossRef] [PubMed]
- Kopecky, B.J.; Dun, H.; Amrute, J.M.; Lin, C.-Y.; Bredemeyer, A.L.; Terada, Y.; Bayguinov, P.O.; Koenig, A.L.; Frye, C.C.; Fitzpatrick, J.A.J.; et al. Donor macrophages modulate rejection after heart transplantation. Circulation 2022, 146, 623–638. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hammond, M.E.; Zollinger, C.; Vidic, A.; Snow, G.L.; Stehlik, J.; Alharethi, R.A.; Kfoury, A.G.; Drakos, S.; Hammond, M.E.H. Donor Age, Sex, and Cause of Death and Their Relationship to Heart Transplant Recipient Cardiac Death. J. Clin. Med. 2023, 12, 7629. https://doi.org/10.3390/jcm12247629
Hammond ME, Zollinger C, Vidic A, Snow GL, Stehlik J, Alharethi RA, Kfoury AG, Drakos S, Hammond MEH. Donor Age, Sex, and Cause of Death and Their Relationship to Heart Transplant Recipient Cardiac Death. Journal of Clinical Medicine. 2023; 12(24):7629. https://doi.org/10.3390/jcm12247629
Chicago/Turabian StyleHammond, Margo E., Charles Zollinger, Andrija Vidic, Gregory L. Snow, Josef Stehlik, Rami A. Alharethi, Abdallah G. Kfoury, Stavros Drakos, and M Elizabeth H. Hammond. 2023. "Donor Age, Sex, and Cause of Death and Their Relationship to Heart Transplant Recipient Cardiac Death" Journal of Clinical Medicine 12, no. 24: 7629. https://doi.org/10.3390/jcm12247629
APA StyleHammond, M. E., Zollinger, C., Vidic, A., Snow, G. L., Stehlik, J., Alharethi, R. A., Kfoury, A. G., Drakos, S., & Hammond, M. E. H. (2023). Donor Age, Sex, and Cause of Death and Their Relationship to Heart Transplant Recipient Cardiac Death. Journal of Clinical Medicine, 12(24), 7629. https://doi.org/10.3390/jcm12247629