
Artificial Intelligence-Powered Left Ventricular Ejection Fraction Analysis Using the LVivoEF Tool for COVID-19 Patients
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Endpoints
2.3. Study Protocol
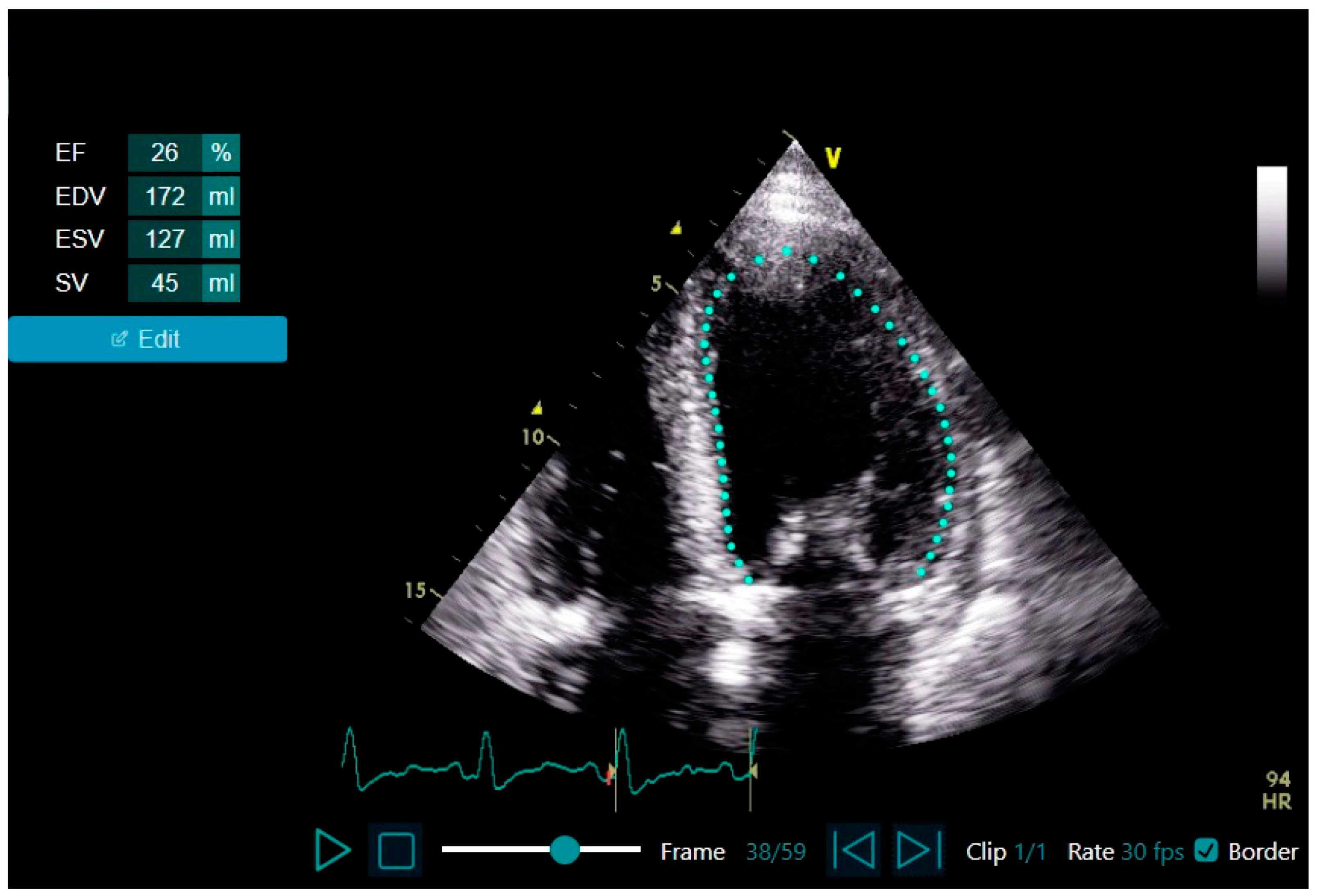
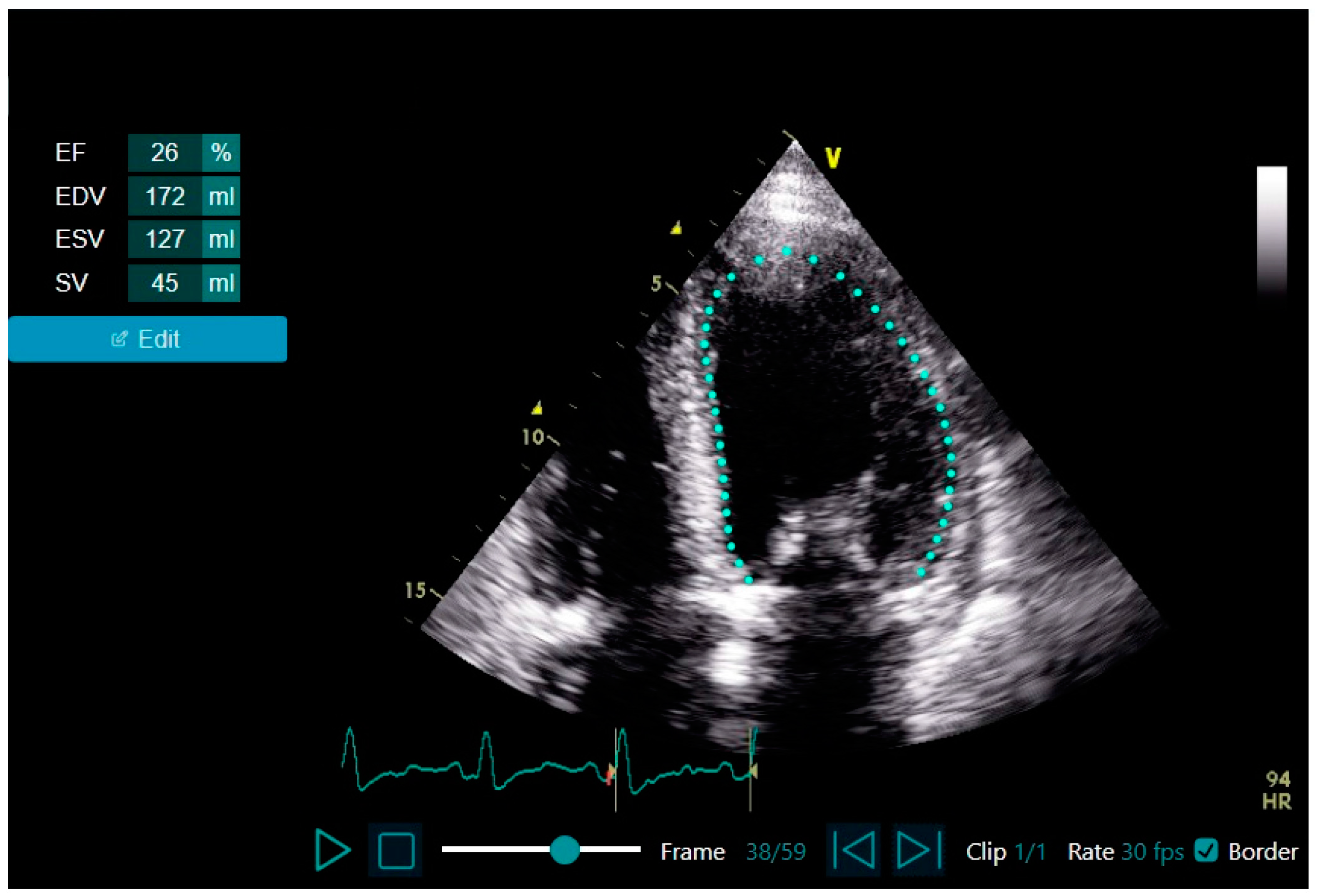
2.4. Echocardiogram Acquisition and LVEF Assessment Using LVivo EF vs. Expert Assessment
2.5. Sample Size Calculation
2.6. Statistical Analyses
3. Results
3.1. Baseline, Clinical, and Test Characteristics and in-Hospital Course: AI-Based Preserved vs. Reduced LVEF (Table 1)

{kind=link}
{kind=link}
{kind=link}
| Variable | All n = 42 | Preserved LVEF n = 31 | Reduced LVEF n = 11 | p-Value |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Age, mean ± SD | 53.3 ± 17.8 | 49.7 ± 17.1 | 63.5 ± 16.3 | 0.026 |
| Male, n (%) | 21 (50.0) | 15 (48.4) | 6 (54.5) | 0.726 |
| Body mass index, mean ± SD | 27.6 ± 5.1 | 27.1 ± 4.3 | 28.7 ± 6.9 | 0.459 |
| Smoking, n (%) | 4 (9.5) | 3 (9.7) | 1 (9.1) | 1.000 |
| Diabetes mellitus, n (%) | 14 (33.3) | 8 (25.8) | 6 (54.5) | 0.082 |
| Hypertension, n (%) | 13 (31.0) | 5 (16.1) | 8 (72.7) | 0.001 |
| Hyperlipidemia, n(%) | 13 (31.0) | 5 (16.1) | 8 (72.7) | 0.001 |
| Ischemic heart disease, n (%) | 7 (16.7) | 2 (6.5) | 5 (45.5) | 0.009 |
| Cerebrovascular accident, n (%) | 1 (2.4) | 1 (3.2) | 0 | 1.000 |
| Revascularization, n (%) | 7 (16.7) | 2 (6.5) | 5 (45.5) | 0.009 |
| Heart failure, n (%) | 5 (11.9) | 1 (3.2) | 4 (36.4) | 0.013 |
| Valve replacement, n (%) | 2 (4.8) | 1 (3.2) | 1 (9.1) | 0.460 |
| CIED, n (%) | 1 (2.4) | 0 | 1 (9.1) | 0.262 |
| Cognitive decline, n (%) | 4 (9.5) | 2 (6.5) | 2 (18.2) | 0.277 |
| Debilitation, n (%) | 6 (14.3) | 3 (9.7) | 3 (27.3) | 0.314 |
| Chronic lung disease, n (%) | 3 (7.1) | 3 (9.7) | 0 | 0.554 |
| Liver disease, n (%) | 1 (2.4) | 1 (3.2) | 0 | 1.000 |
| Prior venous thromboembolism, n (%) | 3 (7.1) | 2 (6.5) | 1 (9.1) | 1.000 |
| Autoimmune disease, n (%) | 2 (4.8) | 1 (3.2) | 1 (9.1) | 0.460 |
| Hypothyroidism, n (%) | 3 (7.1) | 2 (6.5) | 1 (9.1) | 1.000 |
| Chronic medications | ||||
| ACE-I/ARB, n (%) | 10 (23.8) | 2 (6.5) | 8 (72.7) | <0.001 |
| β-blockers, n (%) | 11 (26.2) | 5 (16.1) | 6 (54.5) | 0.021 |
| Calcium channel blockers, n (%) | 3 (7.1) | 2 (6.5) | 1 (9.1) | 1.000 |
| Anti-platelets, n (%) | 10 (23.8) | 4 (12.9) | 6 (54.5) | 0.011 |
| Oral anticoagulation, n (%) | 5 (11.9) | 2 (6.5) | 3 (27.3) | 0.103 |
| Diuretics, n (%) | 2 (4.8) | 1 (3.2) | 1 (9.1) | 0.460 |
| Inhalations, n (%) | 4 (9.5) | 4 (12.9) | 0 | 0.558 |
| SGLT2 inhibitors, n (%) | 1 (2.4) | 0 | 1 (9.1) | 0.262 |
| Statins, n (%) | 13 (31.0) | 5 (16.1) | 8 (72.7) | 0.001 |
| COVID-19 presentation | ||||
| Chest pain, n (%) | 17 (40.5) | 10 (32.3) | 7 (63.6) | 0.086 |
| Shortness of breath, n (%) | 25 (59.5) | 15 (48.4) | 10 (90.9) | 0.016 |
| Heart rate (bpm), mean ± SD | 92.2 ± 21.1 | 91.8 ± 19.7 | 93.6 ± 35.0 | 0.632 |
| SBP (mmHg), mean ± SD | 123.0 ± 18.9 | 122.8 ± 18.6 | 123.3 ± 20.5 | 0.978 |
| DBP (mmHg), mean ± SD | 75.5 ± 12.7 | 75.1 ± 11.1 | 76.6 ± 17.1 | 0.800 |
| Oxygen saturation (%), mean ± SD | 90.3 ± 5.5 | 91.2 ± 5.1 | 87.7 ± 5.9 | 0.092 |
| In-hospital course | ||||
| Sinus tachycardia, n (%) | 5 (11.9) | 3 (9.7) | 2 (18.2) | 0.593 |
| Electrocardiogram changes | 0.078 | |||
| Normal, n (%) | 25 (59.5) | 20 (64.5) | 5 (45.5) | |
| Nonspecific changes, n (%) | 10 (23.8) | 8 (25.8) | 2 (18.2) | |
| TWI/ST-depression, n (%) | 5 (11.9) | 3 (9.7) | 2 (18.2) | |
| ST-elevation, n (%) | 2 (4.8) | 0 | 2 (18.2) | |
| Chest X-ray infiltrates, n (%) | 28 (66.7) | 18 (58.1) | 10 (90.9) | 0.067 |
| Atrial fibrillation/flutter, n (%) | 4 (9.5) | 0 | 4 (36.4) | 0.003 |
| Lab results | ||||
| White blood cells (peak), mean ± SD | 8.6 ± 3.5 | 8.1 ± 2.8 | 10.0 ± 4.9 | 0.322 |
| ANC/ALC (admission), median [IQR] | 4.2 [2.6–8.6] | 3.4 [2.4–6.9] | 6.5 [4.8–9.7] | 0.086 |
| Hemoglobin (admission), mean ± SD | 12.8 ± 2.3 | 13.2 ± 2.1 | 11.7 ± 2.5 | 0.110 |
| Platelets (admission), mean ± SD | 193.6 ± 55.7 | 192.7 ± 58.7 | 196.1 ± 49.0 | 0.591 |
| Creatinine (admission), mean ± SD | 1.0 ± 0.8 | 0.8 ± 0.3 | 1.6 ± 1.4 | 0.005 |
| Potassium (admission), mean ± SD | 4.0 ± 0.6 | 3.8 ± 0.4 | 4.4 ± 0.9 | 0.051 |
| Albumin (trough), mean ± SD | 3.4 ± 0.7 | 3.6 ± 0.6 | 2.8 ± 0.7 | 0.010 |
| Hs-cTnI (peak), median [IQR] | 6.5 [5.0–17.3] | 5 [5–8.5] | 40 [13.5–7467] | <0.001 |
| CRP (peak), median [IQR] | 6.5 [1.2–15.3] | 3.6 [0.7–9.8] | 21.4 [12.7–23.3] | <0.001 |
| D-dimer (peak), median [IQR] | 824 [549–1060] | 728 [402–977] | 1073 [921–1932] | 0.001 |
| Fibrinogen (admission), mean ± SD | 578.7 ± 163.6 | 555.9 ± 151.8 | 640.9 ± 185.4 | 0.226 |
| aPTT (peak), mean ± SD | 3.3 ± 4.9 | 33.3 ± 5.1 | 33.3 ± 4.3 | 0.717 |
| Exam characteristics and technical aspects | ||||
| Ability to turn left, n (%) | 35 (83.3) | 28 (90.3) | 7 (63.6) | 0.063 |
| Effective communication, n (%) | 39 (92.9) | 30 (96.8) | 9 (81.8) | 0.163 |
| Length of study (minutes), mean ± SD | 6.8 ± 2.2 | 6.4 ± 2.1 | 8.1 ± 2.0 | 0.007 |
| Full view successful completion, n (%) | 38 (90.5) | 29 (93.5) | 9 (81.8) | 0.277 |
| Study quality | 0.618 | |||
| Good, n (%) | 27 (64.3) | 19 (61.3) | 8 (72.7) | |
| Fair, n (%) | 8 (19.0) | 7 (22.6) | 1 (9.1) | |
| Poor, n (%) | 7 (16.7) | 5 (16.1) | 2 (18.2) | |
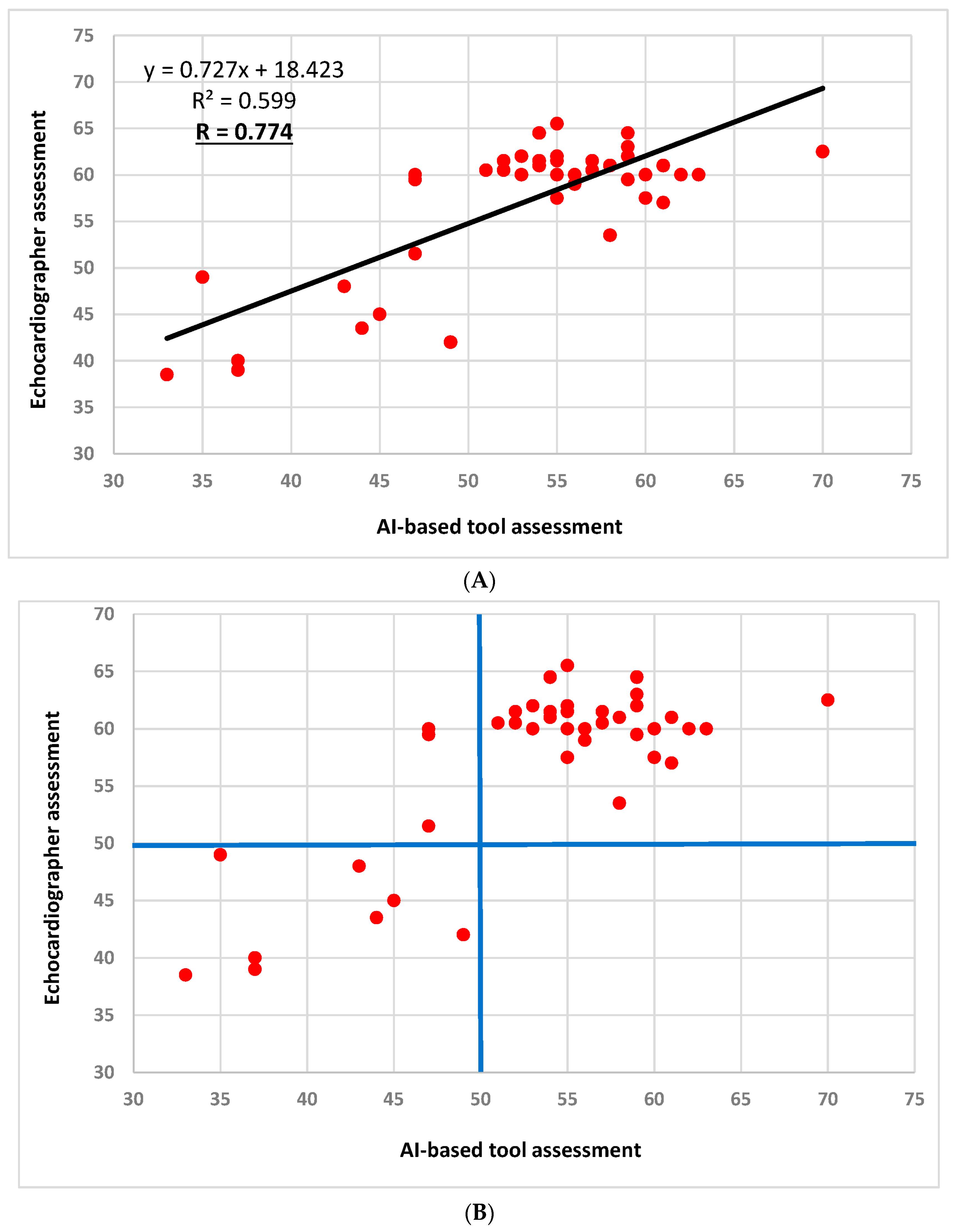
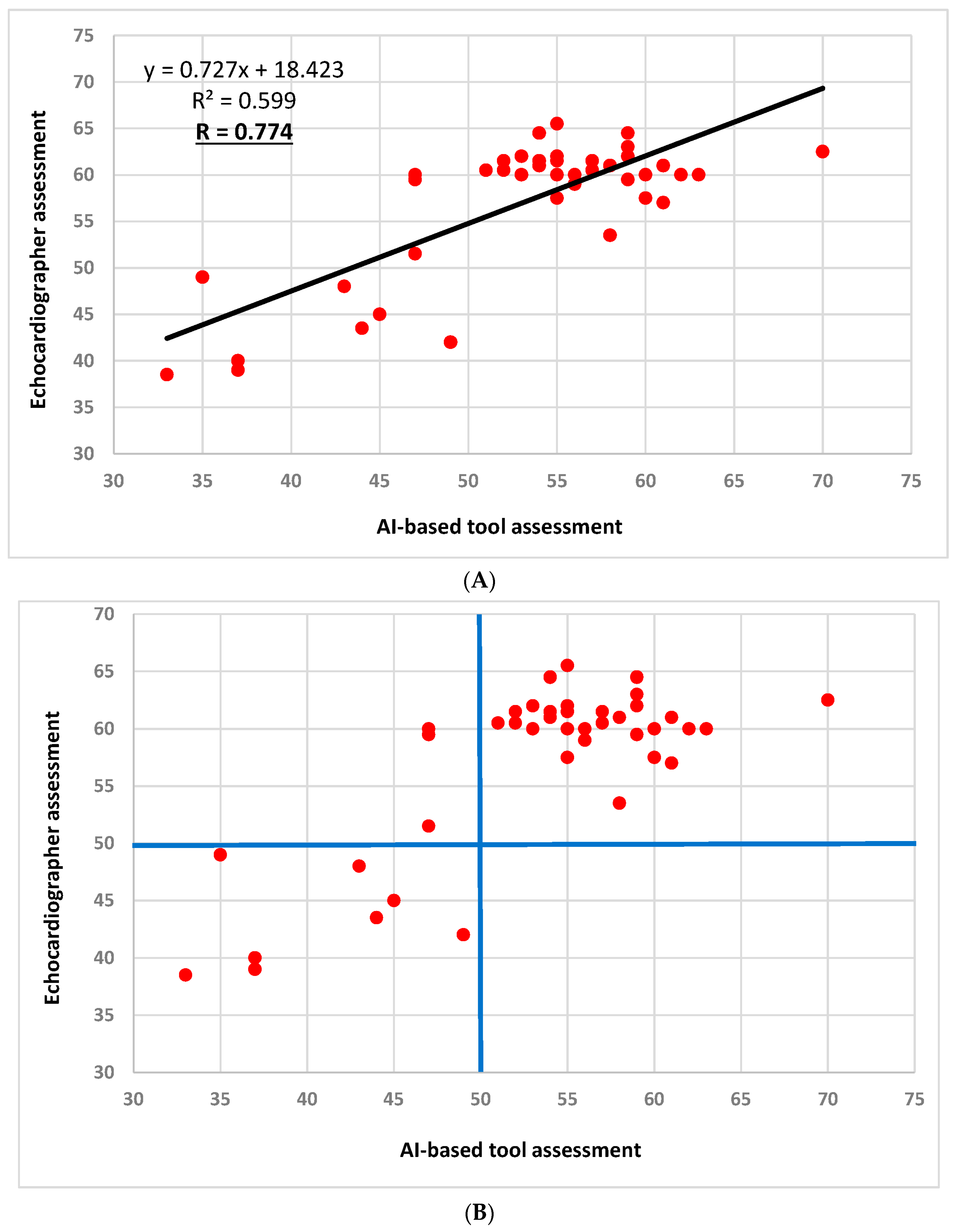
3.2. LVEF Assessment Correlations and Agreement
3.3. Sensitivity and Specificity Analyses
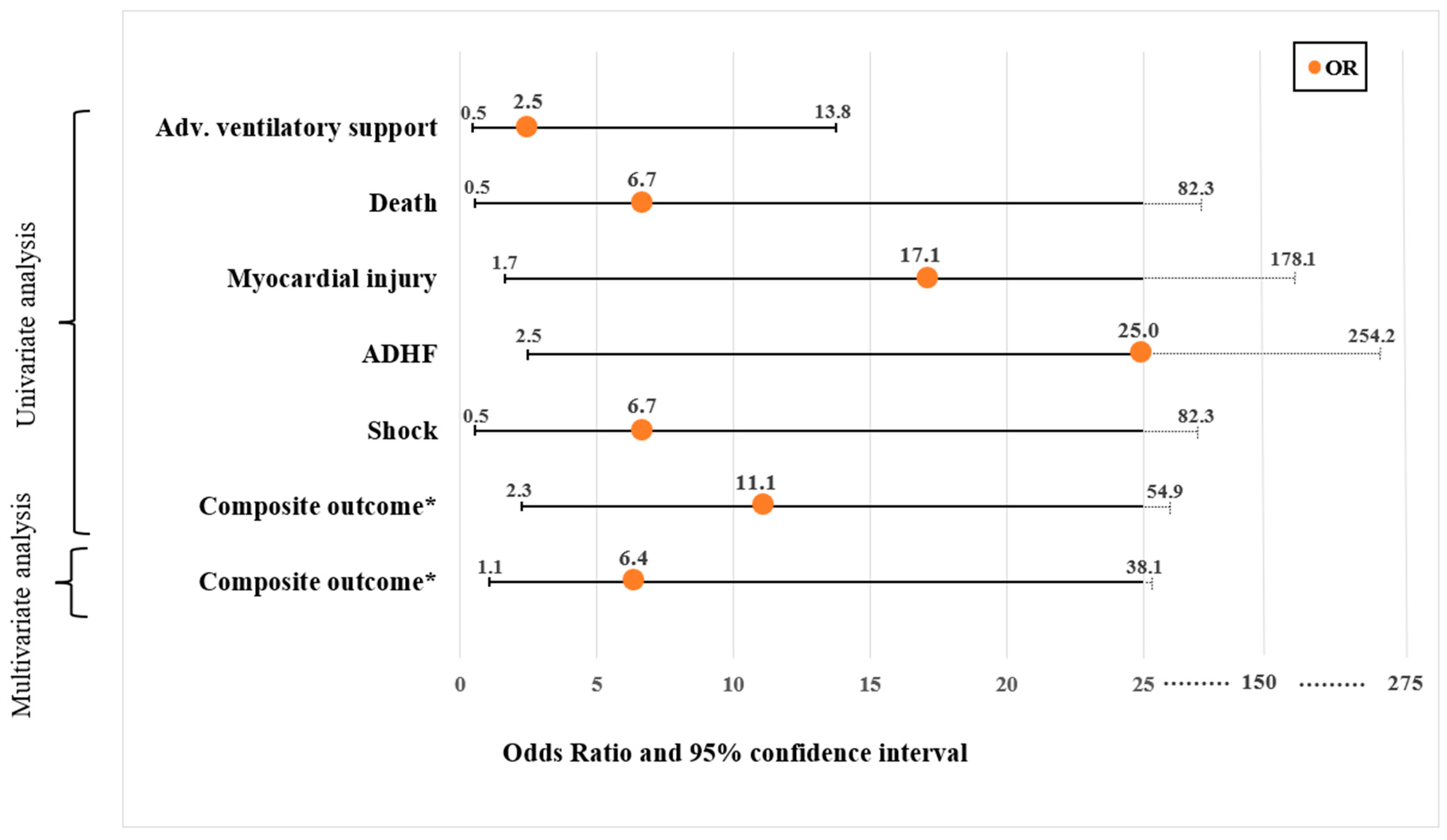
3.4. Association between Reduced LVEF (<50%) Using the AI-Based Tool and Study Endpoints (Table 2 and Figure 3)
| Variable | All n = 42 | Preserved LVEF n = 31 | Reduced LVEF n = 11 | p-Value | Unadjusted OR (95% CI) |
|---|---|---|---|---|---|
| Composite endpoint, n (%) | 14 (33.3) | 6 (19.4) | 8 (72.7) | 0.003 | 11.1 (2.25–54.94) |
| In-hospital death, n (%) | 2 (4.8) | 0 | 2 (18.2) | 0.064 | 6.7 (0.54–82.31) |
| Advanced VS, n (%) | 7 (16.7) | 4 (12.9) | 3 (27.3) | 0.282 | 2.5 (0.47–13.75) |
| Myocardial injury, n (%) | 5 (11.9) | 1 (3.2) | 4 (36.4) | 0.017 | 17.1 (1.65–178.08) |
| Shock, n (%) | 2 (4.8) | 0 | 2 (18.2) | 0.064 | 6.7 (0.54–82.31) |
| ADHF, n (%) | 6 (14.3) | 1 (3.2) | 5 (45.5) | 0.007 | 25 (2.46–254.15) |
| RRT, n (%) | 2 (4.8) | 0 | 2 (18.2) | 0.064 | 6.7 (0.54–82.31) |
| VTE, n (%) | 1 (2.4) | 1 (3.2) | 0 | 1.000 | 3.0 (0.17–52.53) |
| Anti-COVID drugs, n (%) | 18 (42.9) | 12 (38.7) | 6 (54.5) | 0.362 | 1.9 (0.47–7.63) |
| Sepsis, n (%) | 2 (4.8) | 0 | 2 (18.2) | 0.064 | 6.7 (0.54–82.31) |
| Acute kidney injury, n (%) | 6 (14.3) | 5 (16.1) | 1 (9.1) | 0.007 | 25.0 (2.46–254.15) |
| LOS (days), median [IQR] | 5.1 [2.7–10.4] | 4.8 [2.2–10.1] | 6 [4.3–12.4] | 0.201 | |
| LOS > median (5.1 days), n (%) | 21 (50.0) | 16 (51.6) | 5 (45.5) | 0.726 | 1.28 (0.32–5.01) |
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Dweck, M.R.; Bularga, A.; Hahn, R.T.; Bing, R.; Lee, K.K.; Chapman, A.R.; White, A.; Salvo, G.D.; Sade, L.E.; Pearce, K.; et al. Global evaluation of echocardiography in patients with COVID-19. Eur. Heart J. Cardiovasc. Imaging 2020, 21, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Szekely, Y.; Lichter, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Gal Oz, A.; Rothschild, E.; Baruch, G.; Peri, Y.; et al. Spectrum of cardiac manifestations in COVID-19: A systematic echocardiographic study. Circulation 2020, 142, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Vignon, P.; Mekontso-Dessap, A.; Tran, S.; Prat, G.; Chew, M.; Balik, M.; Sanfilippo, F.; Banauch, G.; Clau-Terre, F.; et al. Echocardiography findings in COVID-19 patients admitted to intensive care units: A multi-national observational study (the ECHO-COVID study). Intensive Care Med. 2022, 48, 667–678. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Vieillard-Baron, A.; Evrard, B.; Prat, G.; Chew, M.S.; Balik, M.; Clau-Terré, F.; De Backer, D.; Mekontso Dessap, A.; Orde, S.; et al. Echocardiography phenotypes of right ventricular involvement in COVID-19 ARDS patients and ICU mortality: Post-hoc (exploratory) analysis of repeated data from the ECHO-COVID study. Intensive Care Med. 2023, 49, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Task Force for the Management of COVID-19 of the European Society of Cardiology; Baigent, C.; Windecker, S.; Andreini, D.; Arbelo, E.; Barbato, E.; Bartorelli, A.L.; Baumbach, A.; Behr, E.R.; Berti, S.; et al. European Society of Cardiology guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 1—Epidemiology, pathophysiology, and diagnosis. Cardiovasc. Res. 2022, 118, 1385–1412. [Google Scholar] [PubMed]
- Kirkpatrick, J.N.; Mitchell, C.; Taub, C.; Kort, S.; Hung, J.; Swaminathan, M. ASE Statement on Protection of Patients and Echocardiography Service Providers During the 2019 Novel Coronavirus Outbreak: Endorsed by the American College of Cardiology. J. Am. Soc. Echocardiogr. 2020, 33, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Dadon, Z.; Levi, N.; Alpert, E.A.; Orlev, A.; Belman, D.; Glikson, M.; Butnaru, A.; Gottlieb, S. The quality, safety, feasibility, and interpretive accuracy of echocardiographic and lung ultrasound assessment of COVID-19 patients using a hand-held ultrasound. Echocardiography 2022, 39, 886–894. [Google Scholar] [CrossRef] [PubMed]
- McMahon, S.R.; De Francis, G.; Schwartz, S.; Duvall, W.L.; Arora, B.; Silverman, D.I. Tablet-based limited echocardiography to reduce sonographer scan and decontamination time during the COVID-19 pandemic. J. Am. Soc. Echocardiogr. 2020, 33, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Dadon, Z.; Carasso, S.; Gottlieb, S. The Role of Hand-Held Cardiac Ultrasound in Patients with COVID-19. Biomedicines 2023, 11, 239. [Google Scholar] [CrossRef] [PubMed]
- Maheshwarappa, H.M.; Mishra, S.; Kulkarni, A.V.; Gunaseelan, V.; Kanchi, M. Use of handheld ultrasound device with artificial intelligence for evaluation of cardiorespiratory system in COVID-19. Indian J. Crit. Care Med. 2021, 25, 524. [Google Scholar] [PubMed]
- Dadon, Z.; Levi, N.; Orlev, A.; Belman, D.; Alpert, E.A.; Glikson, M.; Gottlieb, S.; Butnaru, A. The utility of handheld cardiac and lung ultrasound in predicting outcomes of hospitalised patients with COVID-19. Can. J. Cardiol. 2022, 38, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Savino, K.; Ambrosio, G. Handheld ultrasound and focused cardiovascular echography: Use and information. Medicina 2019, 55, 423. [Google Scholar] [CrossRef] [PubMed]
- Motazedian, P.; Marbach, J.A.; Prosperi-Porta, G.; Parlow, S.; Di Santo, P.; Abdel-Razek, O.; Jung, R.; Bradford, W.B.; Tsang, M.; Hyon, M.; et al. Diagnostic accuracy of point-of-care ultrasound with artificial intelligence-assisted assessment of left ventricular ejection fraction. NPJ Digit. Med. 2023, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Filipiak-Strzecka, D.; Kasprzak, J.D.; Wejner-Mik, P.; Szymczyk, E.; Wdowiak-Okrojek, K.; Lipiec, P. Artificial intelligence-powered measurement of left ventricular ejection fraction using a handheld ultrasound device. Ultrasound Med. Biol. 2021, 47, 1120–1125. [Google Scholar] [CrossRef] [PubMed]
- Dzieciatkowski, T.; Szarpak, L.; Filipiak, K.J.; Jaguszewski, M.; Ladny, J.R.; Smereka, J. COVID-19 challenge for modern medicine. Cardiol. J. 2020, 27, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, S.; Mosleh, W.; Shen, J.; Chow, C.M. Automation, machine learning, and artificial intelligence in echocardiography: A brave new world. Echocardiography 2018, 35, 1402–1418. [Google Scholar] [CrossRef] [PubMed]
- Asch, F.M.; Mor-Avi, V.; Rubenson, D.; Goldstein, S.; Saric, M.; Mikati, I.; Surette, S.; Chaudhry, A.; Poilvert, N.; Hong, H.; et al. Deep learning–based automated echocardiographic quantification of left ventricular ejection fraction: A point-of-care solution. Circ. Cardiovasc. Imaging 2021, 14, e012293. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Kwan, A.C.; Cho, J.H.; Yuan, N.; Pollick, C.; Shiota, T.; Ebinger, J.; Bello, N.A.; Wei, J.; Josan, K.; et al. Blinded, randomized trial of sonographer versus AI cardiac function assessment. Nature 2023, 616, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Samtani, R.; Bienstock, S.; Lai, A.C.; Liao, S.; Baber, U.; Croft, L.; Stern, E.; Beerkens, F.; Ting, P.; Goldman, M.E. Assessment and validation of a novel fast fully automated artificial intelligence left ventricular ejection fraction quantification software. Echocardiography 2022, 39, 473–482. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dadon, Z.; Steinmetz, Y.; Levi, N.; Orlev, A.; Belman, D.; Butnaru, A.; Carasso, S.; Glikson, M.; Alpert, E.A.; Gottlieb, S. Artificial Intelligence-Powered Left Ventricular Ejection Fraction Analysis Using the LVivoEF Tool for COVID-19 Patients. J. Clin. Med. 2023, 12, 7571. https://doi.org/10.3390/jcm12247571
Dadon Z, Steinmetz Y, Levi N, Orlev A, Belman D, Butnaru A, Carasso S, Glikson M, Alpert EA, Gottlieb S. Artificial Intelligence-Powered Left Ventricular Ejection Fraction Analysis Using the LVivoEF Tool for COVID-19 Patients. Journal of Clinical Medicine. 2023; 12(24):7571. https://doi.org/10.3390/jcm12247571
Chicago/Turabian StyleDadon, Ziv, Yoed Steinmetz, Nir Levi, Amir Orlev, Daniel Belman, Adi Butnaru, Shemy Carasso, Michael Glikson, Evan Avraham Alpert, and Shmuel Gottlieb. 2023. "Artificial Intelligence-Powered Left Ventricular Ejection Fraction Analysis Using the LVivoEF Tool for COVID-19 Patients" Journal of Clinical Medicine 12, no. 24: 7571. https://doi.org/10.3390/jcm12247571
APA StyleDadon, Z., Steinmetz, Y., Levi, N., Orlev, A., Belman, D., Butnaru, A., Carasso, S., Glikson, M., Alpert, E. A., & Gottlieb, S. (2023). Artificial Intelligence-Powered Left Ventricular Ejection Fraction Analysis Using the LVivoEF Tool for COVID-19 Patients. Journal of Clinical Medicine, 12(24), 7571. https://doi.org/10.3390/jcm12247571