
Myocardial Work Assessment in Patients after Coronary Artery Bypass Grafting during Cardiac Rehabilitation
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Cardiac Rehabilitation Program, Six-Minute Walk Test, and Borg Scale
2.3. Echocardiographic Examination and Myocardial Work Analysis
2.4. Statistical Analysis
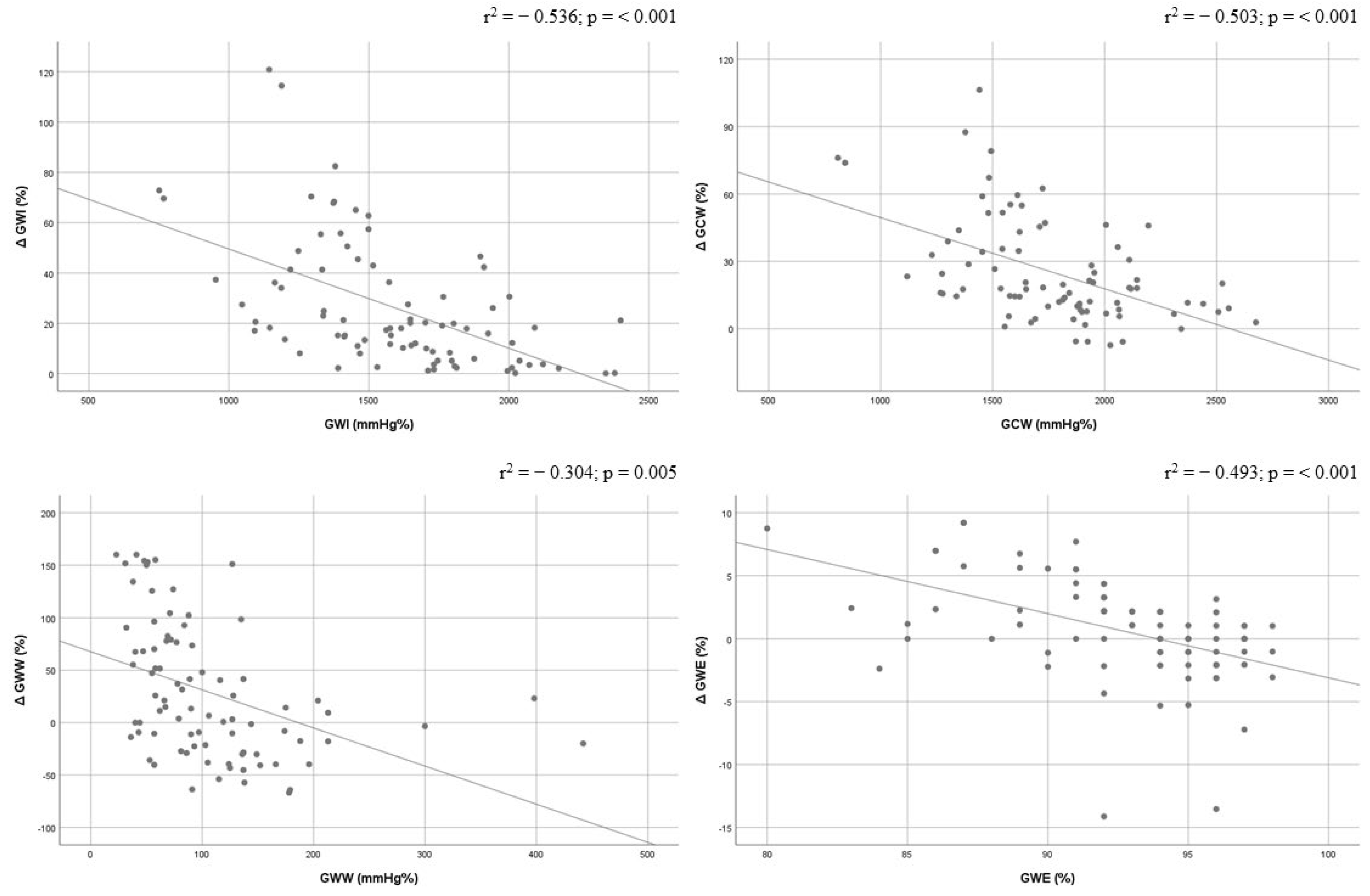
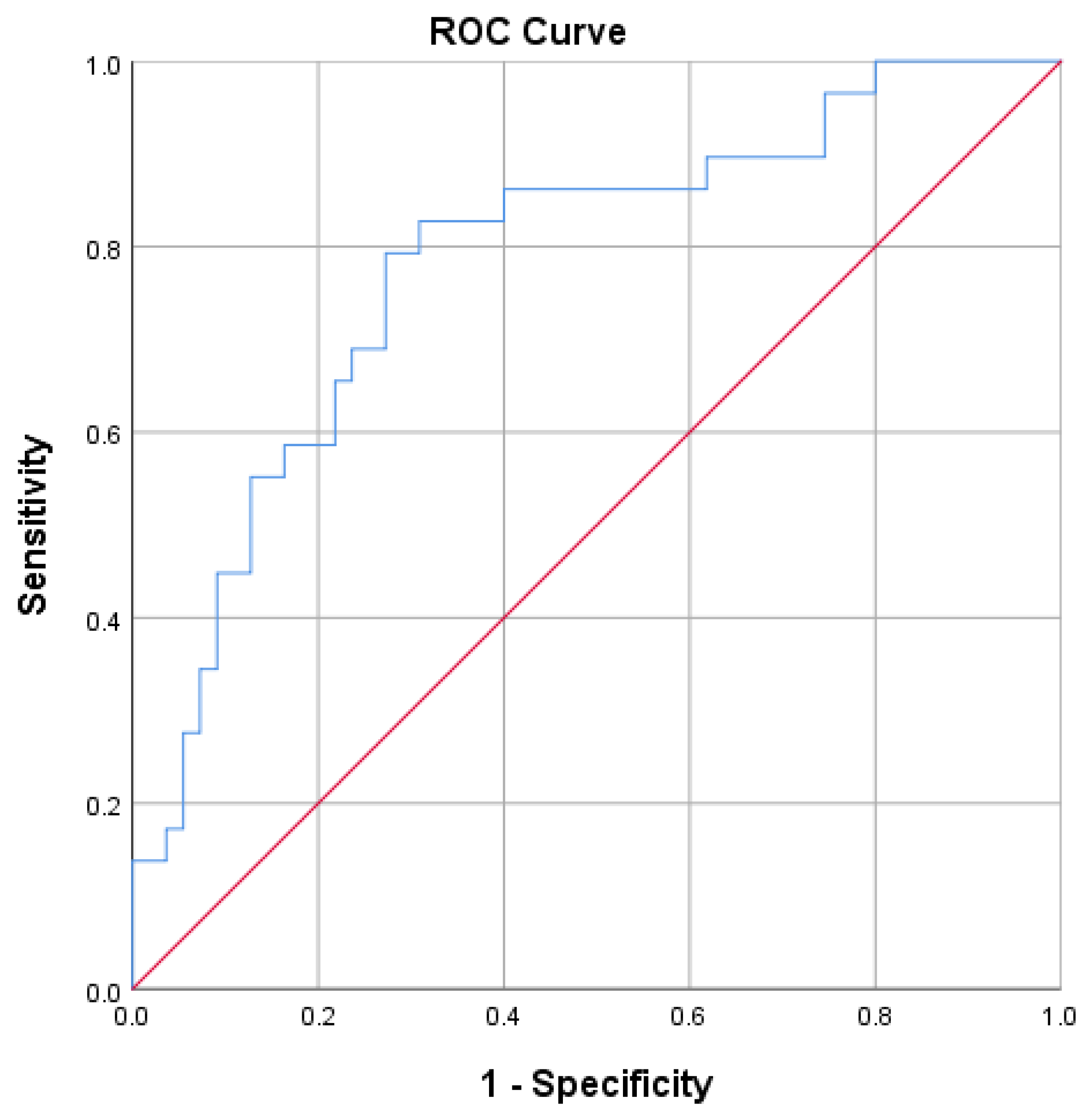
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Ilardi, F.; Sugimoto, T.; Robinet, S.; Cimino, S.; Go, Y.Y.; Bernard, A.; Kacharava, G.; et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270, Erratum in Eur. Heart J. Cardiovasc. Imaging 2016, 17, 412; Erratum in Eur. Heart J. Cardiovasc. Imaging 2016, 17, 969. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Smiseth, O.A.; Donal, E.; Penicka, M.; Sletten, O.J. How to measure left ventricular myocardial work by pressure-strain loops. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 259–261. [Google Scholar] [CrossRef]
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; Iliou, M.C.; Pedretti, R.F.E.; Schmid, J.P.; Vigorito, C.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: From knowledge to implementation. 2020 update. A position paper from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2021, 28, 460–495. [Google Scholar] [CrossRef] [PubMed]
- Rauch, B.; Davos, C.H.; Doherty, P.; Saure, D.; Metzendorf, M.I.; Salzwedel, A.; Völler, H.; Jensen, K.; Schmid, J.P.; the ‘Cardiac Rehabilitation Section’, European Association of Preventive Cardiology (EAPC), in cooperation with the Institute of Medical Biometry and Informatics (IMBI), Department of Medical Biometry, University of Heidelberg, and the Cochrane Metabolic and Endocrine Disorders Group, Institute of General Practice, Heinrich-Heine University, Düsseldorf, Germany. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies—The Cardiac Rehabilitation Outcome Study (CROS). Eur. J. Prev. Cardiol. 2016, 23, 1914–1939. [Google Scholar] [CrossRef] [PubMed]
- Salzwedel, A.; Jensen, K.; Rauch, B.; Doherty, P.; Metzendorf, M.I.; Hackbusch, M.; Völler, H.; Schmid, J.P.; Davos, C.H. Effectiveness of comprehensive cardiac rehabilitation in coronary artery disease patients treated according to contemporary evidence based medicine: Update of the Cardiac Rehabilitation Outcome Study (CROS-II). Eur. J. Prev. Cardiol. 2020, 27, 1756–1774. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477, Erratum in Eur. Heart J. 2020, 41, 4242. [Google Scholar] [CrossRef]
- Ilardi, F.; D’Andrea, A.; D’Ascenzi, F.; Bandera, F.; Benfari, G.; Esposito, R.; Malagoli, A.; Mandoli, G.E.; Santoro, C.; Russo, V.; et al. Myocardial Work by Echocardiography: Principles and Applications in Clinical Practice. J. Clin. Med. 2021, 10, 4521. [Google Scholar] [CrossRef]
- Amzulescu, M.S.; De Craene, M.; Langet, H.; Pasquet, A.; Vancraeynest, D.; Pouleur, A.C.; Vanoverschelde, J.L.; Gerber, B.L. Myocardial strain imaging: Review of general principles, validation, and sources of discrepancies. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Perone, F.; Bernardi, M.; Redheuil, A.; Mafrica, D.; Conte, E.; Spadafora, L.; Ecarnot, F.; Tokgozoglu, L.; Santos-Gallego, C.G.; Kaiser, S.E.; et al. Role of Cardiovascular Imaging in Risk Assessment: Recent Advances, Gaps in Evidence, and Future Directions. J. Clin. Med. 2023, 12, 5563. [Google Scholar] [CrossRef] [PubMed]
- Sahin, A.A.; Ozben, B.; Sunbul, M.; Yagci, I.; Sayar, N.; Cincin, A.; Gurel, E.; Tigen, K.; Basaran, Y. The effect of cardiac rehabilitation on blood pressure, and on left atrial and ventricular functions in hypertensive patients. J. Clin. Ultrasound 2020, 49, 456–465. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, J.M.; Edwards, J.J.; Wiles, J.D.; Taylor, K.A.; Leeson, P.; Sharma, R. Myocardial work and left ventricular mechanical adaptations following isometric exercise training in hypertensive patients. Eur. J. Appl. Physiol. 2022, 122, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Trachsel, L.D.; David, L.P.; Gayda, M.; Henri, C.; Hayami, D.; Thorin-Trescases, N.; Thorin, É.; Blain, M.A.; Cossette, M.; Lalongé, J.; et al. The impact of high-intensity interval training on ventricular remodeling in patients with a recent acute myocardial infarction—A randomized training intervention pilot study. Clin. Cardiol. 2019, 42, 1222–1231. [Google Scholar] [CrossRef] [PubMed]
- Malfatto, G.; Revera, M.; Branzi, G.; Ciambellotti, F.; Giglio, A.; Blengino, S.; Oldani, M.; Facchini, C.; Parati, G.; Facchini, M. A brief period of intensive cardiac rehabilitation improves global longitudinal strain and diastolic function after a first uncomplicated myocardial infarction. Acta Cardiol. 2017, 72, 284–291. [Google Scholar] [CrossRef]
- Van De Heyning, C.M.; De Maeyer, C.; Pattyn, N.; Beckers, P.J.; Cornelissen, V.A.; Goetschalckx, K.; Possemiers, N.; Van Craenenbroeck, E.M.; Voigt, J.U.; Vanhees, L.; et al. Impact of aerobic interval training and continuous training on left ventricular geometry and function: A SAINTEX-CAD substudy. Int. J. Cardiol. 2018, 257, 193–198. [Google Scholar] [CrossRef]
- Eser, P.; Trachsel, L.D.; Marcin, T.; Herzig, D.; Freiburghaus, I.; De Marchi, S.; Zimmermann, A.J.; Schmid, J.P.; Wilhelm, M. Short- and Long-Term Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Left Ventricular Remodeling in Patients Early After ST-Segment Elevation Myocardial Infarction-The HIIT-EARLY Randomized Controlled Trial. Front. Cardiovasc. Med. 2022, 9, 869501. [Google Scholar] [CrossRef]
- Cuomo, G.; Iannone, F.P.; Di Lorenzo, A.; Testa, C.; Ciccarelli, M.; Venturini, E.; Cesaro, A.; Pacileo, M.; Tagliamonte, E.; D’Andrea, A.; et al. Potential Role of Global Longitudinal Strain in Cardiac and Oncological Patients Undergoing Cardio-Oncology Rehabilitation (CORE). Clin. Pract. 2023, 13, 384–397. [Google Scholar] [CrossRef]
- D’Andrea, A.; Carbone, A.; Ilardi, F.; Pacileo, M.; Savarese, C.; Sperlongano, S.; Di Maio, M.; Giallauria, F.; Russo, V.; Bossone, E.; et al. Effects of High Intensity Interval Training Rehabilitation Protocol after an Acute Coronary Syndrome on Myocardial Work and Atrial Strain. Medicina 2022, 58, 453. [Google Scholar] [CrossRef]
- Hansen, D.; Abreu, A.; Ambrosetti, M.; Cornelissen, V.; Gevaert, A.; Kemps, H.; Laukkanen, J.A.; Pedretti, R.; Simonenko, M.; Wilhelm, M.; et al. Exercise intensity assessment and prescription in cardiovascular rehabilitation and beyond: Why and how: A position statement from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 230–245. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117, Erratum in Am. J. Respir. Crit. Care Med. 2016, 193, 1185. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Tsang, W.; Adams, D.H.; Agricola, E.; Buck, T.; Faletra, F.F.; Franke, A.; Hung, J.; de Isla, L.P.; et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. J. Am. Soc. Echocardiogr. 2012, 25, 3–46. [Google Scholar] [CrossRef]
- Moya, A.; Buytaert, D.; Penicka, M.; Bartunek, J.; Vanderheyden, M. State-of-the-Art: Noninvasive Assessment of Left Ventricular Function Through Myocardial Work. J. Am. Soc. Echocardiogr. 2023, 36, 1027–1042. [Google Scholar] [CrossRef]
- Marzlin, N.; Hays, A.G.; Peters, M.; Kaminski, A.; Roemer, S.; O’Leary, P.; Kroboth, S.; Harland, D.R.; Khandheria, B.K.; Tajik, A.J.; et al. Myocardial Work in Echocardiography. Circ. Cardiovasc. Imaging 2023, 16, e014419. [Google Scholar] [CrossRef]
- Antoni, M.L.; Mollema, S.A.; Atary, J.Z.; Borleffs, C.J.; Boersma, E.; van de Veire, N.R.; Holman, E.R.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J. Time course of global left ventricular strain after acute myocardial infarction. Eur. Heart J. 2010, 31, 2006–2013. [Google Scholar] [CrossRef]
- Qin, Y.; Wu, X.; Wang, J.; Li, Y.; Ding, X.; Guo, D.; Jiang, Z.; Zhu, W.; Cai, Q.; Lu, X. Value of territorial work efficiency estimation in non-ST-segment-elevation acute coronary syndrome: A study with non-invasive left ventricular pressure-strain loops. Int. J. Cardiovasc. Imaging 2021, 37, 1255–1265. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Abdani, S.; Stracchi, V.; Elmkies, F.; Boulanger, J.; Botoro, T.; Zemir, H.; Clerc, J. Usefulness of Noninvasive Myocardial Work to Predict Left Ventricular Recovery and Acute Complications after Acute Anterior Myocardial Infarction Treated by Percutaneous Coronary Intervention. J. Am. Soc. Echocardiogr. 2020, 33, 1180–1190. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, S.; Spadafora, L.; Bernardi, M.; Galli, M.; Betti, M.; Perone, F.; Nicolaio, G.; Marzetti, E.; Martone, A.M.; Landi, F.; et al. Management of Coronary Artery Disease in Older Adults: Recent Advances and Gaps in Evidence. J. Clin. Med. 2023, 12, 5233. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165, Erratum in Eur. Heart J. 2019, 40, 3096. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dibben, G.; Faulkner, J.; Oldridge, N.; Rees, K.; Thompson, D.R.; Zwisler, A.D.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2021, 11, CD001800. [Google Scholar] [CrossRef]
- de Vries, H.; Kemps, H.M.; van Engen-Verheul, M.M.; Kraaijenhagen, R.A.; Peek, N. Cardiac rehabilitation and survival in a large representative community cohort of Dutch patients. Eur. Heart J. 2015, 36, 1519–1528. [Google Scholar] [CrossRef]
- Sumin, A.N.; Oleinik, P.A.; Bezdenezhnykh, A.V.; Bezdenezhnykh, N.A. Factors Determining the Functional State of Cardiac Surgery Patients with Complicated Postoperative Period. Int. J. Environ. Res. Public. Health 2022, 19, 4329. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (n = 84) |
|---|---|
| Age, years | 67.96 ± 7.42 |
| Male sex, n (%) | 66 (78.6) |
| BSA, m2 | 1.83 ± 0.17 |
| BMI, kg/m2 | 26.93 (25–29) |
| Arterial hypertension, n (%) | 69 (82.1) |
| Type 2 diabetes mellitus, n (%) | 39 (46.4) |
| Hypercholesterolemia, n (%) | 58 (69) |
| Hypertriglyceridemia, n (%) | 5 (6) |
| Active smoker, n (%) | 19 (22.6) |
| Past smoker, n (%) | 34 (40.5) |
| Previous myocardial infarction, n (%) | 18 (21.4) |
| STEMI, n (%) | 4 (4.8) |
| NSTEMI, n (%) | 17 (20.2) |
| Unstable angina, n (%) | 3 (3.6) |
| Chronic coronary syndrome, n (%) | 60 (71.4) |
| Coronary artery bypass graft surgery
• One, n (%) • Two, n (%) • Three, n (%) • Four, n (%) | 15 (17.9) 41 (48.8) 26 (31) 2 (2.4) |
| Concomitant other cardiac surgery
• Mitral valve surgery, n (%) • Aortic valve surgery, n (%) | 3 (3.6) 15 (17.9) |
| Aspirin, n (%) | 60 (71.4) |
| Dual antiplatelet therapy, n (%) | 24 (28.6) |
| Anticoagulants, n (%) | 9 (10.7) |
| ACE-inhibitors or AT-receptor antagonists, n (%) | 62 (73.8) |
| Beta-blockers, n (%) | 79 (94) |
| Mineralocorticoid receptor antagonists, n (%) | 61 (72.6) |
| Statins, n (%) | 69 (82.1) |
| Loop diuretics, n (%) | 72 (85.7) |
| Six-minute walk test, meters | 70.71 ± 40.2 |
| Variable | Total (n = 84) |
|---|---|
| Heart rate (bpm) | 78.8 ± 13.13 |
| Systolic blood pressure (mmHg) | 118.45 ± 17.58 |
| Diastolic blood pressure (mmHg) | 67.8 ± 6.78 |
| LVEDD (cm) | 4.28 ± 0.6 |
| LVESD (cm) | 2.56 ± 0.55 |
| LV mass index (g/m2) | 98.29 ± 2.6 |
| LVEDV index (mL/m2) | 28.08 (23.18–37.37) |
| LVESV index (mL/m2) | 11.55 (8.77–15.9) |
| 2D LV ejection fraction (%) | 60.58 ± 5.26 |
| 3D LV ejection fraction (%) | 60.49 ± 4.84 |
| Global longitudinal strain (%) | −16.18 ± 2.55 |
| Global work index (mmHg%) | 1588.56 ± 345 |
| Global constructive work (mmHg%) | 1771.27 ± 366.36 |
| Global wasted work (mmHg%) | 105.8 ± 72.02 |
| Global work efficiency (%) | 92.63 ± 3.9 |
| LAV index (mL/m2) | 31.54 (27.59–38.38) |
| Stroke volume (mL) | 60.05 ± 19.44 |
| Parameter | Before Cardiac Rehabilitation | After Cardiac Rehabilitation | p-Value |
|---|---|---|---|
| 2D left ventricle ejection fraction (%) | 60.58 ± 5.26 | 62 ± 5.13 | <0.001 |
| 3D left ventricle ejection fraction (%) | 60.49 ± 4.49 | 62.17 ± 4.67 | 0.001 |
| Global longitudinal strain (%) | −16.17 ± 2.55 | −18.27 ± 2.39 | <0.001 |
| Global work index (mmHg%) | 1588.56 ± 345 | 1960.2 ± 377.03 | <0.001 |
| Global constructive work (mmHg%) | 1771.27 ± 366.36 | 2172.01 ± 418.73 | <0.001 |
| Global wasted work (mmHg%) | 105.8 ± 72.02 | 117.36 ± 74.92 | 0.067 |
| Global work efficiency (%) | 92.63 ± 3.9 | 93.15 ± 7.13 | 0.196 |
| Six-minute walk test (meters) | 70.71 ± 40.2 | 437.5 ± 108.70 | <0.001 |
| Parameter | Δ% |
|---|---|
| Global work index (%) | 26.32 ± 25.38 |
| Global constructive work (%) | 25 ± 23.09 |
| Global wasted work (%) | 23.52 ± 72.14 |
| Global work efficiency (%) | 0.65 ± 4.04 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perone, F.; Ancona, R.; di Stasio, F.; La Gambina, V.; Comenale Pinto, S. Myocardial Work Assessment in Patients after Coronary Artery Bypass Grafting during Cardiac Rehabilitation. J. Clin. Med. 2023, 12, 7540. https://doi.org/10.3390/jcm12247540
Perone F, Ancona R, di Stasio F, La Gambina V, Comenale Pinto S. Myocardial Work Assessment in Patients after Coronary Artery Bypass Grafting during Cardiac Rehabilitation. Journal of Clinical Medicine. 2023; 12(24):7540. https://doi.org/10.3390/jcm12247540
Chicago/Turabian StylePerone, Francesco, Roberta Ancona, Fausto di Stasio, Vito La Gambina, and Salvatore Comenale Pinto. 2023. "Myocardial Work Assessment in Patients after Coronary Artery Bypass Grafting during Cardiac Rehabilitation" Journal of Clinical Medicine 12, no. 24: 7540. https://doi.org/10.3390/jcm12247540
APA StylePerone, F., Ancona, R., di Stasio, F., La Gambina, V., & Comenale Pinto, S. (2023). Myocardial Work Assessment in Patients after Coronary Artery Bypass Grafting during Cardiac Rehabilitation. Journal of Clinical Medicine, 12(24), 7540. https://doi.org/10.3390/jcm12247540