
Alveolar Bone Grafting in Unilateral Cleft Lip and Palate: Impact of Timing on Palatal Shape

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
2.2. Treatment Protocol
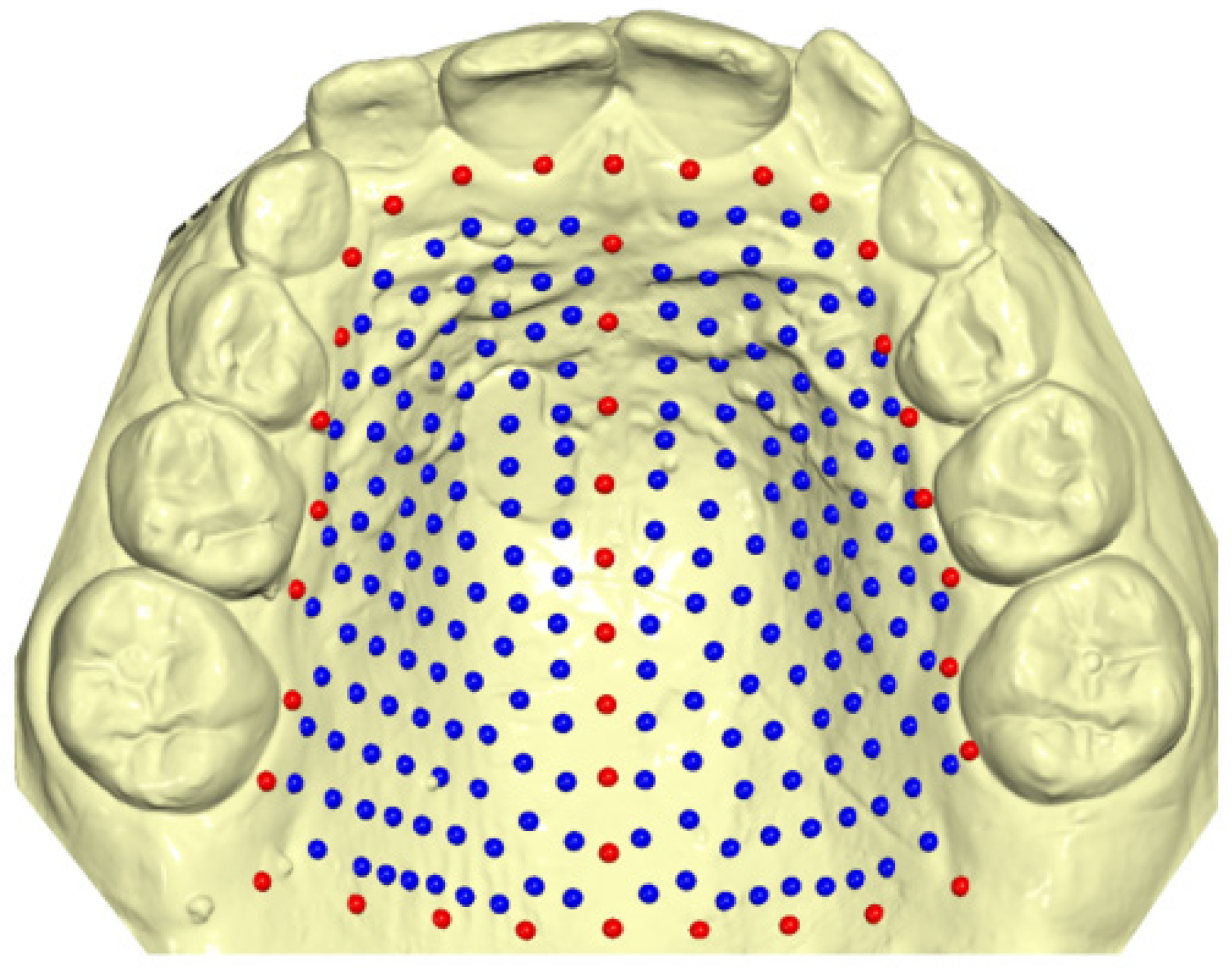
2.3. Evaluation Methods
2.4. Statistical Analysis
3. Results
3.1. Demographic Data and Method Error
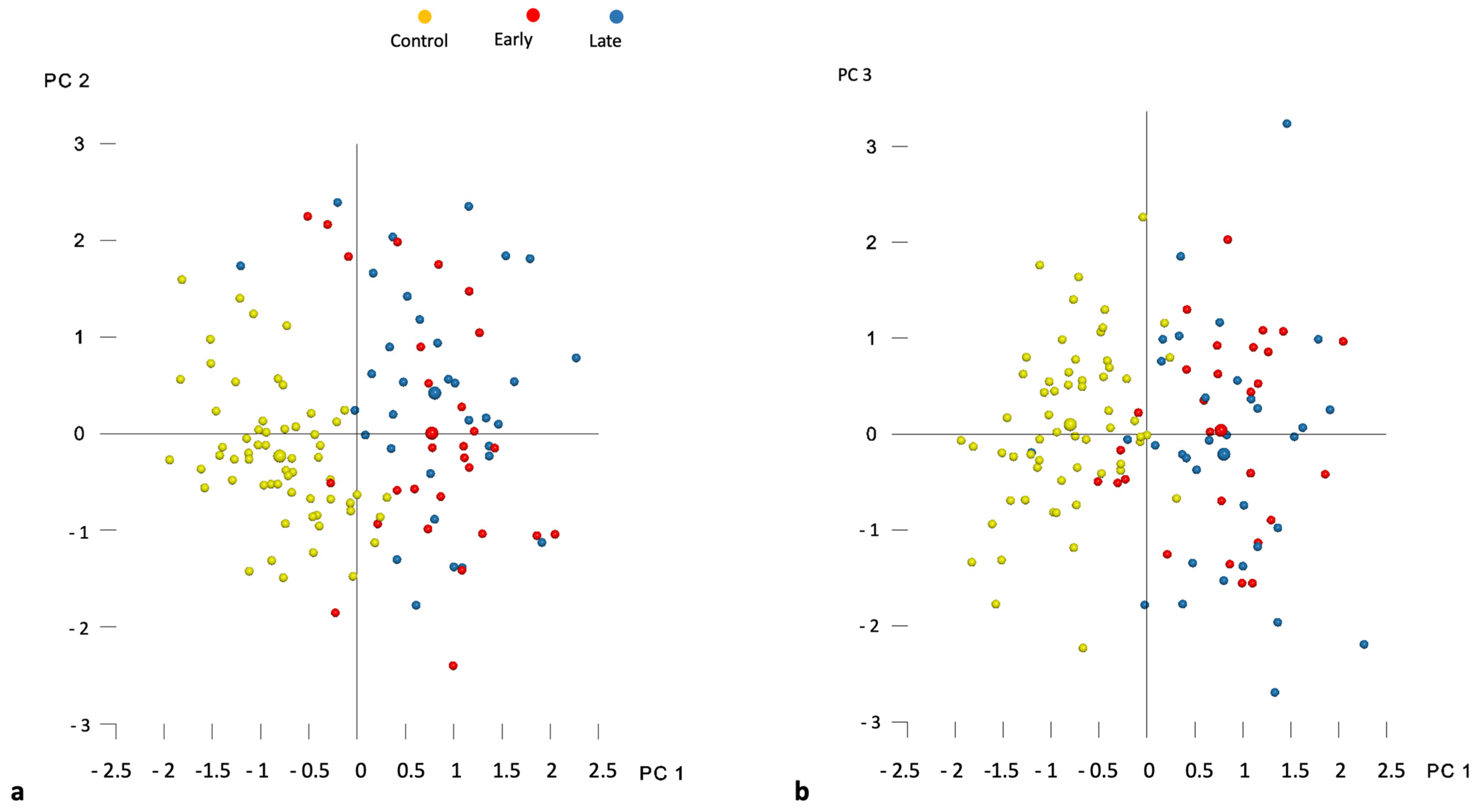
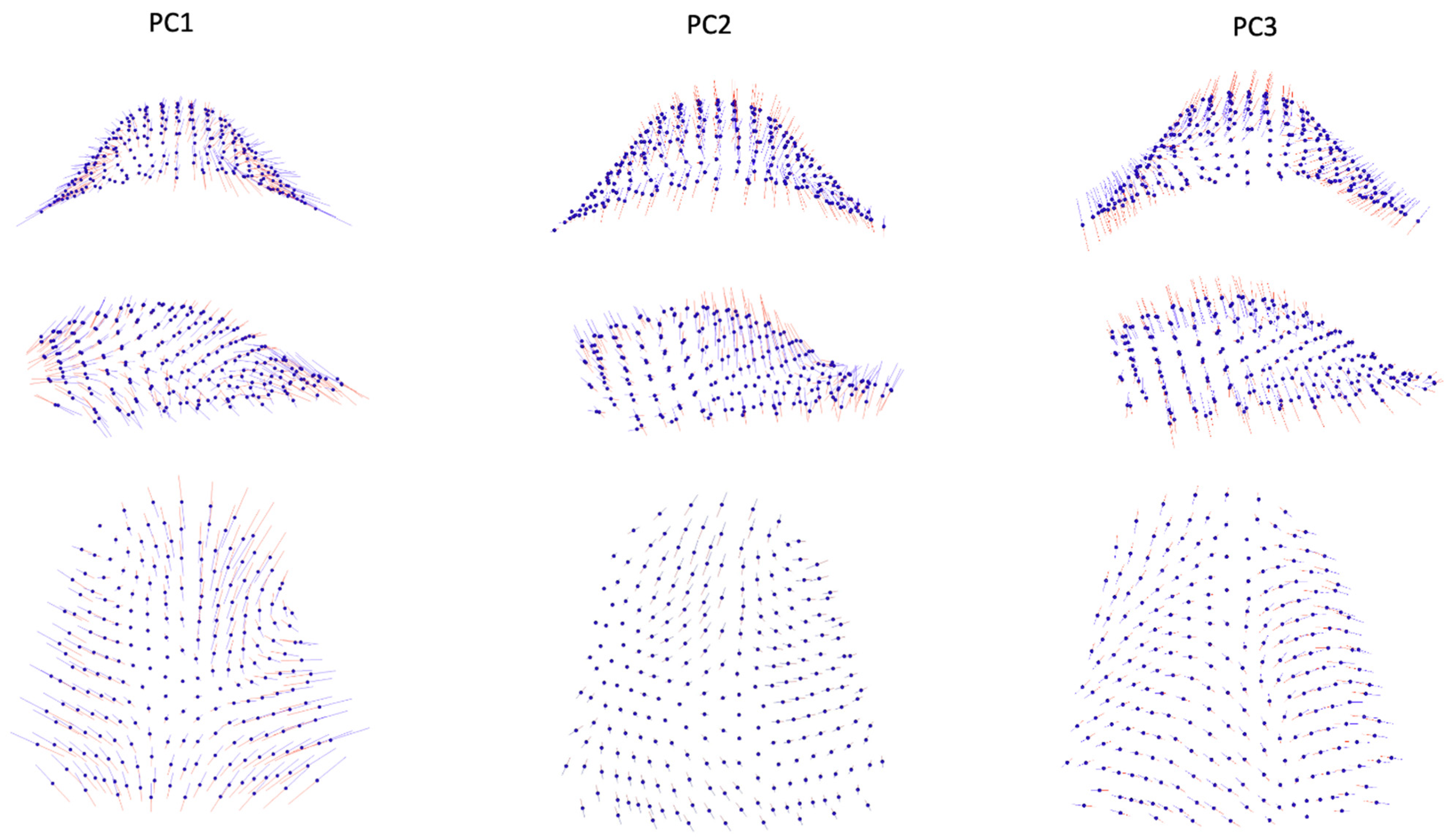
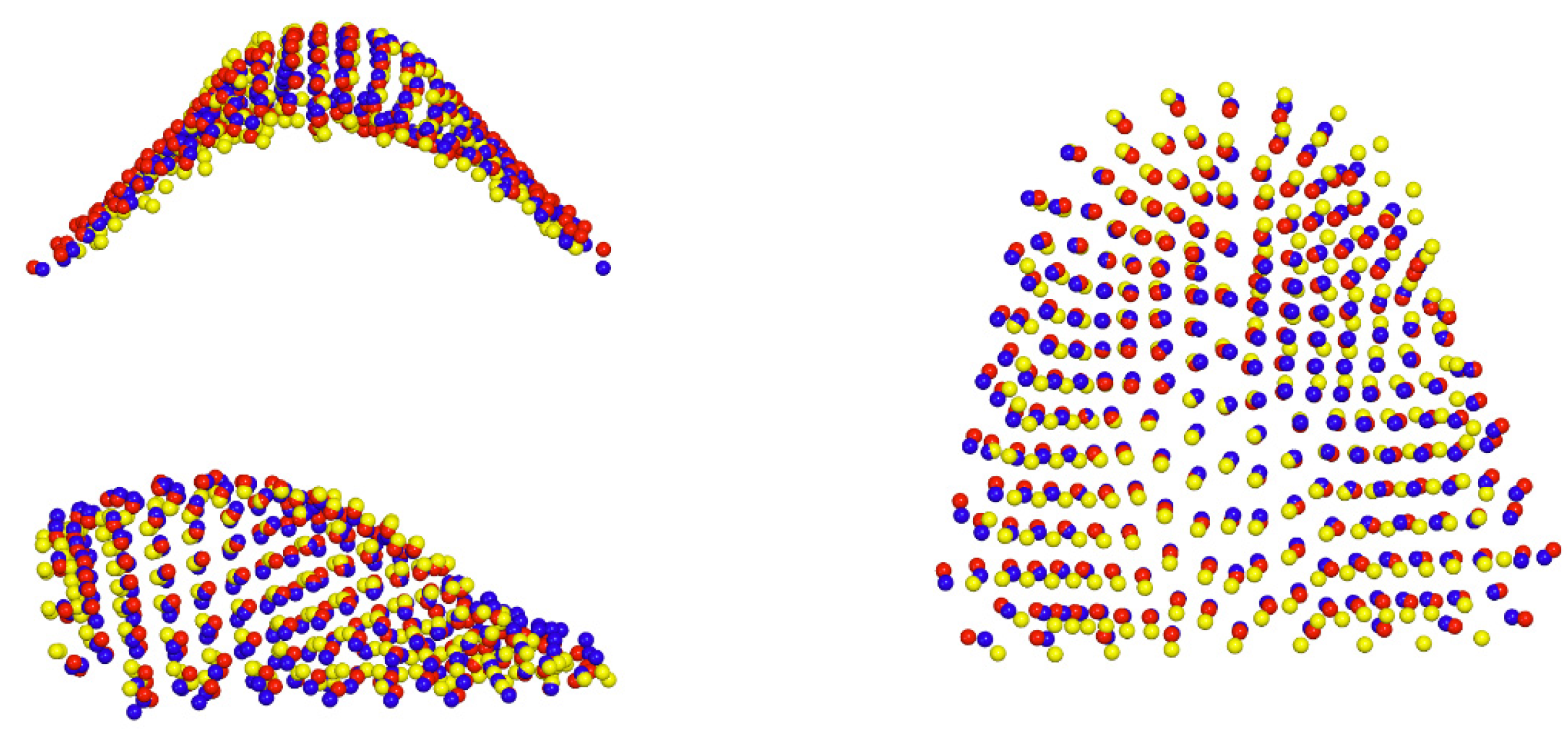
3.2. Procrustes Superimposition and PCA
3.3. Intergroup Differences
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carbullido, M.K.; Dean, R.A.; Kamel, G.N.; Davis, G.L.; Hornacek, M.; Segal, R.M.; Ewing, E.; Lance, S.H.; Gosman, A.A. Long-Term Treatment Outcomes of Primary Alveolar Bone Grafts for Alveolar Clefts: A Qualitative Systematic Review. Cleft Palate-Craniofac. J. 2022, 59, 86–97. [Google Scholar] [CrossRef]
- Padwa, B.L. Alveolar Bone Graft Surgery. In Cleft and Craniofacial Orthodontics; Shatye, P.R., Gibson, T.L., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2023; pp. 333–345. [Google Scholar]
- Boyne, P.J.; Sands, N.R. Combined Orthodontic-Surgical Management of Residual Palato-Alveolar Cleft Defects. Am. J. Orthod. 1976, 70, 20–37. [Google Scholar] [CrossRef]
- Vig, K.W. Alveolar Bone Grafts: The Surgical/Orthodontic Management of the Cleft Maxilla. Ann. Acad. Med. Singap. 1999, 28, 721–727. [Google Scholar]
- Weissler, E.H.; Paine, K.M.; Ahmed, M.K.; Taub, P.J. Alveolar Bone Grafting and Cleft Lip and Palate: A Review. Plast. Reconstr. Surg. 2016, 138, 1287–1295. [Google Scholar] [CrossRef]
- McCrary, H.; Skirko, J.R. Bone Grafting of Alveolar Clefts. Oral. Maxillofac. Surg. Clin. N. Am. 2021, 33, 231–238. [Google Scholar] [CrossRef]
- Qamar, F.; Cray, J.J.; Halsey, J.; Rottgers, S.A. A Survey of Bone Grafting Practice Patterns in North American Cleft Surgeons. Cleft Palate Craniofac. J. 2023, 60, 1366–1375. [Google Scholar] [CrossRef]
- Kannan, P.; Verma, S.; Kumar, V.; Kumar Verma, R.; Pal Singh, S. Effects of Secondary Alveolar Bone Grafting on Maxillary Growth in Cleft Lip or Palate Patients: A Systematic Review and Meta-Analysis. Cleft Palate Craniofac. J. 2023, 12, 10556656231188600. [Google Scholar] [CrossRef] [PubMed]
- Brudnicki, A.; Sawicka, E.; Fudalej, P.S. Maxillofacial Morphology in Post-Pubertal Patients with Unilateral Cleft Lip and Palate Following Early vs. Late Secondary Alveolar Bone Grafting. J. Craniomaxillofac Surg. 2021, 49, 809–814. [Google Scholar] [CrossRef]
- Doucet, J.-C.; Russell, K.A.; Daskalogiannakis, J.; Mercado, A.M.; Emanuele, N.; James, L.; Hathaway, R.R.; Long, R.E. Facial Growth of Patients with Complete Unilateral Cleft Lip and Palate Treated with Alveolar Bone Grafting at 6 Years. Cleft Palate Craniofac. J. 2019, 56, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Lowry, C.H.; Long, R.E.; Russell, K.; Giltner, J.Q.; Weaver, L.; Mercado, A.M.; Beals, S.; Beals, P.; Daskalogiannakis, J.; Hathaway, R.R.; et al. The Effect of Earlier Bone Grafting, Prior to Orthodontic Treatment, on SWAG Ratings of Graft Outcomes. Cleft Palate Craniofac. J. 2021, 58, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Doucet, J.-C.; Russell, K.A.; Daskalogiannakis, J.; Mercado, A.M.; Hathaway, R.R.; Semb, G.; Shaw, W.C.; Long, R.E. Early Secondary Alveolar Bone Grafting and Facial Growth of Patients with Complete Unilateral Cleft Lip and Palate. Cleft Palate Craniofac. J. 2023, 60, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Brudnicki, A.; Sawicka, E.; Brudnicka, R.; Fudalej, P.S. Effects of Different Timing of Alveolar Bone Graft on Craniofacial Morphology in Unilateral Cleft Lip and Palate. Cleft Palate Craniofac. J. 2020, 57, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Meazzini, M.C.; Tortora, C.; Morabito, A.; Garattini, G.; Brusati, R. Alveolar Bone Formation in Patients with Unilateral and Bilateral Cleft Lip and Palate after Early Secondary Gingivoalveoloplasty: Long-Term Results. Plast. Reconstr. Surg. 2007, 119, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Meazzini, M.C.; Capasso, E.; Morabito, A.; Garattini, G.; Brusati, R. Comparison of Growth Results in Patients with Unilateral Cleft Lip and Palate after Early Secondary Gingivoalveoloplasty and Secondary Bone Grafting: 20 Years Follow up. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2008, 42, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Brusati, R.; Meazzini, M.C.; Rezzonico, A.; Biglioli, F.; Garattini, G.; Battista, V.M.A.; Autelitano, L. Evaluation of a Sample of Patients with Unilateral Cleft Lip and Palate Treated with a Two-Stage Protocol. J. Craniofac. Surg. 2018, 29, 2058–2064. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, H.P.; Longaker, M.T. In Utero Surgery for Cleft Lip/Palate: Minimizing the “Ripple Effect” of Scarring. J. Craniofac. Surg. 2003, 14, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, A.; Bell, A.; Simmons, D.; Bowman, A.; Brown, D.; Lo, T.-W.; Xiao, Y. 3D Assessment of Lip Scarring and Residual Dysmorphology Following Surgical Repair of Cleft Lip and Palate: A Preliminary Study. Cleft Palate Craniofac. J. 2011, 48, 379–387. [Google Scholar] [CrossRef]
- Von Den Hoff, J.W.; Ongkosuwito, E.M.; Kuijpers-Jagtman, A.M.; Wagener, F.A.D.T.G.; Latif, A.; Kuijpers, M.A.R.; Carvajal Monroy, P.L. Vom Nutzen der Chirurgie und vom Nachteil der Narben [The Benefit of Surgery and the Drawback of Scars]. Inf. Orthod. Kieferorthop. 2017, 49, 286–294. [Google Scholar] [CrossRef]
- Yew, C.C.; Alam, M.K.; Rahman, S.A. Multivariate Analysis on Unilateral Cleft Lip and Palate Treatment Outcome by EUROCRAN Index: A Retrospective Study. Int. J. Pediatr. Otorhinolaryngol. 2016, 89, 42–49. [Google Scholar] [CrossRef]
- Brudnicki, A.; Regulski, P.A.; Sawicka, E.; Fudalej, P.S. Alveolar Volume Following Different Timings of Secondary Bone Grafting in Patients with Unilateral Cleft Lip and Palate. A Pilot Study. J. Clin. Med. 2021, 10, 3524. [Google Scholar] [CrossRef]
- Klingenberg, C.P. Size, Shape, and Form: Concepts of Allometry in Geometric Morphometrics. Dev. Genes. Evol. 2016, 226, 113–137. [Google Scholar] [CrossRef]
- Mitteroecker, P.; Schaefer, K. Thirty Years of Geometric Morphometrics: Achievements, Challenges, and the Ongoing Quest for Biological Meaningfulness. Am. J. Biol. Anthropol. 2022, 178 (Suppl. S74), 181–210. [Google Scholar] [CrossRef] [PubMed]
- Dao, A.M.; Goudy, S.L. Cleft Palate Repair, Gingivoperiosteoplasty, and Alveolar Bone Grafting. Facial Plast. Surg. Clin. N. Am. 2016, 24, 467–476. [Google Scholar] [CrossRef]
- Bittermann, G.K.P.; de Ruiter, A.P.; Bittermann, A.J.; Mink van de Molen, A.B.; van Es, R.J.; Koole, R.; Rosenberg, A.J. Midfacial Growth and Dental Arch Relationships in Bilateral Cleft Palate Following Secondary Alveolar Bone Grafting and Orthodontic Intervention: Factors Predicting a Le Fort I Osteotomy at Age 18. J. Craniomaxillofac Surg. 2018, 46, 1764–1771. [Google Scholar] [CrossRef] [PubMed]
- Forsetlund, L.; Semb, G.; Farah, M.G.; Flottorp, S. The Scientific Knowledge Base for Treatment of Patients with Cleft Lip, Alveolus and Palate; NIPH Systematic Reviews: Executive Summaries; Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH): Oslo, Norway, 2009; ISBN 978-82-8121-312-8.
- Mink van der Molen, A.B.; van Breugel, J.M.M.; Janssen, N.G.; Admiraal, R.J.C.; van Adrichem, L.N.A.; Bierenbroodspot, F.; Bittermann, D.; van den Boogaard, M.-J.H.; Broos, P.H.; Dijkstra-Putkamer, J.J.M.; et al. Clinical Practice Guidelines on the Treatment of Patients with Cleft Lip, Alveolus, and Palate: An Executive Summary. J. Clin. Med. 2021, 10, 4813. [Google Scholar] [CrossRef] [PubMed]
- Yver, C.M.; Chorath, K.T.; Connolly, J.; Shah, M.; Majmudar, T.; Moreira, A.G.; Rajasekaran, K. Clinical Practice Guidelines for the Management of Patients with Cleft Lip and Palate: A Systematic Quality Appraisal Using the Appraisal of Guidelines for Research and Evaluation II Instrument. J. Craniofac. Surg. 2022, 33, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Fudalej, P.; Janiszewska-Olszowska, J.; Wedrychowska-Szulc, B.; Katsaros, C. Early Alveolar Bone Grafting Has a Negative Effect on Maxillary Dental Arch Dimensions of Pre-School Children with Complete Unilateral Cleft Lip and Palate: Effects of Early Alveolar Bone Grafting. Orthod. Craniofac. Res. 2011, 14, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, F.H.D.S.L.; Drummond, R.J.; Frota, C.M.; Bartzela, T.N.; Dos Santos, P.B. Comparison of Early and Conventional Autogenous Secondary Alveolar Bone Graft in Children with Cleft Lip and Palate: A Systematic Review. Orthod. Craniofac. Res. 2020, 23, 385–397. [Google Scholar] [CrossRef]
- Rusková, H.; Bejdová, Š.; Peterka, M.; Krajíček, V.; Velemínská, J. 3-D Shape Analysis of Palatal Surface in Patients with Unilateral Complete Cleft Lip and Palate. J. Cranio-Maxillofac. Surg. 2014, 42, e140–e147. [Google Scholar] [CrossRef]
- Patrícia Bittencourt Dutra, D.S.; Janson, G.; Assis, V.H.; De Paula Leite Battisti, M.; Garib, D.G. Association between Dental Arch Widths and Interarch Relationships in Children with Operated Unilateral Complete Cleft Lip and Palate. Cleft Palate Craniofac. J. 2015, 52, 196–200. [Google Scholar] [CrossRef]
- Generali, C.; Primozic, J.; Richmond, S.; Bizzarro, M.; Flores-Mir, C.; Ovsenik, M.; Perillo, L. Three-Dimensional Evaluation of the Maxillary Arch and Palate in Unilateral Cleft Lip and Palate Subjects Using Digital Dental Casts. Eur. J. Orthod. 2017, 39, 641–645. [Google Scholar] [CrossRef]
- Primožič, J.; Perinetti, G.; Richmond, S.; Ovsenik, M. Three-Dimensional Longitudinal Evaluation of Palatal Vault Changes in Growing Subjects. Angle Orthod. 2012, 82, 632–636. [Google Scholar] [CrossRef]
- Yang, S.-T.; Kim, H.-K.; Lim, Y.S.; Chang, M.-S.; Lee, S.-P.; Park, Y.-S. A Three Dimensional Observation of Palatal Vault Growth in Children Using Mixed Effect Analysis: A 9 Year Longitudinal Study. Eur. J. Orthod. 2013, 35, 832–840. [Google Scholar] [CrossRef] [PubMed]
- Shafer, D.M. Secondary Bone Grafting for Unilateral Alveolar Clefts: A Review of Surgical Techniques. Atlas Oral. Maxillofac. Surg. Clin. N. Am. 1995, 3, 29–42. [Google Scholar] [CrossRef]
- Junn, A.; Dinis, J.; Lu, X.; Lopez, J.; Steinbacher, D. Alveolar Bone Grafting and Fistula Closure. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4207. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.S.; Jackson, I.T.; Christie, F.B. Improvement in Speech Following Closure of Anterior Palatal Fistulas with Bone Grafts. Br. J. Plast. Surg. 1976, 29, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Bureau, S.; Penko, M.; McFadden, L. Speech Outcome after Closure of Oronasal Fistulas with Bone Grafts. J. Oral. Maxillofac. Surg. 2001, 59, 1408–1413, discussion 1413–1414. [Google Scholar] [CrossRef] [PubMed]
- Semb, G.; Brattström, V.; Mølsted, K.; Prahl-Andersen, B.; Shaw, W.C. The Eurocleft Study: Intercenter Study of Treatment Outcome in Patients with Complete Cleft Lip and Palate. Part 1: Introduction and Treatment Experience. Cleft Palate Craniofac. J. 2005, 42, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Brattström, V.; Mølsted, K.; Prahl-Andersen, B.; Semb, G.; Shaw, W.C. The Eurocleft Study: Intercenter Study of Treatment Outcome in Patients with Complete Cleft Lip and Palate. Part 2: Craniofacial Form and Nasolabial Appearance. Cleft Palate Craniofac. J. 2005, 42, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Mølsted, K.; Brattström, V.; Prahl-Andersen, B.; Shaw, W.C.; Semb, G. The Eurocleft Study: Intercenter Study of Treatment Outcome in Patients with Complete Cleft Lip and Palate. Part 3: Dental Arch Relationships. Cleft Palate Craniofac. J. 2005, 42, 78–82. [Google Scholar] [CrossRef]
- Semb, G.; Brattström, V.; Mølsted, K.; Prahl-Andersen, B.; Zuurbier, P.; Rumsey, N.; Shaw, W.C. The Eurocleft Study: Intercenter Study of Treatment Outcome in Patients with Complete Cleft Lip and Palate. Part 4: Relationship among Treatment Outcome, Patient/Parent Satisfaction, and the Burden of Care. Cleft Palate Craniofac. J. 2005, 42, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Shaw, W.C.; Brattström, V.; Mølsted, K.; Prahl-Andersen, B.; Roberts, C.T.; Semb, G. The Eurocleft Study: Intercenter Study of Treatment Outcome in Patients with Complete Cleft Lip and Palate. Part 5: Discussion and Conclusions. Cleft Palate Craniofac. J. 2005, 42, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Semb, G. International Confederation for Cleft Lip and Palate and Related Craniofacial Anomalies Task Force Report: Beyond Eurocleft. Cleft Palate Craniofac. J. 2014, 51, E146–E155. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Cleft Repair (Yrs.) Mean (SD), [min–max] | Age at ABG (Yrs.) Mean (SD), [min–max] | Age at Collection of Models (Yrs.) Mean (SD), [min–max] | |
|---|---|---|---|
| Early ABG | |||
| males (n = 21) | 0.6 (0.1); [0.4–0.8] | 2.1 (0.6); [1.4–4.1] | 9.5 (0.8); [8–11.3] |
| females (n = 7) | 0.7 (0.2); [0.5–1.1] | 2.1 (0.5); [1.6–3.1] | 9.8 (0.4); [8.8–10.1] |
| males and females (n = 28) | 0.6 (0.1); [0.4–1.1] | 2.1 (0.6); [1.4–4.1] | 9.5 (0.7); [8–11.3] |
| Late ABG | |||
| males (n = 19) | 0.8 (0.2); [0.5–1.2] | 8.5 (1.2); [7.3–12.8] | 11.3 (1.5); [9.5–13.9] |
| females (n= 14) | 0.7 (0.1); [0.5–1] | 8.7 (1.4); [7.2–12.9] | 10.1 (1.3); [8–13.9] |
| males and females (n = 33) | 0.7 (0.2); [0.5–1.2] | 8.6 (1.3); [7.2–12.9] | 10.8; 1.5; [8–13.9] |
| Control | |||
| males (n = 25) | N/A | N/A | 8.5 (1); [6.8–11.6] |
| females (n = 35) | N/A | N/A | 8.6 (1.4); [6.3–11.8] |
| males and females (n = 60) | N/A | N/A | 8.6 (1.2); [6.3–11.8] |
| % Variance | % Cumulative Variance | Broken-Stick Criterion | Variance | |
|---|---|---|---|---|
| PC1 | 26.1% | 26.1% | 1.0% | 0.003247 |
| PC2 | 12.0% | 38.1% | 0.9% | 0.001487 |
| PC3 | 11.9% | 49.9% | 0.8% | 0.001480 |
| PC4 | 7.8% | 57.7% | 0.7% | 0.000967 |
| PC5 | 6.4% | 64.1% | 0.7% | 0.000799 |
| PC6 | 4.7% | 68.8% | 0.7% | 0.000584 |
| PC7 | 3.7% | 72.6% | 0.7% | 0.000465 |
| PC8 | 3.6% | 76.1% | 0.6% | 0.000444 |
| PC9 | 2.9% | 79.1% | 0.6% | 0.000365 |
| PC10 | 2.4% | 81.4% | 0.6% | 0.000296 |
| PC11 | 2.0% | 83.4% | 0.6% | 0.000244 |
| PC12 | 1.6% | 85.0% | 0.6% | 0.000194 |
| PC13 | 1.3% | 86.2% | 0.6% | 0.000157 |
| PC14 | 1.1% | 87.3% | 0.6% | 0.000137 |
| PC15 | 1.0% | 88.3% | 0.5% | 0.000119 |
| PC16 | 0.9% | 89.2% | 0.5% | 0.000110 |
| PC17 | 0.8% | 90.0% | 0.5% | 0.000098 |
| PC18 | 0.7% | 90.7% | 0.5% | 0.000093 |
| PC19 | 0.7% | 91.4% | 0.5% | 0.000083 |
| PC20 | 0.6% | 91.9% | 0.5% | 0.000070 |
| PC21 | 0.5% | 92.4% | 0.5% | 0.000062 |
| PC22 | 0.5% | 92.9% | 0.5% | 0.000057 |
| Difference in Procrustes Distance | p-Value | |
|---|---|---|
| Control vs. Early ABG | 0.0951 | <0.001 |
| Control vs. Late ABG | 0.0967 | <0.001 |
| Early vs. Late ABG | 0.0407 | 0.042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brudnicki, A.; Petrova, T.; Dubovska, I.; Kuijpers-Jagtman, A.M.; Ren, Y.; Fudalej, P.S. Alveolar Bone Grafting in Unilateral Cleft Lip and Palate: Impact of Timing on Palatal Shape. J. Clin. Med. 2023, 12, 7519. https://doi.org/10.3390/jcm12247519
Brudnicki A, Petrova T, Dubovska I, Kuijpers-Jagtman AM, Ren Y, Fudalej PS. Alveolar Bone Grafting in Unilateral Cleft Lip and Palate: Impact of Timing on Palatal Shape. Journal of Clinical Medicine. 2023; 12(24):7519. https://doi.org/10.3390/jcm12247519
Chicago/Turabian StyleBrudnicki, Andrzej, Tereza Petrova, Ivana Dubovska, Anne Marie Kuijpers-Jagtman, Yijin Ren, and Piotr S. Fudalej. 2023. "Alveolar Bone Grafting in Unilateral Cleft Lip and Palate: Impact of Timing on Palatal Shape" Journal of Clinical Medicine 12, no. 24: 7519. https://doi.org/10.3390/jcm12247519
APA StyleBrudnicki, A., Petrova, T., Dubovska, I., Kuijpers-Jagtman, A. M., Ren, Y., & Fudalej, P. S. (2023). Alveolar Bone Grafting in Unilateral Cleft Lip and Palate: Impact of Timing on Palatal Shape. Journal of Clinical Medicine, 12(24), 7519. https://doi.org/10.3390/jcm12247519